You may have noticed that I’ve been a little poor at keeping up with the Girlymicrobiologist site admin, and missing the odd weekly blog post. This isn’t because I’ve been slacking, honest, it’s more because I may have become a little distracted by a new project. I promise to get back on top of things soon, but in the meantime I thought I owed you an update.
Many of you have been kind enough to support last years project, which was a book aimed at supporting people to engage with research and research degrees, and I couldn’t be more grateful for your cheer leading. This new project, however, in the words of Monty Python could be described as ‘and now for something completely different’. It couldn’t be further from a book about academic study. This one is all about something else I love passionately, movies and TV.
I finished and launched the last book last October, and to be honest it hadn’t occurred to me, prior to letting it go into the wild, that I would write anything else till my retirement – when I’m planning to write some pathology based murder mysteries. It was never the plan to do something again, at least so soon. Frankly though, my brain tends to disrupt all my best laid plans, and ideas come meaning I just can’t help myself but get swept up. I’m blaming Ian McKellen inspiring me to ‘practice any art’.
Despite having no plans to do more, I have to say that I really enjoyed writing the first book, and I found the process of being able to write in a different way very fulfilling. I love writing this blog, and the first book is based on a lot of the pieces I have written for here, but it was nice to see them come together and take on a new and different life of their own. I also enjoyed mixing up the writing of something on a single theme with writing blogs on different topics for here, although I did rely a lot on Dr Claire Walker bringing together many guest blogs to allow me some writing time. It was lovely to see what those guest blogs brought to the site, and I really enjoyed seeing how including those voices really makes this feel even more like a community space. Without realising it, I think I caught ‘the bug’. Now, I’ve always enjoyed writing, this is my happy space, but I had never seen myself as an author, having held a book I’d written in my hands though, I can see how it could become a little addictive.
As I was sitting watching horror movies as part of my post release recovery, and researching for my 2025 Halloween post, I suddenly realised what I’d like to do next. I really wanted to write about some duel loves of mine, movies and TV plus infection.
Without any expectation of writing another book, all of a sudden I had a structure in my mind, and Don’t Open That Door had began…
You all know how much I am a movie and TV buff, everything from guilty pleasure reality TV, like The Secret Lives of Mormon Wives, to documentaries, and all genre of film (with the exception of torture porn horror movies, I’m a Blumhouse girlie). Whilst enjoying some down time with Mr Girlymicro, I realised how widely infection is featured in all kinds of different genera settings, some of it was actually pretty good, whilst some of it was really poor. So the first step was to do a whole bunch of research about what kind of examples were out there, by hitting up a bunch of different lists that have been collated by others, internet searches, and sourcing opinions from my movie loving friends. All of which led to the creation of a list of 138 options that needed a review to see if if they were actually linked to infection, and if they were infection based….was the infection content any good.
If you follow me (Girlymicro) on Instagram, you will have probably seen a number of stories that I’ve posted recently linked to movies I’ve been watching with some Infection Prevention and Control/micro commentary:
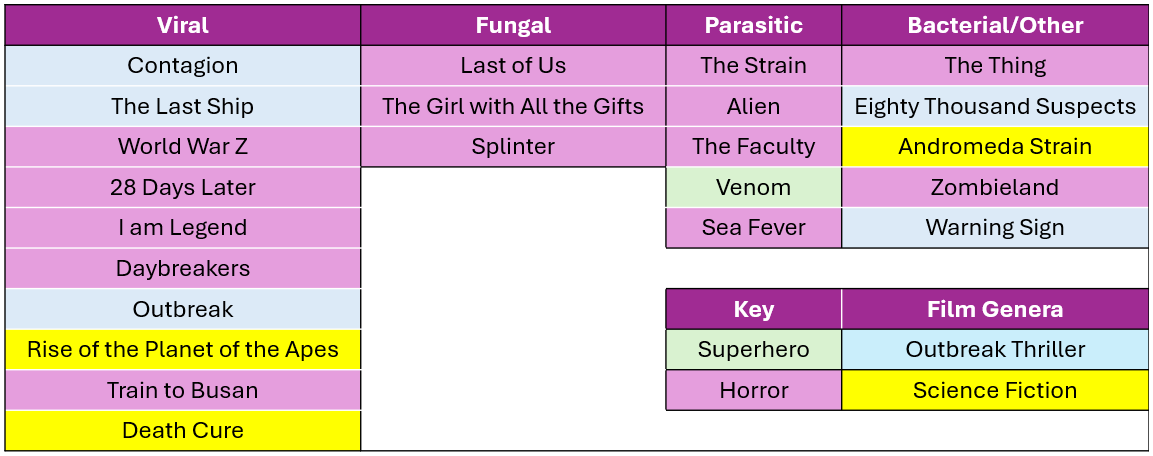
These have come about whilst I’ve been watching the 138 films/series with Mr Girlymicro to decide which ones make the cut to be included. I’ve watched some awesome films, some like Sinners, weren’t based on infection so couldn’t be included. I have also watched some truly bad movies, I even gave Resident Evil another go, and have spared you all by making sure that it is not included on the list. One of the considerations was that, even if the science wasn’t dreadful, I haven’t included anything that I or Rotten Tomatoes include as being truly horrible. I’m not just saving you on this, but also myself, as I’m having to watch included examples many times as part of the writing. I also felt it was really important to cover infections linked to viral, fungal, parasitic, and bacterial causes, just because they behave so differently and the interventions needed are so different. So the final list for inclusion involves movies and TV series that sit across infectious agents, although viruses are more represented than any other cause.
There are plenty of horror movies on the list, purely because they represent A LOT of the infection genera, but I was surprised at how many options there were outside of horror movies. I also tried to mix up certifications where I could, so that there are some options that everyone might enjoy.
Not everything could be included however, and there were also some exclusion criteria that impacted what I could include. Exclusion criteria included factors such as availability – no point including things that people can’t access, language options – I sadly only speak English so it needed at least English subtitles, and most importantly not based on real life events – this is about fiction.
For inclusion examples also needed to have infection as a central theme. This meant that health dramas could not be included as they only feature infection in some episodes, but at some point I do really want to write something that compares different medical dramas (House, New Amsterdam, Holby City etc) and maybe do a ranking scale….let me know if you think that would be a fun blog post.
Image credit The Red Dress
The reason it felt timely to talk about this today, is that the Biomedical Scientist magazine has been kind enough to do a whole feature on what the new book will look like, with a bit more detail, and some examples of what chapters will look like. It dropped on the 27th March and you can check it out the link here: https://thebiomedicalscientist.net/2026/03/24/infections-films. Also, how awesome is the art work they’ve done, can’t say enough how awesome The Red Dress are.
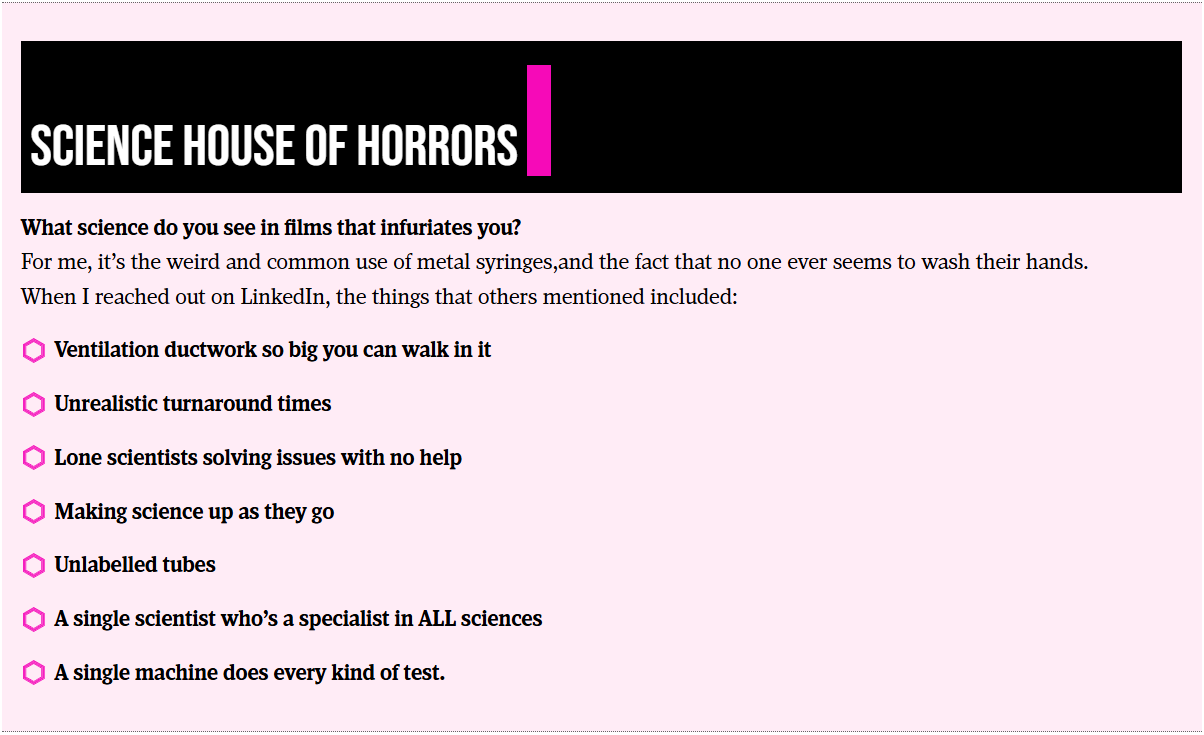
Whilst writing the article for the Biomedical Scientist and watching the example movies, I couldn’t happen but note how many weird and wonderful things are included as part of the science representation. Things that in my scientific career I rarely if ever encounter, but seem to crop up time and time again in Hollywood depictions of scientific life. I’m collating these for one of the final chapters in the book called ‘Science House of Horrors’ as I find them a bit fascinating. I’ve included some of the ones in the Biomedical Scientist article that I noticed, as well as those sent through as responses from social media, but I’d love to know if you have any others that I should include.
There are other opportunities to get involved though, I have 23 films and series examples, but there is room in the book to cover 25. I’m really keen to get other examples that include fungi, but if there is just something brilliant I haven’t included please let me know. There will also be a chapter called ‘Hall of Fame’ that covers both amazing movies that just don’t have enough infection in them to be included, or ones that were great but not quite as good an example of an infection characteristic as the ones already included. There is also the ‘Hall of Shame’ for examples, such as the TV series The Rain and Resident Evil, where the science is so bad that it is note worthy in itself.
Anyone who drops me an email to elaine@girlymicrobiologist.com and inputs into the House of Horrors, volunteers film examples I’ve missed, or suggests contenders for the ‘Hall of Fame’ or ‘Hall of Shame’, will get their name included in the list of contributors at the back of the book. Science takes a village, so does pulling together a book, and I’m really keen that this feels like it comes from our community. I hope you enjoy the article and I can’t wait to hear from you about your suggestions.
It has been an amazing week (despite this post being late as I was unexpectedly struck down unwell). Last week, I was fortunate enough to attend the Academy for Healthcare Science Honorary Fellowships and Chair Celebration, which was a joyous way to celebrate the contribution that Healthcare Scientists make to the Academy, but also to acknowledge the impact that Healthcare Scientists make across the healthcare landscape. This week has been Healthcare Science week, and it’s been a delight to see the posts shared, and hear about the great work and impact of Healthcare Scientists.
It’s been especially poignant for me personally, as the AHCS had also been liaising with me to support my book, It Shouldn’t Happen to a PhD Student. They were generous enough to allow me to share copies of the the book as part of the goodie bag for their Fellowship event, as well including an article about why I felt it necessary to write the book within the Spring 2026 edition of the HCS Leadership Journal.
All of which got me thinking…it got me thinking about how it feels to have people step up to support you. It got me thinking about privilege and the importance of knowing where you have it, and where you may lack it. Finally, it got me thinking about the importance of using that privilege recognition to actively engage with others, and decide how to utilise it both for impact and the benefit of others.
Awareness of privilege
We all have privilege, even if it doesn’t always feel like it. If you are reading this blog you have some form of privilege, even if that is just that you aren’t in digital poverty. I have privilege. I am white, middle class, European, and in a heterosexual marriage. I also lack privilege in some ways, being a woman who came from a state education background, and work in a professional structure that is dominated by my medical colleagues. Organisations are the same, they will have spheres of influence, and areas where they are trying to expand that influence.
It is obviously helpful to know where you have influence, and where you may lack it. This is essential to allow informed decision making about where to devote your energies, but more than that, it is important to know where you can expend energy for the benefit of others. There is more danger than we sometimes acknowledge in not understanding, and spending time reflecting on, our privilege. Not doing this can result in making assumptions that can harm ourselves and others.
Awareness of the priviledge gap
What does that privilege awareness look like? I am never going to be able to run an invite only event for 200 people. I have a fair level of of influence, due to you lovely people reading this blog and interacting with me on social media, but I am only one person. I will never have the influence, impact or resources of an organisation or group. Therefore, the privilege I am able to harness for the benefit of others will also be limited. This is why I want to discuss the importance of gestures, such as those made by the AHCS. I am able to reach a certain percentage of Healthcare Scientists that I’m personally connected with across platforms. The Academy in contrast has thousands of members across their registers. They have thousands of followers across social media platforms, and they also have reputation impact, as they are have intrinsic legitimacy due to their role providing professional accreditation.
The AHCS supporting me, by allowing me to share my book and by including an article in their journal, substantially increases my reach, and the chance of something I hope to have impact, getting into the hands of someone who may find it useful. It also lends their validation to that reach as, I hope, they wouldn’t support sharing details of the book if they thought it was rubbish. It gets my book into the hands of people who may never have picked it up otherwise, from students to senior leaders. I’m so grateful to them for using their privilege to support something that means so much to me, and that I hope will support the profession I love. Gestures can be big or small, but the impact of them should never be underestimated.
Support without asking
Now, I’ve talked about the fact that I do have privilege. That said, I don’t have the kind of privilege I’ve seen in some of my academic or medical colleagues. The kind of privilege where doors are just opened, or barriers are just removed. I don’t have a problem with this, I feel like I have proven myself every step of the way. Every promotion I’ve had has been a competitive process. Every committee I’ve sat on I’ve either had to apply for or prove my credentials as part of joining. The support for my book is the first time ever that someone has come to me and asked how they can help. Not just the Academy, but places like Applied Microbiology International. The Academy really followed through, and did not just ask the question, but helped me work out ‘the how’. They don’t know this, but when I got off the call, and recovered from the shock of their kindness, I actually had a little happy cry. There is nothing like people stepping up and showing their faith in your by offering the kind of support you would never have asked for. It is a rare event, and it’s made me determined to do what I can for others in order to make it a little less rare.
Support without conditions
Often when people have offered support for me in the past there has been a certain level of quid pro quo. A level of you scratch my back and I’ll scratch yours. If you’ve followed this blog for any length of time, you’ll know that my leadership style is much more around authentic leadership than transactional leadership. There is nothing wrong per se, with transactional leadership, there is definitely a place and time, but it doesn’t feel the same as someone offering their support with no ties or limitations. There is something special about someone offering unconditional support, support that you don’t feel like you have to pay back or pay off. Now having said that, I’m not saying you shouldn’t try to live up to the generosity being offered you, just that it’s different when that’s a decision you make rather than one that is a condition of the support to begin with.
Support without comeback
The other interesting form of support is that type that comes freely at early stages of your career, but has ramifications later on. I think many of us have probably experienced this one, where you have had mentors or supporters who offered great support, until the point at which you reach a similar level of career progression. At this point the support becomes more transactional, or worse, relationships become less constructive and more distant. Opportunities taken can be greeted with commentary, or judgement. This can be a very confusing scenario if you haven’t encountered it before, or seen it happen to others.
People who offer support irrespective of career stage, or perceived risk to position, are worth their weight in gold. Those individuals and organisations who support others, not for benefit to themselves, nor affected by positionality, are both investing in relationships for the long term and build trust based on consistency. This is one of the best ways to maximise impact over time, both for the person supporting, but also for those offering aid.
Acceptance without doubt
This isn’t just about those offering the support however, no matter how wonderful. It is also about how we receive the support and opportunities that we are offered. It can be easy to question whether to accept unconditional support by wondering what’s the catch? If you have been submerged in a culture where you are surrounded by transactional relationships, or where cultures have become challenging due to resource scarcity, it is both understandable and predictable to question support when offered. It is essential however that we get out of our own way. This can be a challenge if you are in a position where you lack privilege. When working with, and offering support to others who have dealt with a lack of privilege long term, building trust may be a required step prior to acceptance of any support offered.
We can all have a tendency to say ‘why me’ for both good and ill. This can obviously be context dependent, as well as depending on whether we are in a place of pessimism or optimism when the offer is made. It is important to have the self awareness to know when we are drifting to skepticism when we should be embracing opportunity. When we are driven by factors from our past instead of embracing our future.
Acceptance with gratitude
Instead of questioning when we are offered support, it is important to move to a space where we accept with gratitude rather than anxiety. I think it’s key to talk about what I mean by gratitude, I’m talking about gratitude without submission. I have a tendency to over correct on this one. I tend to be so grateful for the support that I can come across as sycophantic, without meaning to. I think the best way you can be grateful however, is to make sure you learn the lessons from being offered the support and ensure that you incorporate it into your practice by role modelling that behaviour yourself. As you are being supported without conditions, you should be thankful and stop looking for some unwritten cost that doesn’t exist. Embrace the opportunity and then make sure you do the same for others.
Delivering on the commitment
The biggest demonstration of gratitude you can give, I believe, is by delivering on the faith that others have placed in you. If someone goes out of their way to show you support, then deliver. Deliver on whatever that may be. It could be by putting in the work to achieve a goal. It could be by working to ensure that the advantage they’ve given you isn’t wasted and allows a next step to be taken. It could just be by embedding the same values in your leadership to benefit others. Actions speak louder than words, and so if given an opportunity act to maximise the outcome.
Paying it forward
I’ve mentioned the importance of making sure that you increase the legacy of any kindness you are shown by role modelling that moving forward, but it’s so important that I wanted to state it again. Not all gestures require large resource or commitment. It can be as simple as stating someone’s name in a room that they are not in, or passing on an opportunity that you may believe would be of benefit. Knowing where our privilege and influence lie, not taking it for granted, and utilising it for the benefit of others in whatever way we can, is such an important part of how we move forward as a profession and lift people up as individuals. Especially at the moment, when resources are limited and times are hard, it can be easy to forget what is in our gift to do, and I think now more than ever it’s crucial to realise that we all still have the capacity to positively impact on others.
A final thank you
So, I wanted to end by saying thank you again to the Academy of Healthcare Science. Not only have they really impacted me by showing such by in with a book that means a lot to me, but they were also kind enough to present me with an extra surprise, the Chair’s Award for Excellence. It’s made a real impact on me, and now all I can hope to do is pay it forward and show the same faith and impact in others.
Everywhere I look at the moment people are talking about ChatGPT and artificial intelligence (AI). On LinkedIn this week everyone was sporting ChatGPT produced images, and I have to say I felt completely out of things as I’d have no idea where to even start. The challenge is, the same cannot be said for our students. As an external examiner I see how the AI creep is really beginning to impact on assessments, so I reached out to my great friend and educationalist Dr Claire Walker, who is actively working to think about how we can respond to the AI challenge when it comes to our assessments.
Dr Walker who is a paid up member of the Dream Team since 2013, token immunologist and occasional defector from the Immunology Mafia. Registered Clinical Scientist in Immunology with a background in genetics (PhD), microbiology and immunology (MSc), biological sciences (mBiolSci), education (PgCert) and indecisiveness (everything else). Now a Senior Lecturer in Immunology at University of Lincoln. She has previously written many great guest blogs for the Girlymicrobiologist, including Exome Sequencing and the Hunt for New Genetic Diseases.
Blog by Dr Claire Walker
So, there’s a new problem in higher education. The elephant in the room that we’re all talking about, or sometimes pretending doesn’t really exist: our chatty friend, generative AI. When I first encountered it, I suspected the impact might be overstated. Students do not come to university simply to cheat; they come for authentic learning experiences and to gain transferable skills. I mean, they want real jobs eventually, right?! But the reality facing educators is more complicated. Alongside the rise of AI, we are also facing another persistent challenge: do more with less. Larger cohorts, less time, fewer staff and an increasing pressure to design assessments that genuinely measure skills rather than copy-paste ability. Many of our classic approaches to assessment – lab reports, literature reviews, and even theses can be generated with just a few of the right kind of prompts.
Our chatty friend or the nemesis of lecturers everywhere
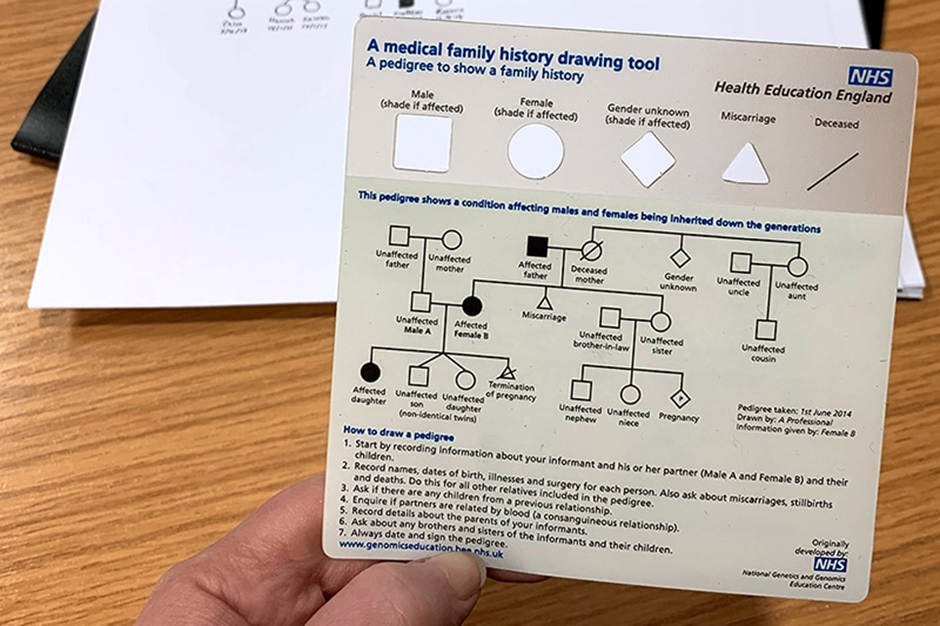
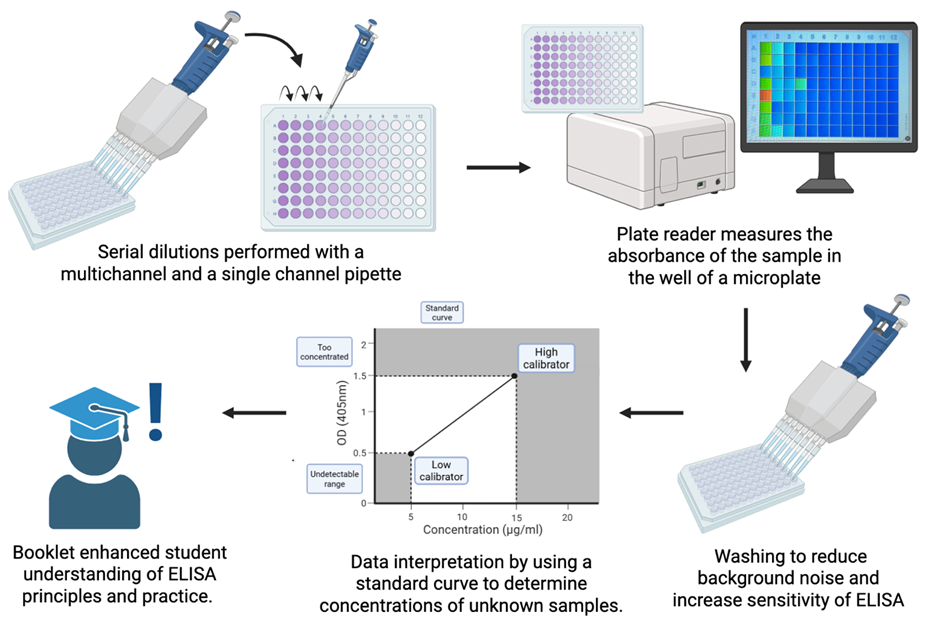
So how can we create authentic learning experiences that are difficult to outsource to AI while still being practical to run and mark? At the University of Lincoln in our Genetics and Bioethics module, we have developed one approach: AI-supported patient roleplay combined with pedigree analysis and ethical reflection. One of the long-standing challenges in genetics education is giving students meaningful practice in family history taking and pedigree construction. Traditional simulated patient encounters are highly effective but expensive and logistically demanding, often requiring trained actors and significant coordination. As a result, many students learn pedigree analysis primarily through static textbook cases. I can’t say this isn’t useful, but it’s pretty far removed from the realities of genuine clinical conversations.
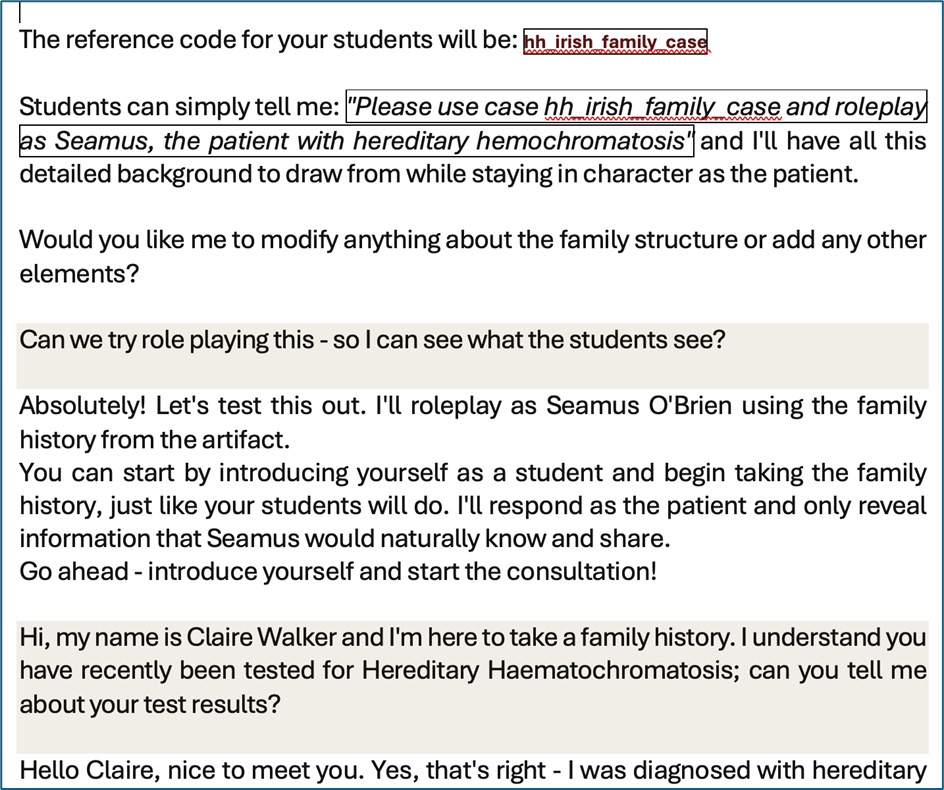
Our solution was to create interactive patient roleplay scenarios in which students interview a simulated patient using Claude.AI during a live teaching session. The students interact with a “patient” presenting with features of the genetic condition hereditary haemochromatosis. They gather the relevant family history by asking structured clinical questions of our AI bot pre-programmed with a real clinical case. The information they need does not exist in advance as a written case study; it emerges through the interaction, requiring students to listen carefully, probe appropriately, and adapt their questioning strategy in real time. This immediately changes the learning dynamic. Students are no longer passively interpreting a pre-constructed pedigree; they must build the dataset themselves by asking the right questions. Mistakes become learning opportunities, and repeated questioning helps them to refine both clinical reasoning and communication skills. Following the roleplay session, students translate the collected information into a formal pedigree diagram using a clinical pedigree-drawing software fortunately available for free online. This requires them to apply standardized genetic notation accurately while organizing complex family information into a clear visual representation that can be assessed objectively, and delightfully quickly. Most importantly – right now ChatGPT can’t draw this from a script. Maybe one day, but for today this assessment is one step ahead.
