Friday just gone, 25th April, was World DNA Day. I’ve had a series of blogs that I’ve been playing around with linked to both DNA in our everyday lives and two book reviews where the world changes because of genetic testing and genetic manipulation. I thought I would write these posts, because as much as artificial intelligence could change the way we live and is frequently discussed, we are all accessing DNA based testing more and more, with many of us not really thinking about how this too is changing the world in which we live. Depending on how you feel about science and needing to have a refresher on what DNA and how we look for it and interpret it, you may want to hit up part one of this blog series first.
In part one I also introduced the kind of testing that DNA and DNA sequencing can be utilised for, not just in a accredited healthcare laboratories, but also linked to private companies who offer information on things like ancestry. In today’s blog I wanted to go a bit more into what can be the less thought about results of sending away your DNA, and also what kinds of things you might want to think about, or have in place, before you do.
Thinking unexpected consequences?
In part one I used this quote from a recent article:
As stated in a recent Independent article:
As they’re based on estimates, I suggest treating home DNA tests as a fun investigation to get to know your family history a little better rather than a to-the-letter representation of everything that’s ever happened in your gene pool – Ella Duggan Friday 28 March 2025
https://www.independent.co.uk/extras/indybest/best-dna-test-uk-ancestry-b1944632.html
It describes sending away of your DNA as a fun investigation, and recommends not taking the results too seriously. This is definitely the right attitude in many ways, as you wouldn’t take key health guidance from a magazine quiz, you’d want to speak to a healthcare professional who can put your results in context. The problem with not taking the tests themselves too seriously is that we don’t really think about the consequences of taking them or where the results might lead. My family have been given these for Christmas, for instance, and it was seen as a fun piece of science that could be done after lunch. Taking and sending away your DNA, the thing that makes you you, however, should always be done with a little more consideration that that. So I thought it might be useful to use just a couple of examples of why.
Health services
Sending away DNA for health reasons to private companies has been controversial ever since it was introduced into the UK and there are a few reasons why this is the case.

Firstly, if you have health concerns, then really you should be accessing medical care through healthcare professionals who you’ll be able questions, and who can put your results into a risk context for you based on your own medical history, rather than just getting a list of genes in isolation.
One of the other reasons you should manage this form of testing through health providers is that you can then be linked into any medication or further testing that is required. The presence of a gene alone can be pretty meaningless, you need to then look for whether that gene is being expressed (see part one) in order to really understand it’s impact, and so there are likely to be follow up requirements to any results received.
If you are going through genetic testing, especially if it has impacts on decision such as reproduction, you would normally be supported through the process ahead of the testing, and when the testing is returned, through professionals such as genetic councillors. If you get your results by sending your DNA away you may get completely shocked and surprised by the results that you can get back, and may make some decisions based on the findings that may not be correct for you and require better input from someone more used to interpreting the results. It could feel like a really lonely way to hear bad news.
Finally, these tests are being sent off to laboratories that don’t require accreditation. They are acting as medical tests, without going through the rigor that is required for the equivalent tests in healthcare, and yet are interpreted, by some, in the same way, and therefore effectively out of context. They may also not have the required levels of validation linked to the information and interpretive guidance that is issued with a result, so that you know what being present or absent for gene X or Y actually means for you. It also means that there may be less processes in place to ensure that you get the result that is actually meant for you and not for Professor X down the road. If you are processing hundreds of samples this kind of error, without safety checks, can be easier than you’d think. Knowing the quality of the result you are receiving may be less than obvious.
Ancestry services
OK, OK, I can hear you say. I wouldn’t send my DNA off for medical testing, but surely sending it off for ancestry services is ‘no harm, no foul’ and just a bit of fun. My first caveat here is that not all ancestry services are the same and not all of them look at the same sections of your genome. Some will look at your mitochondrial DNA (which will always come from your mother and your maternal line) in order to give a view of where your ancestral DNA comes from over generations. This is often referred to ancestral origins, and is much less likely to hit you with real time life dilemmas. Many kits are also paired with items that look at wider genomic matches, or DNA matches, and so you may get back more than you bargained for if you didn’t look closely at what was going to be provided.
I’ve included just a couple of, extreme, examples of how these kinds of unexpected consequences can play out in real life. The first is a BBC News story that came about because a woman was contacted by a stranger after sending off her DNA via an ancestry site. From the results it eventually became apparent that she had been accidentally swapped as a baby in a hospital in her 50’s with another child. Thus having dramatic and rather unexpected consequences for her and her family.
The other example I’ve included links to a couple of documentaries where the use of DNA matching platforms has uncovered serious misdemeanors or crimes, including IVF undertaken using the sperm of medical professionals without the knowledge or consent of the parents involved, and sperm donors being involved in the insemination of more couples than disclosed, thus increasing the risk of their children potentially interacting/dating/mating in later life without knowledge of their genetic linkage. This is obviously not the fault of the DNA matching service, and is something that is beneficial to uncover and stop, but has hugely dramatic impacts on those involved without any prior warning or support in place. It certainly wasn’t what they expected when they sent away their swab.
Is it just human DNA that counts?
Finally, to follow up on the takes of the unexpected, and because infections are fascinating, I wanted to share a link to a video that I think is really great about the first time DNA testing of HIV was actually used to convict someone of a crime. This one isn’t a word of warning, as I suspect that none of us are going to decide to deliberately inject someone with HIV contaminated blood, but I wanted to end this section with something where the use of DNA testing in the hands of people who really know what they are doing is a powerful tool for good. Also, because I wanted to give a non-human example of where I think some of this may go in the future.
What do we need to know before we start to send our DNA away?
Having laid out my warning stall, I wanted to go through some things I think you should actively think about before sending your DNA away.
What is the legal situation?
First and foremost, the sending of DNA away for processing is covered under something called the Human Tissue Act or HTA (in England). I’m flagging this as the first thing as, unlike what you see on TV, you should not be taking DNA from other people and sending it off to see what it says, and especially not for any form of DNA match testing. In the UK, if you do take anyone’s DNA sample without them being aware of it, it is considered a violation and you are liable to prosecution which can result in up to 3 years imprisonment. It is not OK to steal someone else’s DNA without their consent! There’s a lot to this one and I’m not a legal expert, but it seems to be something that many people are not aware of and now you know.

