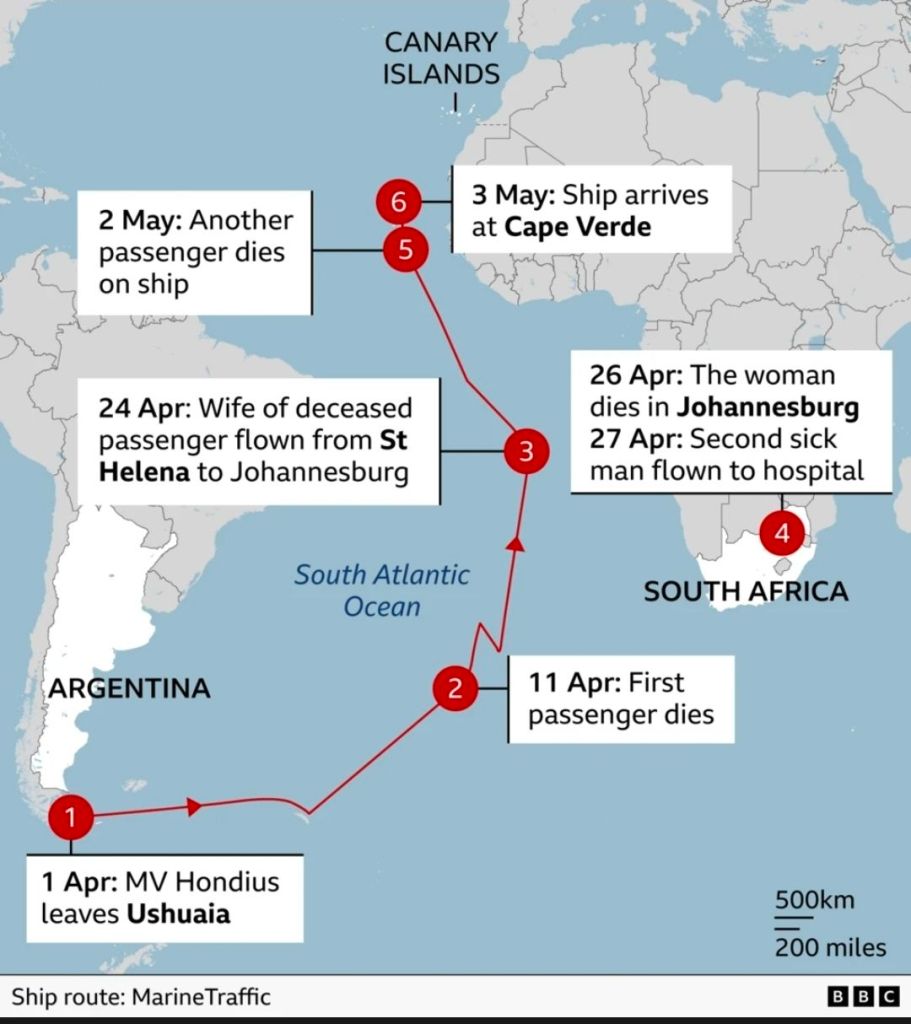
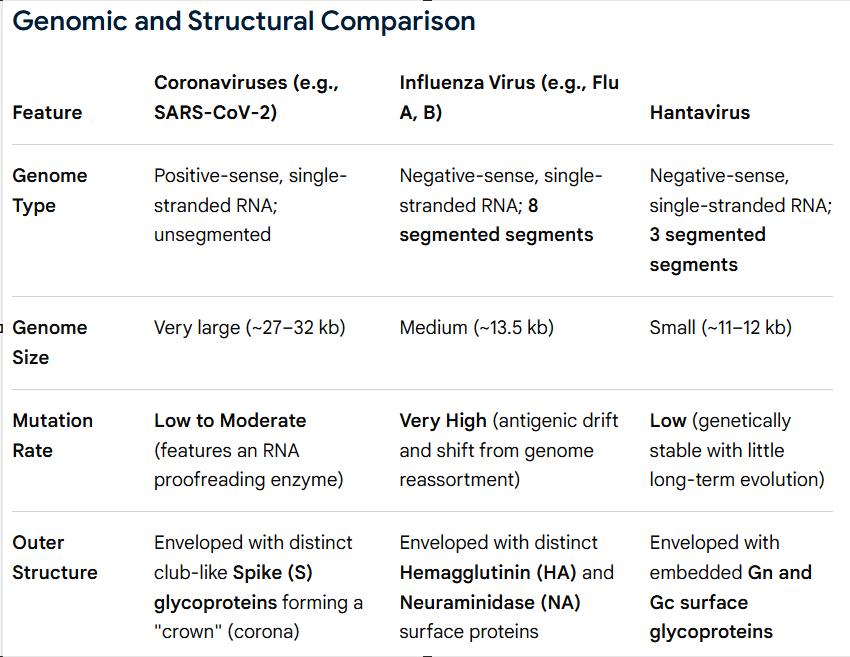
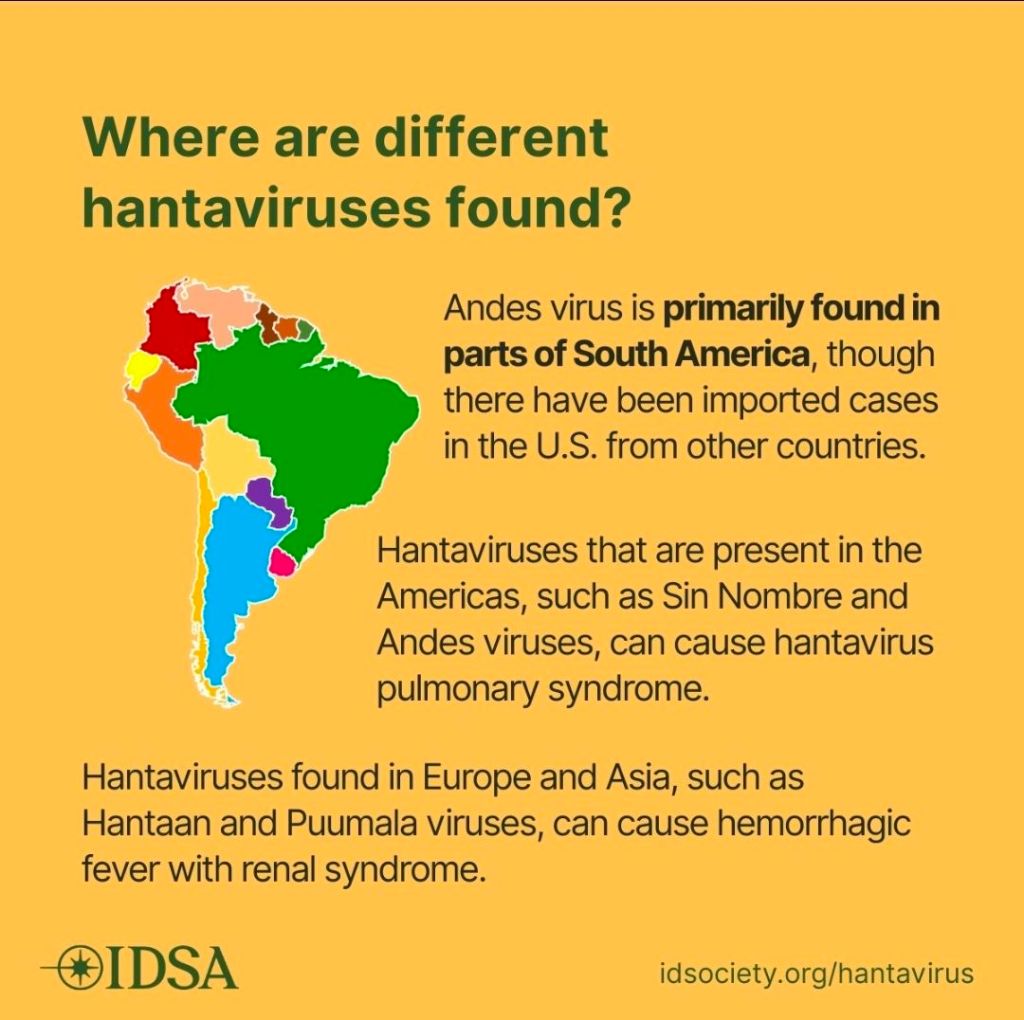
Infectious diseases have been in the news a lot over the last few months, between Hantavirus, Listeria and raw milk, and even Screwworm in cattle, it is hard to ignore the headlines, and after the pandemic it feels like every news article declares a risk to all human life. Ebola is, however, an incredibly difficult virus to manage, with devastating consequences for both countries and communities and so despite the instinct to hide from the reporting we need to continue to engage with the information that is coming out.