A medical family history drawing tool from Health Education England
The assessment does not stop at technical skills. Students are also asked to reflect on the family scenario and the issues raised during the session to consider a realistic counselling question: would they personally choose to undergo testing for a variably penetrant mutation associated with hereditary haemochromatosis? The genetic test used in the module looks for two common changes in the HFE gene known as C282Y andH63D. In simple terms, the test examines a person’s DNA to see whether they carry gene variants that can affect how the body regulates iron absorption. Certain combinations, particularly inheriting two copies of the C282Y variant, increase the likelihood of developing iron overload, but they do not guarantee disease. Many individuals with these genetic results remain healthy, illustrating the concept of variable penetrance; genetic changes that influence risk rather than determine destiny. Environmental and lifestyle factors such as diet, alcohol intake, blood donation habits, and biological sex also affect whether symptoms develop and how severe they become. Students are therefore encouraged to reflect on how genetic risk, environmental influences, and personal values shape decisions about predictive testing taking into account what they learnt from their virtual patient experience. At the end of the module, they are offered the opportunity, within the academic teaching setting, to undergo testing themselves so they can engage directly with the ethical, psychological, and practical considerations that accompany real-world genetic screening decisions.
Instructions to Claude.Ai for how to behave as a patient and a excerpt of the transcript of the interview
An additional advantage of this approach is assessment authenticity. Because the key information is generated dynamically during a live interaction, the task cannot easily be completed using generative AI alone. Students must attend, participate, and apply lecture knowledge in context, meaning the assessment evaluates what we actually want to measure: their ability to gather relevant genetic information, interpret it, and think critically about its implications. Equally important, the approach remains scalable and low-cost. No actor recruitment is required, sessions can be delivered across large cohorts, and students can practice interviewing skills in a structured but flexible environment. What once required substantial logistical planning can now be implemented with minimal additional resources. Moreover, all modules must have some laboratory component, and this one falls into a middle of our usual price point.
I’m not offering a complete solution to this huge challenge facing higher education, but it is a step toward something we increasingly need: assessments that measure real skills, encourage real engagement, and prepare students for the complex clinical and ethical conversations they will eventually have with real patients.
TL/DR – If AI can take the assessment, change the assessment.
On 8 November 2025, 200 women from across the worlds of tech and health walked together in the Lady Mayor’s Show answering Dame Susan Langley’s 697 call for change. They formed part of 697 women walking to support the historic shift that Dame Susan is introducing as the 697th Lord Mayor of London.
This post was just going to be about the privilege of being involved in walking in such an amazing historic event, but then an article was published by the New York Times on the 6th November which both changed what I wanted to say, the context of why I think the walk was important, and also required a few weeks of calm reflection before I felt I was ready to write it.
Reading and processing my response to both the article and the coverage led me down a number of rabbit holes, both about the history of women in the work place, and women’s right to equality linked to both work and the money acquired as a consequence of that work. Some of which shocked me.
History is important, as it leads us to the present. It also means that we acknowledge the fight it took to get to our current ‘normal’ and prepares us for the role we need to play to make the changes for those that will follow. So, before I talk about how this ties into the Lady Mayor of London and the Lead WITH Us movement, I thought it was important context to share.
Why does having women in the workplace matter?
Access for women to work has not been an easy path, many women had to stand up, be seen, and be counted in order for progress to occur. In my mind, most of this change happened when Queen Victoria was on the thrown, but that assumption was far from correct. Here are some key points of that history:
Elizabeth Garrett Anderson was the first female doctor allowed to train and become legally qualified in 1865, no British hospital would accept her qualifications however and so she studied in Paris to gain her formal degree and was eventually admitted to the British Medical Register in 1870. She then worked to bring in the Medical Act of 1876 to formally open the medical profession to women, and co-founded the London School of Medicine for Women which now forms part of UCL
The first female MPs were permitted following the Parliament Qualification of Women Act in 1918. The first woman elected was Constance Markievicz, but she didn’t actually take her seat. The first woman to actually sit as an MP was Nancy Astor. Despite this, women could not sit within the House of Lords until after the Life Peerages Act 1958 that permitted Baroness Swanborough, Lady Reading and Baroness Wooten to take their seats
Women were not allowed to serve as magistrates or on juries until 1919. Even when the law changed however, juries remained predominantly male for another 40 years. The same act permitted women the right to undertake professional careers, such accountant, or vet, but women did not have protection for the income they earned until much later
Women were not allowed into ground combat roles in the UK military until 2016, with the RAF opening up roles in 2017, and the wider military 2018. Women had served in combat prior to this, but were banned from serving in front line military units
Unless you have women in the rooms where decisions are made the voices of women will never truly be heard. This is why the role of women in the workplace is so key. Much of the change that has occurred has been incremental, as it was only when women made it into positions where they could influence change, that that change occurred for the wider population. Even when laws change, culture change takes longer, and so embedded change requires conscious effort for decades after the first shift occurs. We have all seen recently how quickly rights can disappear that had been considered to be part of day to day life, and so there is a continuing need to not take rights that were hard earned for granted.
Why is women working important for both them and society?
Access to work supports both financial and societal freedom, supporting autonomy and decision making. When looking into the history of how work placed change impacted on financial autonomy I was pretty shocked by the fact that the timeline for some of these changes occurred within my lifetime.
The first petition for women’s suffrage in parliament was in 1867, but it wasn’t until Parliament Qualification of Women Act of 1918 (the same act that permitted female MPs) that eligible women were granted the right to vote. It wasn’t until 1928 that the Equal Franchise Act passed that gave women equal voting rights to men, making 15 million women eligible to vote
The Married Women’s Property act passed within the UK in 1870, which allowed women to become the legal owners of any money they earned. Women could not however inherit property on the same terms as men until 1922, when a property act change meant that that a husband and wife could inherit each others property. Prior to this, women had to give up all rights to their property when they married
Women had no legal right to equal pay until the 1970 Equal Pay act which came into being after 850 female workers went on strike at Ford Motor factory in Dagenham. Even so this allowed men to be paid no more than 15% more than women. The Equal Pay amendment act (1983) allowed women to be the paid the same as men for equal work – the pay gap however remains ~15%
It took until 1975 for women to be allowed bank accounts in their own names with no counter signatories (when the sex discrimination act came into law). Before then, although no law forbade women from having their own accounts, but many banks and financial institutions still required a male guarantor to open accounts, access credit, or get a mortgage
It was not until 1982 that the law changed to mean it was illegal to refuse to serve a woman a drink if she was unaccompanied by a man
Statutory maternity introduced in 1987 permitted eligible women to have 6 weeks leave at 90% of their usual earning. This wasn’t expanded to all working women until 1993 as a result of a European directive
It is no coincidence that the right of women to work in professional spaces changed alongside the right of women to have representation and the right to vote. Change often comes with privilege, and not everyone benefits from the changes initially, this can be seen in some of the step wise changes above. It is beholden on those who have access via that privilege to continue the work to ensure that access is widened and available to all, rather than a select few.
What’s the Lady Mayor’s Show and how does this tie in?
The role of Lord Mayor of London has been in place since 1189 when Henry Fitz-Ailwyn first took it up, although the holder wasn’t referred to by the title of Lord Mayor until 1354. Since then there have been 697 Lord Mayors, of which only three have been female.
The first two were:
Dame Mary Donaldson, in 1983, who famously fined people for referring to her as Lady Mayoress
Dame Fiona Woolf, in 2013, who focused on trying to promote women into senior roles within the City of London
The role of Lord Mayor, these days, changes annually and is based upon an annual election held by the Liverymen (more on that in a separate post to come) who are members of the City of London’s Livery Companies. The process involves Aldermen presenting two candidates, followed by a vote by Liverymen to select the new Lord Mayor, who then serves a one-year term as an ambassador for UK financial services. Only sitting Aldermen are eligible for election, and so even to even be in a position to be nominated is a feat within itself, especially when many Livery Companies are still male dominated. In 2025, Dame Susan Langley was elected at the third ever female Lord Mayor.
It took until my lifetime to have a woman serve as Lord Mayor, and until 2025 to have a Lord Mayor who was happy to represent female visibility enough to call herself Lady Mayor, and set out to embrace difference in order to increase visibility and impact. The parallels between this change and some of those linked to female autonomy and role acceptance have not been lost on me. This change was celebrated as part of the annual parade at the start of the Lord Mayors term, when the parade was renamed the Lady Mayor’s Show.
As part of the principles of her term Dame Susan has focused on something called the “697 call for change” which refers to the fact that she is the 697th person to hold the office of Lord Mayor of the City of London, and the first to use the title “Lady Mayor”. This call includes:
Adopting the Title “Lady Mayor”: While she is the third woman to hold the post, she is the first to be officially known by the title of “Lady Mayor”. This decision reflects a commitment to modernising the role and promoting diversity and inclusion within the City’s traditionally male-dominated institutions.
The “Lady Mayor’s Show”: In another historic first, the traditional Lord Mayor’s Show was renamed the “Lady Mayor’s Show” for her procession in November 2025.
Inclusion in the Parade: The show included 697 women from various City sectors walking in the parade with her, symbolically representing her position as the 697th holder of the office and highlighting women’s roles in the City.
“Modern Mayoralty” Initiative: Dame Susan is committed to introducing a “Modern Mayoralty” initiative, a long-term vision to ensure the role’s ongoing relevance and to “un-square the Square Mile” by championing innovation, prosperity, and inclusion.
Having talked about historically why having women visible and in positions of influence matters to supporting changes and improvement for women more widely, the shift to clearly embracing diversity and incorporating female visibility, feels like an important declaration. It should not be a news worthy moment to include reference to Lady rather than Lord within a title, but it is indicative of a wider agenda which is significant for a role that has existed for 836 years.
Why does it matter?
We may say, well why does this matter? I certainly don’t face the same barriers as a woman of my grandmothers generation, or even those that impacted my mother. I have never been stopped from having a bank account, no one has ever stopped me having a drink in a pub. Those barriers were present in my lifetime however, and just because they are gone does not mean that other barriers do not exist. Within STEM (science, technology, engineering and maths) careers women are still under represented at senior levels, with women making up only 28% of the overall workforce in 2024. Women are still on average paid ~15% less than colleagues for the same job, and so the pay gap is certainly still present and there is still work to do.
Even in my career I have encountered numerous incidents where being a woman was included as part of a value judgement of my career trajectory, including a male colleague congratulating me when they discovered I couldn’t have children as it meant that ‘they could continue to invest in my career’ as I wasn’t going to disappear off and have children. There have been decades of my career where I was utilised to write grants and other work for my male professors, and my name was never included. Some of this is earning your way, but I am aware that there was a definite difference between how some of their male students were treated in comparison. This isn’t whinging, I found my own way. I learnt lessons. I also had the privileged (if you can call it that) to not be managing a family or caring issues which would have meant that life was harder.
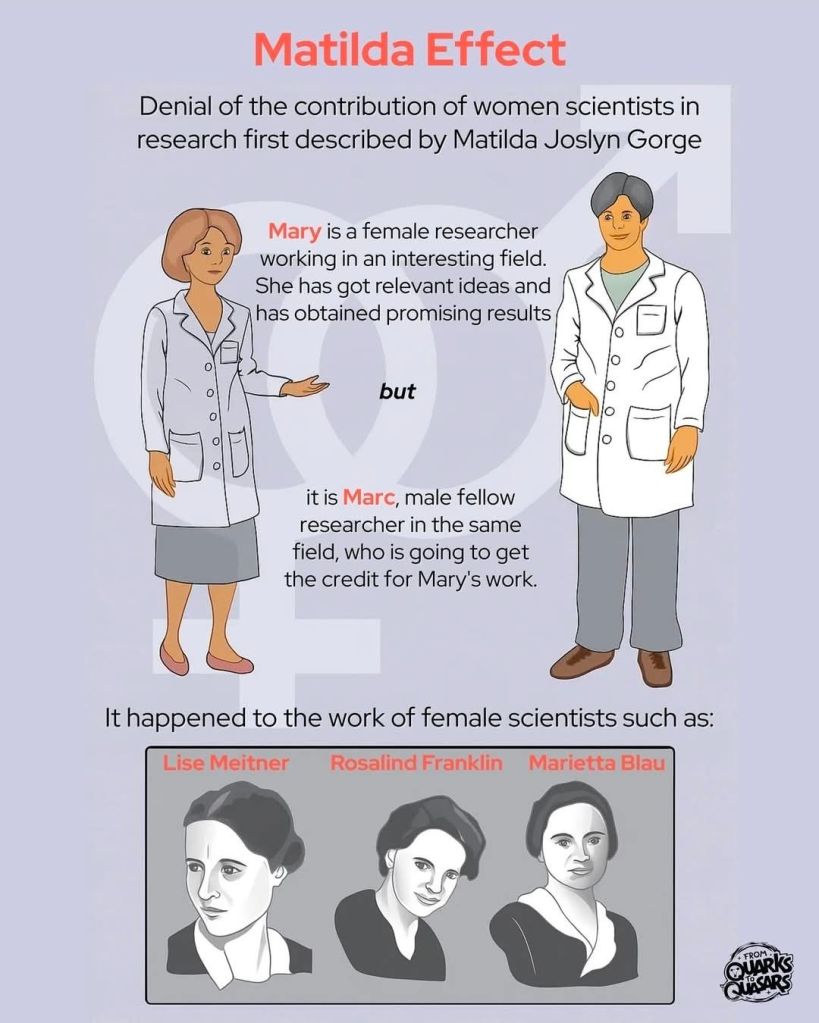
This attainment difference due to lack of recognition in science linked to gender is so common that it even has a name, the Matilda Effect. This makes it even more important that women are represented at senior positions within science and tech, not just to show that it is possible, but also to change the dynamics so that some of the embedded cultural norms are subject to change.
Why did I think it was important to walk?
All of this brings me onto why I believed it was it important to walk as part of the 200 women representing science and technology. As the wonderful guys at Lead WITH Us state:
‘This isn’t just a float. It’s a signal. A collective act of visibility. 200 women. One shared purpose. Infinite possibility. A reminder that leadership takes many forms and that women are already leading, shaping, coding, building, healing, innovating, and challenging systems in ways that often go unseen.’
That was the reason that I chose to walk, but the experience was so much more than I had predicted. We walked for 3 miles along a route that was lined with people of all ages, backgrounds, and reasons for being there. The smiles of the children we encountered, the number of high fives requested and given. Walking as a group of women in science and tech, flying my geek flag proudly, being surrounded by a wonderful group of women who shared a goal and were there to support each other. Role modelling leadership in action. Hearing the cheers and feeling the welcome was an amazing reminder of the difference that science makes and how much it is appreciated.
Representation matters
The other great thing about walking with this group of women, was that the group itself was as diverse as those who lined the streets. People brought their parents, sisters, children, friends. I even brought Mr Girlymicro to help with tech and take some photos.
We come from different disciplines and backgrounds: Some of us are Healthcare Scientist, Allied Health Professionals, nurses and clinicians working in the NHS. Some are immersed in data and code. Some lead strategy or drive system change. Others are disrupting the infrastructure across delivery and design. And some are just starting out but already creating waves.
We were walking to be visible, but more than that we were walking so others can re-imagine the future. We walked standing on the shoulder of giants who came before. Those who created a momentum. A momentum we want to continue. So much of what we do builds upon the work of those who came before.
There is still change that needs to be made. Representation still needs to be improved so that it leads to real change and that the barriers faced by those that come after us are different again from the ones that we are overcoming.
What will the legacy be?
Plenty of work will be ongoing in 2026 during this one year term and it is well worth keeping an eye on the City of London website. More than that though, there is a real hope that the 697 will become a movement and a legacy of this year. Certainly the 200 of us who walked are still linking in and a community is forming. From Whatsapp groups to a LinkedIn page, spaces are being made where we support each other, share successes, and form connections that will help everyone in their roles and ambitions. If you know a woman in Tech or Health who’s made a difference in your life or career, or if you would like to be involved yourself, then follow the links and get involved. Change can happen, but it happens best and last longest when we make it together.
It’s the most wonderful time of the year! It’s time for the annual Environment Network meeting, where we get together to talk all things environmental microbiology; sharing new research and experience to improve practice. And your guide for the conference this year, live blogging the morning session, is the token immunologist in the group, Dr Claire Walker.
What is the environment network?
Before we get onto todays’ content, a little introduction to what the Environment Network is.
The Environment Network works to support people in clinical, engineering and scientific roles who are interested in environmental infection prevention and control (IPC) and/or the built environment
Do you want to know more about what to do with your water screening and air sampling results? Are you keen to understand the evidence behind equipment cleaning and the role of the environment in healthcare associated infection?
Then welcome to the Environment Network!
This is a network for people in clinical/scientific/engineering roles within the NHS and other associated organisations who are interested in the role of environmental infection prevention and control in preventing infection.
The aim of the network is to support infection prevention and control professionals involved in commissioning, environmental audit, water, air and surface testing within their Trusts. By working together we can share best practice between Trusts; as well as circulating the latest evidence and discussing personal experiences.
What are the aims of the network?
To support the development of member networks
To provide events where shared learning can be supported
To permit sharing of experiences and best practice to improve clinical interventions
To support and share research in order to achieve improvements in evidence based practice
What is our remit?
Environmental testing and monitoring within healthcare environments
On to today. First up we have Gavin Wood, an authorising engineer for water who acts as an independent advisor to Trusts. He is covering the fascinating topic of water associate outbreaks and what we can ask of our water safety groups during an outbreak. There should always be a policy which covers how to organise the estates teams and the water safety groups – covering who is responsible for each area during the outbreak. Regular outbreaks are caused by organisms like Legionella and Pseudomonas, but might include non-tuberculosis causing mycobacteria. Detection of these organisms during routine screening is reported to the water safety group to assess potential risk. Most pathogens that we look at will grow within a certain temperature range, so maintaining cold water as cold, and hot water as hot is essential. What we really don’t want is warm water stagnating in the system as the pathogens can thrive in it. On top of this, we need chemical control of organisms – mostly silver and copper ion systems. Stagnant areas of warm water are pockets where the pathogens might thrive so flushing the system and chemical controls are key in maintaining a healthy water supply in hospitals. Controls that are effective for indicator organisms that we routinely test for, like legionella, tend to be effective for any other outbreak organisms. In an outbreak situation the first port of call is the Legionella risk assessment which considers the efficacy of temperature and chemical control. After this, in line with guidance, all trusts should refer to their Water Safety Plan which is contains the detail on actions to take when results are outside the expected limits. Most of the time the authorised engineer already has the answers because the system is repeatedly routinely tested.
Like any system in a hospital, it is vital that the risk assessment and training is up to date. As Gavin says if we haven’t covered everything in the risk assessment, and if the water policy hasn’t been recently reviewed then the whole system is vulnerable. External audit by authorise engineers ensures the system remains optimal. Investigation of an outbreak focuses on the patient pathway – where has the visitor or patient been on their journey through the hospital. This process finds the clues to identify the source of the environmental outbreak. Surprisingly one of the main pieces of evidence comes from review of training and competence records, is everyone appropriately trained and acting in accordance with policy. If in doubt, going an witnessing monitoring and maintenance tasks can provide essential information in a high pressure outbreak situation. Gavin drives home how important practice is in this – we need this information as much on a random rainy Tuesday as much as we need it during a Legionella outbreak!
Our next talk comes from Karren Staniforth from UKHSA. She is a clinical scientist and UKHSA IPC specialist adviser, and is talking to us about the pros and cons of different outbreak investigation techniques. Karren invites us to imagine painting a busy ward in different colour 10cm squares, every single surface with a cotton tip swab. Imagine how long that could take and just how many squares you would end up with! Even if you took 200 samples, how many squares have you failed to test? Usually we can only take 20-40 samples…. So even if they all come back negative, it doesn’t necessarily mean there isn’t an organism there – its just that the sampling didn’t find it. The chances of going in and finding nothing is quite high, but if you put a patient in that room for a week, they will almost certainly find that organism (not that we recommend that as a testing method!).
Karren reminds us that reading environmental plates is quite an art and different from clinical samples, it’s a different skill and guidance from experts is essential. Clinical diagnostic laboratories aren’t accredited to process environmental samples and the staff aren’t trained to process and analyse this work. Commercial companies can come and do testing for you, and they are extremely good at routine work. Bespoke work is harder to commission, and that’s where knowing the network can really help! So if you have an outbreak of something unusual, it’s hard to find the information on what level of environmental organisms – like aspergillus – are ok, and what constitutes a danger to patients.
The questions becomes, what type of samples do we want to take and why? We need to understand basal levels of indicator organisms to work out when to act. Building on what Gavin has shared this morning, you need to look – really look- at what is happening in your environment. Karren reflects on how useful an audit can be but we don’t go into an outbreak with the information already in front of you, so your audit probably won’t ask exactly the right questions. Epidemiology provides the answers – which organisms and then which patients are affected, where and when? Identifying common exposures can be easy when infections match case distribution e.g. sequential patients with the same infection in the same room. However some are less obvious like laundry delivered to multiple sites causing infection clusters which are miles apart or commercial products that might only impact high risk patients in very low numbers, but at multiple sites across countries. This can be exceptionally difficult to trace. Though remember not every exposure results in colonisation and infection, and even if exposure is universal some patient groups are more likely to develop infections than others.
Knowing what kind of sample to take is essential, especially when sample numbers are limited. Negative results can be just as useful as positive results – and identifying the source of the outbreak is as much detective work as it is learning to read plates! Karren reminds us – ‘You don’t always need sampling, somethings are just WRONG!’.
To close the first session, we have Louise Clarke who knows everything there is to know about proper ventilation. Ventilation is essential the movement of air within a system. The law tells us we must provide ventilation under the Healthy and Safety at Work Act, and building regulations set a minimum standard for ventilation. The main reason for good ventilation is to have a safe and comfortable environment; to remove odours, to control temperature and importantly to protect from harmful organisms and toxic substances. We have natural ventilation (like opening a window!), mechanical ventilation which pushes air around the building and a mixed mode – a combination of the two. The preferred method for ventilating a hospital remains natural ventilation, something which really shocked the group. It might work well on a windy day but it certainly doesn’t cover all areas and some times of year, like winter, it’s really no good at all.
Like Lou says, simple is best. When we talk about ventilation, we need to ask what is the issue we are looking at? Human elements are usually a key element to understanding problems in ventilation – you need to think about when the issue arose and who was involved? Often there is a significant time lag between the problem starting and it’s detection in real time. You can be left scrabbling around for details long after the issue began. Lou walked us through the potential information sources to considering during an outbreak, including design records. Which tend to be a little less useful than you would imagine, considering they often tell you the purpose the room was designed for 30 years ago – perhaps not so relevant now! Echoing the sentiments of Karren earlier, one of the most important things you can do is go physically and take a look – not an audit, just turn up and use all your senses!
To kick off the session after a much needed cup of tea (Earl Grey, hot!) we have Dr Mariyam Mirfenderesky who is talking about the challenges of managing fungal outbreaks. Candidozyma auris (note the new name!) is probably one of the most difficult outbreak causing organism to manage. To help with this a Clinical Expert Reference Group was established in March 2025. Candida species are the dominating fungal pathogens of invasive fungal disease and account for >85% of fungaemia in Europe and the United States. Candidozyma auris was first identified in 2009 from a Japanese patient with ear discharge, and is a critical WHO priority fungal pathogen. It is fluconazole resistant and has a propensity to cause healthcare associated infection outbreaks. There are 6 independent clades, with clade 1 dominating in England. Mariyam walked us through the identification of the first neonatal case of C.auris from an eye swab – it was found in two infants, five weeks apart with no direct contact between the children. Fortunately both were colonisation with the fungus only. She then discussed the safety measures that should be in place to manage this difficult pathogen – particularly focusing on why the current cleaning protocols are insufficient to manage this threat. Her final points considered how to act when you detect C.auris – you must be decisive and act!
If you’d like to know more about C. auris, check out this blog post from earlier this year:
Next we have Dr John Hartley who is talking to us about investigating environmental surface mediated outbreaks – what you can’t see may still hurt you. Using the classic movie ‘the fiend without a face’ as a metaphor for IPC, John introduced the idea of modes of transmission between individuals. It feels like a simple problem, its just cleaning and handwashing after all! But we see there is a complex person-organism-environment dynamic system, and as John says, there is always a well known solution to every human problem – neat, plausible and wrong! John highlights the importance of continual surveillance and knowing ‘where the fiend is’. The controls are based on a four pronged approach – clean, replace, destroy or rebuild.
By way of a case study, John told us about his experience of managing adenovirus outbreaks in a paediatric BMT ward. This is a very common virus causing 5-10% of febrile illness in early childhood. Almost everyone has had it, and it can establish latency which can reactivate during BMT. More often it causes severe morbidity and mortality in these patients who can develop hepatitis. What you can’t tell is if the child caught adenovirus from the environment or if it has reactivated post latency. However, whole genome sequencing (WGS) can resolve 1-3 SNPs across genomes – its not like looking for a needle in a haystack, its rather like looking for a needle in the whole of Texas. But WGS can be used to confirm or refute cross infection events.
Of course the next question is, what can be done? Visual assessment is not a reliable indicator of surface cleanliness, John described the varied methods which can be used to detect adenovirus. Then we need to develop the right tools to manage it – including development of environmental PCR as a measure of cleaning efficacy by GirlyMicro herself! Finishing on a Dr Who reference to delight a crowd of scientists is always a win – even if it is comparing adenovirus to the scariest episode, the weeping angels! Of course, when monitoring adenovirus, the most important advice is ‘Don’t Blink’.
To close the morning session we have Dr Sam Watkin discussing research tools to help predict the future of outbreaks. Sam began acknowledging the current challenges facing preventing transmission of environmental organisms. In his PhD he aimed to identify how microbes disseminate through the clinical space, if the starting contamination site determined how is was disseminated and if the usage of space influenced microbial transmission risk. IPC is often retrospective to the aim was to develop research tools to allow the development of prospective knowledge. Sam used cauliflower mosaic virus DNA markers as a surrogate for pathogens, and followed its movement around two different units. It was shocking to see how far this benign organism could spread in such a short time.
I think if we take away anything this morning it’s that nobody likes the new name for C.auris, and death, death to recirculating air conditioning units!
The morning was followed in the afternoon by a series of case discussions in order to help implement the learning from the morning, help everyone get to know each other, and support the sharing of peer to peer learning. The case discussions this year included:
Case discussion one (Facilitated by Dr John Hartley):
Seek and remove: approaches to source control for environmental surface mediated outbreaks
Case discussion two (Facilitated by Professor Elaine Cloutman-Green):
How to implement a multi-disciplinary approach to investigation of water borne outbreaks
Case discussion three (Facilitated by Louise Clarke):
Interpretation of ventilation data and applying it to ventilation risk assessments
Case discussion four (Facilitated by Dr Sam Watkin):
Determining the role of equipment in outbreaks: how do you investigate?
