Content warning – this one is long, and is heavier on the detail than usual. It kind of needed to be as people have died. However, if you want the Cliff Notes version, no, there is no need to panic as Hantavirus is not going to be the cause of the next pandemic.
Everyone seems to be talking about Hantavirus right now, well they were, now people are also talking about Ebola and meningitis. It does rather feel like the infectious disease of the week right now. Despite a lot of effort by scientists and healthcare professionals there seems to be an appetite for panic linked to this. It is worth knowing that although Hantavirus is considered to be a high consequence infectious disease (HCID), that is mainly because it is linked to a potentially severe outcome for an individual if infection is confirmed, rather than potential for wide scale spread.
As I’m being asked about this by everyone from cab drivers to healthcare professionals, and faced with panicked social media commentary about whether this is going to be another pandemic, I thought I should share some of the information that is out there in order to support the ‘don’t panic’ key messaging. I think it is important to note, however, that I am not a Hantavirus expert, just your standard infection prevention and control professional, but having studied zoology in a previous life I couldn’t miss the opportunity to talk about a zoonotic (linked to spread from animals) infection.

What is the current scenario?
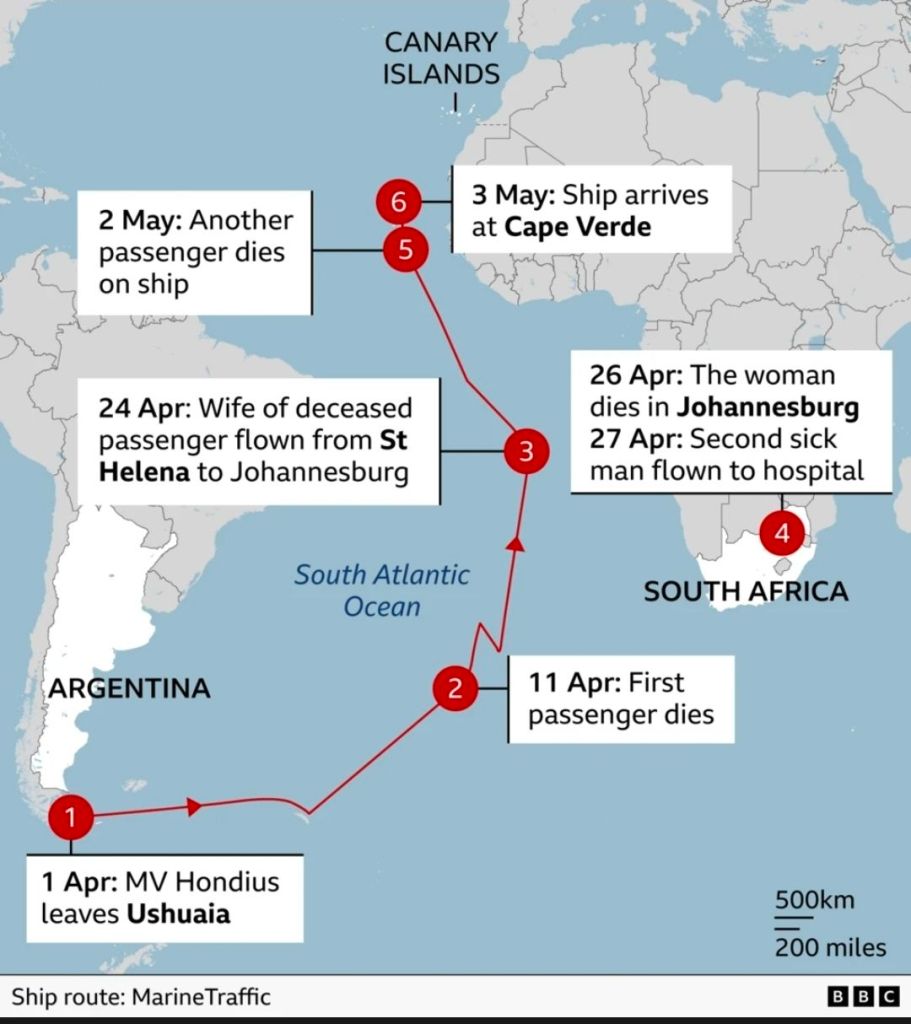
The cruise ship (MV Hondius) that is making headlines departed from Ushuaia, Argentina, on April 1, 2026, and traveled across the South Atlantic Ocean, stopping at several remote locations that including excursions and the opportunity for passengers to get off the ship, standard cruise fare but with more unusual destinations. These included Antarctica, South Georgia Island, Tristan da Cunha, Saint Helena, and Ascension Island.
The ship itself carried 147 people (86 passengers and 61 crew) from 23 different countries, so small for a cruise but still a sizable mix of people to have in one space.

https://www.bbc.co.uk/news/articles/cy0294829ndo
The extent of their contact with wildlife before or during the expedition is either unknown or disputed, although there are plenty of rumours linked to bird watching etc. The importance of all of which will become apparent when we talk more about the virus and it’s standard transmission routes.
It is also worth noting, that unlike many cruises which have a curcular route with all passengers embarking and disembarking at the same point, with this cruise a number of passengers departed at various points as part of planned departures, therefore dissemination of some people involved had already occurred before any clinical symptoms were understood.
Headlines began to appear linked to a possible outbreak onboard in early May, with the outbreak developing, and more information gradually becoming available, as so often happens during any outbreak situation.
What are Hantaviruses?
