Last week I wrote about the challenges of the current Ebola virus outbreak, talking about some details linked to the virus itself, and also some challenges that mean this outbreak may be more challenging to manage. I was involved in previous outbreaks, but definitely in a peripheral support capacity, because of my underlying autoimmune condition I did not travel to Sierra Leone. Context and learning from previous events is important however, so I tapped my good friend and colleague Ant De Souza, who was directly involved in supporting diagnostics, to write me a guest blog of his experiences.
Anthony De Souza is an award-winning Healthcare Science educator with over a decade of experience as Biomedical Scientist in microbiology. He was the first Healthcare Scientist to gain a permanent Practice Educator post, a post he has only continued to develop and expand since its inception. Ant’s transition into strategic education leadership has empowered the Healthcare Science workforce to improve patient outcomes based on his approach; which links strengthening multidisciplinary collaboration, expanding clinical capabilities, and elevating the profile of the healthcare science workforce to ensure they are invited to have a seat at the table. The impact of this has been recognised not just by me, but by him being named on The Pathologist’s Power List for his outstanding contributions to the field.
Ebola Deployment, Sierra Leone – A Personal Reflection
In 2015, when an urgent appeal was issued by Public Health England (now UKHSA) for scientists to support the Ebola crisis in West Africa, I didn’t hesitate—I knew I had to go.
In the past, I’d seen similar calls for volunteers and questioned whether my skills were enough to make a meaningful contribution. The last thing I would ever want was to become a burden on a mission of such importance. But this time felt different. For the first time, my experience, confidence, and mindset aligned with what was needed. I was working as a Band 6 Biomedical Scientist at Watford General Hospital, in a busy microbiology department delivering a 24/7 service. I was used to working under pressure, and I felt ready to contribute.
Before committing, I spoke with my colleagues. A five-week deployment would mean they would take on additional workload, and it was important to me that I had their full support. With their encouragement, I signed up.
Preparation and training
Preparation for deployment was thorough and, at times, intense. I travelled to Porton Down in Salisbury for specialist training, where we learned how to work safely with high-risk pathogens such as Ebola. This included simulation exercises in a laboratory environment designed to mirror the Kerrytown facility, where we practised managing realistic scenarios, including equipment failures and power outages.
We also completed security awareness and hostage survival training, alongside a series of vaccinations for diseases such as yellow fever, cholera, and typhoid. Anti-malarial medication was essential. The preparation highlighted not only the scientific challenges ahead, but also the environmental and personal risks we would face.
The journey
Getting to Sierra Leone was a journey in itself. We travelled by plane, transferred in Morocco, then boarded another flight to Freetown. From there, the journey continued by minibus to a port, a boat crossing, and finally another minibus to the site.
It was a strange experience travelling with a group of people I had never met—yet over the course of five weeks, these individuals would become a close-knit team.
Arrival and first impressions
On arrival, small behavioural changes immediately became part of daily life. Handshakes were replaced with elbow taps, a simple but important measure to reduce transmission risk. Regular temperature checks became routine, particularly at checkpoints when travelling to and from the treatment centre.
We were based at the Ebola Treatment Centre (ETC) in Kerrytown, outside of Freetown—a facility built by the British Army Royal Engineers and funded by the Department for International Development. The scale of the operation was impressive, and there was a strong sense of shared purpose. People from different organisations and backgrounds worked together with a single goal.
The ETC was divided into zones based on risk, from green (low-risk areas) to red (high-risk patient areas). Full personal protective equipment (PPE) was mandatory in higher-risk areas.
