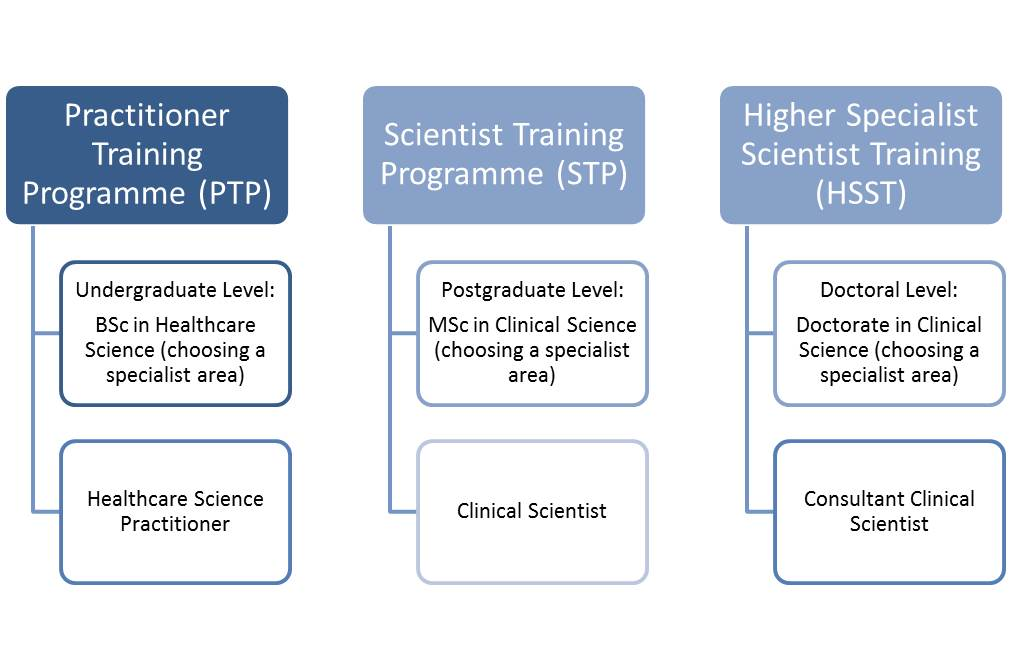
I’ve been thinking a lot about pathways in healthcare lately, from having conversations about T-levels and apprenticeships this week, to equivalence and Higher Specialist Scientific Training (HSST) posts. It’s made me reflect a lot on my own training pathways and the fact that the majority of the advice I received was that the only option, in terms of approach, was to work harder and do more. Now, don’t get me wrong, there is some merit to that, and there is also some truth, but I had it drilled into me that you can’t be successful if you do a 9 – 5. You must always do more. You must always over deliver. You must always be adding to and diversifying your CV.
This advice and approach has been key to me developing into the person I am now. I am objectively successful and so grateful for the support I’ve received along the way. I have the long dreamed of Consultant post, and my dream job. I was made a professor within 10 years of finishing my PhD. I’ve held multi-million pound grants and have over 50 publications. The other side of the coin is that, despite being exhausted, I can never sleep for the number of things I haven’t finished, and I constantly feel like I’m not doing or achieving enough. I’ve also written before about the impact of my anxiety levels when I’m tired or try to step away. So, as new starter season comes upon us, I wanted to take a moment to really talk about the messages we are giving our trainees, and ourselves, to think about how true they are for current training opportunities and what we can do better for those that follow us.
Let’s start with a bit of history and the messaging that we used to focus on as part of training
Goal orientated view of the world
During my first week as a trainee Clinical Scientist, I was sat down and told that it was an 11 year training scheme to Consultant, but it was up to me to put in the work and make it happen. Well, I worked pretty damn hard, including not having a weekend off at one point for 3 years, and it still took me 16 years. Does that make me a failure? I don’t think so. Does that mean that I should have worked hard to make it happen in 11? I’m not sure of how I could. In fact, I don’t know of anyone who made it happen in 11 years. Of the 4 of us who started, only 3 are now Consultants, and we were a pretty committed bunch. So were we all set up to fail?
The whole scheme was designed with that 11 year target in mind. I understand it from a strategic point of view. There are a lot of boxes to be ticked. Our situation was made even harder as there were only 3 years’ worth of funding for a scheme that required 4 years of professional practice to gain registration. That meant you also had to prove yourself worthy and useful enough that someone would decide to fund you for that extra year. Otherwise, everything had been a waste, and you would walk away unregistered and unlikely therefore to get a job.
My main problem with this approach is that it doesn’t really allow scope for exploration, and it really doesn’t allow time for creativity. It trains you into the ‘onto the next thing’ approach. I certainly had no time for celebration or reflection between stages. I was always trying to make sure that I was useful enough to remain employed, and in later stages, as it took me 13 years to be made permanent, I had to also ensure I was bringing in sufficient money to cover my salary so I would be kept in a job. It also means that when you finally do get all those boxes ticked and get your dream job, you are so trained into the tick box way of life that you are left searching for what the next box should be, rather than embedding and celebrating what you have achieved.

