
I’m off for some much needed leave enjoying being a Disney adult this week, it’s really needed as between COVID and a broken foot the start of 2024 has not been kind. I’ve called upon a great friend therefore to help me out and write this weeks blog post, so I can focus on drinking cocktails and braving the Tower of Terror. I hope you enjoy reading it as much as I did.
Dr Walker is a paid up member of the Dream Team since 2013, token immunologist and occasional defector from the Immunology Mafia. Registered Clinical Scientist in Immunology with a background in genetics (PhD), microbiology and immunology (MSc), biological sciences (mBiolSci), education (PgCert) and indecisiveness (everything else). Now a Senior Lecturer in Immunology at University of Lincoln. She has previously written many great guest blogs for The Girlymicrobiologist, including one on turning criticism into a catalyst for change.
I’ve written before on this blog about how inspired I was by the work of Professor Ian Davies and Aimee Pinnington on the introduction of clinical simulation to biomedical science education. Clinical simulation is used widely across medical training but to date, has largely been overlooked in biomedical science education. I signed off my last post on this subject with the intentions to build this into my own immunology module on the iBMS accredited course at the University of Lincoln. We are fortunate to have many Health and Care Professional Council registered members of staff across a wide range of disciplines teaching on our course, as well as a very active iBMS liaison committee with links to local laboratories. So I had many wonderful people to pester endlessly with my ideas for how to integrate more clinical simulation across our course. We already do a brilliant job of incorporating our own experiences as healthcare professions into our teaching through both use of case studies and work with simulated patients. My feeling is that enhancing this work with additional clinical simulation practical sessions can only further benefit our students here.
Immunology, in particular, as a discipline lends itself beautifully to clinical simulation as a learning technique. Students often view immunology as challenging due to its complex and multi-faceted nature. It can be seen as dry because we ask them to develop an understanding of abstract concepts and use a diverse array of terminology which often are difficult to pronounce and even harder to remember. I often remind students that though immunologists are quite brilliant, but we probably shouldn’t have been allowed to name our own findings – especially given how frequently we tend to rename molecules. Furthermore, immunology is a notoriously difficult discipline to find placement opportunities in, thus it is essential for students to have authentic learning experiences in this field whilst at university. As such, using clinical simulation to create realistic scenarios which foster active learning and emotional engagement can only help students with this dry, dusty old subject.

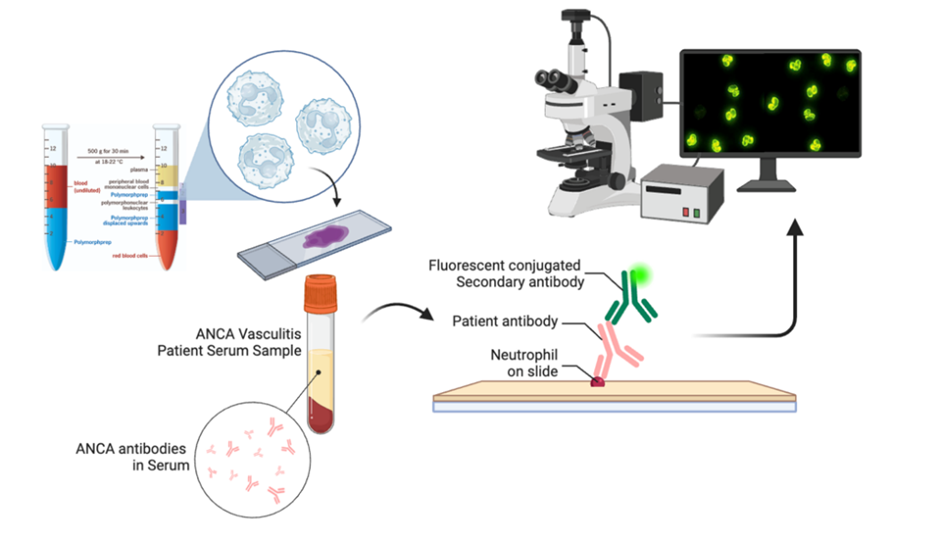
One of the most significant barriers to the introduction of clinical simulation to immunology is the frankly exorbitant cost of the commercial reagents to laboratory practicals. Fortunately, my students here at the University of Lincoln have a dry, dusty old teacher (me!) who remembers the days when we made, rather than bought, all of our kit in the clinical laboratory. To that end, with the help of my favourite histologist Dr Issam Hussain and my delightful mBio student, we have been making ANCA slides and using antibodies to manufacture patient samples for clinical simulation. For those of you who haven’t come across ANCA testing before, this is the preparation of ethanol-fixed neutrophil slides which we use in the clinical laboratory to run immunofluorescence staining to help diagnose patients with autoimmune vasculitis. This is a particularly serious condition which often presents as a clinical emergency and is probably the most urgent test run in the immunology laboratory. The results can be highly subjective and difficult to interpret, with extensive follow-on testing required. The clinical decision is often made based solely on the patient presentation and this single immunology test. Thus, the reporting of these urgent results can be nerve wracking for the most experienced of healthcare scientists. The opportunity to practice this skill in a risk-free environment with a range of clinical scenarios offers the ideal space for students to make mistakes and learn from them without putting a patient at risk. Simulation of this work can help to build confidence and competence, and introduces our students to the concepts of clinical judgment and decision-making.
Before and after the simulation lab session we ran anonymous surveys to evaluate what our students thought of the learning experience. I was delighted to see in our preliminary review of the data that more than 95% of the students felt the simulation improved their understanding of both the techniques and the diagnostic process, and 98% felt that clinical simulation was a good learning experience. With a really significant number of responses, and so few negative comments, I feel my view point on simulation has been reaffirmed. Watch this space. I am now fully committed to the idea that we can really enhance the training of our future workforce of biomedical scientists through this powerful teaching strategy. And thank goodness the students enjoy it too.