What level of information will be gathered?
All of the different tests offered will do things, and companies interpret the results slightly differently. It’s incredibly important to know what you are sending your DNA away to be tested for, how it will be tested and what kind of information you can expect back.
The main types of DNA tests and the areas they analyse are:
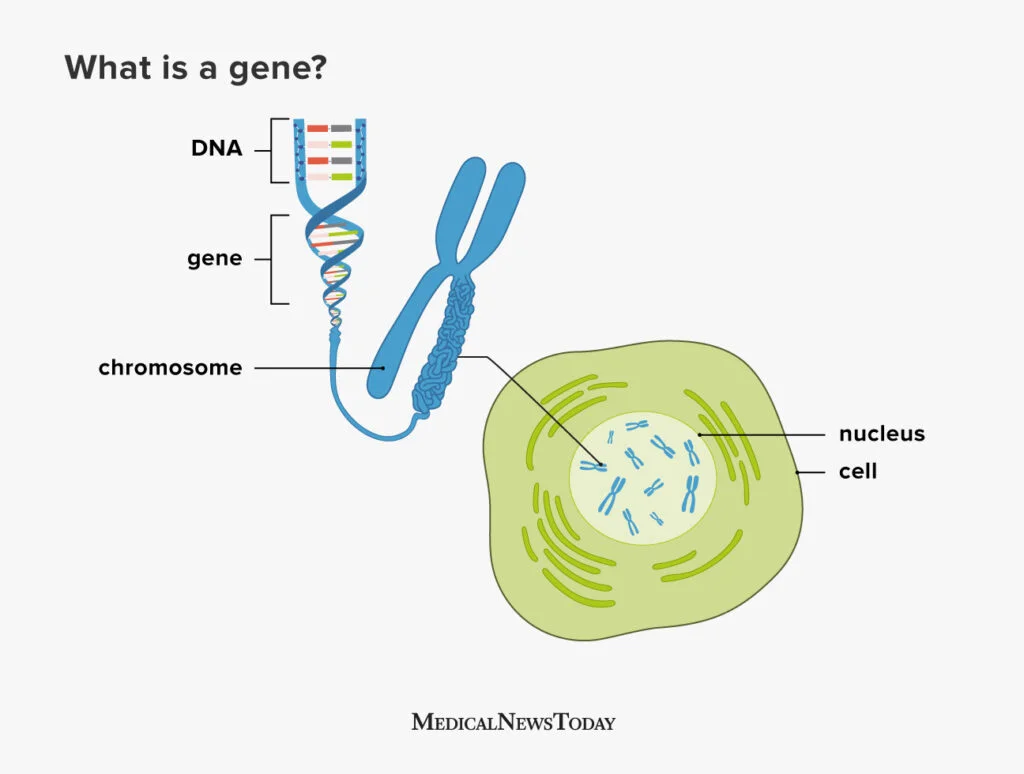
- Autosomal DNA Tests = examine the 22 pairs of autosomes and the X chromosome.
Commonly used for ancestry testing and can help determine ethnic origins, identify genetic predispositions, and find relatives. Utilise single nucleotide polymorphisms (SNPs), which are variations in a single DNA base pair - Y-DNA Tests = analyze the Y chromosome, which is passed down from father to son.
Used for tracing paternal lineage and can be helpful in genealogical research - Mitochondrial DNA (mtDNA) Tests = use mitochondrial DNA, which is inherited maternally (from your mother) used for tracing maternal lineage and can be helpful in genealogical research
- Paternity Tests = examines specific regions (loci) on the chromosomes to look at parental relationships
- Health-Related Genetic Tests = looks for specific genes or regions of the genome that are associated with certain health conditions to try to identify genetic risks, diagnose genetic disorders, or assess treatment options
You may need to read the small print to really understand how the testing will be undertaken and to manage your expectations. If you can, make sure you look up examples of what the results you will receive will look like, and if there would be any follow up support given. Also, crucially see if there will be additional funding required to get access to the full data set you are expecting so you don’t get hit by any unexpected requirements.