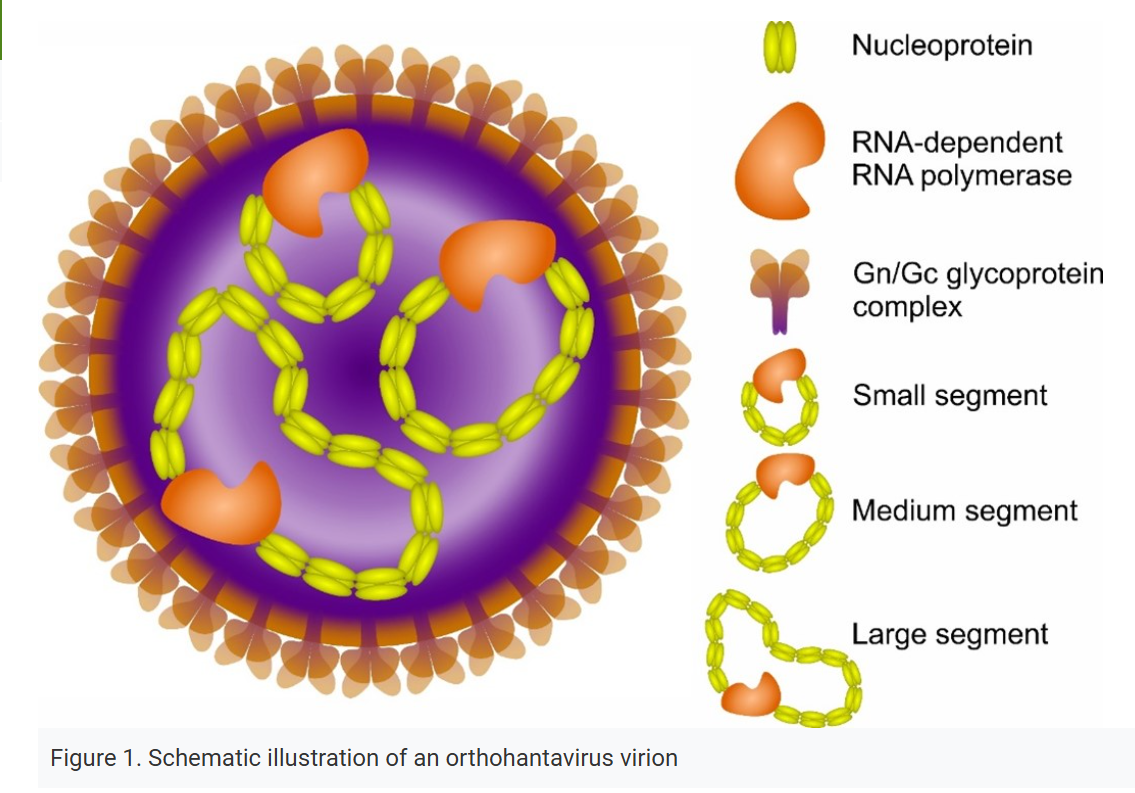
First let’s start with the fact that Hantaviruses are very different from the viruses that we have seen causing pandemics over the last century. Although all three are RNA viruses, Hantaviruses are different in structure, transmission and disease presentation to both coronaviruses and influenza viruses. They demonstrates low comparative rates of mutation and very limited person to person spread, so the same epidemiological principles do not apply.
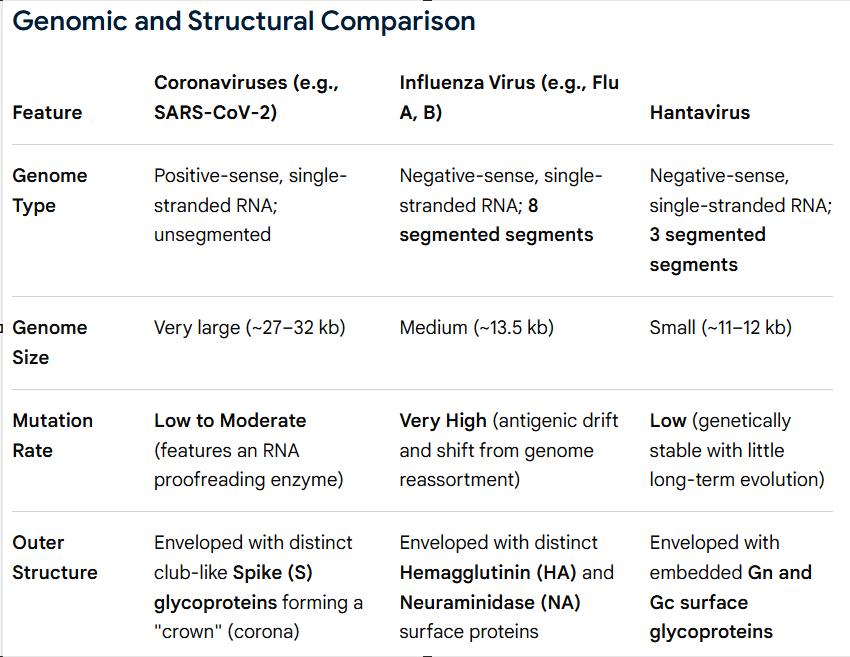
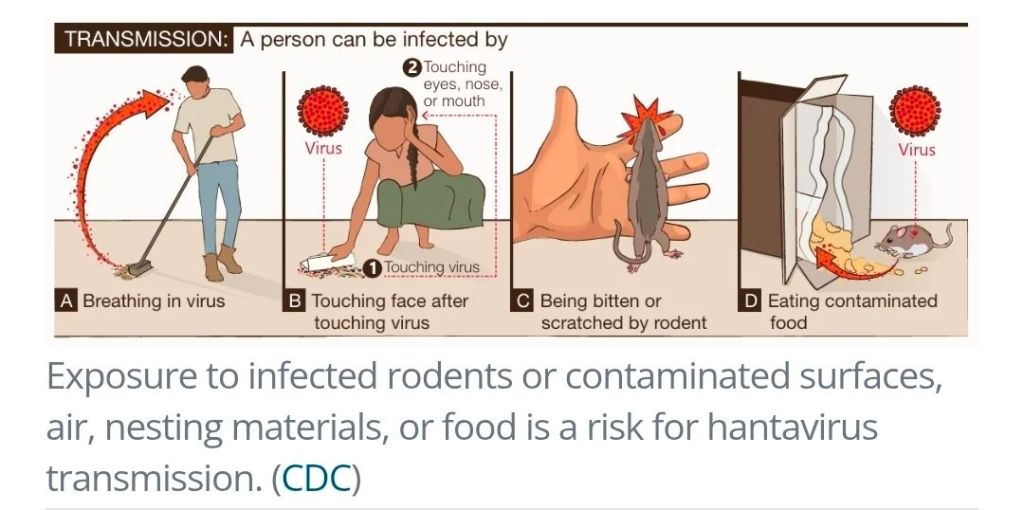
Hantaviruses are RNA viruses that are part of the genus Orthohantavirus. They were named after the Hanta river in South Korea in 1978 (originally called the Hantaan virus) and consist of a family of viruses rather than one single disease, with over 20 species known. As a viral group they have since been split into Old World Hantaviruses and New World Hantaviruses, with viruses found to circulate not just within rodents but also within moles, shrews and other animals. They circulate asymptomatically within their natural zoonotic reservoirs without causing symptomatic infection. When humans are exposed, and infection caused, it is typically due to spread from their normal reservoir with exposure due to interaction with bodily fluids, such as dried urine and droppings.