Working in the laboratory
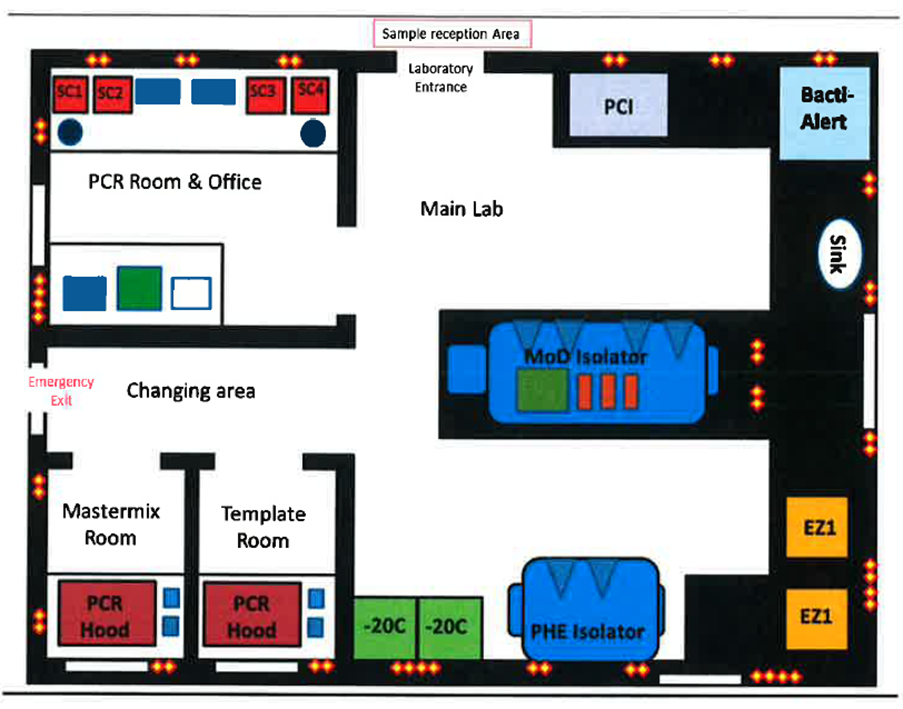
Our laboratory was located centrally within the site, shared with the Ministry of Defence. After donning PPE, we met the outgoing team and received a rapid but essential handover. For a few days, we worked alongside them before taking full responsibility.
Our role was to test blood and swab samples from individuals suspected of having Ebola. We operated six days a week, with two teams of six covering shifts from 06:00 to 22:00.
Many samples came from community settings, including remote villages. A significant proportion were post-mortem samples, taken to determine whether Ebola had caused the death. The high number of samples from children and infants was particularly difficult to process emotionally.
Specimen reception took place outside the lab. Samples were placed into chlorine solution for decontamination before being handled further. Wearing full PPE in the heat of the sun was physically exhausting, and the need for constant vigilance—checking for incorrectly packaged samples or hidden sharps—added to the pressure.
Inside the lab, resources were basic but functional. The space had sealed cement benches, limited air conditioning, and no negative pressure system. Testing was carried out using PCR techniques for Ebola, alongside POCT testing for malaria. A flexible film isolator was used to safely inactivate the virus before analysis.
Life beyond the lab
Outside of the laboratory, the scale of the public health response was visible everywhere. Posters, radio messages, and community outreach efforts aimed to educate people about Ebola transmission, safe burial practices, and how to protect themselves.
Strict measures were in place:
Large gatherings were prohibited
Schools and religious services were disrupted
Curfews were enforced
Checkpoints monitored movement and health status
Movement restrictions between districts
Daily life, as it once was, had largely come to a standstill.
Cultural challenges and adaptation
One of the most striking aspects of the outbreak was its impact on traditional burial practices.
In Sierra Leone, burial rituals are deeply rooted in cultural and religious beliefs. Traditionally, families wash, dress, and physically say goodbye to loved ones. However, in the context of Ebola, these practices posed a significant risk, as the virus remains highly infectious after death.
To reduce transmission, specially trained burial teams were introduced. These teams worked closely with communities and religious leaders to adapt traditions safely. While physical contact was removed, efforts were made to preserve dignity—allowing families to view the body from a distance, limiting attendees, and involving community leaders in the process.
This collaboration was essential. Without it, there was a real risk that families would carry out burials in secret, increasing the spread of the virus.
Reflections
There is much I could say about my time in Sierra Leone—far more than can fit into a single blog. The work was challenging, both physically and emotionally. There were moments of exhaustion, uncertainty, and sadness.
But above all, what stays with me is the resilience of the people.
In the face of immense hardship, communities adapted their traditions, supported one another, and worked alongside international teams to combat the outbreak. It was a powerful reminder that effective public health is not just about science or medicine—it is about trust, collaboration, and cultural understanding.
This experience reshaped my perspective on global health, teamwork, and the role we each play in times of crisis. It remains one of the most challenging and meaningful periods of my career.
Cruise ships and cruise ship outbreaks have been in the news a lot this month. So much so, that I’ve already posted about the Hantavirus outbreak that was associated with a cruise ship in South America:
There have also been headlines, however, linked to 48 passengers displaying symptoms consistent with gastrointestinal illness, as well as one crew member, that has led to another cruise ship asking passengers to isolate.
This second kind of cruise ship outbreak isn’t all that unusual, and I wonder if it would even have reached the headlines if it hadn’t happened during the same month as everyone was talking about Hantavirus. Cruise ships are mobile cities, with large numbers of people confined within a limit space, usually drawn from all over the world. Places where everyone is outside of their ‘normal’, eating different food together, spending time in close quarters with strangers, and sometimes reticent to lose holiday time if they start to feel unwell. That’s without throwing in sea sickness as an alternate reason for nausea and vomiting, which may mean people don’t realise they are ill with something infectious as early as they may do at home.