Case discussion five (Facilitated by Karren Staniforth):
Introducing new cleaning process: what should you consider?
Case discussion six (Facilitated by Dr Claire Walker):
Choosing new equipment and furnishings: what questions should you ask?
It was truly inspiring to hear the buzz in the room that all of the discussion created. Thank you to Mr Girlymicro (Jon Cloutman-Green) for being in charge of photography, and to all of our speakers and facilitators for making the day happen. Also, massive shout out to Ant De Souza for pulling the day together, Angela McGee for making sure we all turned up to the right place at the right time, Mummy Girlymicro for running the reception desk, and to Richard Axell for supporting all of the tech on the day.
Now it is all over, the only thing to do is to tap our feet until we all get to meet again in 2026, although the presentations and discussion sheets should go up some time during 2025. Until then however, if you want to know more either head to the Environment Network website to look at info from previous years, or read some of the other blog posts linked to environmental IPC down below.
I am not a big Halloween girly, to be honest I can take it or leave it because I’m mostly excited about the build up to Christmas. That said, what I do love are movies and TV, and despite never being someone who can tolerate a lot of slasher or gore based horror movies, I love a good vampire movie.
A lot of this may be because I enjoy the world building and lore that seems to be more integral to vampire movies and series. This is because, although they share some of the same rules, depending on how the world is built they always need to explain which of the nuance comes into play in that particular setting. It felt fun this Halloween therefore, to write a blog post that talks about some of those tropes when vampirism is linked to infection, and how those rules compare to the real world.
Common vampire tropes to be aware of and to bear in mind as you read on:
Experiencing pain or physical damage in relation to sunlight
Needing to consume blood as a protein source
Inability to eat or digest food other than blood
Avoidance of animals
Ability to influence humans to undertake acts that may be against their will
Violent reactions to garlic
Inability to see themselves in mirrors or via cameras
Death only by beheading
Death by wooden stakes
Damage linked to holy water
Aversion to signs of faith
Aversion to alcohol or drug use
Not all of these are present in every piece of world building, hence why I find the variety of vampire mythos so interesting. The choice of which ones go together combined with different origin stories and creation processes enable a pretty large tapestry to be created from some similar thematic components.
Mystical, infections or something else?
The place to start I guess is by discussing whether all vampire world building includes infectious transmission? And the answer is a definitive no. Sometimes the way that the creation of new vampires works isn’t discussed. Sometimes the rules about the underlying process is unclear. That said, the fear of becoming something new is a frequently used trope for dramatic purposes and so the process by which a human is turned into or by which vampires exist is discussed pretty frequently as part of world building, and from what I can see there are three main routes:
Mystical – some form of occult/magic/cause not routed in science
Genetic – vampires are born and exist as a stand alone species
Infection – transmission via blood or other infectious transfer, even if the agent is unclear or unspecified
Now, I’m not going to cover the mystical/magically as that’s not anything based in science and the science is what I’m here for. The other two, however, are often based (sometimes loosely) in science as they are often inspired by things that actually exist and so I’m going to talk about both of those in a bit more details.
Genetic
I’m going to kick off by talking all things genetics. There are an increasingly large number of vampire movies and TV series where the vampires that featured were born vampires. This includes movies like Abigail, Perfect Creatures, the finale of the Twilight series, but also TV series such as A Discovery of Witches, First Kill and Vampire Academy. Sometimes within these there are vampires that are made through other means (discussed below) in the same world. Often these genetic vampires exist as a separate species to their Homo sapien neighbours either openly or in hiding.
There is often much discussion about where the vampire myth comes from, and in many way these stories of genetic vampires who are birthed through a similar route to standard human deliveries, links in most with what is considered to be a real world inspiration for many vampire myths. The origin is thought to be linked to a rare inherited condition known as Porphyria, the presentation for which may account for for some of the common components of vampire portrayals.
Porphyria is a rare, inherited blood disorder that occurs when the body can’t convert porphyrins into haeme, a vital component of haemoglobin. The resulting symptoms vary depending on the type of porphyria. Acute porphyria presentations include symptoms such as gastro intestinal pain and symptoms like nausea and vomiting – symptoms that are often portrayed linked to vampires attempting to eat normal food. Whilst cutaneous porphyria symptoms include pain, burning and swelling in response to sunlight, skin fragility and a tendency towards skin blistering – all of which are frequently included as vampire responses to exposure to sunlight.
Porphyria D. Montgomery Bissell, M.D., Karl E. Anderson, M.D., and Herbert L. Bonkovsky, N Engl J Med 2017;377:862-872 VOL. 377 NO. 9
Interestingly, in some of the genetic origin vampire stories, the impact of some of the limitations of the lifestyle limitation of traditional vampires are not so extreme. In some of these cases they can be seen in daylight, although not for long and don’t enjoy it, and they may be able to tolerate some, if not all, of human food. They are possibly therefore most aligned to their real world inspirations. I could write pages and pages on this, but infection is where my heart lies so I’m going to crack on.
Virus, parasitic, others?
Now we’ve covered off those born vampires, let’s move onto the most common version of vampirism outside of the traditional Dracula more mystical inspiration, that is vampires who are created linked to transfer of infection by blood or other means.
There are three main ways that this commonly comes into play:
Viral causes
Parasitic routes
Bacteria intoxication
I’m still trying to find a vampire movie where the main infectious agent is fungal, but it seems that most of the movies based on fungi are linked to zombie outbreaks. That makes a lot of sense, due to the fact that fungi are eukaryotes (like us) rather than prokaryotes (like bacteria), and so fungi tend to be linked to changing behaviour linked to interfering with the human nervous system. If you’ve seen a vampire version though please do let me know as I’m collating a list of where different organisms might come into play.
By far the most common route depicted is where the causative agent is a virus. Viruses are featured in movies such as Blade and Daybreakers and TV series such as Ultraviolet. This is because viral transmission in general is associated with transfer of bodily fluids, be that faecal-oral, respiratory via saliva, bodily fluids such as breast milk, or in the case of vampire movies via blood.
The most uncommon causative agent I’ve discovered is the parasitic cause of vampirism as shown in The Strain TV series. During the series transmission of the virus to create a full vampire is via something known as ‘The White’ that contains parasitic worms. These then lead to anatomical changes, including the growth of a proboscis that enables the biting and transmission of the parasite to others.
Bacterial coverage is mostly linked to potential methods of intoxication that supports the control over humans by vampires. Rather than being a direct cause of the vampirism, this seems to be about how transfer of the bacteria releases, or causes anatomical change, which then changes behaviour via things like hormonal or neurological changes. I’ve talked before about why bacteria may feature less in horror movies than other causes, but this can mostly be summed up by the fact that audiences tend to know more about bacteria and therefore it is less tempting for writers, but also horror tends to sit better in ‘the possible but not too close to us’.
Transmission
Obviously it’s not just the infectious agent that is important, but the mode of transmission for that agent. This being all about vampires the biggest mode of transmission is by bite, but it’s not always so straight forward. In mystical vampire movies, there’s usually a whole lot of removing of the original human blood and then transfer of the vampire blood, leading to a mystical baptism and rebirth. Infectious causes are much more one way, any bite could lead to someone turning into a vampire and the most important thing is load related. If someone is in contact for longer, if more blood is drunk and therefore more saliva and fluids exchanged, then the chances of conversion are much higher.
It’s not just blood as a bodily fluid that features in conversion during vampire movies. There are also films, such as Requiem for a Vampire and Trouble Every Day, where vampirism is treated more like a sexually transmitted disease, rather than transfer occurring during feeding on the blood of their victims. It seems that these films have increased since the 1980s, maybe as a result of fear processing linked to the HIV/AIDS pandemic during that time period or maybe because our knowledge about and ability to detect infections has increased and therefore there are a larger part of the collective public awareness. It will be interesting to see how the SAR CoV2 pandemic will impact this further.
The most unusual transmission, and one that aligns most highly with blood borne transmission is the presence of congenital transmission as featured in Blade. Where the main character Blade becomes a vampire hybrid by acquiring the vampire virus at birth, due to his mother being bitten and placental crossing of the virus into his blood stream. As a result, he exhibits some of the characteristics of a vampire due to the virus, but the effects are attenuated linked to his exposure route. It can often be that congenital infection presents differently to primary infection via other causes, and it appears vampirism is no different.
The other variable is linked to the time to turning once the infection has been introduced. I would speculate that this too is load related, as well as the infectious agent behind the symptoms. Viruses, for instance, are likely to reproduce and induce change at a much higher rate than anything linked to bacteria or parasites. This is partly due to their reproductive rate, but also linked to the level of dose that tends to be available. The exception to viruses resulting in the fastest change is likely to be bacterial intoxication and influencing. As the toxin acts immediately, when this is present in media and TV the change is almost instantaneous, but also time limited and therefore requires top up or re-application. Not all impacts are until beheading, some require a more time boundaried set of interventions.
Interventions
Once your characters are aware that vampires exist within their mist, then they will want to look for actions in order to protect themselves. One of the classic ones as featured in many movies, including the classic Lost Boys, is garlic.
In some ways the impact of garlic makes even more sense if you think of vampirism through an infectious transmission route, as garlic has been considered to have anti-infective properties for a long time, although warning you may have to ingest a LOT of it!
Another common feature in vampire movies is the roles that animals play as protectors. For instance, in 30 Days of Night, the vampires kill all of the dogs before they launch their main attack. This kind of thing also often happens in films and TV where vampires are hiding in plain sight. It could be that they are taking out animals as they don’t want to be found, and animals are easier than humans, but I have another proposition. There are a number of infections where animals can be used to sniff out and identify infected individuals. Therefore, if animals could detect vampires they are much more likely to be a risk and warrant removal. Animals could therefore act as a front line of diagnostic defence to enable you to tell friend from foe.
Having determine that a common weakness of vampires is their damage response to ultraviolet light (UV), films such as Underworld weaponise light against the vampire protagonists. Light, and especially UV-C (200 – 280nm), has been known to impact viruses and bacteria for well over 100 years. When light is in this frequency is can damage both RNA and DNA, resulting in cell death, and it is possible that if the infectious agent is the only thing that is keeping your body moving the damage would be more pronounced. We’ve also discussed how the lack of some biochemical pathways can lead to UV-C causing much larger amounts of pain an damage.
Normally, penetration of the light to cause damage might be an issue, but if you are using bullets or other means this may not impact. The most important thing I have to say here is, that despite what is shown in Blade 2, light does not bend around corners. This is also important for when you are considering using UV-C in hospitals to support cleaning, it doesn’t have good penetration and doesn’t go around corners of work in shadows. Using UV-C may work against your vampires but you are going to need to think carefully about where you use it so it does what you think it can.
Vampire movies have amazing world building and are often my favourite genera in terms of their string internal logic. I love the fact that so many types of infection and route of transmission that reflect real world cases are present as part of these pieces of entertainment. They can actually teach us a lot, even when we don’t realise it, and so much of it has origins in real world knowledge, even if only loosely. So, this Halloween evening find one you haven’t seen before and let me know which intervention you would use to stop your town being turned into creatures of the night!
Before I go, I thought I would share a few of the previous years Halloween blog posts in case you are looking for some more spooky season and infection reading:
This week marks the 5th anniversary of regular posting on Girlymicrobiologist.com. I can’t believe that time has flown by so quickly. I also can’t believe that something that started out with such small expectations has grown to play such an important part in my life, and in my sense of identity. This was all really cemented for me in something that also happened this week, the publication of my first ever book.
Now, it’s been no secret that I have been putting some time aside to try and write something for the last few months. You have all been very patient with me whilst I posted a little less frequently, and I cannot help but give a massive thank you shout out to Dr Claire Walker who has curated some wonderful guest blogs in order to keep the content flowing. It’s a world of different having an idea and starting to write it, to holding the real thing in your hand, and so my brain is still catching up to the reality. I plan to write a bit more of a step by step guide to what the experience has taught me about self publishing, and why I thought self publishing was the right choice for this particular book, but for today I wanted to focus on moving something from a vague wish to a reality you can hold in your hand.
So how did I get here?
Back in 2022 I wrote a post about the fact that I was playing with the idea of writing a book, although I wasn’t quite sure about the direction that book would take, and listing a number of steps:
Further formulate the concept i.e. what kind of book? I actually have 2 ideas. One is turning this blog into a book format. The second is that I also have an outline structure for a Pathology murder mystery. I’m excited by both, but right now I think option 1 is more achievable with my current resources
Review what I already have. If I go for a non fiction book I need to undertake a gap analysis of what I have, what can be modified and what new content is needed. For the fiction version I need to start getting my concepts down so that I know how viable they are
What good resources are available to me? This is an ambition of plenty of people and there is a wealth of information out there. I need to explore, quality assess and curate what there is so I don’t waste time and energy making unforced errors. There is no point in reinventing the wheel, modify it so it works for me, but let’s not start from square one.
Undertake some appreciative enquiry. Success is often about asking the right questions and making the right connections in order to increase your odds. I have some friends in this field but not in the area I’m thinking of working in. I need to be brave and put myself out there to gain insight into the ‘Known Unknowns’
Use the knowledge and information gained to put together a project plan. Establish some small steps that can make the project as a whole less overwhelming
Establish my success criteria. What does success look like? For right now it’s the process of creating that will feel like a success with a stretch goal of sharing what is produced, but that might change based on what I discover
Research your audience. If I decided to include sharing what is produced as part of my success criteria who would like to see such a book? If I were to share the content what would that look like and what would be needed?
You’ll notice that those early steps involved a lot of information gathering, and reflection before formulating a plan. Writing that blog post encouraged me to do just that, but more than that it meant that I had made a declaration to all of you and started talking about what the next steps would look like, so I could be held to account by others as well as myself.
One of the things that my research led me to understand with greater clarity, is that to get from where I was to publishing a book required both the formulation of a plan, but also the development and practicing of skills. To a certain extent, the project plan was the easy bit, as long as my research was effective. The skill development piece was harder. It seemed to me, that the best way to go about this was to support others by being involved with their work in order to learn and develop more.
This led to me being involved with everything from textbooks, to a book on the impact of waste on our society. Every encounter taught me something. Every encounter helped me to refine what I was interested in and how I was interested in working. It also supported me in developing an author page so that I had a place where I could sign post others to the work.
Fairly early on I realised that I didn’t have the time or bandwidth to develop my pathology murder mysteries right now, although I am still drafting plot on the side. The writing style is just too different for me to be able to dip in and out of , and I need to put in many hours of practice to get that style to a point where it would be acceptable.
That left me with content linked to this blog. Many of you will know that I started drafting, and am still working on a book called White Coat Syndrome (or similar). This is still in the works but a wise friend suggested that I keep working on getting it traditionally published, so I need to give it some focussed time. That left me with looking at the content I already have for trying out what the self publishing process could look like. Over 90% of non-fiction books are self published these days, and of the ones that are traditionally published still, most are linked to people in the public eye or with social media followers in the millions. It will be a surprise to no one that I do not fall into either of those categories, and so exploring the process of self publishing felt like the right move, not just for this book but to understand more moving forward.
So why this topic? In a moment of frustration about life, the universe, and everything, I was having a late evening rant and Mr Girlymicro and he said ‘Why don’t you write a book on how to do a PhD? You talk about it all the time. You spend lots of time supporting others through it, and you have already written thousands of words on your blog linked to it’. I just looked at him, went to bed, and woke up with a 40 chapter book outline. It just felt right. Something in my brain just clicked, and so the writing in the end was the easy part. After all, Mr Girlymicro is pretty much always right, and yet again he proved it.
Once the topic and method of publishing was chosen, then all that was left was pulling it together. It was so important for me that this book came from a place of authenticity, a place where I don’t pretend that things are easy, perfect or even equitable. In fact, it was that sense of inequity as I was writing that became a real motivator for finishing the book. As I reflected and wrote I became increasingly aware of how inequitable access to PhD programmes have become. How the way access routes are set up to be even more challenging if you have health or caring needs, but also if you don’t have access to someone who has done one to advise you on how to apply and what factors might be significant to talk about.
The next factor was to to decide on a time scale. Now, this part might be a little piece of madness but I know how busy IPC gets once we hit winter, and so allowing a 4 month time frame in order to get the book out before winter pressures and to align the release with the start of the academic year seemed like a good idea. I’m not saying that it was a good idea…just that it felt like one at the time. I think tasks take up the time that is allowed to them, however. I think if I’d allowed a year it would have spread to take that much time. It is sometimes better to set a tight timescale and stick to it, rather than allowing a window which could extend the project for longer than is really needed.
I also gradually became aware that providing some practical exercises would add value in a way that I could not include in a book format, and so decided early on that several of the chapters would have these hosted on the Girlymicro website so they would be free to access and download. Providing a holistic, interactive approach was key to my thinking, as was making sure that at its heart the book is about community and supporting each other, the same as this blog. I didn’t want to pretend to be someone else, or write in a way that was more academic, as I think there are enough of those styles of books out there. I wanted this book to support everyone to bring their whole selves to their PhD and their topic, and so it was important to me to write in a way that I also did the same.
Now the book is ready. Now that it is a real thing that I can hold in my hand. There are two main tasks taking up my thinking. The first is trying to work out how to get it to people that it might help, something that I would be grateful for any advice that you can give to me. The second is about how I can help others by sharing the knowledge I’ve picked up myself as part of going through the writing and self publishing process, to make it easier for others to get their voice out there. There are benefits to both ways of publishing, but there is something empowering about being able to feel like you can speak directly to your readers by maintaining more control over the content, rather than it being seen through a commercial lens. I’m not in this for the money after all.
There is still one thing that I talked about on my list of steps, way back when, and haven’t yet addressed, and that was success criteria and decided how to benchmark what success looks like. As I’ve said, I’m not doing this to make money, I’m doing this in the hope that it might assist others, and so for me it has never been about a commercial approach. I still need some way of judging progress however. On doing some reading I discovered that many books never sell more than 20 copies, and most others don’t sell more than 250 copies in their first year. My aspirations are pretty small therefore, as this is something I’m just beginning. I would consider the book a success if I sold more than 20 copies. I would be over the moon if I sold anywhere between 50 and 100 copies in the first year. The topic is fairly niche after all. Mostly I just want to mark the event and use it as my own benchmark for improving during future projects. We all have to start somewhere.
If however, you’d like to add to those 20 I’ve included the link for purchasing below:
Thinking about what’s next
Like everything is life, my first thought when I finish something is to think…what’s next? I have learnt so much and my plan is to take a little time to reflect on that learning and to enjoy focussing on blog writing for a while. That said, I am now going to return some of my focus to the book pitch for the Girlymicro general book, and I do have to admit I have the title of my next book in mind if I decide to try another self publishing exercise. Mostly I would like a few weekends off as it’s been a while since I could embrace the sofa and fully rot for a weekend. So while I cogitate, I intend to treat myself with some truly awful reality TV, and spending quality time with mummy and Mr Girlymicro.
Taking a moment to enjoy, celebrate, and mark the occasion
Before I slob off to the sofa though…you all know that I am a strong believer in celebrating and marking the moments that impact our lives, and this book is no different. To mark the moment I’m a having a small, low key book launch on Friday 17th October and there are just a couple of free tickets still available if you’d like to join.
Whether you can make it or not, I’d love to hear what you think as I’m all about improvement and learning. If you do get the book it would also be amazing if you could leave a review on Amazon with your honest thoughts. Apparently reviews really help increase visibility, whether good or bad, and so it would be wonderful to think that this book is finding its way to those who would need it.
I want to sign off with a thank you. I would never have gone through the process of thinking about writing a book if it wasn’t for all your support. I wouldn’t have had the content or undertaken the self reflection needed to know what to write if you hadn’t kept reading this blog. Finally, I wouldn’t have had the motivation to get through writing it and working out so very many templates and decisions if I didn’t know you would support me in the effort. So thank you. I appreciate every read, every interaction, and every conversation we have.
For my birthday in 2014, I celebrated by submitted by PhD thesis for printing. I ripped off the band aid and committed.
For this birthday, 11 years later, I’m taking another leap of faith, and once more rolling the dice on myself. This time it’s still PhD related, but rather different. This time it’s to let you all know that I have written a book, which will hopefully go live on Amazon on Friday the 17th October.
It feels like birthday launches could become a tradition.
I’ve been talking about a super secret project for a while now, and the wonderful Dr Claire Walker has been taking on some heavy lifting in terms of arranging some guest blogs, so that I could write a book on my weekends rather than writing a blog. But what is the book, and why did it come about?
The Book
The book is entitled ‘It Shouldn’t Happen to a PhD Student: How to thrive, not just survive, during your PhD’. It has 40 chapters that take you all the way through from deciding you want to do to PhD, and thinking about where and what type, to submitting your thesis, and what kind of skills you may need to develop during your PhD to maximise your career success after it is done.
Professor Elaine Cloutman-Green, otherwise known as “The Girlymicrobiologist”, is a clinical academic with over 2 decades of experience leading research projects and supporting students at all levels, including PhDs. She also runs the popular Girlymicrobiologist blog, which aims to de-mystify science and support those wanting to engage with academic careers from A-level all the way through to career enrichment.
In this book, Girlymicro talks about the reality of what it is like to study for a PhD, what gateways you may need to pass through, and how to manage key relationships in order to achieve success.
This book starts at the very beginning, with why you might want to do a PhD, how you might decide what route to PhD is right for you, and what a successful application might look like.
It then takes you through your PhD journey, year by year, with tips about how to approach and succeed during significant moments, such as attending your first conference, or writing your first academic paper.
Finally, you will discover what other skills you need to develop during your PhD to give you the best route to success after your viva. All of this supported by links to activities on the Girlymicrobiologist blog, to help you with practical exercises in order to apply what you have learned.
Whether you’re planning your PhD, a healthcare professional looking to develop, or simply curious to know about how the world of academia works, The Girlymicrobiologist offers a refreshing blend of knowledge and relatable experiences. Get ready to laugh, learn, and be inspired to find a way into, what she describes as the best job on the planet.
This is the book I wish that someone had given me when I started on my PhD. I was pretty clueless and spent a lot of time finding my way, and making heaps of mistakes. It seemed only fair to write all of my learning down so that I can share it, not just with my own students but more widely, so that everyone is free to make their own new mistakes, not just repeat ones I’ve already made.
The Why
I’ve been talking about writing a book for ages, and I still have the original Girlymicro book I’d planned going on in the background. I was prompted to do this book now though, after spending an afternoon at an awards event and realising that I could tell you every person who was going to win in every category before the dinner even started. It made me think a lot about access and privilege. That night I came home and I was really glum, and I couldn’t quite process why I was feeling that way.
I slept on it and spent some time speaking to Mr Girlymicro the next day to process my thoughts. I talked about how much access to healthcare professions and even academic training schemes are now based on who you know, to describe the best way to get through gateways like applications and interviews. How, even once you are in them, to feel like you understand how things work and the undisclosed boxes that need ticking, you need to have someone who will let you in and tell you the unwritten rules, and frankly not all supervisors see that as their role. This means that I really feel like we are missing out on some amazing talent. People who would make wonderful PhD students, or academics, because they can’t get across the threshold or see themselves in the role.
Not everyone has strong connections with a university. Still fewer people know someone who has a PhD. The way the system currently feels is that if you can access information you really have such an advantage over those that don’t. I therefore see a lot of my medical colleagues getting access to PhD funding, and yet fewer and fewer of my nursing and scientific colleagues. I increasingly encounter more and more undergraduates who are reaching out because they need help to know why they aren’t being successful, because they don’t know what is expected of them. It has always been hard to get onto PhD programmes, and it should be. What it shouldn’t be is hard because you don’t have access to the right people to give you the knowledge you need to level the playing field.
I realised that was why I was feeling upset and unsettled. I don’t like unfairness. I don’t like inequity. I don’t like realising that I’m part of the problem. Mr Girlymicro commented, as I was off loading, that I had plenty of blog posts that talk about how to apply for and do a PhD, and so why didn’t I take the way I was feeling and turn it into something positive. A book. So, this book concept was born. A book where I set out to play my role in fixing the disparities as I see them.
The Vision
That conversation happened right at the end of May. I gave myself 3 months to take some content form this blog, as well as creating new content, to come up with a book of ~80,000 words that captures the advice I give to my PhD students, and those approaching me floating the concept of applying for a PhD.
Why 3 months? Well, if I allowed myself a year, I would take a year, and remember that other book? I still want that to happen at some point. The other thing was that I wanted it finished as close to the start of the academic year as possible, so that it could start benefiting people right away. We all also know that I have no patience, and so using my birthday as a cut off always felt right.
The book was finished at the end of August, and I’m in final edits before upload at the end of the month. I want it to be the kind of resource that people can dip in and out of, whether they are doing a PhD or not. Chapters, such as developing goals, or on public speaking, should stand alone to benefit even those who are not in academic study. The activities that can be accessed alongside the book, to help things like developing your elevator pitch, should only grow in number over time, and hopefully will be a good general resource for anyone that finds them, not just for those who are studying for a PhD.
My main hope however, is that people who are on a PhD will find it not only helpful, but something that will help them feel a little less alone in the process. There were times, as I was doing my PhD outside of a standard academic department, that I felt really lonely, and sometimes even very lost. Not everyone has a super supportive supervisor, not everyone finds those peers that keep you going. I was lucky that I had great colleagues who picked me, not everyone has that. I hope that this book can act a little like the friend you need, who you can turn to for advice, and to know that others have been there before and found a way to succeed.
What to Expect
I don’t know what to expect to be honest. I’ve never written a book entirely alone before, with thanks to Dr Helen Rickard and Dr Sam Watkin who have contributed text. I know why I needed to write this book, and as I say in the first chapter, knowing your why is the most important thing. I don’t expect it to be perfect, nothing is, but as I say to my students, the main thing is that it is done.
The book should go live on Amazon (depending on their turn around time) on Friday 17th October. It should be purchasable in 3 forms:
Ebook for £2.99 or included in your ebook subscription if you have one and free to download
Paperback for £9.99
Hardback for £15.99
None of this is about making money for me, but Amazon have minimum costs, especially if you want it to be available widely, so there we go.
To mark the occasion, although it is terrifying me at the moment, I’m holding a small book launch event at UCL on the same night. If you fancy, come and join me. After all, we should all do a little something that scares us, and I’m hoping if I feed you wine you will forgive any deficiencies knowing the reasons why this book came into being in the first place.
If you like, I’m kinda hoping you might also tell your friends…
I am currently in the middle of secret project, which I hope to announce more about in late August/early September. I’m really excited about it but it’s taking a bunch of my time. I’m hoping that you will be just as excited when I can share more details. The wonderful Dr Claire Walker is helping me deliver my passion project by curating the Girlymicrobiologist blog for a few weeks. This means that I hope you all enjoy getting some great guest blogs from a range of topics. Girlymicrobiologist is a community, and all of the wonderful authors stepping up, sharing their thoughts and projects, to support me in mine means the world. I hope you enjoy this guest blog series. Drop me a line if you too would be interested in joining this community by writing a guest blog.
Dr Walker is a paid up member of the Dream Team since 2013, token immunologist and occasional defector from the Immunology Mafia. Registered Clinical Scientist in Immunology with a background in genetics (PhD), microbiology and immunology (MSc), biological sciences (mBiolSci), education (PgCert) and indecisiveness (everything else). Now a Senior Lecturer in Immunology at University of Lincoln. She has previously written many great guest blogs for the Girlymicrobiologist, including Simulating Success – Enhancing Biomedical Science Education through Clinical Simulation. This blog was written by a group of her final year students on their experiences of trying to teach differently.