All opinions in this blog are my own

[…] the same things, just in a different way, so does it really matter? Well in fact, yes, it does! As Claire has said previously, the pilot study she did had very good results, so the data is there to back up our work. But […]
LikeLike
[…] The first of these posts is written by Dr Walker who is a paid up member of the Dream Team since 2013, token immunologist and occasional defector from the Immunology Mafia. Registered Clinical Scientist in Immunology with a background in genetics (PhD), microbiology and immunology (MSc), biological sciences (mBiolSci), education (PgCert) and indecisiveness (everything else). Now a Senior Lecturer in Immunology at University of Lincoln. She has previously written many great guest blogs for the Girlymicrobiologist, including Exome Sequencing and the Hunt for New Genetic Diseases. […]
LikeLike
[…] Callum is supervised by Dr Walker who is a paid up member of the Dream Team since 2013, token immunologist and occasional defector from the Immunology Mafia. Registered Clinical Scientist in Immunology with a background in genetics (PhD), microbiology and immunology (MSc), biological sciences (mBiolSci), education (PgCert) and indecisiveness (everything else). Now a Senior Lecturer in Immunology at University of Lincoln. She has previously written many great guest blogs for the Girlymicrobiologist, including Exome Sequencing and the Hunt for New Genetic Diseases. […]
LikeLike
[…] Callum is supervised by Dr Walker who is a paid up member of the Dream Team since 2013, token immunologist and occasional defector from the Immunology Mafia. Registered Clinical Scientist in Immunology with a background in genetics (PhD), microbiology and immunology (MSc), biological sciences (mBiolSci), education (PgCert) and indecisiveness (everything else). Now a Senior Lecturer in Immunology at University of Lincoln. She has previously written many great guest blogs for the Girlymicrobiologist, including Exome Sequencing and the Hunt for New Genetic Diseases. […]
LikeLike
[…] Lincoln. She has previously written many great guest blogs for the Girlymicrobiologist, including Simulating Success – Enhancing Biomedical Science Education through Clinical Simulation. This blog was written by a group of her final year students on their experiences of trying to […]
LikeLike
[…] Dr Walker who is a paid up member of the Dream Team since 2013, token immunologist and occasional defector from the Immunology Mafia. Registered Clinical Scientist in Immunology with a background in genetics (PhD), microbiology and immunology (MSc), biological sciences (mBiolSci), education (PgCert) and indecisiveness (everything else). Now a Senior Lecturer in Immunology at University of Lincoln. She has previously written many great guest blogs for the Girlymicrobiologist, including Exome Sequencing and the Hunt for New Genetic Diseases. […]
LikeLike