I’ve always sworn, for all of these reasons that I would never go on a cruise. I’ve spent way too many hours in lectures listening to outbreak stories related to ships, and yet, due to a birthday surprise, I went on my first ever cruise in 2025 and it surprised me, so I thought I would spend this week talking about a few of the reasons why, but first some outbreak context.
Multi-Year Outbreak Comparison (2019–2026)
According to historical Centres for Disease Control (CDC) data tracking of official gastrointestinal outbreaks across major cruise lines, the frequency of notable incidents varies dramatically by cruise line brand:
Princess Cruises: Highest frequency with 14 outbreaks
Holland America Line: 13 outbreaks
Royal Caribbean International: 10 outbreaks
Celebrity Cruises: 6 outbreaks
Carnival Cruise Line: 2 outbreaks
Disney Cruise Line: 1 outbreak
It’s worth noting, however, that different cruise lines not only have very different numbers and types of ships, with wildly different passengers numbers, but they also have very different passenger profiles. Some, like Virgin, host adult only cruises. Others, like Viking, serve older passenger demographics and undertake river cruising rather than ocean based cruising. Then you have lines like Disney, that focus on family centered cruising, and so will have a high proportion of families and young children as part of their passengers. Some cruises are also much longer than others, with cruises over six months becoming more common, and some cruise ships now consisting of passengers who have permanently brought cabins as their primary homes. All of which is to say, that numbers alone may not tell the whole story, and it is probably important to compare like with like.
NB Interestingly, as the recent Hantavirus outbreak did not impact 3% of passengers, I don’t know believe it would be reported via this system, and I suspect that they only manage US related outbreak numbers.
Outbreak Organisms (CDC list 2023 – 2026)
When you are training in microbiology, virology and infection prevention and control, you study A LOT of outbreak scenarios. Some of theses are almost always linked to outbreaks on cruise ships and/or navel carriers. Studies of re-supply and bringing in vegetables used for salads that took down 2/3 of the ship cohort with multiple organisms. I thought it might, thereofore, be interesting to look at the CDC data related to some recent outbreaks and see what the causative organisms actually are.
From 2023 – 2026 (to date) there were 54 reported outbreaks on the CDC website reaching the 3% of total passengers threshold. The causative organisms, where known, included:
Norovirus
Salmonella
E. coli
Combined Salmonella and E. coli
Now, I’ve previously posted about Norovirus, and how difficult it can be to control, especially the challenges of getting it out of environmental reservoirs (carpets, curtains, bedding) and so I’m not surprised that it is on the list.
I was interested to see how dominant norovirus was compared to other causes. When you look at the numbers it shows that norovirus really does seem to be as dominant as I was taught, with nearly 90% of outbreaks due to noro:
Norovirus: 48 outbreaks
E. coli: 4 outbreaks
Salmonella: 1 outbreak
Combined Salmonella and E. coli: 1 outbreak
Whilst noting that this feels like a lot of cases, it is also worth considering that the CDC states that cruise ship outbreaks account for just 1% of all reported norovirus cases globally. The other interesting thing is that the numbers seem to be pretty stable year on year, whereas out in the community I would expect there to be a significant rise in norovirus cases every 2 – 3 years, as strains change due to mutation, this doesn’t seem to be the case within the cruise data available.
Disney cruise line specific outbreaks
Having noted that Disney had only 1 outbreak listed recently on the CDC site, I thought I would investigate a little further. Disney Cruise Line has had two major officially documented gastrointestinal illness outbreaks that reached the CDC mandatory reporting threshold of 3% or more of passengers or crew, one in 2016 and one in 2002, each on a different ship:
Disney Wonder:
April–May 2016 (Official CDC Outbreak): During a 4-night Bahamian itinerary heading into a Panama Canal cruise, 131 of 2,680 passengers (4.89%) and 14 of 991 crew members (1.41%) fell ill with laboratory-confirmed norovirus.
Disney Magic:
November 2002 (Official CDC Outbreak): A total of 175 passengers and crew members out of 2713 passengers and ~950 crew, contracted norovirus during a Bahamian voyage. Disney temporarily pulled the ship from service for a week to break the infection cycle through a deep chemical sanitation.
Not all ships are equal
Something that struck me, is the outbreaks listed for Disney are to do with the two older ships in the Disney Cruise Line fleet, as they are both part of the Classic Class. This is interesting for 2 reasons:
Is there an accumulation of outbreak risk due to age? Especially for organisms like norovirus which can be linked to environmental reservoirs
The oldest 2 Disney Cruise Line ships were not a custom Disney build and so lack some of the specific design features that may support risk reduction on the newer ships
To aid with understanding this, it is noteworthy Disney has built a number of custom ships since the production of the Classic Class, and therefore have had the opportunity to include many more custom features in the later classes of ships.