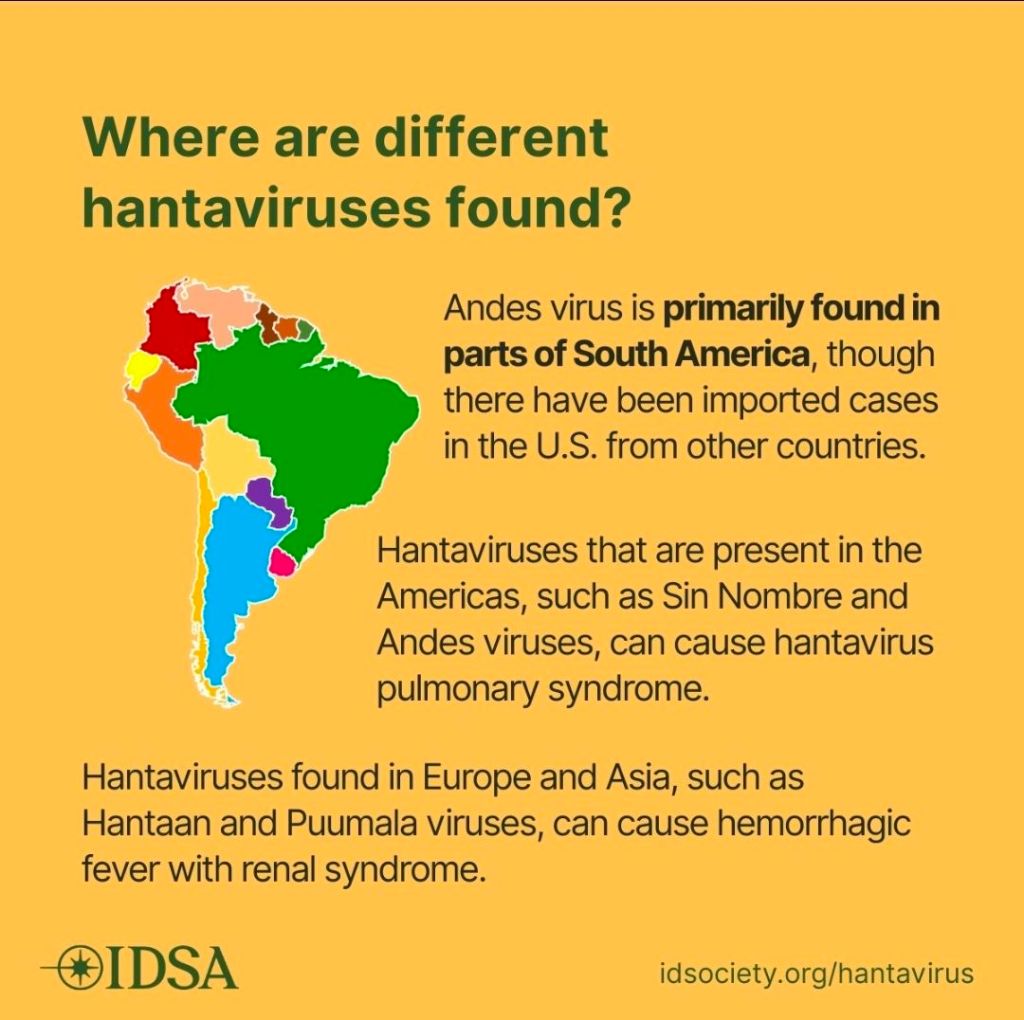
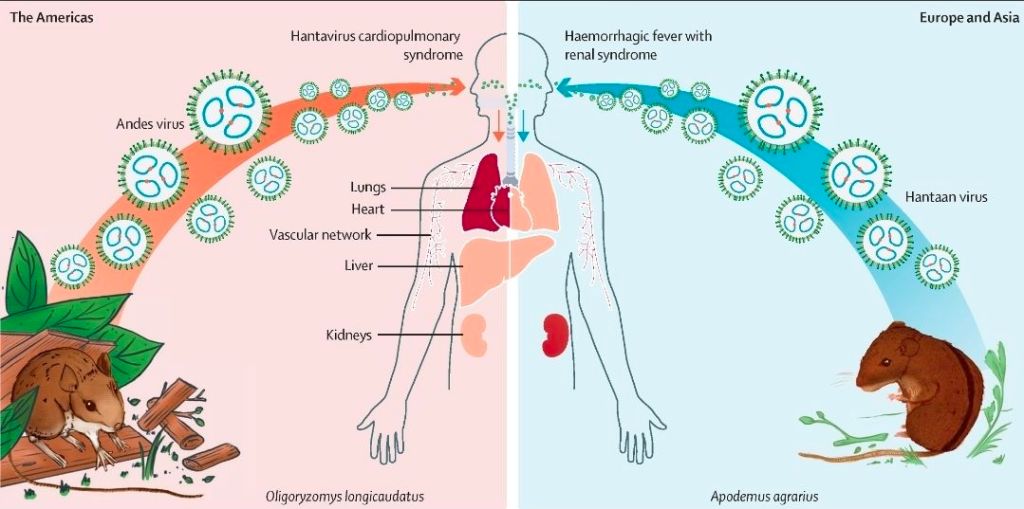
Different Hantavirus species are associated with different animal reservoirs and their associated geographical territories, as well as leading to different clinical presentations in human infection. Old World Hantaviruses are linked with hemorrhagic fever with renal syndrome (HFRS) and are geographically associated with Africa, Asia, and Europe. New World Hantaviruses are associated with hantavirus cardiopulmonary syndrome (HCPS) have a geographical and have a distribution across the Americas, sometimes also called hantavirus pulmonary syndrome (HPS). As the cruise exposure focus is mostly linked to South America, due to both cruise stops and clinical HCPS presentation, the main animal reservoirs of interest are:
- Long-tailed Pygmy Rice Rat (Oligoryzomys longicaudatus)
- Pygmy Rice Rats (Oligoryzomys species)
- Vesper Mice (Calomys species)
Although there have been a number of cases in the current cluster confirmed as positive for the Andes virus, for context, in Europe (according to ECDC), just under 1,900 cases were recorded in 2023 across all different strains/species of Hantavirus. In the Americas, 8 countries reported 229 cases in 2025. There are, therefore, cases of Hantavirus infection detected annually across the globe, and although not huge numbers the impacts on individuals can be significant. The number of cases that are currently being observed linked to the cruise are therefore considered to be an outbreak, but the risk is mainly due to how individuals that will need to be repatriated to their native countries will be managed and how to ensure the best possible outcomes for those exposed.