From an infection point alone this outbreak is worth discussing, but it is especially pertinent because aside from the impact it has locally, is the fact that the number of people currently dying and infected has likely been directly impacted by global policy choices linked to de-funding United States Agency for International Development (USAID). Combine this with the US decision to pull out of the World Health Organisation (WHO) reducing funding for international health responses, has resulted in a public health emergency that took longer to detect, and now requires managing with both less resources, and less available expertise of previous pandemics. All of which lead to making an already difficult and dangerous situation considerably more challenging.
We live in a global community, and the idea that you can step away from global responsibilities without consequence is more than delusional, it is dangerous, so ‘sorry, not sorry’ for the politics in this one, I think it’s too important to ignore.
Previous outbreaks
There have been a number of Ebola outbreaks since the Ebola virus was first identified in 1976. The initial outbreak included two near-simultaneous outbreaks in Central Africa: one in Yambuku, Zaire (now the Democratic Republic of the Congo), near the Ebola River, and the other in Nzara, Sudan (now South Sudan). The largest outbreak, and the one many of us will remember due to both the substantial media coverage and global health response, occurred in and around Sierra Leone. This 2014–2016 outbreak had more than 28,600 cases reported.
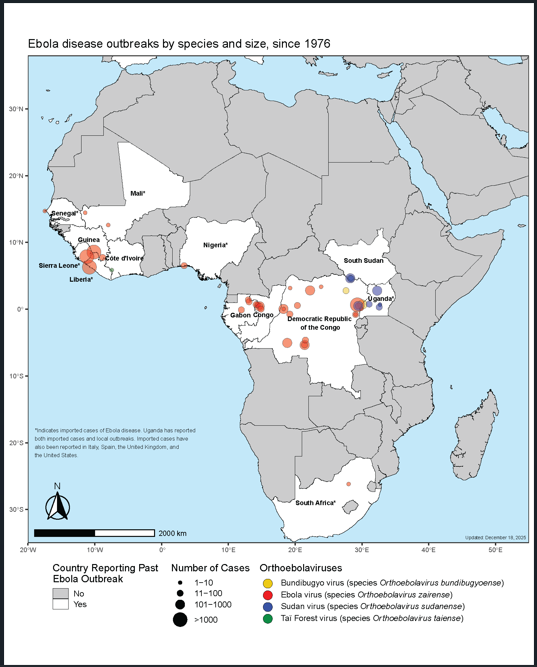
The Centres for Disease Control (CDC) figure show these outbreaks, and the causative Ebola virus (see Ebola virus section below for more details on viral species).
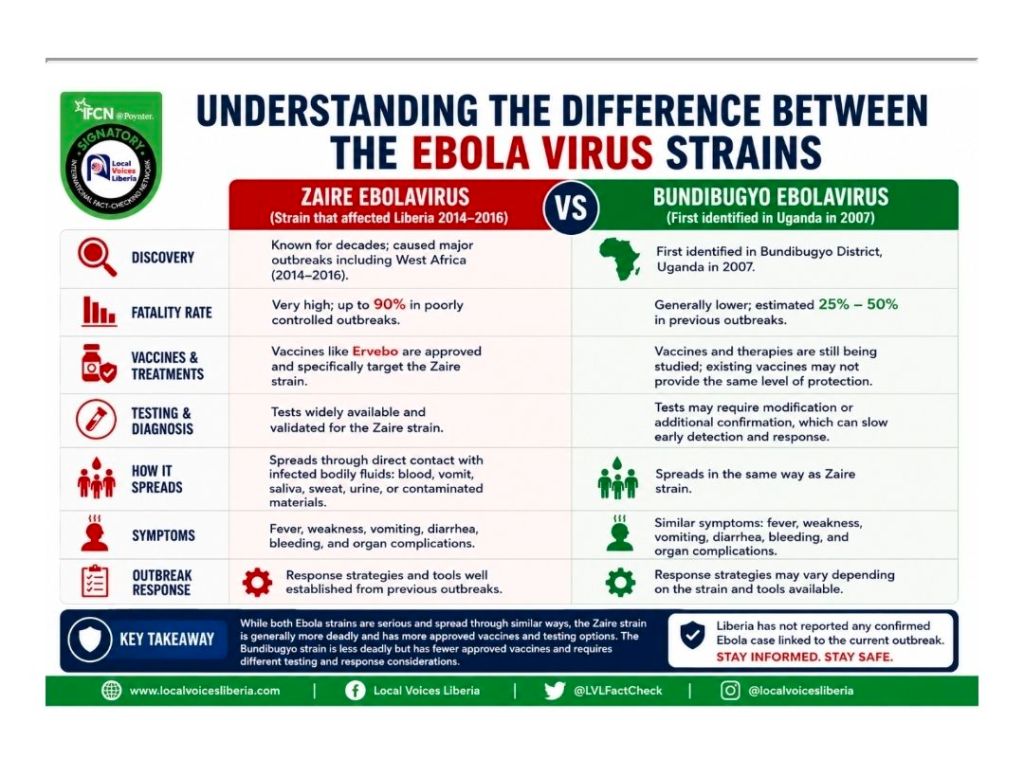
The key takeaway is that the virus causing this outbreak, the Bundibugyo virus, is a rare cause of Ebola virus outbreaks, with considerably less know and understood about how the virus is transmitted, and how it can be detected and managed. This leads to an even greater need for a rapid global response, both in terms of public health, but also in terms of research focus. Making the delay in both even more impactful, and the need for us to get on top of it even more urgent. Some of our prior learning can be ported, but so much of it cannot.
The current outbreak
On the 17th May the WHO declared the current scenario in the Democratic Republic of the Congo (DRC) and Uganda a public health emergency of international concern, but what does this mean? Well, the WHO defines it as of an extraordinary, sudden, or unexpected public health event with a risk to other countries through the international spread of disease, potentially requiring a coordinated global response.