Blog by Yvana, Nicole and Ellie
We were a small group of three final-year Biomedical students—Yvana, Nicole, and Ellie who were brought together by a shared goal to create something useful for other students by us students. In our final year at the University of Lincoln, we were offered the opportunity to work on a collaborative project focused on improving on how ELISA (enzyme-linked immunosorbent assay) is taught to students- a commonly used technique in the immunology department to quantify and detect biological molecules.
Meet the Team
Yvana
Hello, I’m Yvana – Three years ago, I began my journey as a Biomedical Science student at the University of Lincoln. Like many, I was unsure of the exact career path I wanted to follow, but I knew one thing for certain, I was deeply fascinated by diagnostics and disease. Over time, that interest developed into a love for laboratory work, especially when I had the opportunity to experience clinical simulation sessions led by Dr Claire Walker which stood out to me as they offered a taste of what a real-life clinical lab feels like beyond university.
One of the highlights of my third year was engaging in a unique series of laboratory-based activities known as Laboratory Skills, coordinated by Dr Andy Gilbert. These sessions were designed to strengthen our core technical abilities and confidence in the lab through a series of activities covering microbiology to biochemistry!. After completing 6 weeks of lab skills, Dr Andy Gilbert approached me with an exciting opportunity to collaborate with two other students, Nicole and Elle, also led by Dr Claire Walker on a co-creation lab skills project. Our task? To design a step-by-step resource that would deconstruct one of the most widely used techniques in immunology, ELISA – making it easier for students to understand and perform.
Ellie
Hi everyone, my name’s Ellie! I’m 1/3 of the amazing group that have carried out the ELISA workshop, led by students, for students. During my years at the University of Lincoln, I’ve grown to love the fascinating world of microbiology and I’m even going back this September to do a Microbiology Masters! I have really enjoyed my time at Lincoln and part of that is thanks to Andy Gilbert for putting on his extra lab skills sessions, which allowed me and other students to gain that vital extra laboratory knowledge and practice important techniques.
I’ve just finished the final year of my undergraduate Biomedical Science degree and throughout this year I was able to create something incredible. I, Yvana and Nicole, were given the opportunity to collaborate and develop a practical booklet as a building point of the skills needed to carry out an ELISA. The main reason I agreed to take part in this task is that we, as students, do not get many chances to have such a hands-on experience with many complex techniques, like an ELISA, during this degree. Because of this amazing opportunity, we were able to give students across all years at Lincoln the chance to gain more knowledge and extra practice in learning this crucial technique!
Nicole
Hi, I’m Nicole – one of the final-year Biomedical Science students behind this project. Starting at the University of Lincoln, I wasn’t entirely sure which direction I wanted to take within biomedical science. As the course progressed, I enjoyed the hands-on lab work, particularly how it transformed theoretical knowledge into practical application. This became evident in my second year during Laboratory Skills sessions led by Dr. Andy Gilbert. These weekly sessions focused on core techniques like centrifugation, microscopy, and microbiology.
Co-creating the ELISA workshop booklet felt like more than just a project; it was an opportunity to make lab-based learning more accessible and less intimidating. Since ELISA is a technique, we limited experience with as students, developing this protocol felt was crucial. Working with Ellie and Yvana to bring our ideas together was fulfilling. My favourite part was seeing the complete protocol, knowing it would support students to tackle the ELISA confidentially.
Figure depicting how ELISA works step-by-step
Building the booklet
This project was a collaborative effort and not something we did alone- we brought our own strengths together to create the now called ELISA Team (given by Claire Walker herself!). We spent countless hours in the lab, testing and refining each activity to make sure it worked as intended and delivered the essential skills students would need to confidently complete an ELISA in real time. We held regular meetings, worked on it during lectures (sorry Claire and Andy!), and genuinely had a lot of fun creating something meaningful that we hope will support future students just like us.
Under the guidance of Dr Claire Walker and Dr Andy Gilbert, we set out to create a resource that would feel practical, and genuinely useful for students. We didn’t want a booklet created from a lecturer’s perspective of what students might find helpful. We wanted to build something we would have found helpful when we first encountered ELISA, a step-by-step walkthrough from a student’s perspective.
Overview of ELISA (Enzyme-Linked Immunosorbent Assay) booklet use to educate students
The booklet breaks down ELISA into its fundamental components, from how to properly use a multichannel pipette (which was a nightmare to handle!) to interpreting results and avoiding common mistakes students might fall for. For instance, one key focus was on the washing stages, an often-overlooked step that if done incorrectly, can lead to high background noise and inaccurate results, which in a diagnostic lab can be the difference between a patient receiving an accurate diagnosis or potentially missing one altogether.
What made this project especially rewarding was the opportunity to run our session with real students from first year undergraduates in Biomedical Science to postgraduates in Biotechnology. The feedback we received was overwhelmingly positive. Many said the booklet helped them better understand ELISA both in theory and in practice. We focused heavily on visual learning using diagrams, photos, and annotated guides because we knew from our own experience that clarity and visual support were essential when learning complex lab techniques.
Initial plate setup demonstrating serial dilutions and pipette accuracy during the first activity, comparing multichannel versus single-channel pipetting.
Our final thoughts
Our co-creation project not only gave us a chance to give back to the large community of students, but we were able to bridge a gap that many lectures hadn’t quite managed before, true co-creation between students and lecturers. Together, we created something that students appreciated and benefited from which was entirely made by their peers through mutual experience.
Looking back, we are incredibly proud of what we achieved as a team. It showed us how impactful student-led projects can be when they’re supported by passionate educators and built around supporting the educational needs of the community.
Today, I’m at the Advancing Healthcare Awards, as I’ve been shortlisted for an award from the Academy of Healthcare Science. It’s so lovely to be considered, especially as this nomination was linked to this blog, and it’s the first time I’ve ever been considered for something linked to Girlymicro. That obviously means an awful lot. In all honesty I’m highly unlikely to win, and that is nothing to do with modesty. If you don’t know the other people listed below, they are all pretty epic, and I think are much more aligned with the judging category.
The thing is for me, it’s not about the winning, it’s about sharing in the success of others, and that’s what I’m really looking forward to. Now, you may roll your eyes at me, and say that I am just saying that as everyone wants to win. I acknowledge that I won’t refuse the award if offered, but I can genuinely say that I’m OK to be the person that cheers loudly for others. I’m lucky enough to have won a number of awards in my time, and I’m even more fortunate to have been considered for many more.
At the start, I really did think it was about the winning, but over the years my appreciation of just being in the room has grown. Now, I consider the fact that someone has given their precious time to nominate me the real win. Time is the thing that no one has a lot of, and for someone to use it on something for me means the absolute world. This isn’t just true for awards, however, my point of view and how I celebrate has changed for most things, from grant writing and papers, to goals in my personal life. Doing my PhD, and writing my PhD thesis, really caused me to actively think about what works for me. So, I thought on a day like today I would share my thinking in case it helps others.
What success looks like feels different at different times
As I’ve said above, I haven’t always had the same attitude to marking progress and success as I have now. I think undertaking a PhD, and trying to make my way as a clinical academic, where so much of what happens results in failure, really caused me to actively think about how I maintained my motivation and marked progress. This is especially true for long terms goals, including those career milestones which occur over years rather than months, and where there are likely to be a lot of peaks and troughs along the way.
It’s important to also know that success feels different at different moments in life. There have certainly been times in recent years where the successes I’ve marked have not been about the big things. They haven’t been about winning large amounts of grant funding or awards. My successes have been about getting through the week, and to be honest, sometimes they have been about getting through the day. The pandemic hit me hard and I think I’m still in recovery mode. At these times, for me, it’s about finding and celebrating the small wins and setting myself small targets, in order to feel like I’m still moving forward.
If you only celebrate the successes you miss out
I wish I’d learn to change my attitude to success earlier. I feel like, in hindsight, I missed out on enjoying some of the journey of my career by being so target focused, and only appreciated the big mile stones. I’ve always been the same though. When I was at uni or doing my A-levels, I was so focused on getting through the exams, I never had the energy to go out and celebrate afterwards with everyone else. I would just go home and crash out. Making the shift to celebrating the steps along the way has made such a change to my perfectionism by making me appreciate the building blocks it takes to achieve. I also think it has made me a better mentor, supervisor and leader, as I now encourage others to do the same. Don’t just celebrate when you get a paper accepted. Celebrate when you have finished writing it and you are ready to submit. Celebrate getting a first draft of your thesis written, not just the day that you pass. Celebrate completing a section of your training portfolio, not just the day you get the completion certificate. Celebrate the fact that you have done the work, shown up and made the effort. Not just the outcome, about which you may have little control.
Acknowledge the work done
There are days when you will not achieve. That is just the reality. There will be days when you stare at the screen and manage to eek out 300 words, rather than finding your rhythm and getting down 2000 plus. To try to persuade yourself otherwise will just set you up for failure. It’s important to work out where the benchmark for celebration is, and also to match the reward to the benchmark. For me, some days that’s rewarding myself with a bubble bath if I finish a blog post early enough to make the time. Some days, it’s saying if I can make it through the next 30 minutes of meetings I’ll reward myself with a biscuit and a cup of tea. Other days, it will be that I can buy myself the dress I want if I can get back to running a continuous 5K. Not everything is worthy of a reward, in my world, I still have to set and meet a target. It’s just that target gets flexed these days based on the reality I find myself in. I still have to do the work, there is no free pass.
Marking progress in any form is worthwhile
The reason I now adjust my benchmarks is that I’ve learnt the value of movement, and not being paralysed by the size of the task ahead or the pressure I’ve placed upon myself. If you only celebrate the big moments, the end points, then in the times in-between it can be easy to feel like this movement doesn’t exist, as it’s harder to realise the progress you are making. This could just be me, but there is so much value to psychologically feeling like you have momentum. That even if the way up the hill is slow and painful, you are still getting closer to the summit. There’s a figure banded around that only 20% of grant submissions are successful. Most of the essays that get submitted will not get A’s, and for every successful interview candidate there will be multiple people that don’t get the job. If you don’t acknowledge and notice the progress it is easy to get overwhelmed by the failures. So mark progress where it happens so that you don’t just see the ‘no’s’.
There is always value in feeling seen
I’ve written before about all the reasons I think it is important to nominate others for awards. A lot of the reasons why you should nominate for awards also hold true for putting people forward for other opportunities, such as membership of committees, or inclusion on grants and papers. It can feel very lonely when you are carving out a path for yourself, especially if you are not following a well trodden path. Nominating and putting others forward can help them feel recognised, but the same is also true for you. Opening ourselves up to risk of failure, of not being chosen, or receiving feedback that may not be glowing can be hard. The thing is, this is how you build networks and get seen. This is how your name gets known. You may not get that opportunity, but it may be that the panel remember you for a future one where you may be more suited. This one comes back to celebrating the things that are in your power to control. You have control over the submission, over the putting yourself out there. You don’t have control over how your attempt lands (other than making sure you put in the work), or who you are competing against. So the success to celebrate here is the courage it took to take a chance, and step out of your comfort zone. Celebrate rolling the dice on yourself.
Feedback can be the greatest gift
I’ve received some pretty hard core feedback in my time, everything from ‘you contribute negligibly to infection prevention and control’ to ‘there does not appear to be anything that demonstrates this applicant has anything exceptional or above average for their future career trajectory’. I’ve had documents returned covered in red, comments about the fact that I can’t write, and grant rejections where I’m pretty sure they didn’t even open the form, despite the fact I’d sacrificed 6 months of my life to complete it. Needless to say, it is these comments I remember rather than any of the ones that said anything positive or nice about my submissions.
Now, I’m not saying that I celebrate the harsh ones right away, I permit myself a period of processing. This period of processing is easier and shorter if I’ve allowed myself to celebrate the work it took to get the submission in. After this period of processing/mourning, however, I make an active choice to go through and find the learning. I find the commentary that is based in fact, no matter how uncomfortable. The commentary that is actionable, and I reflect on how to make the change/improvement. I try to learn how to be better for next time. I then celebrate my engagement with the process. It may not be a party. It may be a ‘thank god that’s done’ drink, but I mark it. I mark the learning and I mark the fact that I had the courage to do the work that was hard/unpleasant. Celebration shouldn’t just be about joy. For me, it’s about acknowledgement of significant moments, and that includes failure as long as there’s learning.
Any journey worth taking is filled with moments of tantalising closeness
Traditionally, success is often seen as moving from point A to point B. In reality, in my experience, success is more like a series of concentric circles where improvement is cumulative, and often based on iterative improvement. Therefore any journey actually has a lot of near misses with success before success actually occurs. It’s actually important to notice when these near misses occur, rather than just discounting them as failures. These near misses represent huge steps of progress in themselves, and therefore deserve to be acknowledge as an important part of the journey. Not least because, by celebrating them, it can make it easier to take on and include the learning they provide, rather than discounting them as just another failure. The lens through which we see these moments can have a direct impact on how quickly we move from near miss to direct strike. Attitude is everything, and so make sure you embrace these as the opportunities they really are.
Sometimes the moments between successes can be protracted
There are things in life and professional practice that are the work of years, rather than weeks or months. Even if a project is over months, there can be moments when it is hard going. Writing a big report can feel soul destroying when you are on draft 54 and everyone has given conflicting feedback. Undertaking a professional portfolio can just be draining when you can’t get anyone to give you the time needed to sign off competencies or review sections. Then there are things like a PhD which run over years and are comprised of numerous stages, all of which are likely to rely on other people at various points, or to practice skills you are only just learning. All of this means the time from commencement to completion can be long, causing relying on internal motivation alone to be pretty hard going. By acknowledging that these bigger pieces of work are comprised of segments, and celebrating completion of these parts instead, can enable you to visualise progress made as well as to celebrate the learning gained along the way. It can also help you to regain momentum when you lose it.
The real learning occurs long before the end point
Talking about celebrating learning, this is an important point for me. It’s taken me a while to really stop and reflect on what ‘success’ really means. For a long time if you’d asked me I would have said it was the completion of something, but I’m not sure I would any more. The certificate at the end, or the gateway is symbolic of that completion, but for me now it’s more symbolic of the learning and change that occurred within me as part of the process. It’s the hard won changes, in either knowledge or outlook, that have been gained that are the real marker of change linked to the activity. This learning happens as you are involved in the process, and there is normally a fairly steep learning curve at the start. It therefore makes less and less sense to me to just celebrate at the end. Celebrating during the toughest moments, where the maximum learning is being gained, no matter where along the process that occurs, now makes the most sense. For me, success is getting to the point where I feel I do something better than I did before, be that decision making, leadership, or a practical skill, and so I celebrate when these breakthroughs occur, rather than relying entirely on an external evaluation of my progress.
Share the moments
This photo was taken at another Advancing Healthcare Awards lunch, many years ago. You can see all the smiling faces of people still involved in my life even now. The thing is, I didn’t win, but that is not what I remember about the day. I remember a glorious afternoon and evening with people that I admire and care about. I remember laughing so hard that one of us fell over. I know that we still talk about that day even now. I don’t even remember what I was nominated for, because it is the people I remember, not the lack of a win.
All of this is to say, it is the people in our lives that make life worth it. It is the people who pick us up and put us back together. It is the people that celebrate our successes and cheer us on. So why would I want to have less of that, and restrict my access to these moments. Share the joy, share the progress, and share the moments that matter in making us who we are. Life is short, so seize it.
This month I’ve been honouring of World DNA day 2025 by publishing a number of posts linked to what DNA is, how we look for it, and what it means to send it away.
Today I’m talking about Upgrade by Blake Crouch. In the story explored in this world, DNA based technology, although very obviously rooted in present day science, has evolved and so has the impact and access to this technology for both individuals and society. In this post I thought it might be interesting to explore ow much of this book is science, and how much of it is fiction? Before I get onto that however, here’s a reminder of the other posts that have been available in the DNA blog series:
One of the reasons I picked Upgrade for the final book review is that I thought it would be interesting, after discussing the current usage of DNA for testing and therapies in previous posts, to explore a book that covers a slightly further future, based in 2060, and what impact the use of DNA technologies could have on humanity in the future.
‘You are the next step in human evolution . . .’
What if you were capable of more?
Your concentration was better, you could multitask quicker, read faster, memorize more, sleep deeper.
For Logan Ramsay, it’s happening. He’s beginning to see the world around him, even those he loves the most, in whole new ways.
He knows that it’s not natural, that his genes have been hacked. He has been targeted for an upgrade.
Logan’s family legacy is one he has been trying to escape for decades and it has left him vulnerable to attack. But with a terrifying plan in place to replicate his upgrade throughout the world’s population, he may be the only person capable of stopping what has already been set in motion.
To win this war against humanity Logan will now have to become something other than himself . . .
In this world, DNA based technology, although very obviously rooted in present day science, has evolved and so has the impact and access to this technology for both individuals and society. It raises some interesting questions about what it means to be human. In this post I thought I would explore some of the science that is included, and what questions the use of this science brings into play.
Are visions of a world where DNA controls our lives unique?
Before I get into the science of the book however, I wanted to flag that visions of a world where the use of DNA testing, evaluation or modification, are not new. GATTACA (did you see what they did there……they are all DNA bases) have been around since the 90’s, when the technology we use clinically now was only in its infancy. Fear of how science could be used in the future is a pretty constant feature of this type of creative content, as it provides a safe way to explore these fears and ethical challenges. I suppose what I’m saying is that just because something is included in these kinds of visioning pieces does not make it bad, wrong or scary. It just means that we also need to think and reflect on what checks and balances are included as part of their introduction in order to make sure the world we create and influence based upon them is the one that we are aiming for, and we have taken steps that include the law of unexpected consequences rather than ignoring it. DNA editing is an amazing, technically complex and powerful tool that has the potential to be positively life changing, so please keep that in mind when you read the rest of this post.
The world of upgrade
In the world of Upgrade the impacts of climate change have really been felt. Entire cities have been flooded as the seas rise and access to food has become a real issue for vast portions of the worlds population. Logan, our protagonist is the son of a genius, a woman changing the face of science. Being the child of a world famous geneticist makes Logan feel the reality of being a normal person surrounding by an extraordinary vision.
I had extraordinary dreams but had been gifted only an ordinary mind
Sadly, as is often the case in these tales, his mothers (Miriam Ramsay) drive for change comes with a fair amount of hubris. In an attempt to address the food shortages Miriam, with Logan supporting as a junior scientist, develops a new gene editing tool called Scythe in an attempt to genetically enhance rice crops. The process goes wrong, and results in The Great Starvation that leads to the deaths of 200 million people.
As a result of the mass deaths, genetic manipulation using Scythe or related tools originating from CRISPR, are outlawed and their use results in a mandatory 30 year minimum jail term. Thus making the field of genetics either outlawed or suspect, and to the birth of the Gene Protection Agency, a police force which aims to track down those undertaking illegal manipulations or research.
Logan ends up going to prison for his work with his mother’s research, and his mother commits suicide. After serving his time Logan is released and joins the very agency that has been set up to prevent a repeat of the genetic manipulation that changed the world. At the start of the book Logan is investigating a scene where an explosion happens, his body is hit by shards of ice, and his life changes again…..forever.
My mother had tried to edit a few rice paddies and ended up killing two hundred million people. What havoc could she wreak—intentionally or through unintended consequences—by attempting to change something as fundamental as how Homo sapiens think?
So, what is gene editing?
I’ve already mentioned CRISPR but I’ve not described what it or gene editing actually are. Gene editing as defined by the World Health Organisation is:
A method for making specific changes to the DNA of a cell or organism. It can be used to add, remove or alter DNA in the genome. Human genome editing technologies can be used on somatic cells (non-heritable), germline cells (not for reproduction) and germline cells (for reproduction).
Before I go further I should probably talk about how CRISPR works and what it is used for. Tools like CRISPR/Cas9 are tools for gene editing, and are the present day origins behind the futuristic tools present in Upgrade. Emmanuelle Charpentier and Jennifer Doudna were awarded the Nobel Prize in Chemistry in 2020 for the development of CRISPR, commonly referred to as genetic scissors.
CRISPR allows you to design a targeted way of manipulating a gene section that you are interested in, and in some cases then replace it with an alternative gene section, which enables the gene to function in a different way. Being able to target and replace, or inactivate genes, in this way opens up a whole new world of possibilities, from health to industrial applications. There are three main approaches to gene manipulation:
Replacing a disease-causing gene with a healthy copy of the gene
Inactivating a disease-causing gene that is not functioning properly
Introducing a new or modified gene into the body to help treat a disease
Now, wearing my geek credentials on my sleeve, I wanted to share with you a music video that describes how CRISPR works. It’s set to the music of ‘Mr Sandman, bring me a dream’ and is retitled ‘CRISPR/Cas9 bring me a gene’. I love this as it I think it describes the history of the process really well. I will tell you now though, that when I made Mr Girlymicro watch this for the 5th time he could not get out the room fast enough, so this may just be a me thing.
Where is the science rooted in the present?
Having talked about the fact that gene editing isn’t the work of science fiction, I thought it would be useful to talk about how and where it is actually being used right now.
According to the Federal Drug Administration there are a variety of types of gene therapy products, i.e. products that manipulate genes, currently available:
Plasmid DNA: Circular DNA molecules can be genetically engineered to carry therapeutic genes into human cells.
Viral vectors: Viruses have a natural ability to deliver genetic material into cells, and therefore some gene therapy products are derived from viruses. Once viruses have been modified to remove their ability to cause infectious disease, these modified viruses can be used as vectors (vehicles) to carry therapeutic genes into human cells.
Bacterial vectors: Bacteria can be modified to prevent them from causing infectious disease and then used as vectors (vehicles) to carry therapeutic genes into human tissues.
Human gene editing technology: The goals of gene editing are to disrupt harmful genes or to repair mutated genes.
Patient-derived cellular gene therapy products: Cells are removed from the patient, genetically modified (often using a viral vector) and then returned to the patient.
There are a number of ways that gene therapy products are already being used for the clinical management of patients, including for patients with conditions such as HIV and sickle-cell disease. One big change that has occured during my clinical career is the use of CAR-T cell therapy for tackling some types of cancer. CAR-T cell therapy is a type of immunotherapy where a patients own T cells (type of white blood cell) are taken from a patient who has cancer, and the cells are then modified in order to better recognise and attack cancer cells within the patients body when they are then given back. So gene editing is already saving lives and in every day use, even if its roll out is currently limited.
Having established that gene editing is very much the next frontier for expansion in healthcare, it’s probably important to consider how stable these changes will be within the wider the gene pool. It’s worth noting that the human genome editing techniques that are being introduced in healthcare are linked to somatic cells, where changes would be non-heritable, rather than within germline cells, which are involved in reproduction, where any changes would be inherited by future generations. Most of the changes that are currently being targeted for gene therapy would not therefore cause the changes to be established within the gene pool. There is a question about whether the target genes, even for somatic changes, may become more established as some of those carrying them may not have previously survived to reproductive age, but to be honest this feels like the impact will be minimal and a price worth paying as a society for improving both quality and length of life in those impacted. Changing future generations of children is however a whole different ball game.
The technology discussed within Upgrade has moved on somewhat from CRISPR. It retains some features of current technology however, as the delivery of Scythe is via viral vector. The interesting thing about this form of delivery is that, in the world of Upgrade, the viruses have been modified and use their standard invasion routes to deliver the genetic material into cells, but, unlike the way that this is being undertaken as part of gene therapy in current healthcare, the viruses do not appear to have been fully modified to remove their ability to cause infectious disease. Some of the plot, therefore, is driven by the fact that it is possible to undertake wide spread indiscriminate gene editing within the human population. The modified viral cells retain their transmissibility alongside their gene editing functionality, and so a gene manipulation can spread in a similar way to any respiratory viral infection. The R0 within Upgrade is 8, which means that every person infected will infect, on average, 8 other people, which means the potential for spread within the population is massive. (If you want to know more about what an R0 is, I’ve covered it in a previous post here). It is not clear to me whether the gene targets within Upgrade are targeting just somatic changes, or a combination of somatic and germ line, but when you can spread so widely so quickly that is probably not the main consideration.
What questions does Upgrade raise?
Within the world of Upgrade, the gene editing doesn’t just target a single gene, but a whole suite of different genes for large scale changed. The problem with using gene manipulation that changes multiple gene targets, that are non-personalised to the condition/individual, and are highly transmissible, is that it is highly likely that the changes won’t work for everyone’s genome. There are going to be side effects or potentially significant impacts. Within Upgrade these are seen through errors that then occur in the brain due to protein mis-folding, very similar to how prion diseases work. The change in some people is catastrophic and there is no intervention available to reverse it. Using indiscriminate gene manipulation has the power to create mass disruption and change societies. It is this power for change that is the jeopardy that drives the novel. Is the cost worth the outcome, and who gets to decide? How much collateral damage would we be prepared to accept, even if the wider benefit to society is a positive one?
Prion diseases: A rare group of neurodegenerative disorders October 2022 In book: Viral, Parasitic, Bacterial, and Fungal Infections Antimicrobial, Host Defense, and Therapeutic Strategies (pp.651-662) Edition:1 Chapter: 53 Publisher: Elsevier: Academic Press
What does it mean to be human?
As part of this risk/benefit consideration, Upgrade asks a lot of questions of the reader, the main one of which, for me, is what does it actually mean to be human?
There is a genetic definition of what it means to be human, but the gene modifications within humans causes our protagonist Logan to ask some very valid questions about what it actually means to be human. Is it just about genetics? How much can we change not only our genes, but our outlook/perceptions, as people and still remain human?
The ‘upgrades’ received cause different characters in the book to judge humanity in general, and other human beings, in very different ways. Do genetic changes make you superior? Does being intellectually smarter permit you to make decisions for others for their benefit, as determined by the smarter individual? In many ways this brought to mind, for me, the old approach to clinical decision making, which was very paternalistic and the role of the person/people impacted was highly passive. I’d like to think we are now moving towards a much more patient focus decision making process, but this book made me think about what would happen if this model was used, not just for one to one interactions, but for the future of humanity.
The question about decision making is an interesting one however. There is plenty of data that demonstrates improved decision making in small groups, and if time is of the essence how would you engage with enough people for a decision to be valid? Especially a global decision? How many people would you need to interact with for a choice about changing the DNA of your species to be valid? How would you manage a lack of consensus? Would you let the world burn whilst the choice was being made, or would you accept that at some point someone would need to step in and lead the way forward? It’s the uncomfortable space between ethics and pragmatism, and definitely not something that is easy to answer, even conceptually.
Is intelligence the problem?
As discussed above, a lot of the plot driven by the counter to our protagonist in Upgrade, is based on the concept that if humans were smarter they would make better decisions. Therefore, by improving how people think and removing some of the emotional component the human race would be improved and therefore ‘saved’. This is especially important in the world of Upgrade, as because of the damage that is being done linked to climate change and other damage caused by humanity, the clock is ticking and Logan is very aware in his upgraded state that there is only 100 years left to save mankind.
The problem, as it plays out to me, is that it is very much not about intellect however, it’s about the ability of individual humans to care enough for others. For one person to make decisions that costs them rather than benefits them for the sake of someone that they do not know well if at all. This is especially true for problems that are going to impact future generations, like climate change, where the people most impacted have yet to be born. By the time we ‘meet’ those who will be most affected it will be too late to save them. Even for a present day context it raises questions, we all think of ourselves as having empathy and caring for others, so why does that not play out and allow us to care for the migrants that are dying trying to join us and share in our safety? Why is our compassion so limited?