What are Zoonotic infections?
A zoonosis (or zoonotic infection) is an infectious disease that can jump from a non-human animal to humans. Traditionally it will have no, or limited, ongoing human to human spread. Transmission can be:
- Direct – touching, petting, biting, leading to direct contamination by saliva, blood, urine, or other bodily fluids
- Indirect – exposure to saliva, blood, urine, or other bodily fluids via indirect routes such as contamination linked to food, contaminated environments where animal reservoirs live (soil, water etc), contaminated objects
- Vector borne – not linked to Hantaviruses, but for other organisms can be spread linked to insect carriage and transmission via insect bites
I’ve talked about the fact that Hantaviruses have animal reservoirs. But which animal, depends on the Hantavirus species, which then impacts where there is a risk of acquisition, as you can’t be exposed if the animal doesn’t live there.
Old World Hantavirus animal reservoirs:
- Apodemus (Wood Mice / Field Mice) – Dobrava-Belgrade virus (DOBV)/Hantaan virus (HTNV)
- Rattus (Rats) – Seoul virus (SEOV)
- Myodes (Bank Voles) – Puumala virus (PUUV)
- Microtus (Voles) – Tula Virus (TULV)
New World Hantavirus animal reservoirs:
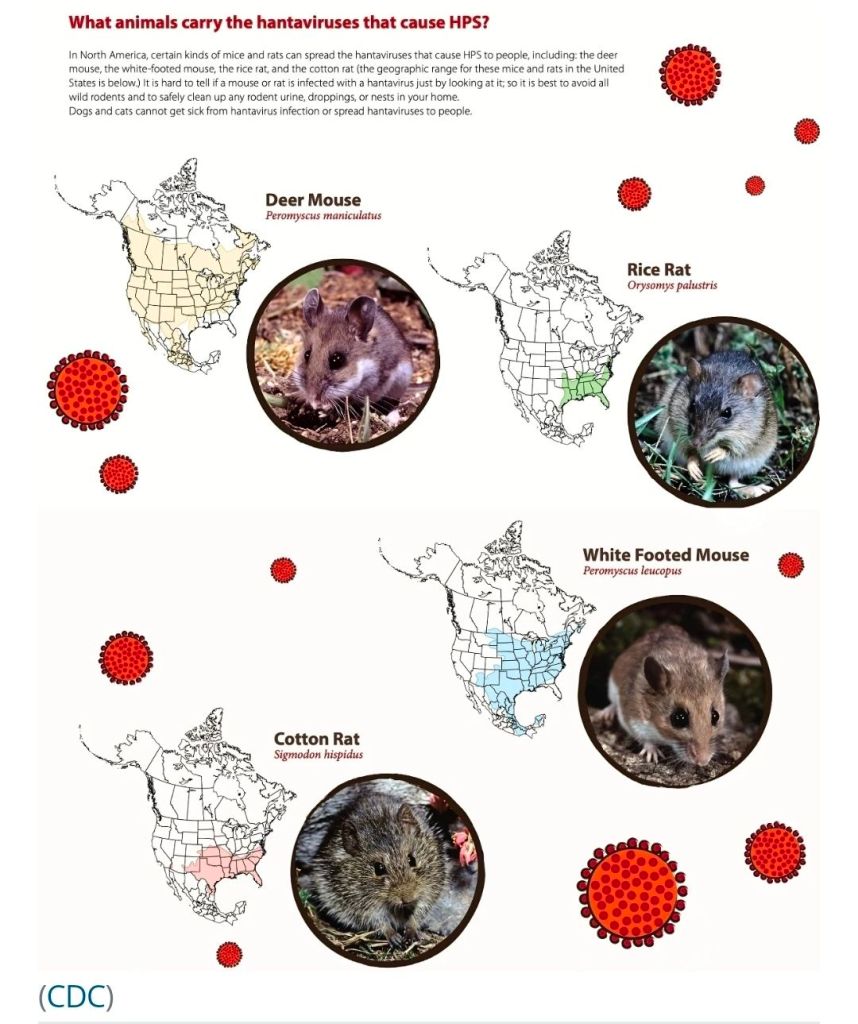
- Deer Mouse (Peromyscus maniculatus) – Sin Nombre virus (SNV)
- White-footed Mouse (Peromyscus leucopus) – New York virus (NYV)
- Cotton Rat (Sigmodon hispidus) – Black Creek Canal virus (BCCV)
- Marsh Rice Rat (Oryzomys palustris) – Bayou virus (BAYV)
- Long-tailed Pygmy Rice Rat (Oligoryzomys longicaudatus) – Andes virus (ANDV)
- Pygmy Rice Rats (Oligoryzomys species) – Andes virus (ANDV)
- Vesper Mice (Calomys species) – Laguna Negra virus (LNV)
The cruise had been visiting remote wildlife areas, so a passenger could have come into contact with the virus then, or before boarding the ship, as the incubation period is prolongued. This can make contact tracing and understanding the epidemiology more challenging, at least initially, and it is possible that the initial transmission event will never be well understood. The animal reservoir associated with the identified Andes virus, the causative agent of the outbreak, long-tailed pygmy rice rat (Oligoryzomys longicaudatus) and Pygmy Rice Rats (Oligoryzomys species) which can help to pin down broad areas, but not precise transmission route.
Transmission
Transmission linked to zoonotic infection happens in two main ways, transmission within the animal reservoir where infection is usually without any symptoms (asymptomatic), and exposure to humans to the virus circulating within the animal reservoir.
Within the animal reservoir transmission can be linked to moments like aggressive acts, such as biting and scratching where saliva or bodily fluids may be transferred. This is probably one of the primary mechanisms. Animals may also share environments leading to close contact, such as sharing nests, and viral transmission can be linked to exposure in close quarters.