On the 5th June the African Centres for Disease Control and WHO launched a joint Ebola continent preparedness and response plan of $518 million to support African countries to prepare for, rapidly detect, and respond to the outbreak.
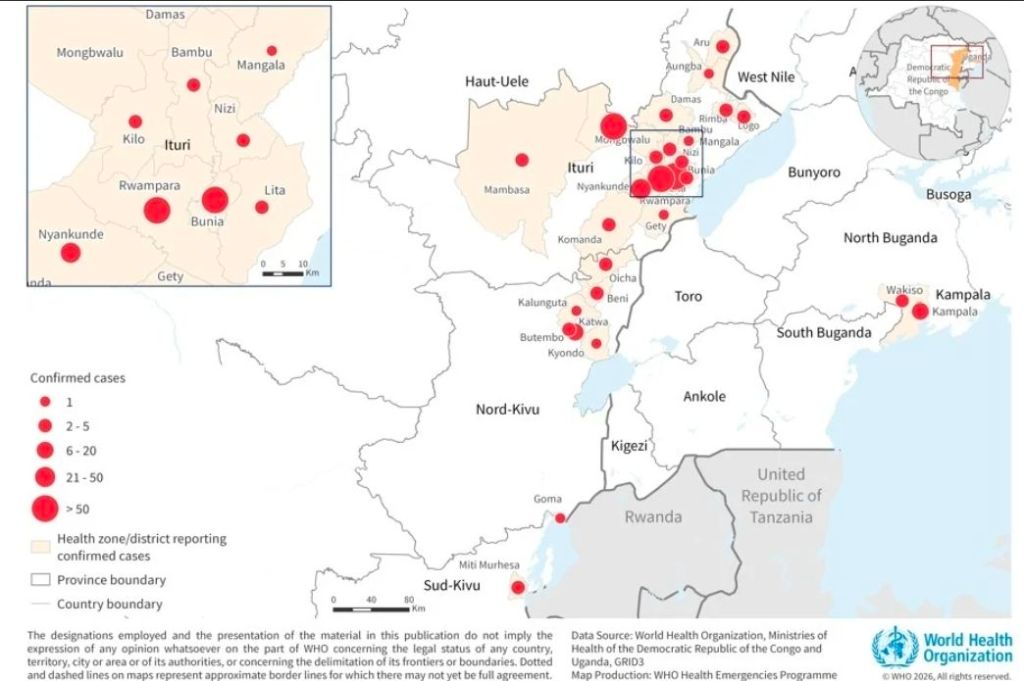
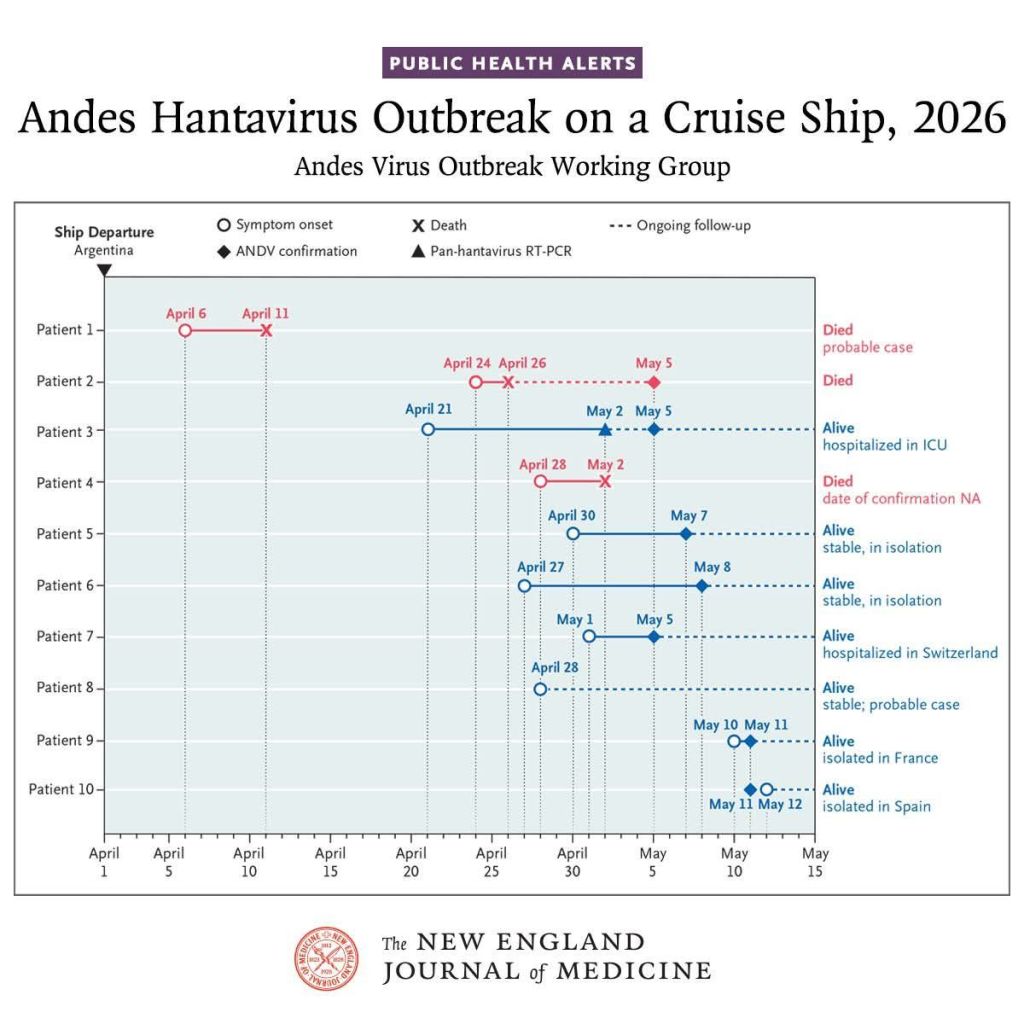
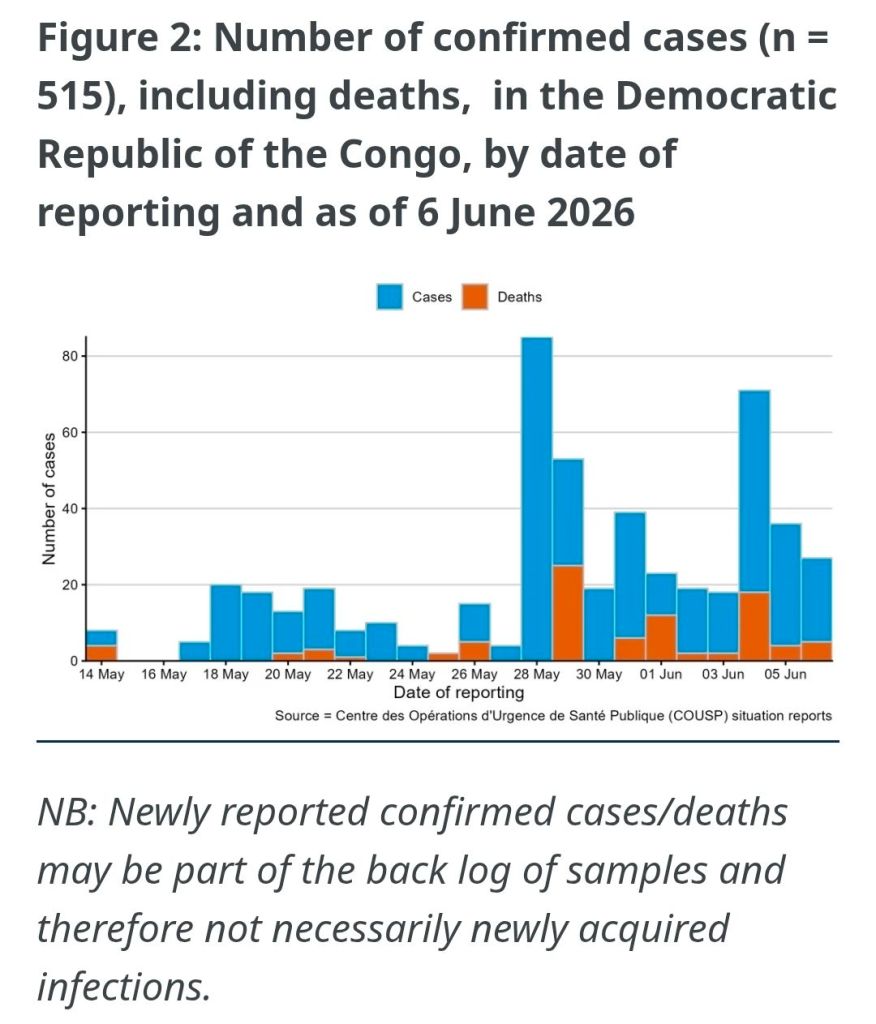
Ebola virus has a number of different variants, and the current outbreak is caused by the Bundibungyo virus. As of the 6th June there have been 515 confirmed cases, with 91 deaths (17.7%). Uganda has 19 confirmed cases and 2 deaths (10.5%). It is worth considering that these numbers are likely to be a significant under estimate, as laboratory backlogs, plus some level of distrust in healthcare systems, are likely to lead to a reduction in confirmed cases, but I’ll discuss the difference between confirmed, probably, and possible cases later. At the moment, all onward cases are still linked with travel to DRC, but patients are currently being treated or followed up in a number of countries outside of Africa, including in Brazil, Germany, and Italy.
What is Ebola virus?
Well, the first thing to realise is that it is not a single virus. Ebola viruses are part of the filoviridae family, most commonly referred to as Filoviruses. They are zoonotic pathogens (associated with animals) that survive in what are known as reservoir species. These are non-human reservoirs, possibly bats, where the virus can circulate without harming the host and leads to occasional spillover into humans where disease is then detected. Ebola disease (EBOD) is a rare and often severe illness in humans that is frequently fatal.
Ebola disease is caused by a group of viruses that belong to the Orthoebolavirus genus of the filoviridae family. Six species of Orthoebolaviruses have been identified to date,with 4 causing disease in humans, three of which are known to cause large outbreaks: Zaire Ebola virus, Sudan virus and Bundibugyo virus. The zoonotic reservoirs are not well understood for Ebola viruses, unlike those for Marburg viruses where a host reservoir has been established by direct isolation from bats.
NB Marburg disease (MARD) caused by Marburg virus was the first filovirus to be discovered in 1967 and also causes disease in humans, but is not an Ebola virus. Ebola Reston virus (RESTV), is another Ebola virus that has been detected in humans but appears to infect them sub-clinically i.e. with no symptoms, and so transmission routes and impacts are not well understood. It does however cause EBOD disease in non-human primates and has been detected in animals such as pigs in the Philippines and China, so there may be a zoonotic reservoir for this virus similar to other members of the genus. This is the virus that featured in The Hot Zone book by Robert Preston, based on the New Yorker article Crisis in the Hot Zone (1992).