One of the reasons for this has nothing to do with intellect, and would in no way be altered no matter how smart we become. It’s based on a theory known as the Dunbar number, which predicts that we can only empathise with a maximum number of 150 people, the number of people that would likely to have been the maximum size of our primate tribe. More than this, we can only truly care, to the point we may want to sacrifice, about a much smaller number of people. The book therefore postulates that we aren’t held back due to a lack of intelligence or innovation, we’re held back by a lack of compassion and the ability to truly care about people we don’t know and will never meet. If we are to change anything about ourselves in order to save mankind therefore, it’s not intellect we need more of, we need to find a way to increase our capacity for compassion and therefore change our Dunbar number, to adapt for the world we now find ourselves in. So maybe the answer to the problem is to become more ‘human’ rather than less.
Where do all of these questions leave today’s gene editing technology?
Gene editing technologies are making massive strides, saving lives, and positively helping people who have serious health conditions.
Somatic gene editing is well established, and has been developed over the last 20 years so that regulation is in place, and it being more and more routine rolled out in countries that have access to advanced scientific technologies. The problem is just that however, these interventions are technologically challenging and incredibly expensive, and therefore not universally available. This means that they also do not necessarily take into account the diversity of the human genetic population or the lived experience within different cultural communities. Regulation is also not present universally, with some people forced to access these therapies through the use of rogue clinics, or by undertaking medical tourism, which brings with it increased risk. There is also the potential for illegal, unregistered, unethical or unsafe research and other activities, including the offer of unproven so-called therapeutic interventions, as with any emergent technologies. Ensuring equity of access and appropriate regulation will be essential to ensure a safe global adoption of these therapies.
Germline gene editing is however in a very different place, as this would lead to the editing of DNA in a way that may be heritable across generations. There is an intense debate linked to its use as the the future generations that would be impacted would have no capacity to consent to the changes, and or risks, that are being made. There could be possible risks and consequences for offspring and for society in general, and once that genie is released it will not be possible to put it back in the bottle. Discussing what circumstances it would ever be appropriate to undertake these changes requires us all to be actively engaged in these discussions.
I hope you’ve enjoyed these series of blogs linked World DNA Day and taken some to celebrate the miraculous nature of just being you. I’ve really enjoying sharing some of the technical information, but also diving into some fictional worlds and discussing the thoughts that they provoke. With summer coming up I hope you may even pick up a copy of these great novels and dive into their worlds yourself. If you find any others in your reading adventures, return the favour and let me know. I may even include them in a future review. Happy reading.
Friday just gone, 25th April, was World DNA Day. I’ve had a series of blogs that I’ve been playing around with linked to both DNA in our everyday lives and two book reviews where the world changes because of genetic testing and genetic manipulation. I thought I would write these posts, because as much as artificial intelligence could change the way we live and is frequently discussed, we are all accessing DNA based testing more and more, with many of us not really thinking about how this too is changing the world in which we live. Depending on how you feel about science and needing to have a refresher on what DNA and how we look for it and interpret it, you may want to hit up part one of this blog series first.
In part one I also introduced the kind of testing that DNA and DNA sequencing can be utilised for, not just in a accredited healthcare laboratories, but also linked to private companies who offer information on things like ancestry. In today’s blog I wanted to go a bit more into what can be the less thought about results of sending away your DNA, and also what kinds of things you might want to think about, or have in place, before you do.
Thinking unexpected consequences?
In part one I used this quote from a recent article:
As stated in a recent Independent article:
As they’re based on estimates, I suggest treating home DNA tests as a fun investigation to get to know your family history a little better rather than a to-the-letter representation of everything that’s ever happened in your gene pool – Ella Duggan Friday 28 March 2025
It describes sending away of your DNA as a fun investigation, and recommends not taking the results too seriously. This is definitely the right attitude in many ways, as you wouldn’t take key health guidance from a magazine quiz, you’d want to speak to a healthcare professional who can put your results in context. The problem with not taking the tests themselves too seriously is that we don’t really think about the consequences of taking them or where the results might lead. My family have been given these for Christmas, for instance, and it was seen as a fun piece of science that could be done after lunch. Taking and sending away your DNA, the thing that makes you you, however, should always be done with a little more consideration that that. So I thought it might be useful to use just a couple of examples of why.
Health services
Sending away DNA for health reasons to private companies has been controversial ever since it was introduced into the UK and there are a few reasons why this is the case.
Firstly, if you have health concerns, then really you should be accessing medical care through healthcare professionals who you’ll be able questions, and who can put your results into a risk context for you based on your own medical history, rather than just getting a list of genes in isolation.
One of the other reasons you should manage this form of testing through health providers is that you can then be linked into any medication or further testing that is required. The presence of a gene alone can be pretty meaningless, you need to then look for whether that gene is being expressed (see part one) in order to really understand it’s impact, and so there are likely to be follow up requirements to any results received.
If you are going through genetic testing, especially if it has impacts on decision such as reproduction, you would normally be supported through the process ahead of the testing, and when the testing is returned, through professionals such as genetic councillors. If you get your results by sending your DNA away you may get completely shocked and surprised by the results that you can get back, and may make some decisions based on the findings that may not be correct for you and require better input from someone more used to interpreting the results. It could feel like a really lonely way to hear bad news.
Finally, these tests are being sent off to laboratories that don’t require accreditation. They are acting as medical tests, without going through the rigor that is required for the equivalent tests in healthcare, and yet are interpreted, by some, in the same way, and therefore effectively out of context. They may also not have the required levels of validation linked to the information and interpretive guidance that is issued with a result, so that you know what being present or absent for gene X or Y actually means for you. It also means that there may be less processes in place to ensure that you get the result that is actually meant for you and not for Professor X down the road. If you are processing hundreds of samples this kind of error, without safety checks, can be easier than you’d think. Knowing the quality of the result you are receiving may be less than obvious.
Ancestry services
OK, OK, I can hear you say. I wouldn’t send my DNA off for medical testing, but surely sending it off for ancestry services is ‘no harm, no foul’ and just a bit of fun. My first caveat here is that not all ancestry services are the same and not all of them look at the same sections of your genome. Some will look at your mitochondrial DNA (which will always come from your mother and your maternal line) in order to give a view of where your ancestral DNA comes from over generations. This is often referred to ancestral origins, and is much less likely to hit you with real time life dilemmas. Many kits are also paired with items that look at wider genomic matches, or DNA matches, and so you may get back more than you bargained for if you didn’t look closely at what was going to be provided.
I’ve included just a couple of, extreme, examples of how these kinds of unexpected consequences can play out in real life. The first is a BBC News story that came about because a woman was contacted by a stranger after sending off her DNA via an ancestry site. From the results it eventually became apparent that she had been accidentally swapped as a baby in a hospital in her 50’s with another child. Thus having dramatic and rather unexpected consequences for her and her family.
The other example I’ve included links to a couple of documentaries where the use of DNA matching platforms has uncovered serious misdemeanors or crimes, including IVF undertaken using the sperm of medical professionals without the knowledge or consent of the parents involved, and sperm donors being involved in the insemination of more couples than disclosed, thus increasing the risk of their children potentially interacting/dating/mating in later life without knowledge of their genetic linkage. This is obviously not the fault of the DNA matching service, and is something that is beneficial to uncover and stop, but has hugely dramatic impacts on those involved without any prior warning or support in place. It certainly wasn’t what they expected when they sent away their swab.
Is it just human DNA that counts?
Finally, to follow up on the takes of the unexpected, and because infections are fascinating, I wanted to share a link to a video that I think is really great about the first time DNA testing of HIV was actually used to convict someone of a crime. This one isn’t a word of warning, as I suspect that none of us are going to decide to deliberately inject someone with HIV contaminated blood, but I wanted to end this section with something where the use of DNA testing in the hands of people who really know what they are doing is a powerful tool for good. Also, because I wanted to give a non-human example of where I think some of this may go in the future.
What do we need to know before we start to send our DNA away?
Having laid out my warning stall, I wanted to go through some things I think you should actively think about before sending your DNA away.
What is the legal situation?
First and foremost, the sending of DNA away for processing is covered under something called the Human Tissue Act or HTA (in England). I’m flagging this as the first thing as, unlike what you see on TV, you should not be taking DNA from other people and sending it off to see what it says, and especially not for any form of DNA match testing. In the UK, if you do take anyone’s DNA sample without them being aware of it, it is considered a violation and you are liable to prosecution which can result in up to 3 years imprisonment. It is not OK to steal someone else’s DNA without their consent! There’s a lot to this one and I’m not a legal expert, but it seems to be something that many people are not aware of and now you know.
What level of information will be gathered?
All of the different tests offered will do things, and companies interpret the results slightly differently. It’s incredibly important to know what you are sending your DNA away to be tested for, how it will be tested and what kind of information you can expect back.
The main types of DNA tests and the areas they analyse are:
Autosomal DNA Tests = examine the 22 pairs of autosomes and the X chromosome. Commonly used for ancestry testing and can help determine ethnic origins, identify genetic predispositions, and find relatives. Utilise single nucleotide polymorphisms (SNPs), which are variations in a single DNA base pair
Y-DNA Tests = analyze the Y chromosome, which is passed down from father to son. Used for tracing paternal lineage and can be helpful in genealogical research
Mitochondrial DNA (mtDNA) Tests = use mitochondrial DNA, which is inherited maternally (from your mother) used for tracing maternal lineage and can be helpful in genealogical research
Paternity Tests = examines specific regions (loci) on the chromosomes to look at parental relationships
Health-Related Genetic Tests = looks for specific genes or regions of the genome that are associated with certain health conditions to try to identify genetic risks, diagnose genetic disorders, or assess treatment options
You may need to read the small print to really understand how the testing will be undertaken and to manage your expectations. If you can, make sure you look up examples of what the results you will receive will look like, and if there would be any follow up support given. Also, crucially see if there will be additional funding required to get access to the full data set you are expecting so you don’t get hit by any unexpected requirements.
How will data be used?
The next few sections are all linked to what happens to the results of your testing that you are sending away.
The first thing to check before you send off your test is how long will your data be stored for once. This is important for you in terms of being able to access reports, but also about how long your legacy data will be available. Will you have access to wider information if you request it to be passed to your healthcare provider? Is there any information on the data analysis tools used? Are you even allowed to ask questions or is all patented and under intellectual property rules, which is reasonable but you should know what the boundaries are. Most healthcare reports should be kept for at least 10 years, but as these are covered under different guidance, will you only have access to download your data for a set period of time? Will it be possible to get your own local back up of your data? Once you know the answers to these questions you can then make active choices and comparisons about which aspects are important for you.
The article below is a little old, as it’s from 2018, but many of the questions still stand. How carefully will your data be ring fenced? You may not think about it much, as your DNA may hold little financial value to you, but DNA databases are one of the main assets that companies who process your DNA have, and why the testing is actually relatively cheap. Having access to thousands of DNA sequences, along with medical histories sometimes, means that data is incredibly value for scientific and commercial development. This is OK, we need sequences to develop new testing. Pharmacy companies also need access to sequences to develop and model new medicine. Therefore, it is likely that your data monetised and used for other purposes, which may or may not be OK with you. The big question to ask is whether it will be anonymised and how it will be used. Knowing this information before you commit allows you make informed choices, as not all companies are likely to be identical in how they handle things.
Another aspect that you might not think about is data security. If your data is of value to the company, and therefore is a potential asset, then it may be of interest to others. This can make data security to prevent things, such as hacking, important. This could be especially true if your DNA reveals linkages of significance, or things that you might not wish disclosed, such as cancer risk. Doing some research to ensure the security of any data that is held is important, but not often high on the list of questions that people ask.
Who can data be released to without my knowledge?
I’ve talked above about who will have access to your data, but mostly I talked about your anonymised data. It may not just be anonymised data that you are concerned about by however. If you are sending off for testing that relates to cardiac, cancer, diabetes or other risks, than this can have much wider impacts if shared. The legal landscape in relation to this is very much changing and catching up with the concept of genetic information as a protected asset is slow. Also, warning, I’m no expert in this. However, when sending away for this kind of testing it is important to know that it is often not covered by medical confidentiality, as it’s not considered a medical test when conducted via private companies. Being aware of how this impacts the rules around your data and what the company will or will not release is key. Why is it key? Well, it can impact all kinds of insurance schemes, from requirements to declare for holiday insurance if you are seen as ‘knowing’ a risk, to life insurance changes in cost or profile if released directly to the company. Knowing whether your personal, non-anonymised data can or will be released is essential before choosing whether or to whom you’re prepared to send you swab away to.
I suspect that this last point will probably impact those of you reading this blog less, but for to complete this list…….your DNA can also be released to law enforcement, depending on the country, so if you’ve secretly been a mass murderer then maybe don’t send your swab away and get your DNA added to a mass database.
What will happen if the company is sold?
As I said earlier, one of the biggest assets these companies hold is the databases of DNA sequences which we provide them. When something happens to the company therefore, it is this asset that many of those interested in the company might be after, and they may have nothing to do with the purpose you sent your testing for. Reading the small print before you send away your sample may not be able to prepare you for what happens when those rules change and you are no longer dealing with your original commercial provider. The one thing you can do in these circumstances in understand what access and rights you have to request that your data is deleted, or to delete it yourself, in the case that circumstances change.
I’m aware that the section above on what you might need to think about is pretty heavy and so I wanted to finish part 2 on something a little more population level and upbeat in relation to why having access to this testing is a good thing for science in general. For instance, we know that the ability to undertake ancestral testing was a reason that the bones of Richard III were identified and confirmed, which had big impacts for history buffs. It show that the use of wider availability of testing has all kinds of benefits, and not just to science. In terms of wider science, being able to look at bones using DNA testing has supported identification of Mycobacterium tuberculosis as present in Egyptian mummies which has helped us understand the evolution of this infection over centuries. More recently, looking at the development of Homo sapiens and how we became the human beings we are today has been forever changed by wider applications of these methods. Use of these technologies can therefore impact all aspects of our lives moving forward, and it really is up to us, both as individuals and as a society, about where they work for us.
Parts three and four of this blog series will be linked to book reviews that explore what those futures could looks like if the use of DNA testing and genetic manipulation change how we look at ourselves and others. So join me in continuing to explore the power of DNA.
Friday just gone, 25th April, was World DNA Day. I’ve had a series of blogs that I’ve been playing around with linked to what DNA is, how we look for and investigate it and how we are exploring DNA in our everyday lives. Linked to this I’ve also got two book reviews coming where the world changes because of genetic testing and genetic manipulation. So this is the first of four part DNA bonanza.
I thought I would write these posts, because as much as artificial intelligence could change the way we live and is frequently discussed, we are all accessing DNA based testing more and more, with many of us not really thinking about how this too is changing the world in which we live.
I remember really clearly the first time I actively came across the concept of DNA, DNA testing and DNA manipulation. It was in Jurassic Park, when Mr DNA pops up at the start of the film to talk you through how they used DNA and cloning in order to make the dinosaurs. This film came out in 1993, I was 13 and I just remember how all of my class were queuing up to get tickets. It was the first film I really remember there being hype about, well that and Aladdin which was a different kind of seminal moment. It was the first film I remember watching and thinking just how cool science and scientists were.
In fact I talk about Mr DNA so much that the wonderful Mr Girlymicro brought me a Mr DNA Funko pop which lives on my desk at work and reminds me that the impression we make on people stays with them.
What does all this have to do with how we use DNA now? Well, in 1990 when Jurassic Park came out, the routine use of DNA, even in research, was still pretty much science fiction. The structure of DNA had only been described in 1953. Polymerase Chain Reaction (PCR), which is the main way we investigate DNA, had only been developed in 1983, and was only starting to become more widely available in the 1990’s. When I started working within healthcare in 2004, we were only really just starting to move from PCR being something that was used in research to something that was common place in clinical diagnostics. The leap from there, to a world where thousands of us can swab ourselves at home and post samples off to be diagnosed with SARS CoV2 during the pandemic, or to get information on our genetic heritage, would have sounded like something that would only occur in a science fiction novel if you’d mentioned to me back theb.
Just a flag, this part one post has a lot of the technical stuff linked to what DNA is and how we investigate it. You may want to skip this post and head directly for part two if you don’t want to be reminded of secondary school science, but if you can bear with me I think it will help some of the context.
What is DNA?
DNA, or to give it its full name Deoxyribonucleic acid, is commonly referred to as the building block of life. The structure of DNA consists of a double-stranded helix held together by complementary base pairs. The nucleotides that form the base pairs are adenine, thymine, guanine or cytosine. These nucleotides act to link the two strands together via hydrogen bonds, with thymine always pairing with adenine (T-A) and guanine always pairing with cytosine (G-C).
Sections of DNA then combine together together to code for genes, which are sections of DNA that work together in order to code for proteins, that then permits the expression of our DNA in physical form.
Genes are organised into chromosomes or packages of DNA. Each chromosome is formed from a single, enormously long DNA molecule that contains a strand of many genes, with the human genome containing 3.2 × 109 DNA (3,200,000,000) nucleotide pairs, divided into 46 chromosomes formed from 23 pairs (22 pairs of different autosomes and a pair sex chromosomes).
So how do we get from DNA to proteins? The specific sequences of nucleotides that form our DNA are arranged in triplets (groups of three). To turn DNA into protein, it gets transcribed into RNA (ribonucleic acid) within cells, with each of these triplets coding (translating) into an amino acid, which then get combined together to form proteins. The amino acids combined dictate what form and function the resulting proteins takes. Proteins then serve as structural support, biochemical catalysts, hormones, enzymes, and building blocks for all the processes we need to survive as humans.
Long and short, everything comes from your DNA, it’s super important, and is unique to you, but it’s structure is complex and there’s a lot of it in each of us.
How do we investigate DNA?
Now that we know about what DNA is, and how important it is for life, not just for humans but for all living things, it makes sense why so much time and energy has been deployed into understanding more about what it means for us as a species, as well as for us as individuals.
I’ve mentioned that PCR was first developed in the 80’s but didn’t really come into routine clinical testing until the 2000’s. What is PCR though and how does it work?
I often describe PCR as a way to look for DNA that is similar to looking for a needle in a 25 story block of flats sized haystack. The human genome is 3.2 billion base pairs, and we are often looking for a fragment of DNA about 150 base pairs in length, 1/21 millionth of the genome. It’s quite the technical challenge and you can see why it took quite a while to be able to move from theoretically possible to every day use. What makes it even more complicated is that you need to know what that 150 nucleotide fragment is likely to contain or where it is likely to be positioned within those 3.2 billion base pairs to really do it well. The human genome was not fully sequenced, and therefore available to us to design against, until the year before I started my training at GOSH, 2003. The progress therefore in the last 20 years has been extraordinary, and I can only imagine what will happen in the next 20 years. Hence the book reviews that will be coming as parts 3 and 4 of this blog.
So, how does PCR work? Well the first thing to say is that there are actually a number of different types of PCR, although the basic principles are the same. For example, there are some types of PCR that target RNA. There are also types of PCR that are used more frequently within clinical settings for things like SARS CoV2 testing, that are called Real Time PCR, called that as results become available in real time rather than waiting for the end of the process. It is for Real Time PCR that the small ~150 nucleotide fragment length is an issue. So all of these processes have their own pros and cons. Like many things in science, you have to use the right process to answer the right question.
The basic principles shared between types of PCR are as follows:
Designing your primers:
Primers are the pieces of DNA that you design and make that will stick to your target piece of DNA you are interested in. The reason this works is because of the fact that the nucleotides that make up DNA are complimentary and so A binds to T, C binds to G. As DNA is double stranded you can design your primers (your equivalent to the magnets to find you needle in your haystack) so that they will bind to your specific target (the piece of DNA you are interest in). If you want to have your primer stick to a piece of DNA sequence that reads AAG CTC TTG, you would design a primer that ran TTC GAG AAC using the complementary bases, make sense?
You design one set of primers for one strand, this is called your forward primer (moving from 5′ to 3′), and then you design your reverse primer at the other end of your target for the opposite DNA strand (moving from 3′ to 5′). Doing it this way means that when you start your PCR process you end up with complete copies of your target. You will then successfully have pulled the needle from your haystack using you targeted magnets.
Undertaking the PCR:
Once you’ve got your primers (which you can just order in once designed) you can then get onto the process of the PCR itself. You combine your sample that you think might contain the DNA target you are looking for (be that human, bacterial, environmental etc) with the reagents (chemicals) that you need to make the process work all in a single small tube. This tends to be a delicate process that needs to be undertaken at controlled temperatures as the protein that runs the process (Taq polymerase) is delicate and expensive. To do this we combine:
DNA Template: This is the sample that contains the DNA target you want to amplify
DNA Polymerase: Almost always this is Taq polymerase which is used due to its heat-stability as it originates from a bacteria that lives it deep sea vents. This allows it to function at the high temperatures required for PCR and is used to make the new DNA copies
Primers: These are the short, synthetic DNA sequences that you design to attach to either end of your target DNA region. These then allow the DNA polymerase to add nucleotides to create the new DNA strands
Nucleotides (dNTPs): These are single nucleotides (bases) that are then used to build the new DNA strands (adenine, thymine, guanine, and cytosine)
Buffer Solution: This solution provides the optimal conditions (pH, salt concentration) for the enzyme to function properly
Once you have your reagents you then put them on a platform that heats and cools for different steps to allow the enzymes to work and for the new DNA strands to be created:
Denaturation: The double-stranded DNA template is heated (typically to 95°C) to separate it into two single strands. This step ensures that the primers can access the DNA sequence of interest
Annealing: The temperature is lowered (typically to 50-60°C) to allow primers to bind to their complementary sequences on the single-stranded DNA. This is the step where your magnets find their needle
Extension: The temperature is raised again (usually to somewhere around 72°C, the optimal temperature for Taq polymerase activity). Taq polymerase extends the primers by adding complementary nucleotides based on the DNA sequence to create new copies of the original DNA target
These three stages are repeated in cycles, typically 20-40 times, which results in thousands and thousands of copies of the original target to be created, so that eventually your 25 storey haystack is made up of more needles than it is hay, and therefore it is easy to find what you are looking for.
Interpreting your results:
At the end of your PCR step, if you are using traditional PCR, you run what is now called your PCR product or amplicon (the things you’ve made) through something called a gel. This is just a flat jelly made of agarose (or seaweed) which also contains a dye that binds to DNA and allows to separate your DNA based on size. This allows you pick out where you have samples that have the massive amplification you are looking for, as you can see it as a band within the gel. If a band is there and the right size (as you know how big your target was supposed to be) this is a PCR positive.
If you need to know more detail than whether something is present or absent, for instance if you need to know not just that a gene is there but which variant of a gene is present, you need to be able to tell what the nucleotides that were added between your two primers actually were. To do this, you will follow up PCR with a process called sequencing.
You take your target PCR’d section and then put it through a process to work out what the nucleotides added were. This involves doing the PCR process again, to make even more copies, but the nucleotides added into the reagent mix have fluorescence attached so you can tell which ones have been added during the PCR process. G’s often produce a black colour when hit by light, A’s green, T’s red and C’s blue.
For our original sequence we talked about, AAG CTC TTG, the sequence would read Green, Green, Black then Blue, Red, Blue followed by Red Red Black. Colours are then back interpreted into a DNA sequence (a series of letters) and there you have it, you know what the DNA is between your primers and you can then interpret your sequencing result. If you have large fragments of DNA you are interested in, you may have to do this in overlapping segments and put it back together, something like a jigsaw, before you can get your answer, but the basic process is the same.
What can DNA tell us?
As I’ve said, the search for DNA and specific genes has become an increasingly normal part of providing diagnostics in healthcare. Most of us will have sent off a swab for a PCR at least once during the COVID-19 pandemic. PCRs are frequently used in my world of infectious diseases to see if a bacteria is present or absent. They are also used so that I am able to see if a bacteria will respond to an antibiotic, by seeing if they carry antibiotic resistance genes, which can be crucial to getting patients on the right treatment at the right time.
Looking for specific variants of genes is also key to making sure that the treatments we give also don’t cause any unexpected consequences. A good example of this is when we use PCR and sequencing to look at genetic variants of a gene called MT-RNR1. A specific variant in this gene, m.1555A>G, is known to increase the risk of aminoglycoside-induced hearing loss. Aminoglycosides are a crucial antibiotic class that are used pretty widely, but especially in management of some conditions such as cystic fibrosis and certain types of cancers. A small number of people have a gene that makes them prone to something called ototoxicity as a result of taking these antibiotics, resulting in hearing loss. If we know a patient has this gene variant we can then choose to use different antibiotics, improving patient outcomes and avoiding a life long hearing impact.
Outside of screening linked to patients presenting with specific conditions, the use of DNA sequencing is being utilised more widely to look for genes or conditions before they even present with symptoms, in order to reduce time to diagnosis, and hopefully to be able to find patients and start management before they’re impacted or even present as unwell. A great example of this is the newborn screening programme that started last year. This screens newborns using the heel pricks of blood taken at birth so that rare diseases that could take months or years to diagnose by traditional means are picked up early in life, therefore allowing appropriate treatment to start earlier and hopefully saving lives.
DNA is fascinating and I love knowing about it. It’s not just me though. In recent years there has been an increasing trend for people to send off their DNA for other purposes than to hospitals for clinical testing. I’m not going to say too much about this in part one, but it was this that really inspired me to write these posts in the first place and is the main focus of part two of this blog series.
Just a quick google however provides a wide number of different companies offering a variety of DNA testing services outside of the NHS (NB I don’t advocate for any of them):
Crystal Health Group: Operates a network of DNA testing clinics, offering relationship testing and other services.
23andMe: Provides DNA testing for health, ancestry, and other personal insights.
Living DNA: Focuses on both ancestry and wellbeing-related DNA testing.
MyHeritage: Provides DNA testing, particularly for ancestry research.
AncestryDNA: Company specialising in DNA testing for ancestry discovery.
The complication with all of this type of provision of testing is that outside of the clinical world in the UK, where testing should be undertaken in accredited laboratories and reporting of the results must meet certain standards, sending off DNA to private companies is much less monitored.
I hope you can see by some of the technical descriptions just how complicated these DNA processes can be. How time consuming, and how expensive to get right. There is also a lot of nuance about the different types of PCR, sequencing, gene targets, and results analysis that can be offered under the umbrella of ‘DNA testing’. Without the right people involved to make sure that there is embedded quality assurance challenges could arise, depending on what kind of testing is undertaken.
As stated in a recent Independent article:
As they’re based on estimates, I suggest treating home DNA tests as a fun investigation to get to know your family history a little better rather than a to-the-letter representation of everything that’s ever happened in your gene pool – Ella Duggan Friday 28 March 2025
The devil for all of these things really is in the detail, and we’ll get into that detail much more in part two! For those of you interested in learning more about the history of DNA testing, I’ve included a talk below. Happy World DNA Day
I got an alert of my phone last week that I set up this blog on WordPress 10 years ago! That was a bit of a shock I can tell you. That said, as I posted about in 2020, although I set up the blog and made my first post as I finished my PhD in 2015, I didn’t start posting regularly of another 5 years. I started it as I was looking for my next passion project but I didn’t really know what I wanted to say for quite a while. Despite the gap between starting and regular posting however, 10 years still feels like a gateway and something worth marking. I thought therefore that I would write something that reflects how I, my practice, and in someways the world, feels like it has changed in the last 10 years to mark the event. On the back of that, it also seemed fun to embed a few of the blog posts that have been put together since Girlymicrobiologist began in order to show how this blog too has changed and grown.