The Classic Class – purchased by Disney but not a custom Disney design
Disney Magic (1998) ~2700 passengers
Disney Wonder (1999) ~ 2700 passengers
The Dream Class – commissioned by Disney for Disney
Disney Dream (2011) ~4000 passengers
Disney Fantasy (2012) ~4000 passengers
The Wish Class – commissioned by Disney for Disney
Disney Wish (2022) ~4000 passengers
Disney Treasure (2024) ~4000 passengers
Disney Destiny (2025) ~4000 passengers
The Global Class – purchased by Disney but part built before acquisition
Disney Adventure (2026) ~6700 passengers
One thing I didn’t realise, until I started to investigate this area more, is that cruise ships need to go into dry dock at least twice in every 5 year period by maritime law. Obviously mostly this is to do with safety, linked to the hull etc, but most cruise lines will use this opportunity to re-fit and manage any fittings and soft furnishings, which can aid with managing ongoing outbreak risk.
Why does Disney Cruise Line have to do things differently?
Full disclaimer here, I haven’t been on cruise lines with anyone else, but I have done a lot of talking to people and watching videos to enable some comparison, but my only first hand knowledge is from what I have experienced. I have only been on the Fantasy, and there are other classes of ships, obviously if Disney Cruise Line would like me to travel on them all to do an infection control audit, I’d be happy to, they wouldn’t even have to pay me.
I think, from my experience, one of the reasons that Disney Cruise Line is different, and has to be different, is because of the passenger demographic they serve. Their passenger number contain a huge amount of children under the age of ten. Children who may be shedding high viral loads, and carrying asymptomatic infection. Children who may also be too small to be able to communicate how they are feeling when symptoms come into play, and who may also not be compliant with hand and other hygiene practices, and are likely to be in close contact with others when playing etc. The ships are therefore at higher risk, potentially, than other cruise lines of having significant spread once a virus is onboard. It is also much harder to be able to isolate small children, and they are much more likely to need clinical support if they become unwell, which is a risk to the child and logistically complicated to manage. It is therefore much better to invest in steps to prevent infection spread.
What does Disney Cruise Line say they do to prevent the transmission of infectious disease?
Disney consistently ranks in the top five cleanest cruise lines globally. Their fleet frequently achieves perfect 100 scores during unannounced CDC sanitation inspections. They also have an advantage as they are an independent fleet, they don’t rent their ships out to others for events or specialist cruises, where they would have periods of time where they couldn’t control their risk. This allows them to maintain control of their fleet, what activities are undertaken, and ongoing control methods. The ships are also on the smaller size in terms of passenger numbers compared to some of the very large cruise ships managed by other companies (~2,700 to ~6,700 guests compared to ~5500 to ~7600 on some other lines).
Below is what Disney Cruise Line states about how they control their infection risks:
Key Quarantine and Isolation Protocols
Mandatory Isolation: If you test positive for COVID-19 or another contagious illness during your cruise, you and your stateroom occupants will likely be required to isolate in your stateroom or a specially designated, safer area of the ship.
Medical Evaluation: Shipboard medical centers are staffed with experienced doctors and nurses to provide care, and you may be required to quarantine at the sole discretion of the shipboard physician.
Disembarkation/Evacuation: If necessary, you may be required to disembark early for medical reasons, which could occur in a foreign port.
Pre-Boarding Screening: While pre-boarding testing is not always required, all guests must complete a mandatory health questionnaire before boarding, which includes screening for symptoms like fever, cough, vomiting, or diarrhea.
Compliance: You are required to abide by all health safety protocols, which can change without notice, and failure to comply may result in denied boarding or forced disembarkation.
Stateroom Support: If you are required to isolate, Disney provides necessary support, including food delivery and medical check-ins.
Illness Prevention: The crew conducts extensive cleaning and sanitization of common areas and staterooms
Now, luckily for me, I didn’t experience any sickness onboard and so I can’t testify to the accuracy from all of these portrayals. I can, however, attest to many of other aspects, such as pre-screening, cleaning, and hand hygiene support.
Operational approaches
There were some brilliant operational choices that made me both happy and also surprised me. There were also some really simple design decisions, which now I’ve seen I don’t understand why they aren’t present everywhere. The best example of this was the way that plates on the buffet were stored upside down. This means that no one is in contact when taking a plate with the surface that someone else will then eat off. This is such a simple change but makes so much sense in terms of infection control I can’t believe I have neither thought about it myself or seen it elsewhere.