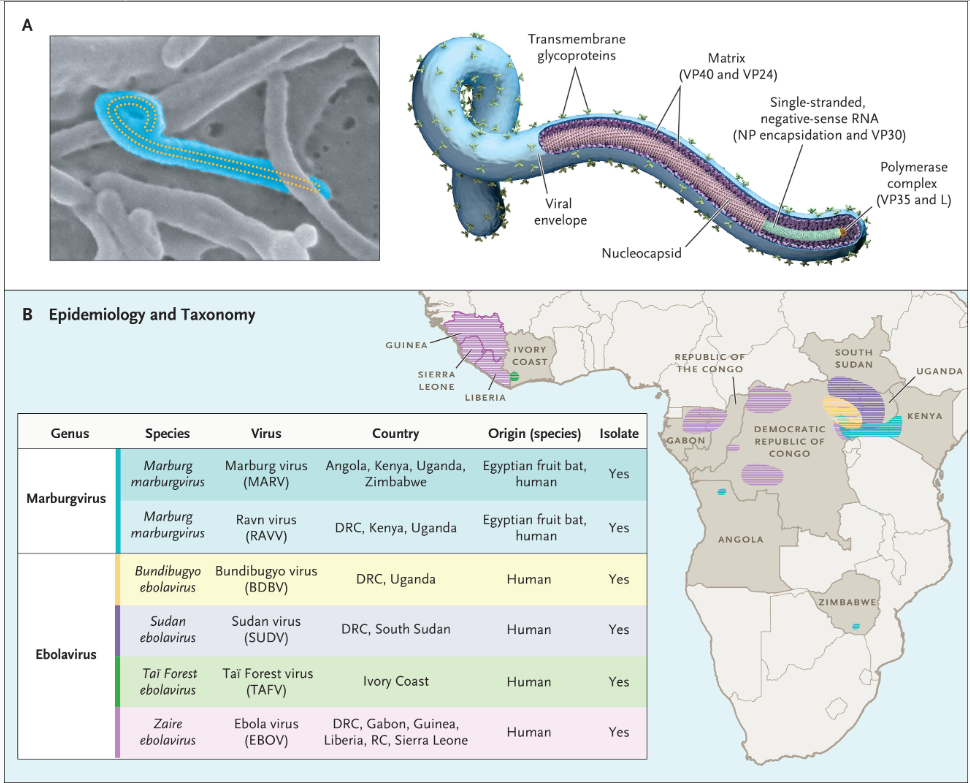
Filoviruses are enveloped, non-segmented, negative-sense RNA viruses. The genomes between Bundibugyo and Zaire Ebola species differ by about 30%, and the pathogenesis and clinical outcomes also appear to differ, but there is still limited information regarding the viral mechanism/s that lead to these differences. Importantly, it is worth noting that the cause of the current outbreak, Bundibugyo Ebolavirus, behaves differently in terms of mortality than the more commonly detected outbreak species. Vaccines and other targeted therapy are also not yet established, as the virus has been seen much less frequently.
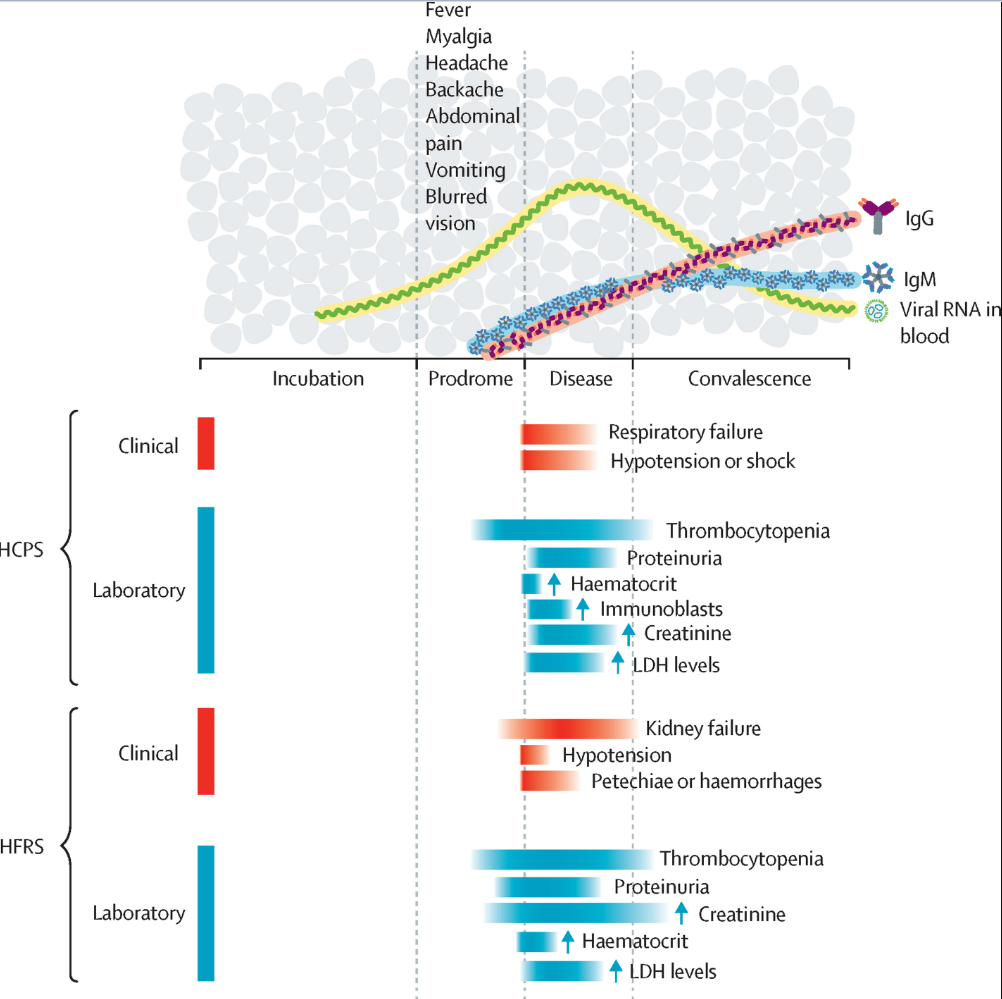
What are the symptoms?
Patients usually have an initial non-specific presentation which includes fever with malaise (discomfort/unease), fatigue, and myalgia (muscle pain). A few days after this, patients may develop gastrointestinal infections that can include anorexia (loss of appetite), nausea, vomiting, and diarrhoea. Although many people associate EBOD with haemorrhagic fever (i.e. temperatures and bleeding), bleeding abnormalities actually occur in less than half of patients. If bleeding is present, it is usually linked to bleeding from the gums, subconjunctival haemorrhage (broken blood vessels in the eye), and blood in vomit and stool.
The incubation period is between 2 to 21 days (typically, 6 to 10 days) and probably depends on the Ebola virus, as well as the exposure dose and route.
Diagnosis and patient management
Diagnostic testing for Ebola is mainly via reverse transcription–polymerase chain reaction (RT-PCR) targeting the RNA of the virus, but it is made more challenging because it can only be detected in blood once symptoms appear. It is also possible to use Antigen-Capture Enzyme-Linked Immunosorbent Assay (ELISA) tests, these are often less sensitive but easier to implement. Point of care tests, finger prick tests, can also be used but they again have much lower sensitivity than PCR. Many of these tests have been designed for the main outbreak strains of Ebola, and so modification may be needed to allow detection of the Bundibugyo virus, or test sensitivity may be further reduced.
Once patients have developed symptoms, especially during this outbreak as there is a lack of specific treatment options, the main response is linked to supportive care:
- Fluid & electrolyte resuscitation as patients have severe fluid loss from diarrhoea and vomiting
- Cardiovascular support as patients frequently go into shock
- Respiratory support, as patients enter respiratory failure, using equipment such as ventilators
- Symptom management as patients may end up needing dialysis for renal failure
Most of which require complex medical equipment which may not be available, or available in large enough numbers within local treatment centres. Lack of equipment availability and access to supportive treatments directly impacts clinical outcomes. The mortality (death) rates without treatment also show a great disparity between Ebola viruses:
- Ebola Zaire: 90% (20 – 40% with early treatment and supportive therapy intervention)
- Sudan virus: 50% (no approved vaccines or specific antiviral therapeutics available)
- Bundibugyo virus: 30% (no approved vaccines or specific antiviral therapeutics available)
Although there isn’t currently an established treatment for Bundibugyo virus, Peter Stafford, the US doctor who contracted Ebola in DRC and was flown to Germany, has been treated with an experimental antibody MBP-134. The BBC has also reported that three vaccines are currently in development which would target the glycoprotein of the Bundibugyo Ebola virus.
Each vaccine aims to train the body to spot the same structure on the surface of the virus but each uses a different technology in order to support an immune response. All three still require testing using clinical trials, and so although it is good that vaccines are being developed, their ability to influence the outbreak is currently still unknown.
For patients that recover, post infection morbidity (long term effects) have not always been well captured due to the devastating impacts of the outbreaks themselves, but during the 2014–2016 EBOV epidemic caused by Ebola Zaire, musculoskeletal pain, headache, encephalitis, and ocular problems were noted in survivors and were referred to collectively as the “post-Ebola syndrome.” Recovery, therefore, can be a protracted process and is likely to vary by causative species.