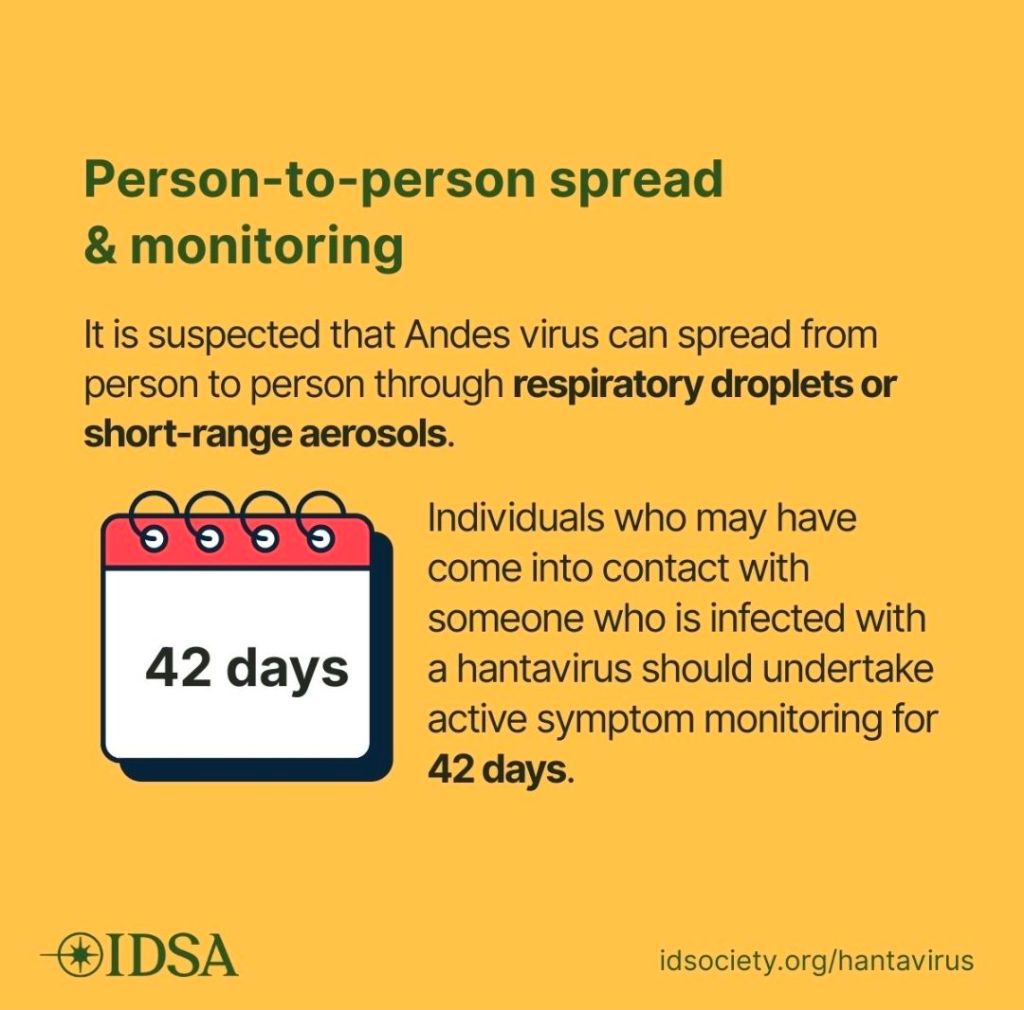
This transmission linked to close contact is also an unusual feature of the Andes Hantavirus and can occur in humans and not just within the animal reservoir. Even so, human to human transmission is relatively rare, but can occur when individuals have prolongued close contact with someone who is symptomatic, especially if exchange of bodily fluids can occur via kissing or other close contact. There is also believed to be an airborne transmission route for the Andes virus, although the route by which this occurs is not well understood. This is addition to the transmission routes from the animal reservoirs that can be due to a number of exposure routes:
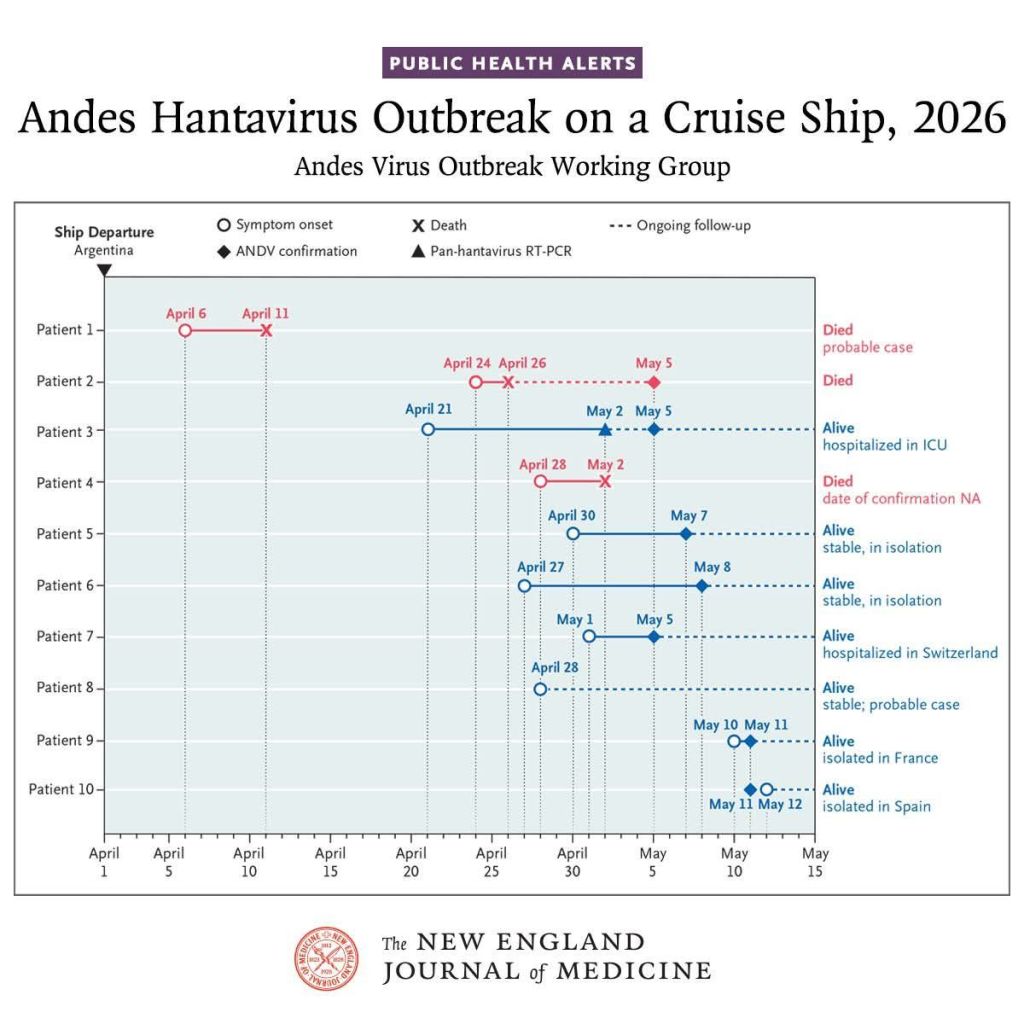
The initial clinical presentation of the 70-year-old Dutch passenger, who developed a fever, headache, and diarrhea day 6 of the cruise, five full days after boarding, and who then died on day 11. This timeline means the passenger is unlikely to have acquired Hantavirus onboard as the minimum Hantavirus incubation is believed to be 7 days, meaning that the exposure was likely to have occurred before the passengers even boarded the ship. Ongoing transmission onboard is therefore unlikely to have been point source from an animal exposure, and is more likely to have been linked to close contact of human passengers.