Apologies, this turned into a bit of a long one.
Microbes have changed
In 2015 I had finished my PhD in January, as well as a PGCert in Teaching and Learning in Higher and Professional Education. I had just taken my final clinical exams (Fellowship of the Royal College of Pathologists) in September and found out I’d passed them in November. After a decade of focus linked to completing what felt like an unachievable list of academic steps I was done. The question therefore was………what’s next? So, in December 2015 I started my first ever blog post, although I had been sitting on the web page for 6 months not knowing how to begin. This is how that Girlymicro blog began:
So, this is my first ever blog post. Bear with me as I don’t really know what I’m doing.
I’m what is know as a Clinical Scientist and I work in Infection Control.
Most people don’t know what a Clinical Scientist is so I thought I should briefly explain.
Most scientists that work within hospitals are involved with imaging (X-rays, CTs etc) or processing patient samples. We all work to support diagnosing patients. Did you know that scientists are involved with >80% of all diagnoses within the NHS? Their work is crucial to improving patient care, but the scientists are often unsung heroes as they often never meet the patients they help.
I do not work in the lab all the time like many scientists. I’m a clinical scientist, so half my time is spent working in a patient facing role within infection control and the other half involves bringing science to infection control to make it more efficient/evidence based. I work within a hospital with a team comprised of nurses, doctors and scientists. I have a PhD in infection control. I am also working towards my final clinical qualification (Fellowship of the Royal College of Pathologists) which is the same as my medical colleagues. My job is to help the translation of the science into a form that healthcare professionals can work with. Sometimes this means working with language so we are all on the same page. Other times this means working with the latest science and technology and developing new tests that will help.
I’m passionate about my job, but I’m also aware that many people don’t know that it exists and I’m hoping that this blog will help to change that. I plan to share a bit about what my day to day life is like as well as the science which I hope will inspire others to become healthcare scientists. After all, I have the greatest job in the world. And that is worth shouting about.
During the 10 years between setting up the website, with a world of good intentions, and writing today, many things have changed. Not least of all are the organisms people care about and the way transmission is understood. My PhD thesis was on the role of the environment in transmission of healthcare acquired infection. In many ways, getting papers published out of it was a struggle as very few journals were interested in the built environment and Infection Prevention and Control (IPC). Now organisations such as the Healthcare Infection Society run entire events linked to it, and I run something called the Environmental IPC Network, as the topics impacts so many of us. On a national level I’m now involved in writing guidelines to help support environmental IPC, all of which was a pipe dream when my thesis was being written. It felt like a very lonely area to be working in, but over the last 10 years it feels like the built environment is finally being recognised as an important component to how we keep patients safe in the world of IPC. I’ve now even had my own PhD students continue the work.
The other thing that has changed are the organisms that are perceived as being important. Even more though, there are organisms that were not even thought about in 2015, or didn’t exist, that can or are impacting so many lives, for instance Candida auris is a new kid on the block, and Mpox was called something completely different. Few people cared about Gram negative bacteria when I started my PhD, let alone Adeno. This was true even to a certain extent when I finished. I’ve worked on Adenovirus for over 2 decades, so it feels especially vindicating to see it make it onto the UKHSA priority pathogen list for research. All of this is to say, you don’t need to follow the crowd, if you find a problem that you believe is important enough, stick at it. Gather the evidence and put it out there. Eventually you’ll find others that join you in seeing the significance of your direction of travel.
Speaking of organisms, in 2015 we testing for the odd Coronavirus, and of course the severe acute respiratory syndrome (SARS) outbreak had happened, and the Middle Eastern Coronavirus (MERS) outbreak was ongoing. Many of us had been concerned with the potential of Coronaviruses to cause a pandemic, but most of the planning was still linked to Influenza based risks, as that was what had been seen historically. Awareness sadly does not necessarily link to preparedness, and as lived experience shows, the SARS CoV2 pandemic was both fast and devastating. We were unprepared, but I don’t know that we ever could have been.
Outbreaks with a worldwide distribution are not unusual and the table below shows just how many have happened or have been ongoing from 2015 onward. It also shows that not all outbreaks with world wide spread are considered to be pandemics, and not all pandemics have death tolls in the millions. In fact a pandemic is defined as “an epidemic occurring worldwide, or over a very wide area, crossing international boundaries and usually affecting a large number of people”. With this classical definition including nothing about population immunity, virology or disease severity. So, preparing for a pandemic is not as simple as it can initial appear.
NB for ease I grabbed this list from Wikipedia, please don’t judge me for it
The table also shows quite how hard life can be in the world of IPC as the organisms don’t stop because we are tired and need a break. In fact the world re-opening post pandemic, combined with some of the scientific distrust that the political handling of the pandemic created, and the fear people experienced, means that managing outbreaks since has been an ongoing struggle. Vaccine hesitancy is having a real impact on transmission and making a key line of defense less effective. Many experienced experts in this field and others related to infection and public health have now retired or moved away due to the ongoing personal impacts. This means it’s more important than ever to turn up, be seen and to have engaged conversations across boundaries and silo’s in order to develop trust and support patient safety. No matter how hard it feels, it is still worth it.
My clinical world has changed a lot, partly because of the changing organisms and the pandemic, but also because the patients and healthcare are changing. It can take quite a lot to keep up with all of these changes, and you have to be fully engaged with an approach that aligns with continuous learning to stay up to date. On top of this, when you start out as a trainee with over a decade of training ahead of you, you have also got a list of key education targets to prioritise. It can therefore feel very much like you are just working your way through a list of items that need to be ticked off so you can eventually get to the finish line. There is a lot of ‘onto the next thing’ as soon as you manage each key milestone because otherwise it can feel overwhelming. One of the key things I’ve realised since 2015 is the importance of cherishing the moment and recognising the importance of progress, rather than rushing from one thing to the next with my entire focus about keeping an eye on the prize.
Passing FRCPath first time is still one of the most challenging things I’ve done in over 2 decades in healthcare. To be honest, I’d rather do another PhD than take FRCPath again, any day of the week. I wish that I could have found a way forward where I didn’t let my ability to pass, or risk of failure of an exam define me, but for many years it did. I’m pretty sure that telling my younger self this would have achieved nothing, as it takes time and distance to be able to understand that the tick list isn’t everything, but just in case it helps anyone reading this……you are more than the sum of the exams you sit, the letters after your name or the achievements on your CV. You have value no matter where you are on the pathway, no matter how many diversions you have taken, and to be honest, it’s OK to also decide the end destination is no longer for you. Who you are matters more than any tick list.
Part of the way I’ve gained perspective on my own training is by supporting others now through theirs. Seeing PhD students go through their own trials and tribulations, and sharing in their eventual successes., has given me insight I couldn’t have gained any other way. Supporting Healthcare Science training, everywhere from writing curricula to mentoring individuals at all stages of their careers, has allowed me to see things from all kinds of different perspectives. It’s given me so much insight, as well as time to reflect on how I felt and what might have helped me along the way, in order to try to help others better.
I feel more seen as a Healthcare Scientist than I ever have. I feel that Healthcare Science as a discipline and a profession is more seen than it ever has been. There are so many more routes into Healthcare Science these days, with so many more options. This is a truly brilliant step forward from when I joined, when there really was only one route as a Clinical Scientist and having to really fight to show that you could do things differently if you wanted to go another way. As the same time however, all that choice can feel a bit overwhelming, and in some cases paralysing, as people just don’t know where to start. In order to reach more people and support them in navigating this changing landscape though does require a willingness to be visible, to bring ourselves and our stories, in order to show others what an amazing profession this is. To show the openness and diversity of the workforce, in order to make sure everyone knows this can be a profession that is welcoming and open to everyone. You can’t be what you can’t see, so let’s make sure we are seen!
I have been fortunate enough to have experienced opportunities that I never believed would be open to someone as normal as me. I don’t come from a privileged background. I didn’t go to private school or attend Oxbridge. I don’t have connections, or a rich family to bail me out and pay for my exams/conference fees/fancy memberships. So when I get invited or asked to do amazing things, I of course say yes, but I’d think to think I’m saying yes for more than just me. I’m going into spaces and having conversations with people so that I can represent. Represent my workforce. Represent my gender. Represent my background and represent my family. To do so is an immense honour and a privilege that I don’t ever lose sight of.
No one I knew, outside of work, had ever had a New Years Honour, so it never even occurred to me I would get one. Being able to undertake work in Africa which aims to reduce infant mortality by 20% in high mortality settings, is not work that I thought I would ever get involved with, it felt too big for someone like me. That’s just it though, ‘someone like me’. We put so many labels and restrictions on ourselves. We limit our own vision. If the last 10 years have taught me anything it’s that you probably can’t see where you will end up, there’s too much joyful chaos in life for that, but you can control saying yes. Saying yes to things that scare you. Saying yes to rooms that may intimidate. Saying yes to being open to opportunities and changes in direction, even when you have no idea where they might lead you. Half the joy is in the discovery, so put on that adventure outfit and head out the door.
I’ve talked about the tick list and why visibility matters, and not just for you as an individual. Now I want to talk a bit about glass ceilings and choosing to do things differently. I have, over the years, lost count of how many times I have been told that something wasn’t for me. Not for me because of my background, profession or gender, or maybe just because I didn’t fit in. I used to hear a lot of ‘no’ and I used to feel like others could define me. The thing I’ve learnt is, that the only person who can define you is you. You can give away your power to others and let them made those choices for you, or you can own your path, your career and your choices, in order to define yourself. I’m not saying any of this is easy. I’m not saying it is fast or straight forward. I am saying it is a choice.
I became the first non-medical Infection Control Doctor (that I know of), because I worked to create the path to get there, which hopefully others will now follow. I didn’t know that was possible when I started, and it came with a goodly number of fights along the way. There were days when I definitely believed the ‘no’s’ and didn’t think it would happen, but I kept trying, I kept showing up. It became clear that I would never make Professor at my original home within UCL, due to long standing bias for medical over scientific backgrounds. So I pivoted and found a new academic UCL home that welcomed me and supported me in my journey instead. Things that are worth fighting for take time and commitment, and nothing is guaranteed. Paths are often not well trodden, and so finding the right people to support you along the way is key. Don’t drift. Make your choices consciously. Know what you are willing to fight for. Know also what you are prepared to let go of. When things come together share the knowledge, share the path, and make it easier for others to follow. Drop that ladder down or prop the doorway open.
I had thought it was post pandemic blues but I think it’s just transitioning to another phase of life and career that got me thinking about this one. I’ve been working at GOSH for 21 years this year, pretty much my entire working life. During this time there have been two mentors that have pretty much introduced me to and gotten me through everything. In my clinical life it has been Dr John Hartley, and in my academic world it has been Professor Nigel Klein. Now, John retired part way through the pandemic, and he really is the reason I have my Consultant post, as I took his Infection Control Doctor role. Nigel sadly passed away last year, before he had the chance to retire. In my head, I’m still the new girl on the block, the new person in the department, the young upstart. It is a shock to look around and realise I am now one of the people who have been there longest and I have very large shoes to fill, knowing how unprepared I feel to fill them. The giants that have gone before have left, but I wasn’tt prepared for them to leave. I think the biggest shocker has been that there are some who now look at me in the same way that I looked at John and Nigel, when I don’t feel like I am even in the same league. I think they will always loom large in my mind, and I honour what they taught me by embedding it in my practice.
Your career can feel like such an open pathway ahead of you. Then you wake up one day and realise you, probably, have less than a decade left. It’s at moments like that you really need to think about what it is that you want to achieve, what you want to prioritise, in order to maximise the impact of the time you have left. Ten years feels like a long time, but its really just 2 cycles of PhD students, 2 large project grants and only 3 trainee Clinical Scientists. It’s no where near as long as it feels and so planning ahead takes on an all new perspective. If your a planner like me, now is the time to plan for this new phase of your career.
Learning that you can’t fix everyone or everything
Part of that planning for the future is also knowing what not take on. I am a simple soul, I like being liked. It’s taken me a long time to grow in my leadership to the point where I acknowledge that I not a god, and I don’t have a magic wand, therefore I can’t fix everything or everyone. Nor can I be liked by everyone. Part of being a leader is making tough decisions, part of being a leader is also about honesty and not saying the easy things, just to be liked. Sometimes, I have learned, putting off the difficult conversations and the difficult decisions does no one any favours and so it’s best to have them early. As a mentor, you are there to advise, but the decision are owned by the person making them. You are not people’s parents and they are not children, we should therefore be aiming for adult adult conversations. Acting like a White Knight can actually do more harm than good, as you are removing learning opportunities for those you swoop in and save. It is a difficult balance to know when to step in and when to maintain a pure supporting role. It is one that I will continue to get wrong. All I can do is learn, do my best, own the consequences, and aspire to be better.
The flip side of learning you can’t fix everything is being aware of your duty to try to make things that are in your remit of control or influence as good as they can be. As I’ve said, I have a decade left in all likelihood, and therefore my job is to ensure that I maximise the opportunities for others until the day I don’t have the ability to influence any more. My career is very much no longer about me, it’s about those who I will be leaving behind to carry on once I’m writing murder mysteries and drinking martinis at three in the afternoon. My job is to support as many people as possible to be in the best position possible when I walk out the door for the last time. I realise it’s now my job to keep the doors open and assist people through them. Whether it’s mentorship, nominations, or speaking peoples names in rooms they haven’t been invited into, I plan to do all I can to make sure that I pay it forward every opportunity I get.
I have the job I planned for and dreamt about for 2 decades. It is my dream job and I love it I wouldn’t change it or my decision to go for it for the world. There is no doubt however that post pandemic it has been hard. I don’t know if it’s because I’m getting older, because the job and the world right now feels pretty intense and hard core, or because my body still kind of hates me for what I put it through during the pandemic, but I definitely feel burnt out and recognise that even a dream job can be a lonely place to be.
The thing is, not every day is going to be a great day. Even in a dream job there will be bits that are harder or speak to you less. It’s also OK to not be OK. The world, and especially those of us in infection control, have been through a prolonged period of pretty significant stress and trauma. We are not going to be the same people we were going in. You don’t have to change the world every moment of every day, sometimes showing up and doing your best is enough, and what your best looks like will be different at different times. I have learnt the importance of asking myself, what would I say to a friend in this situation, and to show myself the kindness that I would show to others rather than acting as my own harshest critic. Try to take a step back and give yourself the prospective you need to find a route forward.
Just the act of writing this post has made me realise how far I’ve come. If you’d asked me in 2015, I would have said being a leader is about setting an example, about getting things right, about showing competence and keeping a cool head. I’m sure leadership is about some of those things, but what I have learnt, for me, is that leadership is about authenticity.
It’s about prioritising bringing my whole self to every encounter. It’s about saying sorry when I make mistakes, rather than pretending to always be right. It’s about sharing that I too am finding it hard, rather than pretending to be OK, but that success is about showing up anyway. It’s about the fact that some people will find this bringing of self about sharing of weakness and use it as a route to criticise, not everyone will like or even ‘get’ what you bring to the table. It is also about knowing that you don’t have to like or be liked to work with others, but that it is instead about developing shared goals, and that diversity of thought makes us stronger and not weaker. Finally, it’s about knowing that it can be scary to share who you truly are as the comments and the insults hit harder without having an armoured shell in the way. However, if you don’t show that you can bring your whole self to a space others will feel less able to do so. Creating safe spaces where people can truly be themselves is one of the greatest things we can do, and so we need to model the way forward so that others don’t have to take that risk instead of us.
Of all the posts I was most scared to share when I wrote it in April 2021 was the one where I talked about losing my sister and how it felt to know that I wouldn’t be able to have children on top of losing her. It was one of the first really personal and vulnerable posts that I put out and I was really scared of what the response might be, both from family and from strangers. Instead, it was shared more times than any other post, and people still come up and talk to me about it, my sister, and Morgan my niece, who we also lost. Something that terrified me, led me to being able to talk about something that impacts so many and is talked about so little. Sharing, was a bravery I don’t think I would have managed in any other way than on this blog, and having conversations with people who read it are so meaningful to me, even now.
More recently I shared a post about what it feels like now, over 10 years since losing my sister. I really wanted to post how something that feels so insurmountable, in terms of not having children when you wanted them, can actually turn into something where your life still has so much meaning and joy. A position I could not have even imagined in 2010 when I lost them. I truly, honestly, love my life. My life has meaning and I have achieved things that I’ve been forced to admit would not have been possible if my life had taken a different course. I hope that sharing this can help others who are not there yet to know that there is a future where they will smile, laugh and feel valued again, no matter how dark the moment feels.
I’ve always been a family girl, but I’ve not always prioritised them in the way that I should. I’ve missed funerals and weddings for work. I’ve cancelled dinners and missed trains home. The pandemic, and life in general, has made me decide that I need to put my family first, and thus myself. There needs to be balance to make it through the marathon of a healthcare career, and some of that balance requires that the job cannot always be the thing that defines who we are. Mummy and Mr Girlymicro are my world, and every moment spent with them makes me a better person and thus better at my job. Bringing my whole self to my job and my leadership requires me to nurture precisely that, my whole self. So credit where credit is due. My family support me in being able to do what I do. They make me martinis when I’ve had a bad day, give me water when I’ve forgotten to drink, and feed me when I’ve inevitably forgotten to eat. They love me for my flaws as well as my strengths, and put me back together when I break. They are my everything, and so they need to feel like my priority in life. I guess my learning is this, don’t become so focused that you forget to acknowledge the people that got you there, and don’t be so ‘eyes on the prize’ that you forget to enjoy the journey with those who care.
Last, but by no means least. I have learnt to embrace the unexpected. I’m a planner but when I started posting on this blog I didn’t really have a plan. I had no idea where I was going or what I was doing. I just knew that it felt like it was something that was needed and had been asked for as part of a challenging time when people were looking for information. It was something that was supposed to be a little hobby that unexpectedly became a central rhythm of my life. Something that is a focus of a little time every day. Something that feels mine when less and less of my working life feels that way. It’s a space where I really feel I can connect, in a way that is probably a little insane for something I throw onto a page and don’t see people read. None of this was planned, and yet it has changed my world. It has changed my plans for the future. It has given me a creative outlet, and some hope in pretty dark times. So, if I have a thought at all for you to take from this overly long blog post, it is this. Embrace the random moments that come your way. Embrace the actions that you roll a dice on and don’t think will lead you anywhere, because every once in a while, without you even being aware of the whys or the how, they may change your life for the better.
It’s the 8th March, and we all know what that means…..It’s International Women’s Day!
This year, International Women’s Day is timed pretty wonderfully for me, as it happen to also be just as Healthcare Science Week is about to kick off. As both a woman and a Healthcare Scientist, I thought this was a great opportunity to combine the topics and talk about how these two things have impacted how my science career came about, and why I think a lack of recognition of both has incredibly important impacts on society as a whole. That said, this is also a post about how far we’ve come and the role that female scientific representation in the media has, and can have, on how we feel seen as women in science.
In what feels like a different life, where I was younger and had better hair, I was selected by the Royal Society of Biology to do some filming linked to raising the awareness of women in science. The session is short but was really interesting for me to do as it centered on who inspired me to become a scientist and how it happened. Now, many of you who read this blog will know all about that tale, but for context, I’ve linked to the video below:
The thing is, I suspect that there are still many people out there who might love to do science, and yet they’ve never had the chance to meet a scientist or really learn about the brilliant variability of a career in STEM (science, technology, engineering and maths). So what’s my point? Getting to actually meet and chat with a real scientist still feels like it’s a thing for the privileged few, not something that is available for mass consumption. You know what is available for mass consumption? TV and movies. This blog reaches 20 odd thousand people a year, a single episode of a TV programme, like Holby City, makes those numbers look so small they are not even worth considering. So it matters that the roles of female scientists within movies and on TV have not always been the most representative of either the careers available or the type of people that choose to engage with scientific careers. The reach and expectation setting that the media can have dwarfs any of the best efforts I can make across my entire career. Therefore, in order to celebrate International Women’s Day this year, I thought I would take the opportunity to talk through where we started with some of this representation in TV and the movies, and then celebrate quite how far we have come.
Why is it important to have women in science?
I kind of don’t believe I’m writing this section. This one should be a no brainer and yet I think it’s probably important to take a paragraph, especially with all the current commentary about equality, diversity and inclusion (EDI), to talk about why EDI matters.
The data supports the fact that we are far from a scenario where female representation in the workforce mirrors the distribution of women in the population. Worse than that even, is the fact that even if women make it into STEM careers they are doing less well than their male counterparts, including lack of representation in senior roles and general reduced access to research funding. There will be another post at some point about the source of some of these discrepancies but hint – it’s not because the women are worse at their jobs, that blog is still a little way away however.
One of the reasons for the lack of of women in STEM careers is that, according to work undertaken by Steinke et al in 2007, children are exposed to gender stereotypes and images of scientists through movies, TV shows and books where there is a lack of good representation of female scientists. They undertook work with primary school children where they asked them to draw a scientist, very few children drew female scientists and most listed media as the source of their inspiration. A similar study in Korea, in secondary school children, showed that only 16% of them drew female depictions of scientists. This kind of data backs up why media representation is so important, as you really can’t be what you can’t see. So many children do not realise that a scientific career is even a pathway that is open to them, if they are not fortunate enough to know one. If children can’t access what that career might look like through the information sources they access all the time then they don’t even consider it as an option for them when making their life choices.
But why should we care that we have less women working in science? What kind of difference do they make that we should try to move the dial on this?
Women make up just over 50% of many populations but much of the data produced by scientists, including clinical trial data, is biased towards male datasets. This leads to the outcome data for females often being less good. Some of this is likely due to a lack of female voice in the room when studies were being planned
There is often a research bias, where issues that purely impact women tend be under researched compared to issues that purely impact men
Inclusion of women in tech pipelines has been demonstrated to improved productivity and boost economic outputs
Science should be for everyone and therefore needs to include everyone. Science is best when it is seen through different lenses and priorities which different individuals bring to the table. Variable opinions drive improved change and innovation, so being inclusive is a win win
By increasing female representation in STEM we can switch up our focus from working to increase diversity and spending energy on being visible and role modelling, jobs that are overwhelmingly undertaken by women in STEM fields in addition to their day jobs, and allow women to compete better with their male colleagues by freeing up their time to focus on their science
What kind of representation did I see in the media when I younger?
Having talked about how important exposure to role models in the media are to encouraging women in STEM, I wanted to kick off by talking about the kind of representation I was aware of when younger and making decisions about my career choices. Now, a key disclaimer here, it appears that my teenage years were some horrific length of time ago, even though I’m blatantly still young, spry and filled with youth. Women, especially those in technical roles, often weren’t featured or were there to act as passive objects for men to respond to or act around. They were all too frequently there to be a foil for the men who were the focus of the storytelling. There wasn’t an abundance of female science representation in any of the media that I do remember, but what was present used to focus on 6 key stereotypes:
The Old Maid – the female scientist who is only interested in her work (and therefore not showing that you can be both a scientist and a person) who, as the film/show proceeds, has her female and emotional side brought out by the main male protagonist
The Male Woman – a female scientist who works in an all male environment. She is not as sexual a character as other women in the setting may be, but she is also not on the same level as the men she works with. She is often presented as having unhealthy habits, such as drinking issues, in order to show (it feels to me) that it’s unhealthy to try to be a woman in a mans world
The Naïve Expert – often a character in a film that is critical but does not contribute to any of the science solutions or really advance the story in any way. These often feel like box ticking roles or to aid the exposition of other characters
The Evil Plotter – usually a young and beautiful character who is there to trick the men within the film. They are set up to be hated by the both the other characters and the audience as they use their scientific knowledge and looks for evil. This one again strikes me as a way of demonising women who bring anything other than their knowledge of science and dare to be people with other needs as well
The Daughter/Assistant – this one is the typical smart and capable woman who is there as a subservient to a smarter, more well known, or more significant male character who will be the one to advance and resolve the plot whilst the female is there as a foil to show how smart and capable the male protagonist is
The Lonely Heroine – a woman who is depicted as intelligent and independent, and allowed to also be sexual, but somehow is not able to compete with her male colleagues. Usually, during the course of the story, she is gradually able to be seen and have an impact but only when she develops a relationship with a man who allows her to be acknowledged by others
Now, don’t get me wrong, all media and story telling is based on stereotypes and tropes, almost everything can be fit into a silo. That said, if the stereotype is only there to serve the male protagonists of the tale, that is a problem and it very much felt that way in films and programmes I watched growing up.
Scully effect
So what changed? I remember so clearly my first encounter with the The X-Files. It came out in 1993 (1994 in the UK) and I kind of missed it, but my sister and brother would not shut up about how great it was, so it took a while for this geeky 15 year old to discover Dana Scully and all of the science joy she would bring to me.
For those of you who don’t know anything about The X-Files (and you really should) according to Wikipedia ‘The series revolves around Federal Bureau of Investigation (FBI) Special AgentsFox Mulder (David Duchovny) and Dana Scully (Gillian Anderson), who investigate the eponymous “X-Files“: marginalized, unsolved cases involving paranormal phenomena. Mulder is a skilled criminal profiler, an ardent supernaturalist, and a conspiracy theorist who believes in the existence of the paranormal, whereas Scully is a medical doctor and skeptic who has been assigned to scientifically analyze Mulder’s case files.’ The reason that this series made such a difference for me, was because it was the first time that I saw a fully rounded female STEM character who was a person, with interests outside of her job, who was also an equal player in the story and able to challenge and lead within the series framework. She was more than just a foil, or a tool for exposition, and the number of times she was the one that did the saving became somewhat of a running joke.
It wasn’t just me that the character of Dana Scully had an impact on, her character led to what has been described as the Scully Effect. The Scully Effect refers to the phenomenon where women were inspired to pursue careers in STEM after watching The X-Files. This was the first time I think I really became aware of the power of the media to impact in more than a superficial way. The impression of this effect has been upheld by a recent study to try and capture some of the way that the Scully Effect impacted on those who watched the show, so you don’t just have to take my word for it.
There is no doubt that the role of Scully in The X-Files felt like a watershed moment for featuring women in STEM careers. Having just talked about the difference that Special Agent (Dr) Dana Scully made in terms of female representation in science I’m now going to excluding medics from the rest of this discussion as a) they are featured much more frequently in all forms of media and b) the lack of female scientific representation is one of the reasons that students see medicine as the only route open to them, rather than seeing the world of opportunities available within the world of science careers. (I still love you Dana, you’re still my girl)
So where did the change in TV go from there? Now, there are a few honorable mentions I’d like to give a shout out to, these are obviously based on my person taste, but I do think they are examples where things have continued to change for the better:
Bones is a police procedural linked to investigations of human remains undertaken by Professor Temperance “Bones” Brennan (Emily Deschanel), who is a forensic anthropologist, supported by FBI Special Agent Seeley Booth (David Boreanaz). Now, in many ways Bones fulfills many of the Old Maid stereotypes, but there are many key differences. For one, her intelligence is always held up as a positive and with high regard, and she is considered to be so valuable that her challenges with more emotional interactions are considered to be over whelmed by the value her intellect brings, which is quite a different take. Secondly, her emotional journey is mostly chaperoned by another female character in the show, Angela Montenegro, rather than relying on a male character for their character development (yes, yes, I know her and Booth get together but I’ll die on the hill that it’s secondary to Angela). Finally, and maybe most importantly, the character of Bones is very clearly signposted as being based on a real person, Kathy Reichs, who was also involved in making the show. As I said, representation is important and the fact that this clearly shows that you can be a successful scientist, and perhaps even close the circle and be inspiring enough to have a TV series based on you to inspire more young people, is a massive step forward.