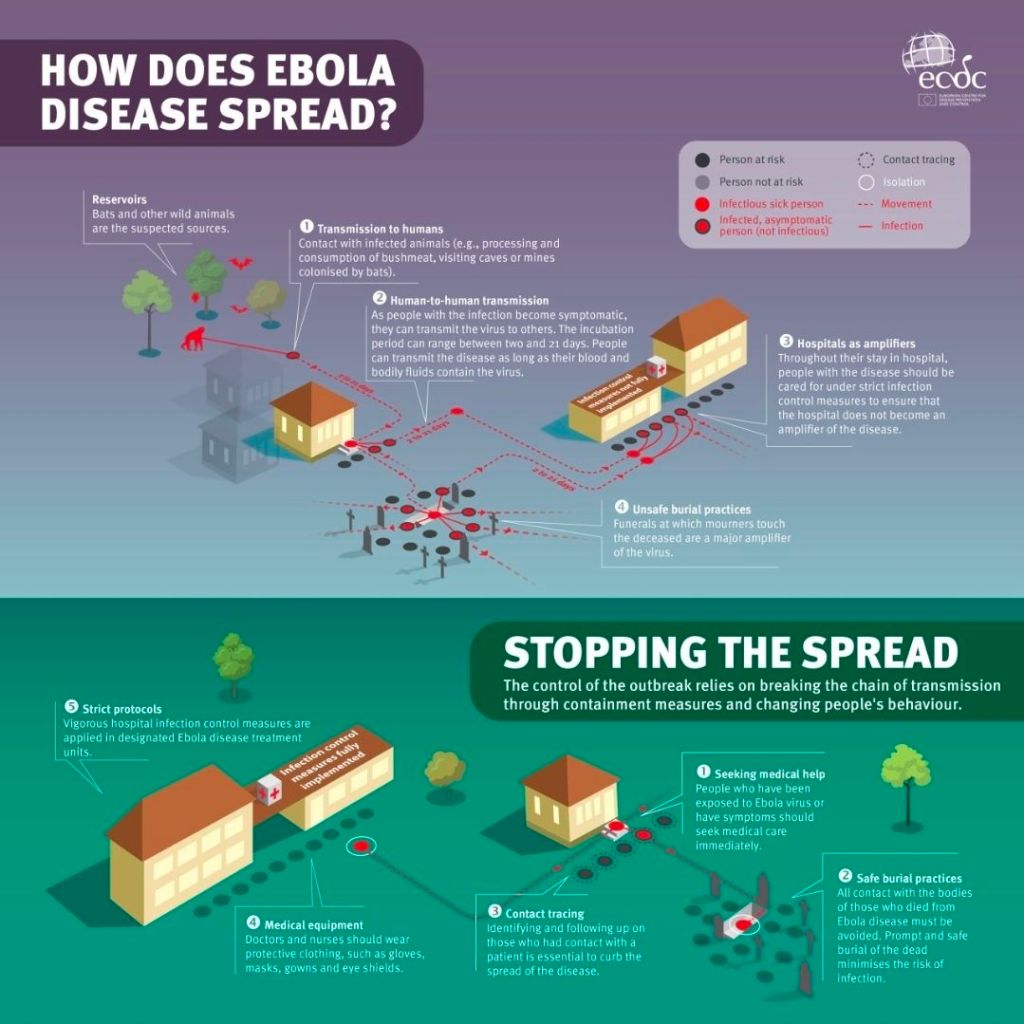
How does it spread?
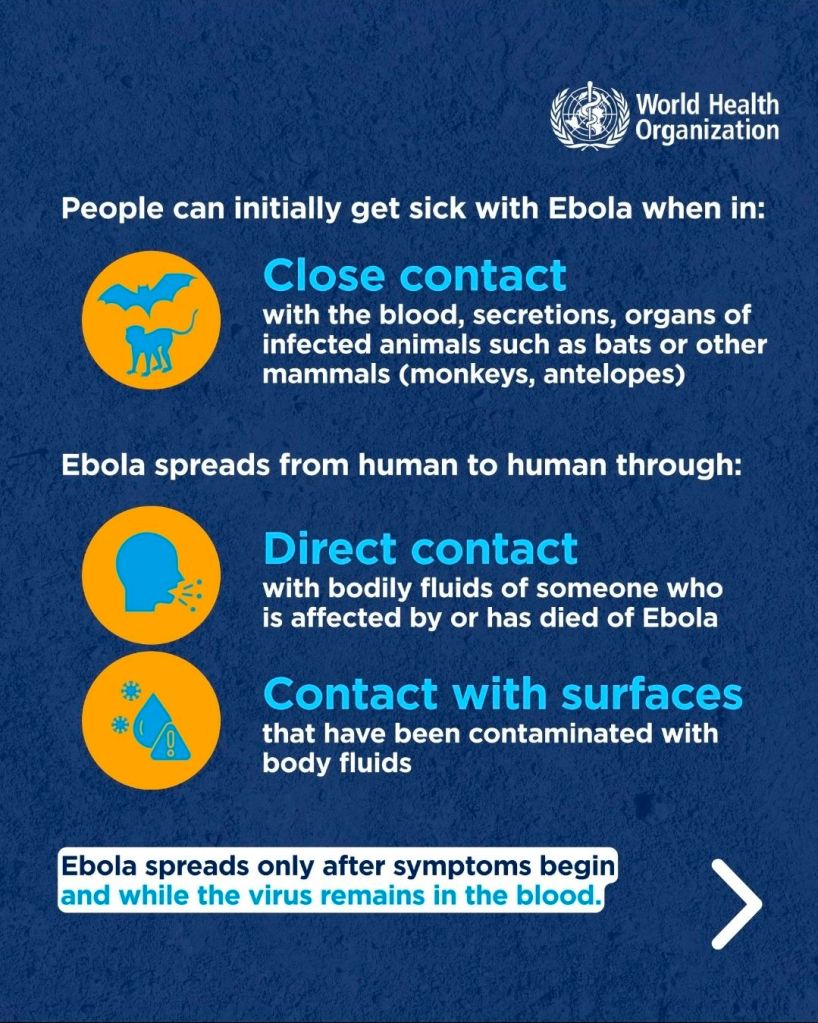
One challenge for outbreaks on this scale, and for Ebola viruses in particular, is the fact that cases occur throughout communities as well as in healthcare settings. Some of the people most needed to stop spread and to care for patients are the ones at the highest risk of acquisition. Those caring for the living, and the dead, as well as those who are going into homes and other environments to make them safe again for others. The level of selflessness required is huge, especially when you are having to step up knowing that the equipment and support you need to keep you safe may not be there.
During this outbreak there have been numerous reports of people putting themselves at risk to do their roles as items like personal protective equipment (PPE) are just not available. This happens because, although Ebola is spread by close contact with blood and bodily fluids, those infected produce significant amounts of excretions that are also likely to be heavily viral loaded. I talked in the patient management section that one of the biggest challenges is fluid loss via diarrhoea and vomiting and all of those fluids contain risk for those caring for them, or their environment.
Some of the additional challenges that occur during Ebola outbreaks are linked to how it impacts communities. Traditional burial practices often require kissing or interacting with the dead. In many Congolese communities, physical contact with the body is seen as a vital, respectful “final farewell”. This isn’t just a ‘nice to have’ it’s part of embedded in ritual and is highly significant as a way of saying goodbye to loved ones. There are also components that include family members washing the deceased. This is obviously a significant risk moment for transmission.
During significant outbreaks bodies may be disposed of using safe and dignified burial protocols, meaning funerals are undertaken using no touch protocols (the family cannot see or touch the body), bodies are sealed and specially transported, and bodies are buried in deep graves of at least 2 meters deep. Funerals themselves are events where people gather, which may be impacted public heath regulations, so at a time where people are most vulnerable they may expected to manage without support of friends and family, or the rituals traditionally used to help process loss. This can cause to distrust of authority and can lead to clashes between communities and those enforcing the protocols.
On final thing to consider for filovirus spread is that they have been detected in multiple body fluids, including breast milk and semen, in survivors of infection. The persistence in semen, with the potential for sexual transmission has been noted for more than 500 days after disease onset, amd is a serious concern for recovering individuals. However, onward transmission this long after disease onset is very rare with undetermined effects. Even so, this means that survivors and communities may need to consider transmission for protracted periods post recovery and it can represent a source of anxiety.
How is it managed differently?