Clinical presentation
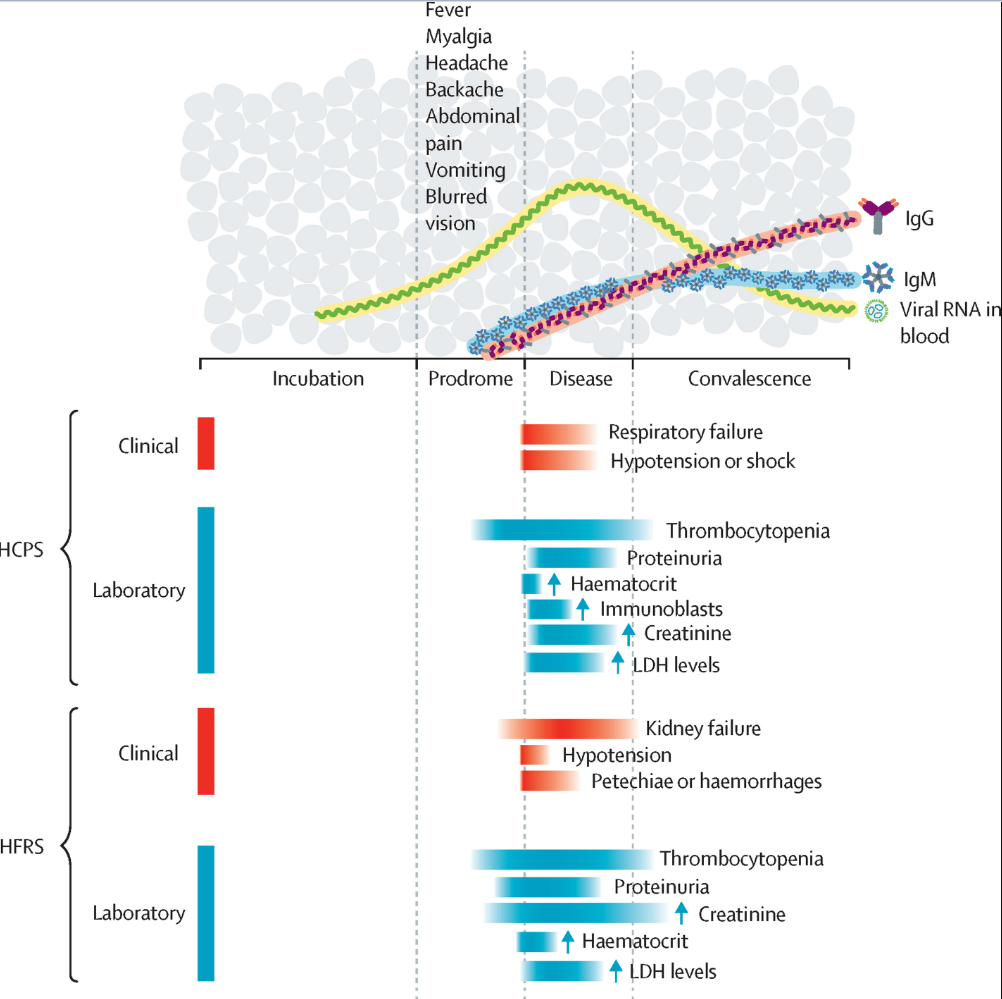
Initial presentation of HCPS is pretty generic, and could easily be hard to recognise as Hantavirus infection without a string travel or exposure history. The prodrome phase, or early onset phase is usually 1 – 5 days long and can occur 4-42 days after exposure. Symptoms can be confused with many other viral illnesses and include:
- High fever, chills, and profound fatigue
- Severe myalgia (muscle aches), particularly in large muscle groups like the thighs and back
- Prominent gastrointestinal symptoms: nausea, vomiting, diarrhea, and abdominal pain
- Headaches and dizziness
One to two days after the initial phase patients can enter a cardiopulmonary phase where patients can become critically unwell:
- Rapidly progressive dyspnea (shortness of breath) and hypoxia
- Noncardiogenic pulmonary edema (fluid in the lungs) and coughing
- Hypotension, tachycardia, and cardiogenic shock
- Potential myocardial depression and acute metabolic acidosis
Hantavirus in humans: a review of clinical aspects and management
The Lancet Infectious Diseases, 2023; 23, e371-e382
This is different to the progression of HFRS, which typically has five phases:
- Febrile Phase (3–7 Days)
- Hypotensive Phase (Hours to 2 Days)
- Oliguric Phase (3–7 Days)
- Diuretic / Polyuric Phase (Days to Weeks)
- Convalescent Phase (Weeks to 6 Months)
The initial febrile phase is still pretty non-specific in terms of presentation, but tends to include high fever, chills, intense headache, severe backache, and abdominal pain. Mortality rates vary by causative species, but range from 1 – 15%.