Other simple things included the fact that all cutlery was left fully wrapped, and so no one was touching the implements that anyone else was going to eat with. This fully enclosing, rather than just wrapping, is another easy way of prevention cross transmission routes, as asymptomatic, or even symptomatic excreters, are not in a position to pass on their organism to others. It also prevents deposition on cutlery from other routes, such as when people sneeze, effectively providing a protective barrier.
Self serve vs cast member led
Another key thing, on some ships, is that the buffet is served by cast members rather than self serve. This means that the food is kept behind screens and significantly lowers contamination risk. All main meals are served plated by cast members, which also reduces reduces the risk. Even self serve items, have guidance linked to risk reduction. For instance the fizzy drink dispensers advice people not to use reusable cups, so that the dispenser outlet does not risk re-contamination after someone has drunk from the cup.
Keeping hand hygiene easy
Something else, that is very prominent, is the emphasis placed on hand hygiene wherever you go onboard. Hand hygiene stations are conspicuously present with both adult and child height basins. Special sinks are also present in all the child specific areas that can help children with hand hygiene, as all they have to do is submerge their hands and the sink itself undertakes the agitation. This helps hygiene efficacy for children who younger or less engaged.
Multiple hand hygiene stations are available at the entrances to the buffet, and there are enough of them that no one should skip unintentionally because they haven’t seen them, or because people are off-put because of queues. Making hand hygiene easy and visible has been found to be key from healthcare studies, and I imagine cruise ships are no different.