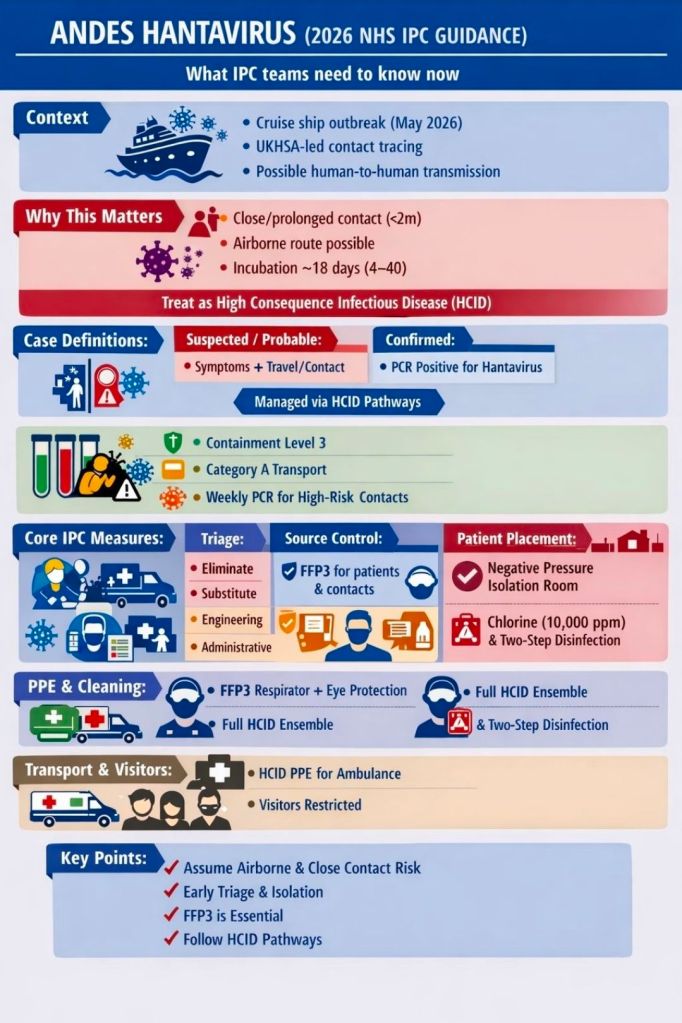
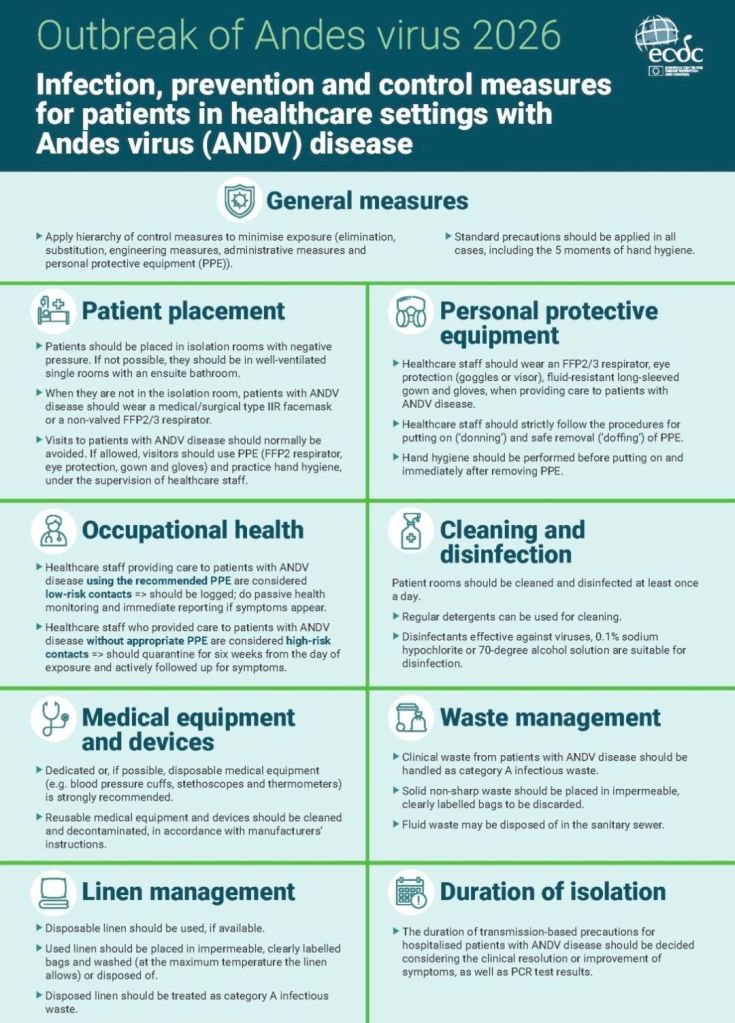
Ebola is classified as a Risk Group 4 (or Biosafety Level 4, BSL-4) pathogen, meaning that is requires the highest level of biological containment This impacts everything from the way patients are diagnosed and managed in clinical environments, to what kind of laboratory facilities are required to work in developing vaccines and other treatments.
Within the UK it is referred to as a high consequence infectious disease (HCID) which is defined based on the following criteria:
- Requires an enhanced individual, population and system response to ensure it is managed effectively, efficiently and safely
- Acute infectious disease
- Typically has a high case-fatality rate
- May not have effective prophylaxis or treatment
- Often difficult to recognise and detect rapidly
- Ability to spread in the community and within healthcare settings
Local guidelines for those managing these kinds of outbreaks evolved a lot as a results of the 2014 – 2016 Ebola Zaire outbreak, where the CDC modified guidance, in part due to the number of healthcare worker acquisitions early in the process.
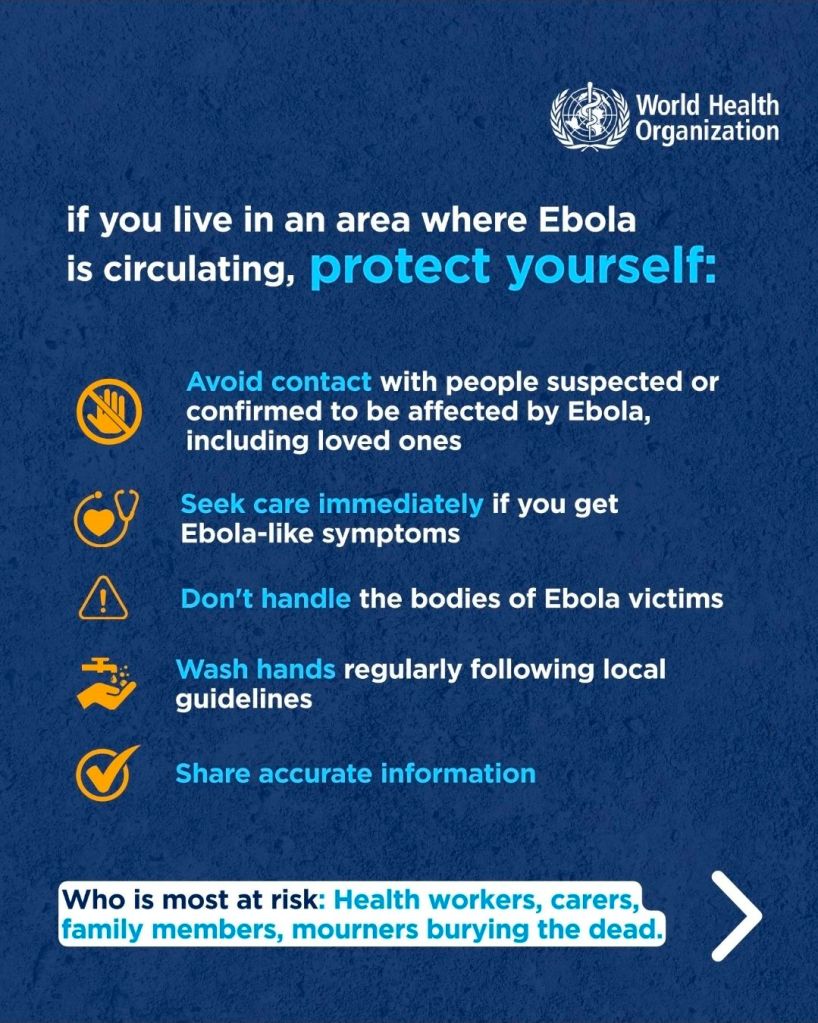
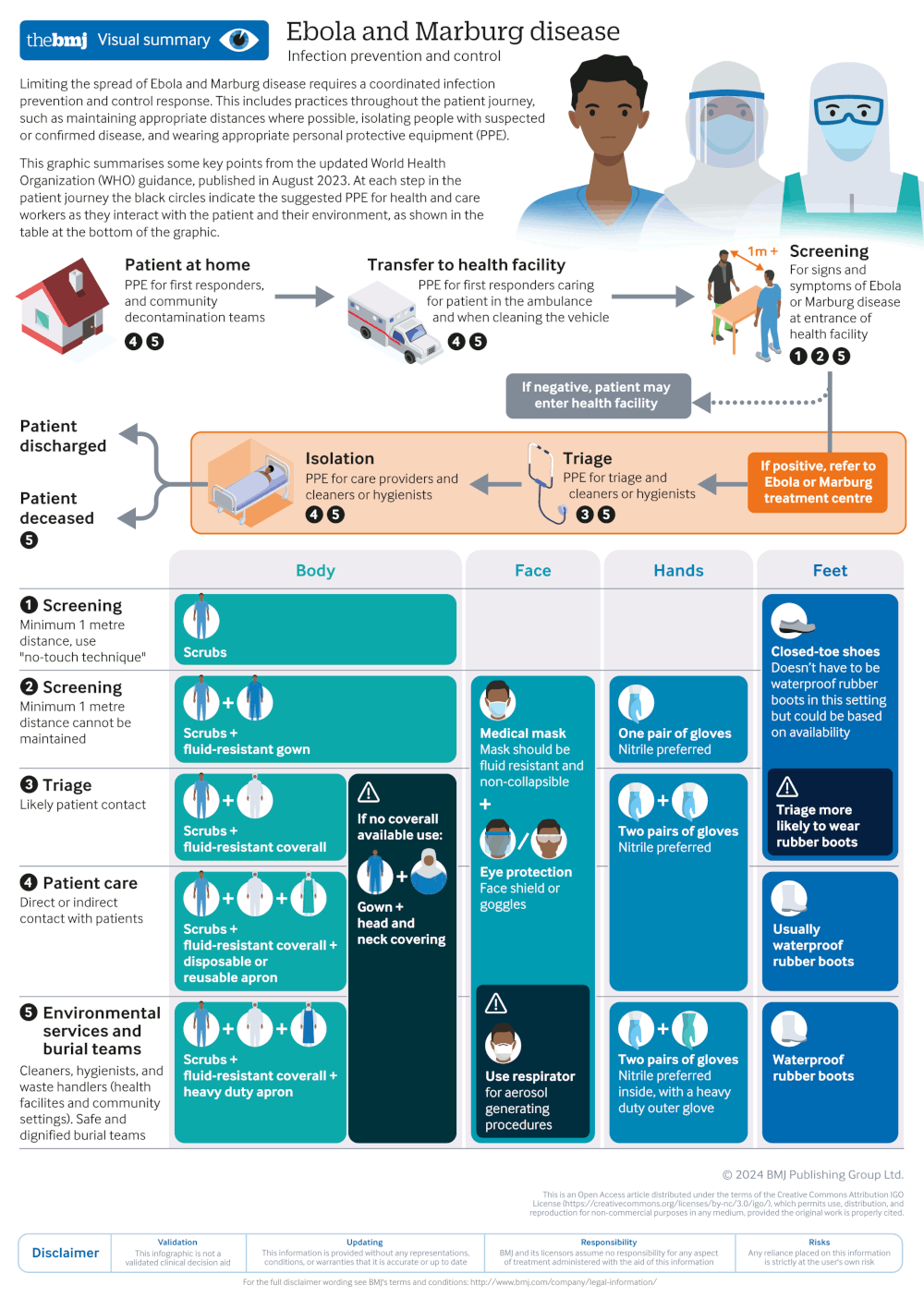
As it is not just those in hospitals that require PPE to protect staff, the WHO have also released guidance to aid decision making about what kind of PPE is needed for different workers and interactions across the patient pathway. This obviously has a caveat that if the PPE is not available you are not able to wear it.