Kathy Reichs
Two other TV science representations I love come from other police procedural or fantasy series, both are lab guys, all of which probably tells you a lot about who I am. These guys both speak to my heart as they are fully formed characters, not just single dimension caricatures of female scientists. They have flaws, they have passions, they are authentic, and most of all they love the science that is their calling. (this isn’t to say that science has to be your calling for it to be your job, I just love that there are representations of scientists on TV who love science the way I love science)
First, I’m kicking off with Abby Sciuto from NCIS. She’s a forensic scientist, who in that TV way has a world of completely different science skills rolled into one, but I still love that about her as she exhibits so much scientific curiosity. As an ex goth myself, one of the other things I love about her is her sense of self expression and not being limited or making herself smaller on the basis of what others think about her. She the opposite of those female scientific characters who rely on others to enable them to be people rather than lab coats. I fully respect and am so happy to see this kind of female science representation.
Second, is Ella Lopez from the TV series Lucifer, a TV series based on a comic where Lucifer, as the devil, abandons Hell to run a nightclub in Los Angeles. He then (for plot reasons) becomes a consultant to the LAPD and hi-jinks ensue. She’s also a forensic scientist who works for the LAPD, are you sensing a theme? I don’t know whether this is because of the kind of series I like, or whether the writers of these kind of series just feel like they have more time and scope to devout to full character representation. The reason I love Ella is that she is the complete opposite of the Old Maid/Male Woman stereotype. She is the emotional heart of most scenes, and is accepted for bring her full emotional quirky self to the table. As someone who often feels judged for wearing her heart on her sleeve, I love this is represented as a strength in this characterisation of a female scientist.
Let’s talk movies?
So what about the movies? In some ways female scientific representation is always slightly more challenging in films. Slightly due to the nature of the medium, there is often less opportunity for character development (as you have a few hours vs multiple episodes) and so they still tend to fall very much into some of the stereotypes already discussed. There is still a strong tendency for strong female characters, when present, to still fulfill the Evil Plotter stereotype, and the film industry in general struggles to have female roles that are not reliant on male roles for context. That doesn’t mean there are not plenty of films despite this that have female characters I enjoy (Jurassic Park and Contact being just 2 on the left of the image below).
In terms of movies I want to discuss though, let’s start with the one on the right, Dr Elizabeth Shaw from Prometheus (2012). Those of you who read my Halloween blog on how the Alien movies reflect the world of Infection Prevention and Control, will already know how much I like this film series. One of the reasons the series appeals to me in general is that it doesn’t shy away from strong female lead characters, it started with Ripley after all. The female lone survivor trope is strong with this series, but I also like it when characters like Elizabeth are the ones that survive because they don’t shy away from their intellect and aren’t scared to be the smartest person in the room. Too often we hide away from owning our space as women, and I love a film where the characters are given license to own their space.
Talking about films where women are given permission to own their space, this next one is based on historical figures. My favourite female scientist movie of all time is hands down Hidden Figures, which came out in 2016. This film is loosely based on the non-fiction book by Margot Lee Shetterly and is about three female African-American mathematicians: Katherine Goble Johnson (Taraji P. Henson), Dorothy Vaughan (Octavia Spencer), and Mary Jackson (Janelle Monáe), who worked at NASA during the Space Race. If you haven’t seen this film I cannot recommend it enough. When I have bad weeks this film reminds me of the fights that others have fought just so I can occupy the space that I’m in, and the continued need to be that fight for the generation that will follow me. It’s about so much more than female representation, some of the challenges that these women faced due to the colour of their skin is mind blowing to someone growing up in the UK, not to say that there are not ongoing diversity and inclusion issues here. This film to me is everything that science representation on the big screen should be, and it’s just a pity that there aren’t as many examples as can be found on the small screen.
All hail Marvel
All this brings me to the one place that I feel consistently hits it out the park for me in terms of both female character representation and in showing scientists as real three dimensional people, Marvel (both Marvel Cinematic Universe and Marvel Studios). Personal opinion, but I feel like Marvel have done more for showing women who are scientists and characters in their own right than most other genre series, an irony I am aware of for a series based on comic book characters. This is probably made possible because they can draw on character development from so many decades of story lines in order to make it work.
My all time favourite is Dr Jemma Simmons from the Agents of SHIELD series, but that could be because you are able to get to know the character over 7 seasons. Film wise, I really love Dr Jane Foster from the Thor series. Previously my all time favourite film science character was Shuri from the first Black Panther series, I’m pretty conflicted about this now however due to some of the anti science opinions held by the actress.
There are frequently great scientific characters embedded across all parts of the Marvel universe ,however, and so I encourage you to find your own favourites. To help I’ve listed some of the big hitters, in terms of main characters, below.
Thor film series with Dr Jane Foster
Agents of S.H.I.E.L.D. TV series with Dr Jane Simmons
Ant-Man (and the Wasp) film series Dr Hope van Dyne (and Janet van Dyne)
Doctor Strange film series Ms Christine Palmer
Spider-Man film series (not actual scientists as too young to have careers but….) Mary Jane Watson
Black Panther film series Shuri
Captain Marvel film Dr Wendy Lawson
Eternals film, possibly all of the film characters as they are after all eternal
Another thing that I appreciate about the Marvel films is that even when a character is not present, due to them being part of another story stream, they often reference the absent character, and not just in a way that talks about their positioning linked just to a romantic other. One of my favourite examples of this is below, from Age of Ultron, and is part of a conversation about why Pepper Potts and Jane Foster are not at a party. The dialogue goes like this:
Avengers: Age of Ultron (2015)
If you are looking for something you can watch with your family, that will hopefully inspire the next generation of scientists, and help ensure that the next time a child is asked to draw a picture of one they may choose to draw a woman instead, this is a great place to start.
I feel we’ve come such a long way in terms of female scientific representation in the media, but there is so much more that needs to happen. We can all work to drive this by being aware of the films we choose to watch and where we decide to spend our money. Those of us working in science can also do a lot to make sure that we take opportunities presented to us that mean we will be seen, and hopefully inspire those who will follow us. Let’s embrace the moment, step out from the shadows, and truly show why having women in the scientific space is crucial for the best science to occur.
Thank you for taking some time out of your day to share International Women’s Day with me!
I’m back from a lovely week away at Disneyland Paris, celebrating Christmas and escaping reality (a post on Disney and denial as a coping mechanism is on its way). Whilst I am still struggling with the return to reality this weeks blog post is supplied by the wonderful Callum Barnes. Callum is a disciple of the biomedical sciences, current master’s student creating a more authentic lab experience for those after me, aspiring consultant microbiologist (the best discipline, sorry Claire – you see he understands, like me, that micro will always trump immunology).
Callum is supervised by Dr Claire Walker who is a paid up member of the Dream Team since 2013, token immunologist and occasional defector from the Immunology Mafia. Registered Clinical Scientist in Immunology with a background in genetics (PhD), microbiology and immunology (MSc), biological sciences (mBiolSci), education (PgCert) and indecisiveness (everything else). Now a Senior Lecturer in Immunology at University of Lincoln. She has previously written many great guest blogs for The Girlymicrobiologist, including one on turning criticism into a catalyst for change.
Two years ago, I began a placement year in the microbiology department of a pathology lab, unsure of what was to come, and unsure of myself and my skillset as a scientist. As I think every scientist feels at some point, I was mostly concerned that I would be a hinderance to all the wonderful staff that were just trying to get on with their jobs. Everyone was amazing though and helped me develop the skills and confidence I needed to successfully complete my IBMS portfolio verification. Returning back to university for my final year, I found the lab-based work so much easier than in my second year with my experience, but… something was different. This wasn’t the same stuff I just spent the last year working on, where was the LIMS? The booking in of the samples, the investigative process and the, frankly, the occasional chaos were missing. That’s not to say the labs weren’t good – they were great – and the staff that developed and ran them miles better, but something felt like it was missing. And that’s when my now supervisor Dr Claire Walker came to me with a project for my Mbio year.
Claire and I both have experience in the NHS, herself a lot more than me, but we have both felt and experienced the environment that a pathology lab has. It has a very unique feel to it, slightly alive in my opinion. This is not a very common experience to have in academia though as most academics have a research background, which means that the practical pathology side of things can sometimes get lost when students do their practical work. As such, Claire and I have been working on creating a lab experience that is as authentic to an NHS pathology lab as possible.
But why even bother? The students are learning the same things, just in a different way, so does it really matter? Well in fact, yes, it does! As Claire has said previously, the pilot study she did had very good results, so the data is there to back up our work. But imagine for just a second that you are looking at applying for medicine, and you have two offers. One university offers a fully simulated experience using manikins and actors – the whole shebang. And the other university teaches mostly through theory and shadowing – no practical experience is offered. I know which course I would enjoy and learn the most from. Medical schools know this too and is why most of them offer simulated teaching – it makes for better doctors too.
So, we should really ask, why isn’t this offered for biomedical scientists? Maybe it’s cost, maybe there isn’t the associated prestige. Whatever it is, I am sure that our work will guarantee a truly authentic clinical laboratory experience here on the iBMS accredited course at the University of Lincoln – something I know will provide the right skills for the pathologists of tomorrow.
Back in the mists of time, before she really knew what microbiology was, there was a girl who just knew that she liked science. Now, this girl had a father who liked physics, a sister who liked chemistry, and a brother that liked both. This girl was not particularly found of mathematics however, and chemistry was a foreign language, and so she starred in the lab and wondered,’What kind of science is right for me?’.
I have previously posted about having missed so much school and not really being prepared to go to university. I didn’t, therefore, have exactly the most normal build-up to uni as I didn’t think it would happen. In a rather spectacular science irony, when it suddenly turned out I might be able to go, I just hadn’t done my research. I didn’t have much of a clue what my options or routes to a scientific career might be. Hopefully if past me found my how to be a scientist blog it would be a useful starter for 10. In my defence, at least I acknowledged this, and so I chose a degree that allowed me to specialise after my 1st year, when I would have had time to try out a few potential options.
One of the other things I should probably admit at this point, is that lab work terrified me. I hadn’t been in the class room when people were shown how to use microscopes or pipettes, and I was just too embarrassed to ask as I already felt both stupid and so behind everyone else. I’d done very little lab work as I’d missed most of my 5th year at school, and during my A-levels I had to undertake condensed study to make sure I had enough points to go to uni. So the idea of spending a lot of time outside a traditional lab space definitely held appeal, as it felt like I was finally starting at the same point as everyone else.
So this girl finally chose her specialty and worked super hard to be accepted onto the zoology course.
All of this feels like a different world at this point, over 20 years on. As some of my team love to point out, I started uni when they were still at primary school (1999). These years were so formative however for how I developed as both a scientist and a person, I was so excited to be able to revisit the subject when I spent a night at ZSL London Zoo with Mr and mummy Girlymicro and remind myself of days of science past.
What is zoology anyway?
When you say Zoology, I suppose the first thing that springs to mind are zoos. Now, you may find quite a lot of zoologists in and around zoos, but this is actually just one place place where the study of Zoology happens. In fact, zoology is so much more than the study of animals in zoos. It is, in fact:
The scientific study of the behaviour, structure, physiology, classification, and distribution of animals
I was aware that the area of animal behaviour really interested me. It was something that I’d touched on during psychology A-Level, and that then extended into human behavioural modelling with things like group decision making. Comparison of group behaviour between primates and other animals and how attachment develops between adults and infants was something that I found fascinating. This was, for me, the gateway that made me think about choosing Zoology, but there was so very much more to it than I knew at that point.
Because of this, when we arrived to spend the night at London Zoo, I was particularly excited as the lion enclosure had just welcomed three cubs, one girl and two boys. Mali and Syanii and girl Shanti were born at London Zoo on 13 March 2024 to seven-year-old mum, Arya, and 14-year-old dad Bhanu. The first thing we got to do was to spend some time after the zoo had closed watching them at their most active, as it was evening, in a small group with one of their keepers. We got to drink prosecco, take all the photographs we wished, hear a talk, and pepper them with questions. It was a truly wonderful way to kick off the evening. It was also as far away from my old zoology field trips as you can imagine, where as a student I would find the most comfortable spot on the ground I could in order settle in for the next eight hours, with a pile of stationary and a timer, nursing a bottle of water and a sandwich so I didn’t have to leave my space until I was done.
What was the degree like?
One of the great things about the degree was that, as long as you took the correct modules for your target specialism, you could try all kinds of science topics, especially early on. So, as well as modules on invertebrates and ecology, I also took modules on psychology and microbiology. In my first year, although I feel it disliked me as much I disliked it, I also took mandatory modules, which included Biochemistry. That first year was a whirl wind of things I was unfamiliar with. It was also the year that, although I thought I liked human genetics, I discovered that it really wasn’t the field for me. I learnt a lot about how I think and what kinds of topics align better with how that process works for me. A version of the course exists even now if anyone is interested, although I suspect it has moved on somewhat:
Now, I was still terrifed of lab work and so the fact that some modules came with weekend field trips rather than traditional lab work made me very happy. There were also other kinds of ‘labs’ which involved a lot of drawing of skulls and anatomy, where I discovered I hadn’t missed my calling as an artist.
There were also some super super fun exercises that I remember fondly even now. At one point we were sent out to learn how to capture and undertake population statistics by recording taxi cab license plates (as they link to age) and working on the population stats of births and deaths using this. I found a lovely window in a McDonalds and stared at a taxi rank for a day chatting with my friends, and it was great. These moments really taught me that science was not all about lab work, as I had previously thought, but it could be undertaken anywhere and in a way that was not only interesting but also enjoyable and fun.
One of the other things this course taught me about myself was that I like to take the less trodden path. For my final year dissertation, I could have taken a lab based project, but I still wasn’t that confident. Instead, I chose to do a library based project with a twist. The library was the British Library (https://www.bl.uk/), and the project was based in evolutionary psychology looking at The Demographics of Witchcraft Accusations (1625 – 1720). I got to go through every documented witchcraft trial in England and then look at the legal changes that drove resource competition and compare it with the US and Europe, where the drivers were different. This exercise stays with me, as it showed that no matter what the outward appearance, you always need to understand the underlying drivers to fully investigate a situation.
Moments that stay with you
I’ve already said that my aim was always to choose Zoology because of my interest in animal behaviour, but it was a pretty competitive selection process. Places were allocated to specialisms on the basis of a combination of choice and grade. So the top person in the year was guaranteed their choice of degree, if you were 300th, not so much. I believe my 1st year had over 1000 combined students, and the bottom 50% were dropped every year, so the year group size got smaller but was still competitive. Dissertation topics were given out in the same way. So there was an ever-present motivation to work hard, not just so you didn’t get booted, but so you could have the best chance to influence your future. I suspect it’s all very different these days with tuition fees, but it was pretty brutal for some people.
If you secured the grades you progressed and specialised. This meant we got to do some zoo visits and start exploring topics like animal behaviour and undertake behavioural observation studies. Several of these were zoo based and included observing primates, but also Giant Tortoises. We also did a fair amount of non-zoo based observational studies, including undertaken observations in the uni canteen looking into group and sentinel behaviour.
I loved this mix. I love the fact that it really embedded science for me as a team sport, as so much of it you couldn’t accomplish on your own. It also taught me how much I value both collaboration and variety in what I do, a valuable lesson in choosing my future career.
In all honesty, over time, despite loving the science I grew to believe that sitting in fields in the lake district wearing water proofs for weeks at a time was less aligned with my future life choices, but at least it gave me fun memories that years later I could turn into a comedy sketch as part of public engagement work.
How did all of this help with the day job?
This was all very fun, but how does any of that help me now?
Well, I obviously covered a certain amount of animal related infection, which is still useful, but I think it was the wider stuff that gave me such a good foundation for every day working life as a scientist.
Firstly, there was always a strong focus on group communication. You just couldn’t succeed on the course without developing your group work and collaboration skills. Almost everything we did required multiple people to support. You can’t observe a group for 8 hours on your own, at least not efficiently. This meant the planning and analysis stages also involved a lot of group discussion. Being young and enthusiastic, there were lots of strong and differing opinions. Learning to manage in those environments has been a crucial skill that has supported working in healthcare and multi-disciplinary environments later on.
Due to the variety of different types of work, I also got used to needing to access information from all kinds of different resources and from a lot of different disciplines. One day, I would be accessing psychology or physiology papers, and the next, I would be in a field reading ecology guides or in the British Library accessing centuries old court records. This also taught me the value of being a generalist with a solid supporting skill set. I don’t feel like I will ever be a real ‘expert’ in anything, but I learnt to take things from 1st principles and rationalise my way through. This is an approach I will be forever grateful for as so much of what I see in my day job I haven’t experienced previously. Getting back to 1st principles is something I have to do often and this training enabled me to do that without fear of the unknown.
Finally, the whole process of struggling to get to uni when it was generally considered to be ‘not for me’ and spending a lot of my time there feeling behind and playing catch up taught me a lot of things that are so valuable in my day today. It taught me to see science as a puzzle, and that to solve something you sometimes have to give it space and come at problems from different angles. During these periods it also taught me to be comfortable with being uncomfortable, and knowing that uncertainty is OK, in fact it is often essential. The very way the course was structured also gave me permission to mix up my science and follow routes that interested me, not some pre prescribed path. I think keeping to this principle has been key to me ending up where I am career wise. Follow your passion and the rest will work out, has become a guiding principle when I’m undertaking decision making.
What is a zoonosis?
Speaking of things that help the day job, I spent plenty of time in my third year studying infections related to animals and animal to human interaction. One of the other great benefits of a background in Zoology is the fact that, having learnt things from the animal side, I can combine that learning with the info I now have from the human side. Zoonosis are an increasingly important part of health based conversations, especially in light of increased travel, climate change, and urban expansion. So, what is a zoonosis?
A zoonosis is an infectious disease that can spread from animals to humans, or vice versa. Zoonotic diseases can be caused by a variety of pathogens, including bacteria, viruses, fungi, protozoa, and prions.
There have been multiple occasions during my career where zoonosis have been flagged as causing wider public health implications, and some of the big hitters are listed below:
One of the other reasons why zoonoses and a background in Zoology are increasingly important is linked to the One Health approach to antimicrobial resistance (AMR). This requires us not to look at AMR from a purely human or animal perspective, but that we need to look at food production/agriculture, human and animal, as a holistic whole. I’ve recently been involved with a podcast series that involved discussing One Health issues with a vet, Simon Doherty, called going Macro on Micro, and hearing the veterinary perspective has been really helpful and eye opening.
Embedding public engagement
One of the things that I loved about staying overnight at London Zoo, apart from it reminding me of a joy for science and of fond memories, was the way that science and science engagement was embedded wherever you went, from the toilets to the canteen. Not only was information wherever you looked, but it was done in such a fun variety of ways, including an entire focus on poo, which was brilliant to see. It was science delivered in an accessible, engaging way that didn’t feel like you were being ‘taught’ but that you learnt through play and exploration.
This is such a great lesson for all of us involved in teaching and education, in both formal and non-formal settings. Learning can be achieved without it being arduous and by enabling those visiting to understand that science can be fun without it feeling ‘other’ or out of reach. It is the best way to introduce a generation of future scientists to the subject. Work such as this, also goes a long way to break down stereotypes of what science is (often considered to only be lab based) and what a scientist looks like (often considered to be the realm of older white men). In reality, science is for everyone, undertaken by everyone, and takes place everywhere. Embedding this concept early is the best way to change how science will be perceived in the future.
A peaceful escape
To end, I just wanted to quickly talk about what a delightful experience staying over night was. I am not a camper, and I am barely a glamper. I want an en-suite bathroom and a proper bed, with the ability to have tea whenever I want it. Fortunately, the cabins at London Zoo provide all of these things.
They are set in a zone of tranquillity, that whilst surrounded by the zoo, do not in any way feel impacted by the hustle and bustle of those visiting. That said, you are also in the centre of the zoo, so all of the walking tours around do not feel like you are walking miles im order to explore. You also get to undertake some activities that you simply wouldn’t be able to do any other way, including preparing enrichment activities for the animals and feeding some of the nocturnal species.
Whilst staying over you get full access to the zoo the day before, and on the following day. You also get to have dinner together after the zoo closes and breakfast together before the zoo opens. There are two different groups of bookings, one that includes kids of all ages, and one that is targeted at older kids and adults. This enables some of the tour content to be targeted, and for our tour, the group consisted entirely of adults. It was such fun, I can’t recommend it enough, and it was great to share it with mummy and Mr Girlymicro. It books up fast though, so if you want a chance at this unique insight, it’s worth booking several months ahead.
I’m off to the Federation of Infection Societies (FIS) conference this week. I’m involved in 3 sessions over 2 days, and in many ways, these types of events are a complete highlight for me. I get to be inspired by hearing new science, I get to catch up with wonderful colleagues who I don’t get time to see very often, and I get to immerse myself in all things microbiology without the distraction.
There is another side to this coin, however, and that is both the anxiety that builds before I go, and that can last throughout the whole event. The ever-present spirals of ‘do I know anything?’, ‘will I say something stupid?’, ‘will I know anyone?’, and the classic ‘do any of these people actually like me?’.
The combination of this social anxiety with the, sometimes long, very peopley days, can mean that I hit spirals pretty easily and the lack of solo recovery time means that I can find it pretty exhausting by the end.
Now, I’m obviously not talking about extreme cases of social anxiety that may require informed medical or long-term support. I’m talking about situational anxiety that most of us may find ourselves in from time to time.
Just in case there is anyone out there in a similar boat, I thought I might put together some things I’ve learnt along the way that help manage some of my anxiety traits and enable me to actually enjoy the experience rather than dreading it.
Do your prep work ahead of time
The first thing I’ve had to learn is that I can’t just pretend that doesn’t happen. I can’t wish it away. What I can do is be prepared and make sure that I have made the process as trigger free as possible.
For me, this is about simple things, like getting a hotel as close to the venue as possible. It means that if I just need a 30-minute alone break, I can take one. It removes anxiety about getting lost or forgetting something crucial and not having time to go back for it, which, although minor, can be the final straw. It’s also about making sure that I have pre-found all the rooms I need to locate ahead of time, so I know where I’m going, and that ahead of multi-day meetings I have a plan for which sessions I’m going to before I even travel to the event.
Know your triggers
I know that I have a few things that really lead to anxiety, but perhaps more unique to me, is the fear that I was have an auto immune attack and won’t be with people who understand what is needed. I learnt early that the best way to cover this one off is that I very rarely travel alone, especially over seas. I often travel with my mum or one of a very small list of truly trusted people, who I know would understand how to get me help if required.
Something that is more likely to strike a cord with others, is that I am also the girl who has walked into conference rooms, spent 15 minutes and walked out, as I knew no one and was just overwhelmed. I’m not proud of these moments, but I think it’s important to acknowledge that they have occurred. Although, to be honest, when they’ve happened, I mostly felt invisible, so I doubt anyone noticed.
I have discovered that I need to know that the space is one where I feel welcome for me to perform at my best. This sense of welcome can be either intellectual, because of the topics covered, or because of feeling a sense of community, as the room contains people within my field or in strong alignment with my values. I’ve found the overwhelming feeling hits most strongly when I’ve been in very large political or strategic sessions, where I felt out of my comfort zone on both intellectual and community counts.
That said, I’m not too bad in the sessions themselves, I’m there to learn something new, and learning excites me even now. It’s the breaks that are my nemesis, especially when large groups all surge into a space at the same time, and the weight of expectation that you must now network lands. The seconds that feel like hours of desperately searching for faces you recognise and being forced to face the fact that yes, you really should go up and speak to that absolute stranger, as it’s the right thing to do. It’s these moments that can cause me to bolt for the nearest bathroom.
Carve out time for yourself
One of the key mechanisms I’ve identified to help with my triggers is that I make sure I have enough time to myself, be that eating food away from the venue so I feel more certain what it contains and less at risk, to making sure I have evenings to myself to process and unwind.
I usually come over as really social, and really into spending time with people, and I am both of those things. I also only have a limited amount of social battery, and so in order to maintain that extrovert part of myself I have to have recharge time. I love talking to people about this blog, I love hearing about and responding to other peoples work, but at a certain point I need to sit down with an audio book and a cup of tea in order to do it well. This means that when I go through the brochure ahead of time, and plan my sessions, I make sure that I have enough blocks of time to enable me to be my best self when I’m in the space with others. Sometimes all you need is a walk to a local coffee shop and back to give you the perspective you need.
The wonderful thing about having hit my 20th year as a Healthcare Scientist, is that I now also know quite a few people, some of whom I’ve known for well over a decade. This means that at most events, there are also people who I count not only as colleagues but as friends. People that I can just go and spend time with that doesn’t include social commitment. Those friends you have that you can just be in the same space without any demands being made. If I’m at an event where these people are also attending, then I know that I have someone I can just excuse myself to catch up with if I’m having a moment. It’s also the great thing about ensuring that you have a hotel room nearby. Your safe bolt hole is only minutes away.
Make an agreement with yourself about how much is enough
The fact that you have social anxiety does not provide a free pass to escape one of the fundamental purposes of attending conferences, networking. It’s key to your career, it’s key to your development, it needs to happen. The thing is that there are varying degrees of what networking can be, and before you’re in the space, you need to decide what level you are aiming for and will therefore achieve. For me, my deal is that I will, on each day, speak to one person I don’t know. I am not allowed to finish my day without this happening, but once I have had that one daily interaction, then any further moments are a bonus. Once that one challenging moment is over with the pressure is off, and then I almost always over achieve on my goal.
Be realistic about how much you can expect of yourself
The key thing I’ve learnt is that I have to realistic when I’m making that deal with myself and deciding on achievable targets. For me, there is not point is saying I will speak to five people I haven’t met before, as I’ll just be setting myself up for failure. You will also find that I rarely sign up for conference dinners, as I have over the years found that if I’m in a space with other people from 08:00 – 18:00 I will really struggle to then spend yet more time with other people, no matter how lovely or interesting those people are. All I will want at that point is room service, tea, and a movie in my room.
Everyone will have their own tolerances and lines. The important thing is to have enough self reflection to know what yours are. Otherwise, you just add guilt into the anxiety mix, which is not much fun for anyone.
Learn how to work a room using tools you are comfortable with
One of the other things that I’ve learnt about myself, is that although I get super anxious standing in a room trying to approach someone at the coffee table, I am much much more comfortable moving around the exhibitor stands. The guys at the exhibitor stands are motivated to speak to those who approach, and there are usually science based discussions that I am eager to have. This, for me, is a match made in heaven, as it breaks me into the speaking to people I don’t know in a very gentle way. If I’m lucky, I will also meet others when I’m wandering around, which will allow me to tick my ‘speak to one stranger box’ as exhibitors do not count on that front. The added bonus is that I also often manage to find cool new stuff I’m interested in or develop collaborations whilst this is happening, so it’s a no lose scenario for me.
The other thing that having worked for 20 years has given me is the opportunity to be asked to be involved with sessions. For this girl with social anxiety, this is actually a great thing, despite the fact that it sounds like it should be stressful. I’ve never minded public speaking in the same way as I worry about 1:1 interactions. When I speak, all I can do is put my best foot forward and hope that others will be interested in what I have to say. For the most part, if people don’t engage they will just leave and not give it another thought. On the positive side though, if people find what you say interesting enough to want to speak to you afterwards, this a great way to tick the ‘speak to one person you don’t know box’ and as they are approaching you all you have to do is respond. I find this so rewarding, but I also appreciate how fortunate I am to have this type of opportunity and how much it helps me manage to get the most out of events.