Gatekeeping
At main dining room meals, in the evening, hand hygiene is actively enforced. As there are too many people entering the dining rooms at each sitting (as everyone eats at either early or late dining) Disney enforce hand hygiene by having crew members physically hand out hand sanitising wipes directly to each passenger as they enter the dining room. The same happens at the buffet at busy times. This is very different (from what I can tell) to other cruise lines and definitely contributes to risk reduction. Having these multiple points, every day, where hand hygiene is enforced really helps to impact the collective risk level onboard.
Bathrooms
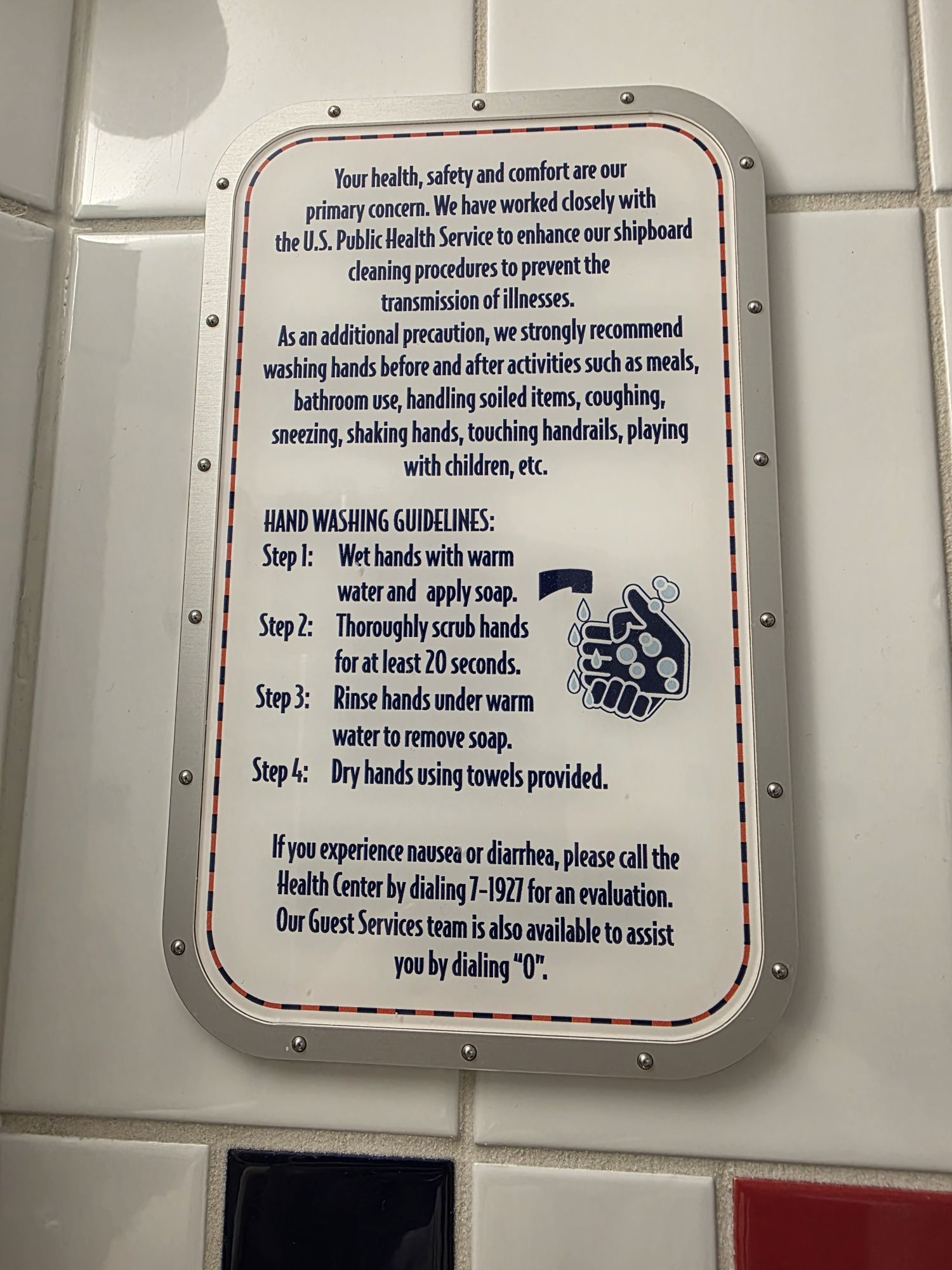
Even the bathrooms pleased me, and not just because of the Mickey shaped mirrors. Having a feature that attracts people towards the sink does help with hand hygiene compliance, however. They also have signage on how to wash your hands by every sink, to encourage that it is done appropriately. Additionally, many have access to hand hygiene in areas after you have exited the bathroom door, to manage any exit contamination risk, as an additional option.
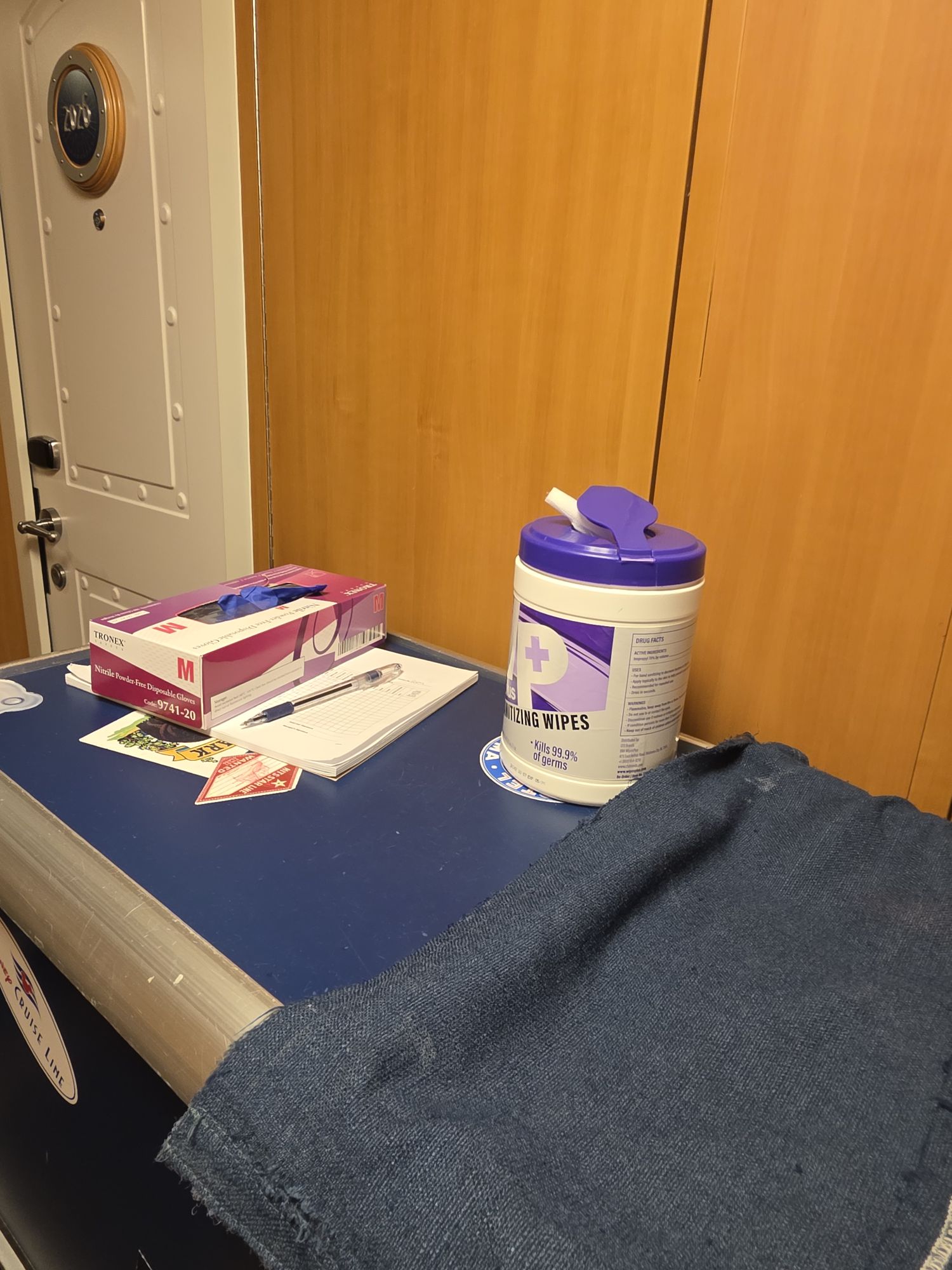
Domestic cleaning
Cleaning is obvious everywhere you go. I may have been the only person on that cruise who spent time photographing the cleaners trolley rather than the ‘big five’. All rooms got cleaned at least once a day, but in my experience many rooms got cleaned twice a day, as they get a morning clean and an evening turn down. Eating areas are also rotated and open at different times which allowed cleaning to be supported. Spending so much time auditing, I am often super aware of environmental grime, and no once was I brought out of the magic of being onboard by seeing anything that triggers my IPC brain.