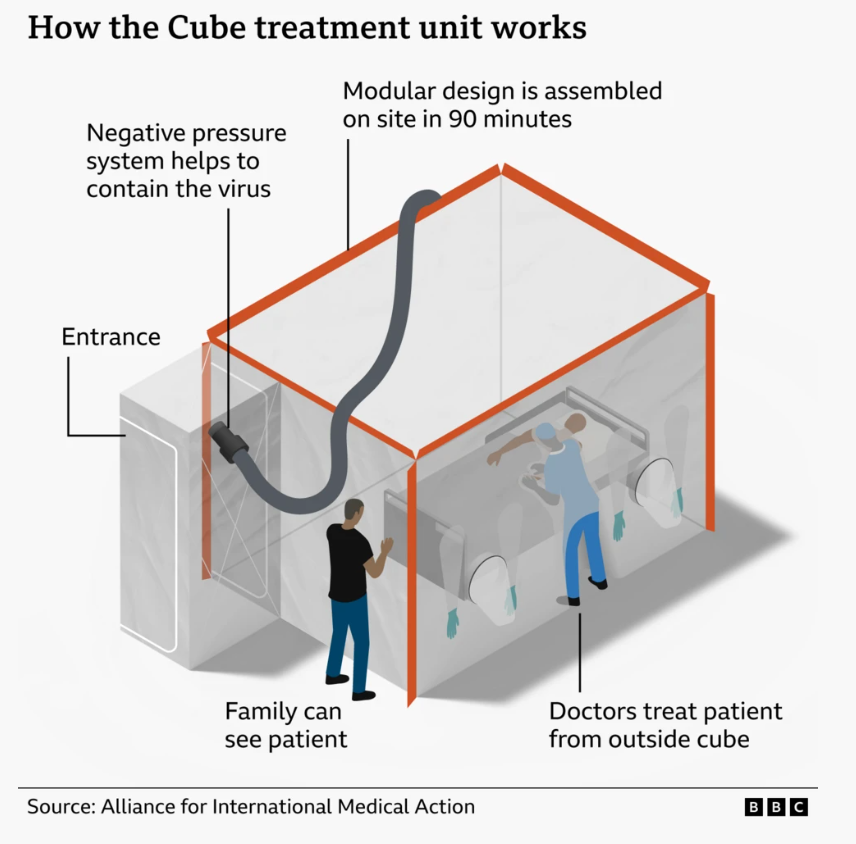
There are also some fantastic design solutions that can enable patients to be cared for in a way that limits the exposure of those undertaking that caring. These solutions also support patients having continued access for families, where they can be seen and communicate. This is also important as families may be expected to continue to provide food, even during hospitalisation, meaning they need to ve able to visit safely.
From the videos that I have seen, these facilities do not seem to be widely accessibly within the DRC, but the scenario might quickly change with the increasing recognition of the need for a global response to the outbreak.
Although it would be nice to imagine that everyone is being cared for in facilities, like those pictured above, many of the reports I have seen are much more similar to the New York Times video pictured below, which is really night and day to what we would wish for patients, staff, and families in terms of infrastructure access.
What does this mean for returning travelers?
The world cup has just started. People are travelling from all over the world to the USA, Canada, and Mexico. The report below shows some of the challenges that this kind of travel can lead to.
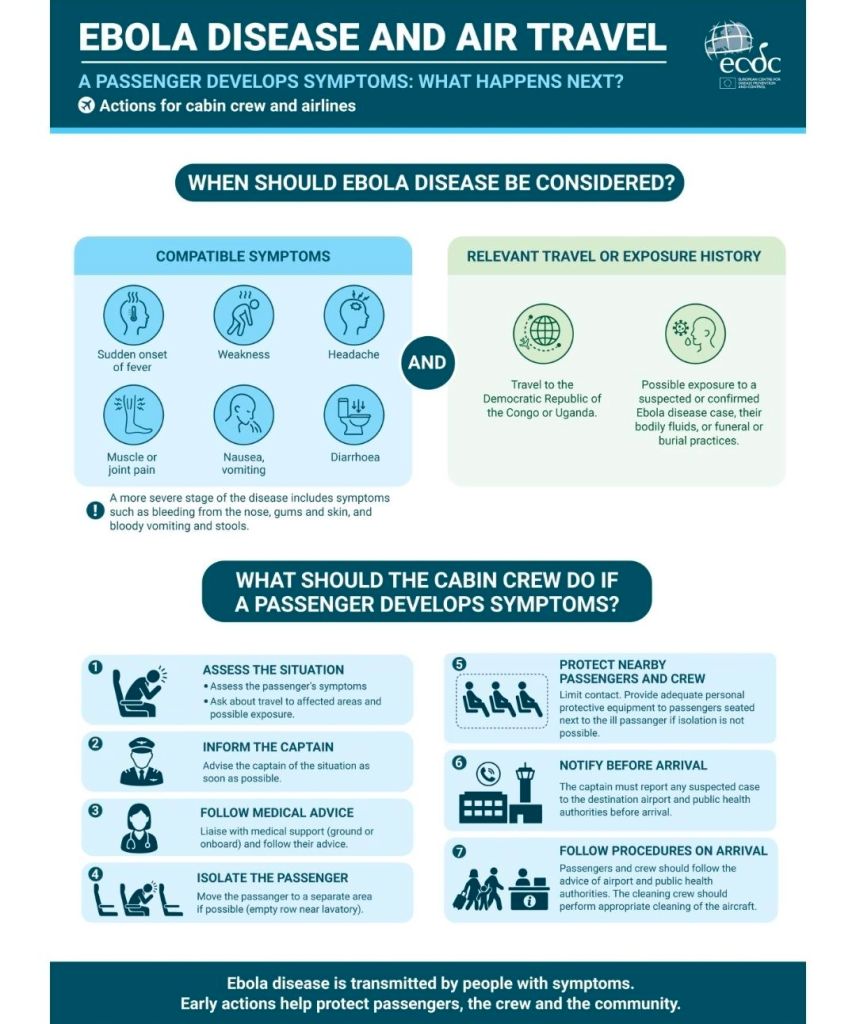
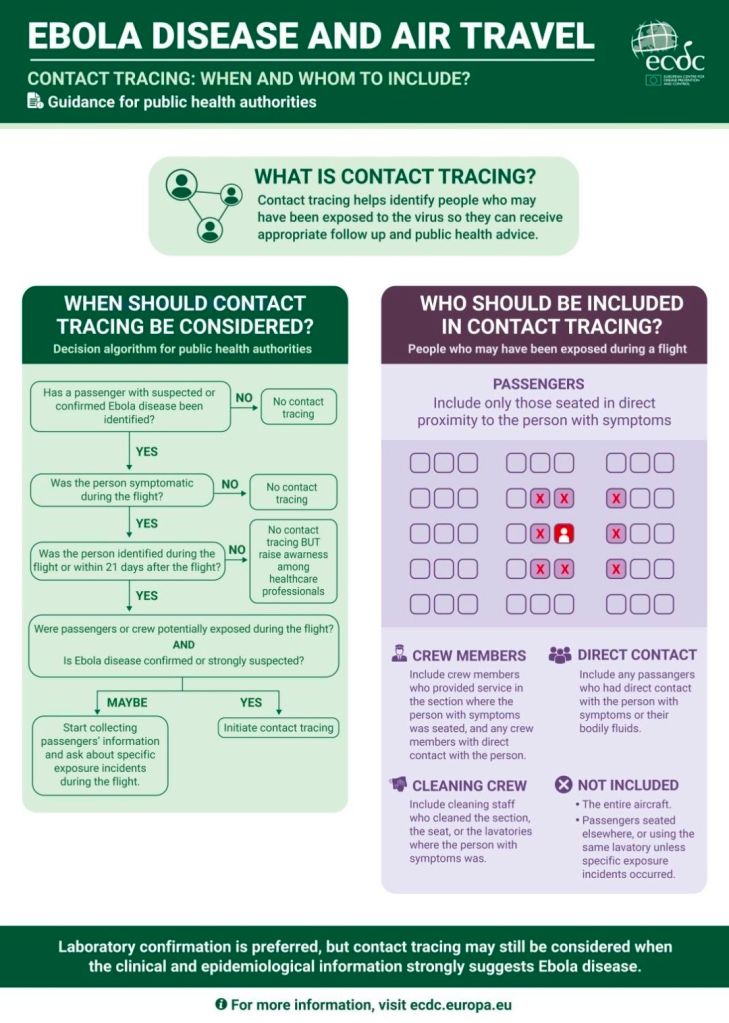
Events like these have led to places like the European Centres for Disease Control (ECDC) to issue guidance on what to think about if a passenger develops symptoms on a flight. This is so crucial because, as discussed, the initial symptoms are pretty non-specific, and if someone has a possible contact history it can be difficult to separate EBOD from a number of other infections that could initially present the same way.