There is nothing that cannot be fixed if you work hard enough
When I started work, I used to read a book at my desk during my lunchtime, like I had when I worked at Birmingham City Council. It would always be some variety of fiction novel. I came into work one day during my first few months, and a pile of textbooks had been left on my desk with a post-it note suggesting that maybe I should read these instead. The implication, to me, was that it was not acceptable to have downtime, that any moment I had should be used to continuously work and improve myself. In short,’I must try harder’ ‘I must work more’ in order to justify the privileged position I was in. If I wasn’t going to lunchtime talks, the time should be used for other improving activities.
I also remember clearly listening to amazing female Healthcare Scientists talking at events about how, to achieve as a woman, you always had to work harder and do more than anyone around you. It was made very clear that it was required to constantly go above and beyond if you wanted to reach their position, if you wanted to succeed, if you wanted to make a difference.
The messaging has always been pretty clear. No matter how hard you are working, it probably isn’t enough, and you must work harder. Otherwise, you will fail and let everyone who had faith in you down, as well as yourself. If experiments fail, you don’t go home, rest and reflect, and come back tomorrow. You stay and set it up again. There were just too many midnight finishes to count during my journey to Consultant. If you want it, you will just work harder until it happens. I submitted my PhD a year early in order to achieve FRCPath whilst on my fellowship. At the same time, I took a PGCert in education because I recognised that it was important for my career path and my interests. Looking back, doing those three things simultaneously was foolish beyond measure. At the time, I thought I was just demonstrating that I had what it took.

Effort must be continuous
At the very start of training, I remember sitting over a bunsen burner crying. I was so ill, but no one around me ever took any time off sick, and it was just not considered to be OK. Eventually, I was sent home as I just couldn’t breathe, but it was very much ‘see you tomorrow’. Having an ‘off day’ was not something that happened. The hard earned truth I’ve learned to accept is that my best looks different from day to day. Some days, I could take on the world. Other days, I struggle to crawl across the line at the end of the day. Especially with a health condition made worse by stress, the idea that I can just ignore it, carry on, and always achieve amazing things every day is sheer madness. This was how I tried to work, however, and it took seniority and growing older to come to terms with the fact that this was just not achievable.
The thing about seniority is interesting. There is something about seniority and being able to give yourself permission to do things differently, which is worth mentioning. That’s not the real difference, though. I think the real difference is in the expectation setting. I try to be the person who gives others permission to acknowledge that some days are harder than others. Who checks why people are still there when they should have gone home. Doing this for others has the side benefit of reminding me that sometimes it’s OK to also do this for myself. It is not possible, nor is it necessary, to work at 100% all of the time. There will be days when you absolutely need to bring it, but there will be recovery days when what you should do is catch your breath, and if possible, do some reflection in order to make things better long term. A career is a marathon and not a sprint, after all.

There is no room for failure
This one isn’t just a work thing. It’s definitely a family thing too. My father is infamous for saying that no child of his has ever failed anything, and we weren’t about to start now when I was worried about FRCPath.
The Clinical Scientist training programme has always been competitive. Getting into the programme was competitive, but even when you were in it, my experience was that the programme itself was pretty competitive. The people on it were used to being at the top of their class, and I experienced a fair amount of posturing throughout my first 4 years. Far from being tackled and a focus placed in peer support and collaboration, I feel like the rhetoric around the programme added to this. The focus on there not being enough places for us all to get posts when we finished, and the constant commentary on only the best of the best being able to get Consultant posts, placed us in direct competition with each other from day one. Therefore, you couldn’t talk about challenges for fear of disclosing weakness that would impact your future. That atmosphere is one of the reasons I’m so passionate about talking about the reality of the job on this blog, both the highs and the lows, as I didn’t have any way to normalise my experiences when I was training and in the midst of them. I hope posting will help others in finding a benchmark for ‘normal’ that I didn’t have.
Even on a day to day basis failure was not an acceptable part of training. To this day, I remember that one of my fellow trainees reported a NEQAS result (part of a quality control scheme), and she got it wrong. The result got reported, and the department lost a point on the national scheme. In reality, it should have been checked by someone else before it went out, but it happened. The virology consultant at the time never spoke to them again. We would sit in joint tutorials, and he would ask a question, he would then wait for my response even if I was just repeating what my colleague just said. He would respond to my answer but not theirs. There was never a review of what had happened and how the mistake had occurred. There was no acceptance of the fact that being part of a quality scheme is there to support learning and to identify where improvements can be made. There was just a long-term change in the way that trainee was seen and how they were then supported. It was a clear demonstration of what would happen if a mistake was made and that it would impact how your working life would be from that point on.