Hantavirus in humans: a review of clinical aspects and management
The Lancet Infectious Diseases, 2023; 23, e371-e382
Transmission control
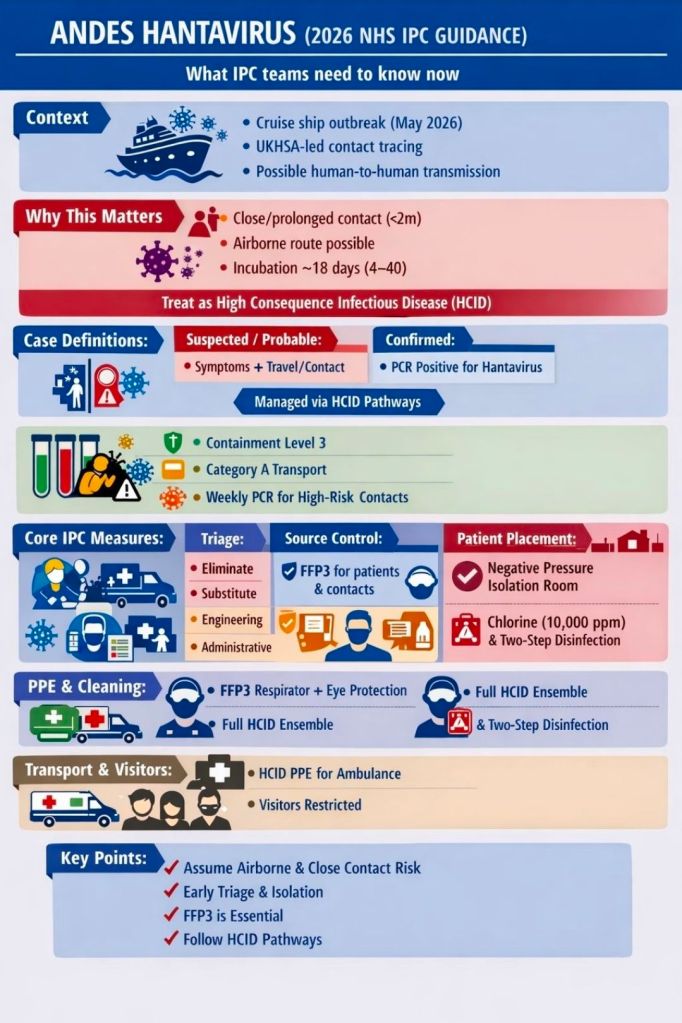
Within the UK, Hantavirus infection caused by Andes virus is classified as a high consequence infectious disease (HCID). HCIDs are defined based on the following criteria:
- Requires an enhanced individual, population and system response to ensure it is managed effectively, efficiently and safely
- Acute infectious disease
- Typically has a high case-fatality rate
- May not have effective prophylaxis or treatment
- Often difficult to recognise and detect rapidly
- Ability to spread in the community and within healthcare settings
Interestingly, only the Andes Hantavirus is listed as a HCID, due to the risk of airborne human to human transmission. Once an HCID is confirmed or highly probable based on a combination of exposure history, symptoms, and diagnostic testing outcomes, the patient will be transferred by specialist transport teams to a designated HCID Treatment Center or High-Level Isolation Unit (HLIU). There are 7 adult and 5 paediatric Airborne HCID Treatment Centres in England, all of whom will hold specialist isolation facilities.
Early diagnosis of Hantavirus infection can be difficult, especially within the first 72 hours of symptoms, before the virus can be accurately detected in body secretions and excretions. Repeat diagnostic testing is often done 72 hours after symptom onset. As the initial presentation is fairly generic, it can take some time to realise what additional testing is required, and a good travel and activity history is key to informing diagnostic steps.
Within the UK, diagnostic testing options include:
- Serology (Blood Tests): This is the primary diagnostic method. Laboratories use Enzyme-Linked Immunosorbent Assays (ELISA) or immunoblot assays to detect hantavirus-specific Immunoglobulin M (IgM) which looks for recent infection and IgG antibodies which looks for more established immune response, both by testing blood serum samples.
- Molecular Testing (RT-PCR): Reverse transcription-polymerase chain reaction (RT-PCR) is used to detect hantavirus viral RNA in acute blood or blood samples during the viraemic phase, when the virus is present within the blood stream.
Internationally, one of the challenges for control in this specific outbreak, was that this wasn’t a point source exposure where everyone is incubating according to the same time frame, as people left the ship at different times, and were also isolating onboard the ship over different time periods based on the level of contact with the initially cases. This made initial components of contact tracing challenging, which then led to further possible exposures as some of the initial passengers returned to their home countries before the extent of the outbreak was understood.
Clinical management
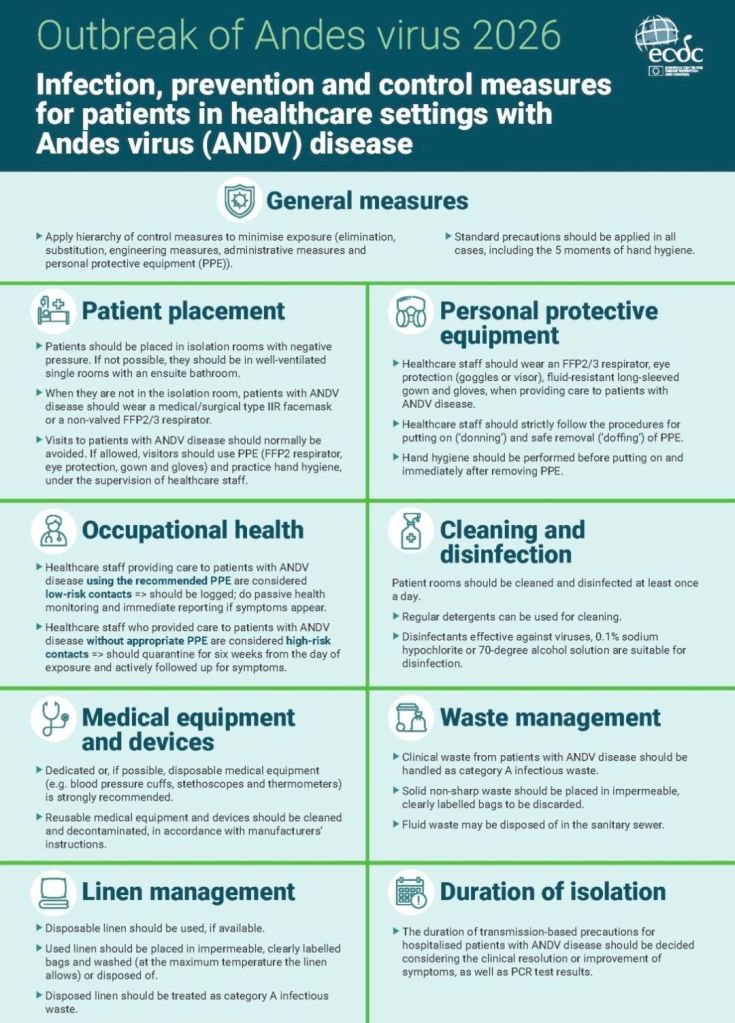
There is no specific antiviral treatment option for Hantavirus so management focuses on supportive therapy, respiratory support (often in intensive care), fluid management, and for HFRS dialysis. Among patients who have severe respiratory symptoms as part of HCPS, the case fatality rate has been estimated to be approximately 38%.