They have also issues guidance about who might need to be followed up after an exposure event. Anxiety can drive extreme responses to having a probable/confirmed case, and so having guidance in these circumstances is key. As Ebola is transmitted by direct contact it is important to be able to differentiate those who are contacts from others who will have just been in the same space but are not at minimal to no risk (contact free exposure has a risk if <1%).
Terminology is key
As I’ve been talking about possible/probably/confirmed cases I thought it was important to include what those definitions actually mean within the UK health setting at least:
Confirmed case
An individual (alive or dead) with a positive laboratory test result (real time polymerase chain reaction (PCR)) from a blood or other body fluid sample.
Probable case
An individual for whom no laboratory results are available (for example waiting for testing or results), who meets both of the following criteria:
Clinical illness compatible with EBOD including any of the following symptoms:
- fever (temperature greater than 37.5°C)
- severe weakness
- severe headache
- myalgia
- abdominal pain
- sore throat
- vomiting
- diarrhoea
- unexplained haemorrhage
PLUS
Contact with an Ebola virus in one or more of the following ways in the 21 days before the onset of symptoms:
- contact with an identified potential source of EBOD (for example, direct contact with a probable or confirmed case without wearing adequate PPE or where there were breaches in PPE
- exposure to an Ebola virus-infected body fluids or tissues without wearing adequate PPE or where there were breaches in PPE
- direct handling of bats, antelopes or primates, from Ebola affected areas without wearing adequate PPE or where there were breaches in PPE
Possible case
A possible case is a deceased individual with epidemiological risks for EBOD
OR
An individual for whom no laboratory results are available (for example waiting for testing or results), but who meets both of the following criteria:
Clinical illness compatible with EBOD including any of the following symptoms:
- fever (temperature greater than 37.5°C)
- severe weakness
- severe headache
- myalgia
- abdominal pain
- sore throat
- vomiting
- diarrhoea
- unexplained haemorrhage
PLUS
One or more of the following epidemiological criteria in the 21 days before the onset of symptoms:
- history of travel to EBOD affected areas
- direct contact with a confirmed case of EBOD,
- or their body fluids (including laboratory staff), but trained and wore appropriate PPE, and had no known breaches in PPE
- direct contact with a confirmed case of EBOD, or their body fluids (including laboratory staff), but trained and wore appropriate PPE, and had no known breaches in PPE
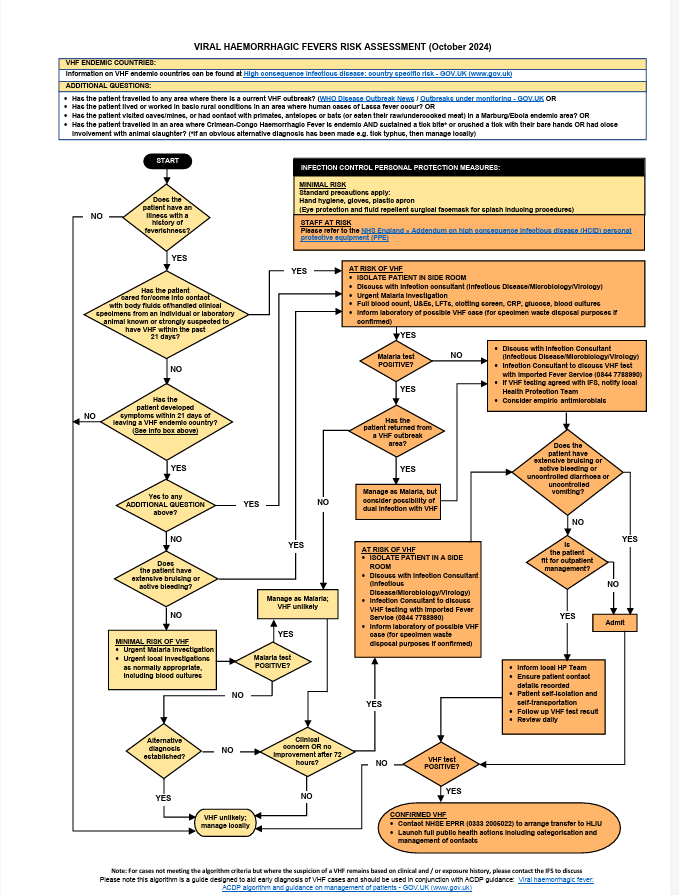
For someone arriving into the NHS, the application of these terms in linked to the flow chart below (https://www.gov.uk/government/collections/ebola-virus-disease-clinical-management-and-guidance) with the guidance last updated 4 September 2025. This also helps to remind people to go through steps such as ruling out other possible causes for the symptoms present, such as malaria.
Being able to use precise case definitions means that healthcare staff can ensure that the level of PPE and other protections are matched to the likelihood of risk being present.
Global health matters
As discussed at the start of this post, returning travelers or healthcare workers are already being monitored in numerous countries outside of the outbreak zones, and this is only likely to increase within the next 21 days, linked to the incubation period of the virus.
Until the infrastructure is present to support prevention of onward transmission the risk of global spread will continue to be present. Let me be honest here, I don’t think this is turning into a pandemic. I think there may be risk of acquisition to a small number of healthcare workers if for any reason communication linked to prior travel history fails. This isn’t the point though. We should not just mount public health responses because of a fear that they may impact us personally. I think we have an obligation to utilise the knowledge, experience, and resources available to help save, potentially, thousands of lives.
https://www.bbc.co.uk/news/articles/cy72z48zd7po
The time of it taking months of sea travel to get from point A to point B are far behind us. You can be anywhere in the globe in 24 hours, far shorter than the shortest incubation period for most infectious diseases. If the COVID-19 pandemic taught those of us working in the world of infection anything it was that global networks can make a real difference. A difference is the time it takes to recognise that there is a problem to be addressed. A difference in the number of people who are impacted. A difference in the time it takes to take a possible solution to an infectious problem, like vaccines, to a state where they are ready to be implemented.
We cannot live in a world where we think in terms of them and us. Where we think something isn’t happening in our back yard and therefore we don’t need to get involved. The truth is so far from this. Global health has the word global in it for a reason, and the eco systems we live in are global. We need to make networks and connections stronger, not let them be degraded.
So let’s put the pressure on where we can, use what influence we have, and try to ensure that the outcome of this outbreak is not determined by what resources are lacking and who makes the expertise available to help. Let’s behave as we hope someone else would in return, step up and be counted in order to save lives. Let’s be the global family that the pandemic showed us we could be if we tried.
All opinions in this blog are my own