Quitting is not an option
The same trainee went through a hard time during her final year. She basically spent a lot of her time crying, and the response was that she was allowed to come in 30 minutes late. She started to see a therapist, and even though we never met, I owe that therapist a lot. Her therapist pointed out that in the three years she had been in post she had never been out for a cup of tea with a colleague, so she was given homework to ask someone out for tea, and she asked me. This was a real turning point for me. We went for tea, and we had a real conversation about the things that were both hard and good. It was the first time that I felt less alone. It was also the start of a conscious decision I made to take people off site for tea, to support better conversations, that I’ve continued to this day.
Later that year, she walked away. She made a decision to go a different way. It took enormous strength to do it, and even now, I have enormous admiration for her. Until that point, I hadn’t known anyone make a decision that prioritised their wellbeing rather than the CV tick boxing. The general attitude was that Healthcare Science is a small world, and you were incredibly fortunate to be a part of it. It was so hard to get into, and you had put in so much that you would be crazy to walk away. There was judgement linked to failed experiments, let alone walking away from the programme. Seeing someone break that mould was incredibly powerful.
The truth is none of these messages are entirely true, so how do we do a better job of messaging for current training programmes?
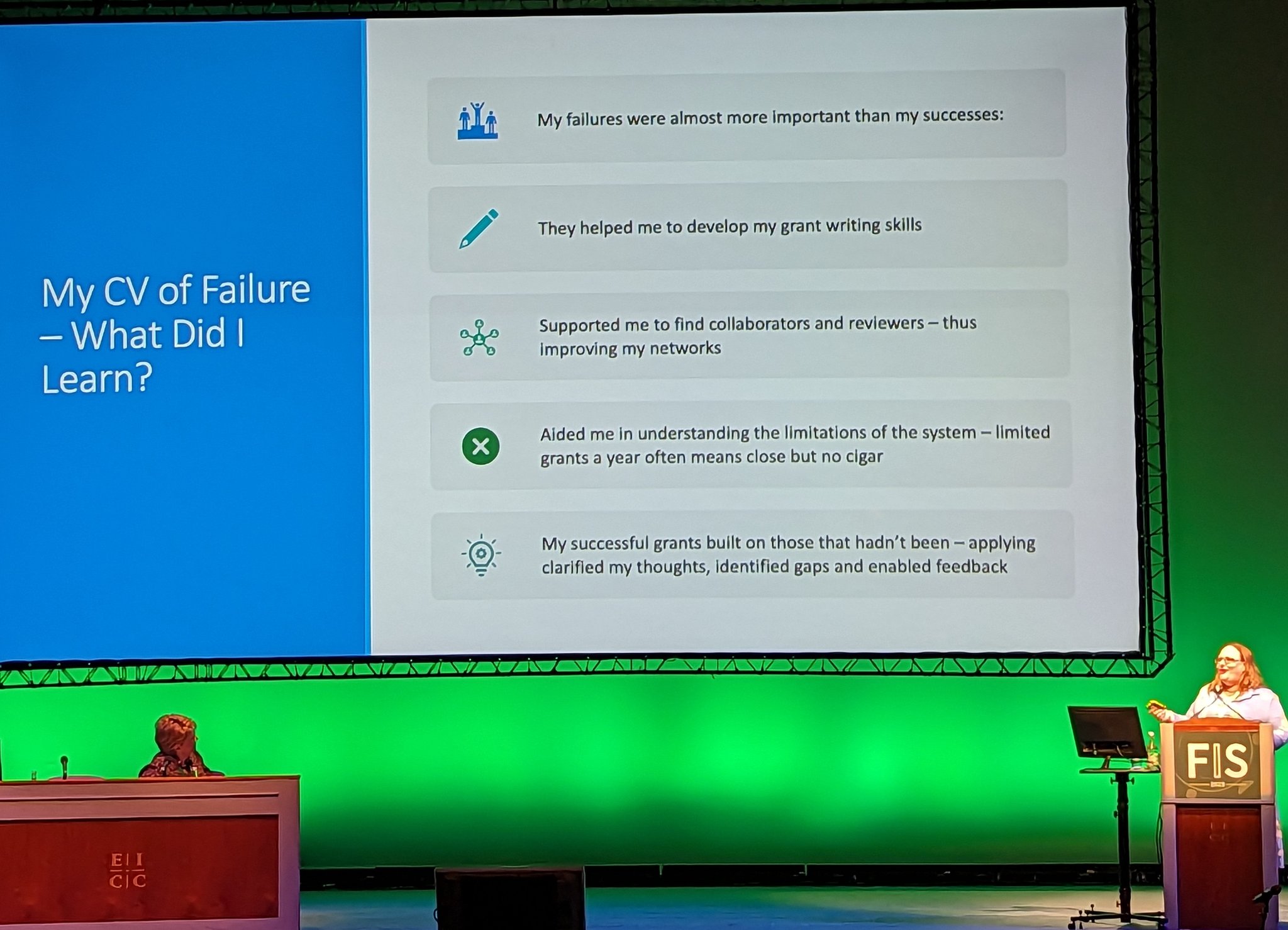
Training is just that, a learning programme, a time to explore, fail, and reflect on those failures in order to learn to do things better. If the messaging I experienced as a trainee now feel less than ideal, what messages should we be encouraging? I’ve been having a think and these are some that I would like us to have better conversations about:
We are more than the sum of our qualifications
Not everyone is going to become a Consultant. Not everyone is going to get FRCPath and a PhD. You know what, that’s perfectly OK. It doesn’t stop you aspiring for those things if that’s what you want. However, our trainees are not in a Hunger Games style competition to be the last one standing. More than that, how good you are at your job is not dictated by how many qualifications you pick up along the way. Some of the most amazing Biomedical Scientists I know and have the privilege to work with don’t have a masters degree. It’s OK to be a brilliant band 7, and be satisfied and fulfilled by the role you have. Your qualifications don’t define your worth, and it’s OK to make choices that aren’t about playing CV bingo. It is also OK to decide that those things matter to you, you still aren’t defined by them. They have the value you choose to give them.