How will data be used?
The next few sections are all linked to what happens to the results of your testing that you are sending away.
The first thing to check before you send off your test is how long will your data be stored for once. This is important for you in terms of being able to access reports, but also about how long your legacy data will be available. Will you have access to wider information if you request it to be passed to your healthcare provider? Is there any information on the data analysis tools used? Are you even allowed to ask questions or is all patented and under intellectual property rules, which is reasonable but you should know what the boundaries are. Most healthcare reports should be kept for at least 10 years, but as these are covered under different guidance, will you only have access to download your data for a set period of time? Will it be possible to get your own local back up of your data? Once you know the answers to these questions you can then make active choices and comparisons about which aspects are important for you.
Who will have access to the data?
The article below is a little old, as it’s from 2018, but many of the questions still stand. How carefully will your data be ring fenced? You may not think about it much, as your DNA may hold little financial value to you, but DNA databases are one of the main assets that companies who process your DNA have, and why the testing is actually relatively cheap. Having access to thousands of DNA sequences, along with medical histories sometimes, means that data is incredibly value for scientific and commercial development. This is OK, we need sequences to develop new testing. Pharmacy companies also need access to sequences to develop and model new medicine. Therefore, it is likely that your data monetised and used for other purposes, which may or may not be OK with you. The big question to ask is whether it will be anonymised and how it will be used. Knowing this information before you commit allows you make informed choices, as not all companies are likely to be identical in how they handle things.
Another aspect that you might not think about is data security. If your data is of value to the company, and therefore is a potential asset, then it may be of interest to others. This can make data security to prevent things, such as hacking, important. This could be especially true if your DNA reveals linkages of significance, or things that you might not wish disclosed, such as cancer risk. Doing some research to ensure the security of any data that is held is important, but not often high on the list of questions that people ask.
Who can data be released to without my knowledge?
I’ve talked above about who will have access to your data, but mostly I talked about your anonymised data. It may not just be anonymised data that you are concerned about by however. If you are sending off for testing that relates to cardiac, cancer, diabetes or other risks, than this can have much wider impacts if shared. The legal landscape in relation to this is very much changing and catching up with the concept of genetic information as a protected asset is slow. Also, warning, I’m no expert in this. However, when sending away for this kind of testing it is important to know that it is often not covered by medical confidentiality, as it’s not considered a medical test when conducted via private companies. Being aware of how this impacts the rules around your data and what the company will or will not release is key. Why is it key? Well, it can impact all kinds of insurance schemes, from requirements to declare for holiday insurance if you are seen as ‘knowing’ a risk, to life insurance changes in cost or profile if released directly to the company. Knowing whether your personal, non-anonymised data can or will be released is essential before choosing whether or to whom you’re prepared to send you swab away to.

I suspect that this last point will probably impact those of you reading this blog less, but for to complete this list…….your DNA can also be released to law enforcement, depending on the country, so if you’ve secretly been a mass murderer then maybe don’t send your swab away and get your DNA added to a mass database.
What will happen if the company is sold?
As I said earlier, one of the biggest assets these companies hold is the databases of DNA sequences which we provide them. When something happens to the company therefore, it is this asset that many of those interested in the company might be after, and they may have nothing to do with the purpose you sent your testing for. Reading the small print before you send away your sample may not be able to prepare you for what happens when those rules change and you are no longer dealing with your original commercial provider. The one thing you can do in these circumstances in understand what access and rights you have to request that your data is deleted, or to delete it yourself, in the case that circumstances change.

And now for something different
I’m aware that the section above on what you might need to think about is pretty heavy and so I wanted to finish part 2 on something a little more population level and upbeat in relation to why having access to this testing is a good thing for science in general. For instance, we know that the ability to undertake ancestral testing was a reason that the bones of Richard III were identified and confirmed, which had big impacts for history buffs. It show that the use of wider availability of testing has all kinds of benefits, and not just to science. In terms of wider science, being able to look at bones using DNA testing has supported identification of Mycobacterium tuberculosis as present in Egyptian mummies which has helped us understand the evolution of this infection over centuries. More recently, looking at the development of Homo sapiens and how we became the human beings we are today has been forever changed by wider applications of these methods. Use of these technologies can therefore impact all aspects of our lives moving forward, and it really is up to us, both as individuals and as a society, about where they work for us.
Parts three and four of this blog series will be linked to book reviews that explore what those futures could looks like if the use of DNA testing and genetic manipulation change how we look at ourselves and others. So join me in continuing to explore the power of DNA.

All opinions in this blog are my own