Cleaning trolleys have freshly made up cleaning solution, alongside cleaning wipes. Fresh cloths and easy access to gloves. The level of cleaning we experienced was immaculate, and this does seem to align with the CDC audit scores.
Pre boarding
There are steps taken to reduce risk, however, before you even get on board. Disney Cruise Line requires all guests to complete a mandatory, online health questionnaire on the morning of embarkation, typically arriving via email between 5:00 a.m. and 6:00 a.m. The is pretty brief and asks a series of “Yes/No” questions regarding recent fever/respiratory symptoms, gastrointestinal issues, and pregnancy status (specifically for those 24 weeks or more). Although not infection related the pregnancy question is an interesting one and often catches people out. Disney, like many cruise lines, won’t let women sail if they are over 24 weeks pregnant. This appears to be standard across the industry because , if a medical emergency or preterm labour occurs, ships do not carry the specialized equipment or staff required to safely manage delivery or provide neonatal care for a premature infant.
If you reply in the positive to any question, other than the pregnancy question which is an immediate no board, then you will usually be reviewed prior to boarding and a risk assessment performed.
During cruising
If you develop symptoms of any kind, once you are onboard, there is support available from the medical team. It may be hard to distinguish between gastrointestinal symptoms and sea sickness, and everyone is encouraged to flag anything in order to ensure the right risk review is undertaken. If it is felt to be an infectious cause, passengers will be asked to isolate, and enhanced cleaning is undertaken.
Not only is hand hygiene reinforced during signage, by telling you not only how but when to wash your hands, it also clearly flags that you should contact medical support staff if you experience symptoms, and helpfully even flags what they are. All of this means that they are multiple contact points every day where passengers can access information that may be helpful in reducing infection risk (also, how clean are those tiles).
During excursions
Hand hygiene is also enforced after excursions before you get back onboard the ship. Alcohol gel dispensers are brought out by the crew, and cool towels, as well as water, are available to aid passengers stay cool and hydrated. I’m sure if you were in colder climes these would be aimed at warming you up.
Signage is also placed outside of disembarkation points that can help guide whether special measures may be needed or advised before you start on excursions. I think most people are more concerned with COVID still than norovirus, whereas I am very much concerned about diarrhoea and vomiting as part of my ship board experience.
Visible prioritisation
In general the communication of the need for hand hygiene is ubiquitous onboard. The signage below was part of the display in the lifts on the Fantasy. Embedding this guidance, and having it reinforced by cast members, means that for the most part everyone just complies without the need for prompting. I suppose it should be no shock that Disney do communication well, so much so I think there are some things we could learn in hospitals about how it is approached.
Design led solutions
The other area that healthcare could learn from is some of the design based solutions. We obviously have a lot of hands free options in healthcare but it was great to see these design points across the ship to minimise areas where hand contact is concentrated by needing to touch single points. A lot of thought has been given to pinch points in the system, and actions like manually supporting hand hygiene using wipes really also helps to address these.
Things I still can’t get over
Having talked about everything I loved, there is one thing that I don’t think I’ll ever get over, the people soup that are shared spa pools. The idea of sharing warm bubbling water with strangers and imagining our shared bacteria growing is something I can’t get passed. Also, I need to see the Pseudomonas testing certificates. This isn’t a Disney specific aversion, I just don’t think I can get my head around them anywhere. Nothing is perfect.
Where can I learn more?