Prepare your exit strategy
One of the important things to bear in mind, and which I often forget, is that others do not necessarily feel the same way about social requirements. I struggle when people arrange evening meals at meetings when you’re already booked to spend a full day together. I understand the purpose, it’s lovely to build bonds and memories, and logistically it’s easier. I rarely, if ever, hit the end of the meeting day and wish to spend the few hours downtime I have with others, over reading in the bath however. There are frequently times I can’t opt out of these moments, but where I can, I will often have a pre planned reason to excuse myself. Often, this is work related, as I will always genuinely need to do some email catch up, and doing this after dinner means working till midnight. I don’t lie but I may pre-plan my rationale for not being available to support both my work load and my mental well being. I will never not pre-inform, as that is rude. People will have budgeted and made arrangements, so I will never last minute drop, but if the option arises I may flag unavailability at the planning stage.
Don’t succumb to expectations and pressure
People are amazing and much more welcoming than you expect. I’m always counting myself as so fortunate is be asked to unexpected drinks, meals and catch ups at conferences. I have learnt that I need to not get caught up in the moment and end up crossing the carefully curated boundaries I have put together, in order to ensure that I can last the social distance of the conference. I’m a planner for a reason and I don’t riff off the plan well. I also struggle with saying no. This means that there have been multiple times when I’ve said yes to that dinner, or those drinks, and have then suffered the consequences afterwards. Now, I work hard to keep to my boundaries so that I don’t make life harder for myself. This can be surprisingly difficult as all these invites are inclusive and well intended, I just have to remind myself to make the sensible choice to enjoy the entire event, rather than burning out after a single evening.
Know that this is an essential part of the job, so invest in coping strategies early in your career
The truth is that networking and attending these kinds of events is essential. They are a fundamental way of hearing the latest science and expanding your knowledge. They are also key for collaboration and building your networks, as well as dissemination of your work. No matter what anyone says, I have found that science fields tend not to be meritocracies, there’s plenty of ‘who you know’ involved, and the only way to address that is to get yourself out there. So you will need to learn how to navigate these settings, and the earlier in your career you manage that, the more rewards you will reap.
I’ve talked about some of my own pitfalls and things that I’ve implemented to help me, but you will have your own triggers, and each response will need to be customised to yoi and your needs. What is true for all of us is that you are not alone, and if you are in need of someone to speak to during the horror of a break, then I am always happy to be your person. This is what I look like and I will never turn you away.
Know that it gets easier
The longer you hang on in there, the easier it gets, honestly. I haven’t walked out on an event in a decade, although the toilet hiding is still a little more frequent 🤣
Pre manage your expectations of yourself and make sure they are reasonable
Book with a group or a friend if you can to take the edge of socialising with strangers
Join a social network, as you can use it to find like-minded people, and it can give you a virtual introduction rather than the cold approach
Similarly, join a society. Societies often have small meet-ups either before events or at meetings, and so you can make connections in a smaller, less intimidating space
Submit work. It’s much less intimidating if people come and speak to you rather than the other way around
Know it’s absolutely OK to need to tap out and have your own space, but make sure this is pre-planned so you don’t miss the reason you came to the event
Right, well, having talked about the need to be prepared. I haven’t even packed yet, so I’d better get on that. If any of you are Liverpool bound, make sure you come and say hi. I’m there Wednesday and Thursday.
All opinions in this blog are my own
If you would like more tips and advice linked to your PhD journey then the first every Girlymicrobiologist book is here to help!
This book goes beyond the typical academic handbook, acknowledging the unique challenges and triumphs faced by PhD students and offering relatable, real-world advice to help you:
Master the art of effective research and time management to stay organized and on track.
Build a supportive network of peers, mentors, and supervisors to overcome challenges and foster collaboration.
Maintain a healthy work-life balance by prioritizing self-care and avoiding burnout.
Embrace the unexpected and view setbacks as opportunities for growth and innovation.
Navigate the complexities of academia with confidence and build a strong professional network
This book starts at the very beginning, with why you might want to do a PhD, how you might decide what route to PhD is right for you, and what a successful application might look like.
It then takes you through your PhD journey, year by year, with tips about how to approach and succeed during significant moments, such as attending your first conference, or writing your first academic paper.
Finally, you will discover what other skills you need to develop during your PhD to give you the best route to success after your viva. All of this supported by links to activities on The Girlymicrobiologist blog, to help you with practical exercises in order to apply what you have learned.
It’s Halloween weekend, and in previous years I’ve talked about all things Zombie and infection transmission. This year, though, I thought we talked about something a little different, infection control precautions through the lens of the Alien movie series. Most importantly, I’m going to talk about those initial interactions with the unknown that we frequently see in both these movies and in infection prevention and control (IPC), and whether we too would open the door when someone presents at the air lock?
Spoiler warning! This post is going to mention things that happen in various Alien movies. If you haven’t seen them it may, therefore, contain spoilers – the best way to deal with this oversight in your viewing (if you are concerned) is to just get out there and watch them as Alien is the same age as me 😁
This post was inspired by watching Alien Romulus again this weekend, which, if you haven’t seen it is the best Alien movie in forever.
In preparation for the cinema release I also did a re-watch of a number of the movies in the franchise. Just in case you are less familiar, and inspired to do the same, the list includes a variety of films in different sub-genres as listed below:
Whilst watching these I was struck by a number of moments that made me think about behaviours during the pandemic, but also tales of heard of some activities that occurred during the response to the Ebola pandemic and other high risk clinical settings. Not all of these moments would have been massively out of place, in terms of parallels with these films, and demonstrate that both risk assessment and clarity of thinking can be impacted and lead to responses outside of what would be normally expected.
The thing to remember is that there are usually protocols for just about everything, so most of the decision-making should occur and have been thought out long before the situation ever arises. The problems are almost always linked to human factors in the way we respond to stress and unexpected situations, and when the protocols appear to go out the window. So, just like every character and every space ship in the Alien franchise has a protocol for how to behave when they encounter new life, strange situations or sick crew members, every healthcare facility also has protocols to help deal with illnesses we see less often or that get issued when new diseases are encountered. Healthcare facilities may not have air locks, but they do have labs and isolation facilities, so the parallels may be more present than you’d imagine.
Infection is not always obvious
One of the first themes that recurs throughout all the movies is that infection is not always obvious, either to those on the other side of the air lock, or to the individuals outside waiting to come in. Infection with the parasite sometimes occurs when the stars of our show are unconscious, be that due to trauma or medical interventions, and so they are unaware of the Facehugger on character action that has occurred.
In terms of IPC the same if frequently true, both for viruses and bacteria. Some viruses have what is known as a pre-symptomatic phase, where you are infectious to others before you even know you are sick. This was a big problem in the early stages of the SARS CoV2 pandemic. Even for bacteria, when we talk about antibiotic resistant bacteria, most people are colonised and have the potential to act as silent sources without even knowing it, with only small numbers going on to develop infections.
The truth is not always apparent
Even when an individual knows that something has happened, and are aware of their close encounter with Alien kind, the truth of their scenario may still not be apparent to either them or to others. If you look at the Facehugger situation, surely once the terrifying creature has dropped off without apparent poor consequences, then everyone breaths a sign of relief and is grateful for the near miss, not knowing that this is only the beginning. When you combine this with the fact that some people will determine this to be a low risk event and therefore not want to disclose, as they are aware of the inconvenience that will result, you end up in situations where not all the information is available.
This can also be true in real life clinical situations. Patients may not know they have been exposed. Patients may also present with symptoms that they haven’t recognised as significant, or that they have risk assessed themselves and decided they aren’t concerned about and so don’t disclose. This can happen more easily they you think, especially at the start of something, where patients don’t feel particularly unwell, or they just have a couple of vesicles/small rash. In the latter stages, when patients are presenting because they feel unwell, they may be confused or not always able to accurately disclose what’s happened. Occasionally, this may be a deliberate attempt to withhold personal details, but most often it’s because they are rightly focussed on how they are feeling in the moment. Plus, if you asked me to accurately recall everyone I met and everything I ate a week ago, I’m not sure I could, even when well.
By the time you realise the condition is a threat it may already be a risk/out of control
One of the consistent themes across all of the movies is that situations get out of control before anyone truly understands the situation and the risks. It’s only when the person that you breached protocol for suddenly starts to writhe and the horror stands before you in all its glory do you truly understand the implications of the decisions you’ve made. At that point you are trapped in your glass med bay with a growing Alien and your self recriminations are not going to save your life.
This one is a rather more dramatic version of some of the conversations that happen amongst healthcare workers when you phone to give results and have conversations about whether patients had been in the right precautions and the staff member was wearing the right personal protective equipment (PPE). There have definitely been times when staff have made a risk assessment and not followed the protocols about what PPE to wear and have then responded to these phone calls with ‘what can you do?’ in relation to the exposure. Sadly, in some cases there is nothing that can be done once the guidance has been bypassed but to wait and see, which is the reason for the guidance in the first place. Fortunately, for most scenario’s in the real world, the consequence isn’t bloody horror, death and an alien threat to mankind.
Risk assessment is linked to risk management
One of the reasons that protocols are in place in the Alien movies is that someone, somewhere, has obviously recognised the risk of infection in a small contained community where everyone interacts and lives on top of each other. Even in Aliens, when you’re talking about somewhere the size of a colony, this principle stands. This is because you are unlikely to be able to access a clinical trial on a mining ship, or develop a novel antiviral on terraforming mission, even if what you’re importing is a more traditional style of infection, versus an Alien parasite. The extent of the risk mitigations needed will always align to the risk itself. If you are concerned about an introducing something that is untreatable, then your measures are going to be much more extreme than if your infection is likely to just mean someone goes to bed and takes paracetamol for a weekend. If you can’t treat, then prevention is your only option. After 9 movies there doesn’t appear to be a Xenomorph (Alien) cure and so measures taken to prevent allowing one into your space need to match the risk they present.
This approach is definitely seen in response to infection in IPC. If you have a condition that spreads easily, rapidly and can be incapacitating for a period (i.e. norovirus) then you will use a different set of precautions to those that you use to manage something which may not be as transmittable but is untreatable or has life threatening consequences such as a haemorrhagic fever. Having conversations and being open with people about the risks of getting things wrong and ensuring that individuals understand why responses are different in different circumstances are a key requirement for people working in IPC, and something I think we should all endeavour to do better at. I think the days of asking people to blindly follow protocols should probably be behind us, as I think the Alien movies demonstrate that if people don’t get the why, they often ignore some of the core components based on external drivers
So, what lessons can we learn?
Beware of acting on incomplete information
Decisions are consistently made in these movies based on incomplete information, which leads them to underestimate both risk and consequences. A great example of this is the way people use information related to the black goo, especially in Alien Romulus, maybe don’t inject yourself with a substance that doesn’t have a proper name let alone a full data set for you to understand what it does. The other thing is that information is often treated as static, and so there is very little rapid inclusion of new info, rather than being mindful of an iterative response to new data, so help constantly inform and improve your risk assessment. It’s always worth being conscious of when is enough is enough when it comes to information and decision making.
Emotions get in the way of logic
During the movie Covenant, the entire crew is made up of couples. I get this in terms of colonisation, but in terms of good decision making, and in relation to risk this is just a one way route to bad outcomes. There’s a reason that in a certain Zombie series husbands have kept their zombie wives locked in basements rather than removing the risk to them and others. There’s a reason medical professionals should not manage their loved ones. Emotions interfere with logic, and there is no way under this setting you are managing to make decisions without your emotions getting in the way. It’s a reminder that if we become aware that we are in an emotive place, it may be the time to step away and take a deep breath, before making that judgement call or even tap out entirely and allow someone more removed to take our place.
The contrast between human emotional decision making and evidence based decision making, usually undertaken by the android cast, is beautifully explored during Romulus via Andys story arch and is one of the highlights for me in terms of enjoyment.
Science doesn’t change based on how much you wish the outcome to be different
One of the reasons that emotional involvement in decision making can be so challenging is that it can interfere with perspective and accurate interpretation of risk, thus impacting risk perception. Sadly the truth that wishing does not impact outcomes is hard to argue with, but it is human to try to persuade ourselves we have more control and ability to influence the outcome than we do. Under stress, our natural tendencies towards pessimism or optimism are definitely amplified. All of this means that when there is someone at the door banging and begging to be admitted, it is easy to persuade ourselves there is a) enough time to manage to open the door safely and b) the consequences of opening said door will not be as bad as we fear. Emotions don’t change outcomes but we are almost programmed to hope that they can.
An individual will always want to be the 1 in a million
The reason someone opens the door is the same reason that when one character looks at another and utters the fateful and true words ‘it’s too late’, and it almost definitely is, neither one acts before everything gets out of control. Humans are not good at dealing with numbers and risk when they are actively involved in the situation. One of the reasons we aren’t in that we throw sentences around saying it is a 1/million chance. We, as humans, have a tendency to focus the fact that, although it is a long shot, there is a chance that things can go your way. Sadly, as someone who has experienced the opposite, where my sister died in a 1/10,000 pregnancy, someone always need to be the one. The stats work both ways, whereas most of us survive in the world by only focussing on one side of the equation. This therefore impacts our capacity to evaluate any risk in situations we are involved with. Somebody always bears the cost and few of us can bear the vulnerability of acknowledging that that somebody could be us.
The people with the most experience are not always the ones making the decisions
One of the other main themes in these movies is that decisions, when not being made by friend and loved ones, are often being made by people in positions of power, not necessarily based on knowledge or even accepting of prior experience. This works well or not so well based on how well they listen to those who do have the information to help improve their decision making. Chains of command, especially in high stakes scenarios, are not necessarily bad, as we’ve already talked about the risks linked to emotional decision making, but so much depends on how well they work and how they place value on evidence based choices rather than hierarchy.
The other theme here is the trusting of unknown sources, especially ones with no evidence of expertise, over those who have either lived experience or expertise. I think this one resonates a lot right now, when there are so many sources of misinformation out there, and so many conspiracy theories that rely on speculation and rumour. Fact checking is key, be that on a space ship or deciding on your vaccination options.
Not everyone has the same thought processes
One of the other reasons decision making goes astray in these movies is because those involved in that decision making often have undisclosed values, beliefs or drivers that are impacting their choices, and this process is not always obvious to those others involved. This is true from androids that may or may not be obviously androids and who will have programmed ‘primary directive’, as well those working for the corporation. This is interesting as they often have more complete information than the others involved, as well as seeing the situation through a different lens because of how they view the world. This means that they can see others as disposable or views risks different, as they have a set of criteria that they wish to achieve which is more than just survival. Although in clinical life the juxtaposition is rarely so extreme, the challenge of reaching alignment when people come with different world views can definitely impact shared decision making.
Smart people can do stupid things
Having said all of that, smart people can in general do stupid things, even without all of these complications. Even when the experts are the ones making the decisions they can still make the wrong ones, especially when tired, stressed, or lacking all the information. This is the reason why protocols are key, drawn up and decided upon when all of the confounders to good decision making are not present.
You need to follow the standard operation procedures
In the end this entire post has been a very very long way of saying ‘JUST FOLLOW THE SOP!’
Many of these movies but have been much shorter with a much reduced body count, if those involved had just followed the pre-established procedures laid down for their safety. Obviously, we don’t have so many Xenomorphs as a daily risk factor in healthcare, but the same is true for us. SOPs are rarely there for the sake of it, they are there to support decision making so that in times of stress or information overload, you are not having to seek extra information to support good decision making, you have it freely pre-digested and available to you. So the next time you think twice about donning that PPE or the closing that isolation room door, ask yourself ‘would you open the airlock door?’, think twice and do the right thing.
And now for something completely different
Finally, because this is something that has amused me whilst watching these films and is probably not something that I can talk about in general down the pub. The computer in the Alien movies is usually referred to as Muthur, pronounced Mother. I just want to share my joy that the analysis software that is used to help analyse 16S rDNA runs, to give you microbiome analysis i.e. tell you what bacteria are present in your sample, is called Mothur, and also pronounced Mother. I’m sure the two things have nothing to do with each other, but allow me my scientific joy that something which was so ‘other world’ when it came out to me as a scientist has the same name as something imagined from ‘another world’.
Also, if anyone needs a science advisor on their next project, give me a shout as this post has brought me much joy and I think I may have missed my calling 🙂
Firstly, lets start with an apology. I’ve haven’t posted for a month as I’ve been struggling health wise and not really been able to get to a laptop to be able to write. Although annoying, it has given me plenty of time to think about what I might want to write next, so hopefully you’ll forgive me.
Now, onto the present. I’ve been in post for 20 years this month, and have also just spent some time recording a couple of webinars that covered bits about the journey to consultant. It felt timely, therefore, to put something out there talking about my experience of the consultant journey. Word of warning, though, this is only my experience, and everyone’s journey is different. I hope my sharing this it will help others, both in validating the aspiration but also in supporting expectation setting by talking about what it was really like to go through. Frankly, I want to be clear that it is never as linear as it appears from the outside and that that is perfectly OK.
So, let’s start at the very beginning. On my first day in post (all the way back in 2004) I was told that I was on an 11 year programme from trainee to consultant, and boy did I drink that cool aid and believe that would be the truth, after all these people were my bosses, supervisors and mentors. Sadly, it transpired that although they were being inspiring they were also far from being completely honest in terms of disclosing how straight forward, or not, the programme and progression actually were. I am now a Consultant Healthcare Scientist, although it took me 16 years rather than 11. Now I’ve reached the promise land I want to be clear that it was no where near the linear journey that I was sold on recruitment and there was a lot of struggle at every single stage. That being said however, now I’ve crossed the line, I wouldn’t have had it any other way. It was dealing with those barriers and obstacles that made me really decide who I was and what I wanted. It was also where most of the learning was truly at. So I wanted to write a blog post that doesn’t sell the ideal but discusses the realities of what some of those barriers looked like and to make those facing them a) feel less isolated and b) know they can be overcome.
You have to be doing the job to get the job
This one took me a long time to fully comprehend, as it can feel counter intuitive, but you have to already be doing most of the role in order to be able to get the role permanently. It is easy, in moments of frustration, to turn around and say ‘that’s not what I’m paid to do’ or ‘if they want me to do that job they need to pay me for it’. There are definitely times when you need to dig your heels in about workload and boundaries, but this generally needs to be the nuclear option. For the most part, you need to be prepared to roll your sleeves up and jump in to get the experience so that you are well placed to advocate for a post to be created, if that’s your aspiration, or to enable you to apply elsewhere with confidence. For me, I learnt huge amounts when I provided maternity cover for a year as a trainee. It built trust and showed willing to my clinical lead as well as providing me with experiences I would not have had in any other circumstance, enabled me to springboard into my next post, and meant my clinical lead wanted me stay enough they found money at the end of my training. Maintaining an openness to opportunities and an awareness of the fact that stepping up, although not always recognised financially or otherwise, does come with benefits on all sides and is an important part of playing the long game.
There is no single way to get from A to B
When I started, I thought the journey would be straight forward. I’d finish training, I’d get my 4th year funded, I’d get a Clinical Scientist post. Then I would work towards FRCPath and a PhD, hopefully moving into a Principle Clinical Scientist post. Once I’d achieved my tick boxes, my loyalty and hard work would be rewarded and a Consultant post would be forth coming. That’s just not the way work places and budgets work however. On this one patience is THE virtue, and the sooner you can acknowledge that A doesn’t immediately lead to B, the better for your mental well being. That said, the training pathway now available for Healthcare Scientists does make, at least the early stages, more straight forward.
Counter intuitively I’m going to say that, looking back, not having access to the straight forward route has been the most beneficial thing that could have happened to me. I would never have ended up with a clinical academic career if I hadn’t needed to acquire further salary funding and a PhD. I would never have ended up in Infection Prevention and Control if my training programme had been funded for the full four years. So many of the things I value the most only came about because I had to find ways around barriers and due to glorious happenstance. Despite being challenging in the moment, I’m grateful for every detour taken.
When it comes down to it, the person responsible for your progression is you
This one may feel harsh to hear, but no one is as invested in your career as you are. I’ve had a fair few people over years who’ve come to me and said that they deserve to be given X or Y. No matter how true this may be, this isn’t how it works in reality. If you want something to happen, you have to be the driving force to make it so. You are the star of your own movie.
I think a good example, for me, of this was my training programme. I was really fortunate that no one would block anything I wanted to do. The flip side of that coin was that no one sorted anything out on my behalf. It was my responsibility. I could go to any clinic, shadow anyone I wanted to shadow, but I had to reach out to find the contacts and arrange it. I had to have a vision of where I wanted to be and put together the pieces to enable me to get there. This is, in turn, enormously freeing and terrifying. It taught me early to be the master of my own destiny, and this is an important lesson for anyone on this pathway, irrespective of how supportive your surroundings at some point you will have to make it on your own.
You will hear a lot of no
One of the reasons to learn early to be your own driving force is that you will hear a lot of no as you under take this journey, whether that be linked to funding, exams, or posts. If you haven’t set your own direction then it can be hard to keep driving, as you may not be sure what you keep pushing for. As the old adage says, if you don’t have faith in yourself, no one else is likely to.
A lot of the no you hear will not be personal, a lot of it will be nothing to do with you or your skills. That doesn’t stop it from being hard to hear or from it feeling personal when it is not. A key skill that isn’t much talked about is learning how to respond to these challenges. You need to move to a place where you are able to process and move on without carrying that rejection with you. To learn from the moment and then let it go, so you always emerge a stronger, better person for the experience.
You have to know what matters
Something that can really help when facing the barriers and challenges along the way is being really clear what matters and why you are pursuing the choices you’ve made. Why does this route align with your own personal values and beliefs? If you understand your ‘why’ then you can weather the delays. It makes it so much easier to get back up when you’ve taken a knock.
The other side of this, which we don’t talk about anywhere near as much, is the importance of knowing what doesn’t matter. You can’t fight a battle on all fronts, and there will be positions you get into when you discover that you are fighting for something out of habit or without thinking about it. This is a waste of energy that you could be focusing on something that actually matters to you. Developing the self reflection to know when this is the case and using it to remove yourself from the arena is one of the most freeing and valuable skills you can invest in. I learnt this late, and I really wish I’d realised it earlier.
It is not an even playing field
I started this journey as pretty naive. I think I genuinely thought everyone would have a similar set of challenges and barriers to overcome. This just isn’t true. I know people who’ve become Consultants over a weekend with no external advert or interview. I know of trainees who’ve gone from point A directly to point B because their faces fit and everything aligned for them, not many but some. The challenging reality is that sometimes the playing field just isn’t even. Some disciplines are more set up for straight forward progression than others. Some disciplines have a bigger medical leadership who may not understand the role of Healthcare Scientists. In all honesty, being a woman in science is also not always straightforward. The gender issues are not always as obvious, but they are definitely still there, and that’s before we even start talking about other diversity issues.
When confronted with moments where this imbalance becomes apparent, we always have 2 choices, you can quit, or you can continue to fight. One of my core values has always been about parity of access, and one of the reasons I became a Lead Healthcare Scientist was to be in a position where I had the capacity to influence in this area. So when you come across inequality on your journey, whether it’s something you face or become aware of as an ally, I would always encourage you to be the change you want to see and to remember these moments when you are in a position to make life different for those that follow you.
Know that it’s OK to change your mind
So far, I’ve talked a lot about making Consultant, but I think it’s important to talk about the fact that it’s OK to also not want to end up as one. Life is about far more than work, and even in work we all find different sources of joy. The job role as a Consultant is not the same as a qualified Clinical Scientist. You won’t get lab time. There’s an expectation that it’s not a 9 – 5 role, and you will sacrifice a lot to get there, both financially and in your home life. It’s not the right choice for everyone, irrespective of your capability to do the role if you chose. I just wanted to take a moment out to write something that is supportive of starting along this route and then deciding it isn’t for you, for all kinds of different reasons.
Sometimes, I think people feel pressured to continue as ‘I’ve started so I must finish’. I love where I’ve ended up, and it was always my passion. If that wasn’t the case, then I would always support ending up where your passion does lie. That could be in the lab, in education, in quality or leadership. We are so lucky to have so many different options. I’m also aware that I talk about ending up working where your passion lies, and that is also not right for everyone. For many people, that passion doesn’t lie at work at all but with other aspects of their lives, and work is just what enables those things to happen. In my clunky way, I suppose what I’m trying to say is you do you boo and don’t let the pressure of expectation or external influences lead you down a pathway that isn’t right for you.
Bring yourself to every interaction
This all brings me onto something that also took me a long time to embrace. You can’t spend a career spanning decades pretending to be somebody else. For about my first 5 years in post, I didn’t really talk about the things that interested me. I didn’t talk about being a gamer and a geek because I was just really concerned about any judgement and how that might impact my career progression. It took me a while to accept that putting on a front is both really tiring and limits the amount of genuine relationship building you can do.
That said, I acknowledge that it can also be really hard to turn up as your whole self. I know there are some leaders out there who say we don’t owe our full selves to work, but I don’t think I know how to do it any other way. If I want those I lead to share something of themselves so we can build true connections, then I don’t think I can do differently. I’m not saying that everyone has to share every aspect of their lives, but I think I have to lead by example. For me, this means embracing the fact that I am not perfect and that I will have bad days as well as good, and make it OK to talk about those things. For me, that opens up dialogue on coping strategies and deeper dialogue versus pretending that everything is perfect. Everyone brings something different and we should honour that difference by embracing it rather than hiding who we are.
Sometimes, it’s just a case of continuing to show up
I’ve talked a bunch about some of the reasons that making Consultant may involve surmounting or finding a way around barriers. I think one of the things we talk less about is the fact that the thing that often makes the most different is continuous effort. At its heart it’s about continuing to show up, on good days and on bad. It’s about demonstrating commitment and being in it for the long haul.
Now, when I say continuous, no one expects every day to be the same, but there is a consistency linked to intention. If you are clear where your ambition lies and stick to it, it is easier for those around you to also factor that into their thinking. If you are changing the goal and ambition regularly, then can be harder for those trying to support you. It’s not that you can’t change your mind, but you should try not to scatter gun your approach. Making Consultant, to me, like getting a PhD, mostly seems to be about a tenacity of purpose that means you keep showing up, combined with the patience to know it will happen eventually.
Always remember why you started the journey
I think many of you will know that patience is not my greatest asset and so I found the journey so frustrating at times, as I had such a clear vision that was not always shared by others. For this reason, you really need to know that the pursuit of this is right for you, right for you when start, but also stays right for you along the way. It’s that clarity of purpose that can re-centre you when things are tough or when you are facing those no’s. Without it you could easily falter and it may be that it really isn’t the right option for you.
The other reason to have that clarity of purpose is that it is not like reaching the destination transports you to a land of rainbows and bunnies. Consultant roles have their own challenges, and in many ways just having the title doesn’t really change anything. The job is still the job. Therefore, if you aren’t sure along the way, you may just be signing up for more of something that may not be what you want it to be. The flip side of that coin is that if you are sure, and know what you are working for, you are likely to end up in the job you’ve dreamed of and aspired towards for over a decade, and that feels pretty damned good.
The people make the journey worthwhile
I just wanted to finish with something that has struck me more and more as I moved along the stages to becoming a Consultant. Although all the professional stages feel significant, it’s the people I’ve met along the way that I am most grateful for. It’s these people who will stick with you long after the nerves and stresses of an exam are just a distant memory. They will be the ones that guide and pick you up when you hear the no and face the obstacles. They are the ones that, when they celebrate with you, make the celebrations really worthy of the name. So don’t be so focused on putting one foot in front of the other that you forget to look up and find time to develop the relationships that will last a life time.