As part of the follow up for this current outbreak, UK nationals, once repatriated have been taken to an isolation facility where they will be kept for up to 72 hours and initial clinical review and testing will be undertaken. As part of this clinical teams will then assess whether contacts who are not displaying symptoms can isolate at home or at another suitable location based on their living arrangements. Exposed individuals are generally being advised to self-isolate for up to 45 days from their last known exposure, but this self-isolation is voluntary. During the isolation period clinical networks will maintain daily contact to check for potential symptoms and undertake regular testing.
The World Health Organization (WHO) has recommended a 42-day quarantine period for the cruise passengers from their last exposure, although within the UK this has been extended to 45 days. Cases are managed, if symptoms develop using the following case definitions:
- Confirmed Case: A patient with positive PCR testing for hantavirus in clinical samples, combined with travel on the MV Hondius from 1 April 2026 or contact with a passenger within 45 days of symptom onset.
- Probable Case: A patient with compatible symptoms (e.g., fever, respiratory distress) and no other identified pathogen, linked by travel or close contact to the MV Hondius outbreak.
- Possible/Suspected Case: A patient with compatible symptoms and no other identified pathogen, who had contact with a MV Hondius passenger within 45 days of symptom onset.
Previous outbreaks
Although all of this information seems rather intense and it is easy to see why the new media are trying to make a big story out of it, apart from those exposed we do need to put this outbreak into context. Outbreaks of Hantavirus happen with relative frequency, probably more than we know as diagnosis can be difficult identification may be underestimated, and some local outbreaks are probably under reported. To help demonstrate this I’ve put together a list of previous, easy to find, outbreaks along with their case numbers:
- Argentina Regional Outbreak (Late 2025 – Early 2026)
- Cases: A spike in localized regional cases with the NEJM reporting 34 cases from a single event.
- Deaths: Up to 20 deaths.
- Germany Voles-Linked Surge (2025)
- Cases: 55 cases in the first half of the year (predominantly in Bavaria)
- Driven by an ecological spike in the local bank vole population.
- Brazil Farmland Outbreak (September 2022)
- Cases: 22 cases.
- Deaths: 10 deaths.
- Traced to wood and rice mice exposure on agricultural properties.
- Episodic Outbreaks in Los Santos, Panama (2022)
- Cases: 29 cases recorded over nine months.
- 16 manifested as severe HCPS; no fatalities reported.
- Argentina Andes Outbreak (2018)
- Cases: 34 confirmed cases.
- Deaths: 11 deaths.
- Someone sick with ANDV attended a birthday party with 100 people; 5 people who were seated close to the individual later developed symptoms
- Yosemite National Park, USA (2012)
- Cases: 10 confirmed cases.
- Deaths: 3 deaths.
- Contracted by visitors staying in signature tent cabins infested with deer mice.
- Chili (1997 – 1998)
- Cases: 25 cases were officially recognized as part of the primary outbreak wave from July 1997 to January 1998.
- When expanding the surveillance period from October 1995 through January 22, 1998, a total of 33 cases were confirmed nationwide
- Epidemiologists verified human-to-human transmission across two out of three family clusters identified during the outbreak
- The Korean War Epidemic (1950–1953)
- Cases: 3,000+ UN soldiers infected.
- The landmark historical event that first clinically defined Hantavirus Hemorrhagic Fever with Renal Syndrome (HFRS)
What is currently happening with this outbreak?
As this post has taken me a couple of weeks to pull together, I thought it was worth ending with the latest update I have available from the European Centre for Disease Prevention and Control (ECDC) on 24 May. At this point 12 cases have been reported in total, including 10 confirmed and 2 probable cases. One new case and no new deaths have been reported since the previous update (unclear when the last update was).

The cruise ship M/V Hondius has had all passengers and crew disembarked and is currently docked in Rotterdam, the Netherlands, undergoing sanitation procedure.
Do I need to be concerned?
The short answer is no, I don’t believe so and neither do many people who are far more expert than I that you will hear write and talk on this subject. This scenario has got me thinking though, if this outbreak hadn’t impacted European and US passengers whether we would have even heard about this outbreak at all. As you’ve seen in the outbreak section, Hantavirus outbreaks are not that uncommon. Was it because of passenger social media that it made headlines, because the cruise industry is big business, or because it impacted audiences because they saw passengers as being ‘like them’ and worrying that they too could be impacted on a holiday?
I think, whatever the reason, that this should be used as a wake up call for all of us to realise that infection diseases are global, and that we ignore infections that we don’t consider to impact ‘us’ at our risk. With global travel, with climate change, with changes in health surveillance due to certain US policies, the old way of looking at infectious diseases may not be fit for purpose. Too much of the world is in pandemic denial, and just doesn’t want to think about infection risk. We either experience coverage that induces panic, or ostriching where we don’t talk about it at all. Neither of these approaches are going to lead to the best outcomes or knowledge sharing in the face of a changing infection landscape. What needs to happen is for global networks to be built, for infrastructure to be invested in, and for communication to occur in a way that supports surveillance and knowledge acquisition. I don’t believe that Hantavirus is a risk for developing a new pandemic, but if we don’t take the time we have available to invest in planning, we won’t be as prepared for the next outbreak that could be.
Reading you might find interesting
Curr Treat Options Infect Dis. 2020 Oct 29;12(4):410–421. doi: 10.1007/s40506-020-00236-3
BBC News – Hantavirus may have spread between passengers on cruise ship, WHO says – BBC News
https://www.bbc.co.uk/news/articles/cm2p186gyp2o
BBC News – Cruise passengers tell of life on board stranded ship after hantavirus outbreak – BBC News
https://www.bbc.co.uk/news/articles/clype7ededzo
BBC News – Hantavirus: Race to trace passengers who left MV Hondius at St Helena – BBC News
https://www.bbc.co.uk/news/articles/cnvpzgn26edo
BBC News – Hantavirus strain that spreads between humans found in cruise ship passengers – BBC News
https://www.bbc.co.uk/news/articles/ce8pypvjx1ko
BBC News – Britons on hantavirus cruise ship face 45 days of self-isolation – BBC News
https://www.bbc.co.uk/news/articles/c9wepl8we90o
BBC News – British passengers on virus-hit cruise ship to isolate on Wirral – BBC News
https://www.bbc.co.uk/news/articles/c2029r42w8wo
BBC News – Tourist hotspot at ‘end of the world’ denies causing hantavirus outbreak
https://www.bbc.co.uk/news/articles/cx21ej471g2o
All opinions in this blog are my own