It’s OK to pause and reflect
No career is a straight path, no matter how it looks from the outside. There will be bumps along the way and the odd hill/mountain to climb. You will reach the destination better for it. You will be able to handle the journey a whole lot better if you allow yourself time to pause and reflect along the way. A big part of development is about making time to reflect on where you are and where you are going to, but also asking the big questions about whether those decisions and reflections you’ve made previously are valid for where you are now. You will be working for decades, and the decisions you make in your 20s are unlikely to reflect the decisions you might make in your 40s, so making time for active reflection isn’t a luxury, it’s an essential part of a professional career.

Knowing when to change direction requires courage
In many ways, I’ve been pretty fortunate, the things that I’ve wanted have aligned with my values and have stayed pretty consistent. This could easily have changed, however. I suspect that if I’d been able to have a family, my focus may have altered somewhat. Knowing when to change your focus or direction is important. This a balancing act between knowing when you just need to double down because things are getting difficult, or when you have truly shifted as a person and that you have to change direction to reflect this. Mentorship and coaching can really help with both this and the reflection that may get you to that moment. Acknowledging that continuing down a path ‘just because’ may not be the right thing and that it requires courage to sometimes jump off a cliff and make a big switch is a step that may require additional support.

Your value is not defined by your productivity
This is the one that I struggle with most and therefore know I probably fail to provide the best leadership around. I often feel that ‘I’m do what I say’ not ‘do what I do’ in this area. I often feel defined by my to-do list, and when that gets out of control, as it often does, I place a LOT of judgement on myself. The thing is, if I get hit by a car tomorrow, no one is talking about my to-do list failures at my funeral. I hope that they will talk about how I made them feel, and maybe even this blog. It is hard, but we can choose what defines us. You have that power. One of the reasons this blog is ‘Tales of a recovering workaholic’ is because I recognise I need to change, and I’m hoping to do a better job of playing this on forward and encouraging our trainees to be defined as well rounded individuals with interests outside of work. We need to encourage a holistic view of value in ourselves and others.

There is no prize for working the hardest
The biggest lie I felt that was embedded in my original training programme was that if you just worked hard enough and ticked the required boxes, the prize was there at the end of the race. The hard truth is working hardest does not get you the job. Ticking all the boxes makes the outcome more likely, but it doesn’t guarantee you anything. There is no prize for the most midnight finishes. Trust me, I’ve done enough of them to know. To a certain extent, the prize for working hard is more work. If you set the bar at working most weekends, then your work just expands, so you have to work most weekends in order to keep on top of everything. If you require external validation, like me, this can be a really dangerous game to get into. If we see this in our trainees or ourselves, I think it’s important to recognise and actively find other ways to find that validation before it becomes built in or results in negative consequences.
The next generation of trainees deserve to benefit from the experiences of those that came before, both in terms of knowledge and in learning how we could do it differently. The working environment has changed, as have our trainees and training pathways. By thinking more about our messaging we can make the work place right now more suited to where we want it to be, rather than relying on chance to make it better. Everyone has a role to play, but we, as leaders and educators, should be prepared to lead by example and own the change we wish to see.
All opinions in this blog are my own