I was taking on my cruise as a surprise, but Mummy and Mr Girlymicro has done a LOT of research before we want, so much so they even had to delete their YouTube histories so I wouldn’t notice. All lines have different risks, so I would advise doing some research to see which ones have risks that you are prepared to engage with. For me, I’m a Disney girl and I’m yet to see information from any other cruise line to temp me into doing something different. What can I say, I’m a convert to cruising, but only under a very specific set of parameters, and if Disney ever need infection control support, all they have to do is call me.
If you want to learn more, or check out your own cruise line of choice, the CDC website that contains a lot of info:
Content warning – this one is long, and is heavier on the detail than usual. It kind of needed to be as people have died. However, if you want the Cliff Notes version, no, there is no need to panic as Hantavirus is not going to be the cause of the next pandemic.
Everyone seems to be talking about Hantavirus right now, well they were, now people are also talking about Ebola and meningitis. It does rather feel like the infectious disease of the week right now. Despite a lot of effort by scientists and healthcare professionals there seems to be an appetite for panic linked to this. It is worth knowing that although Hantavirus is considered to be a high consequence infectious disease (HCID), that is mainly because it is linked to a potentially severe outcome for an individual if infection is confirmed, rather than potential for wide scale spread.
As I’m being asked about this by everyone from cab drivers to healthcare professionals, and faced with panicked social media commentary about whether this is going to be another pandemic, I thought I should share some of the information that is out there in order to support the ‘don’t panic’ key messaging. I think it is important to note, however, that I am not a Hantavirus expert, just your standard infection prevention and control professional, but having studied zoology in a previous life I couldn’t miss the opportunity to talk about a zoonotic (linked to spread from animals) infection.
What is the current scenario?
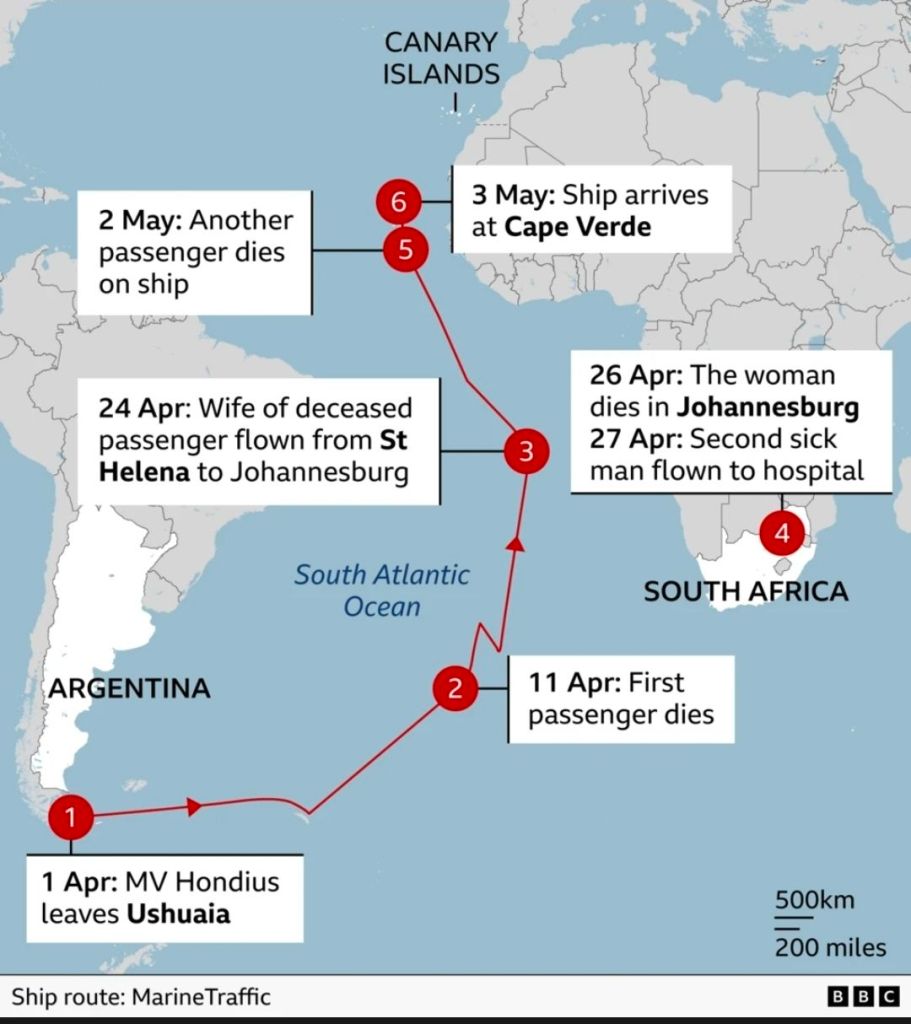
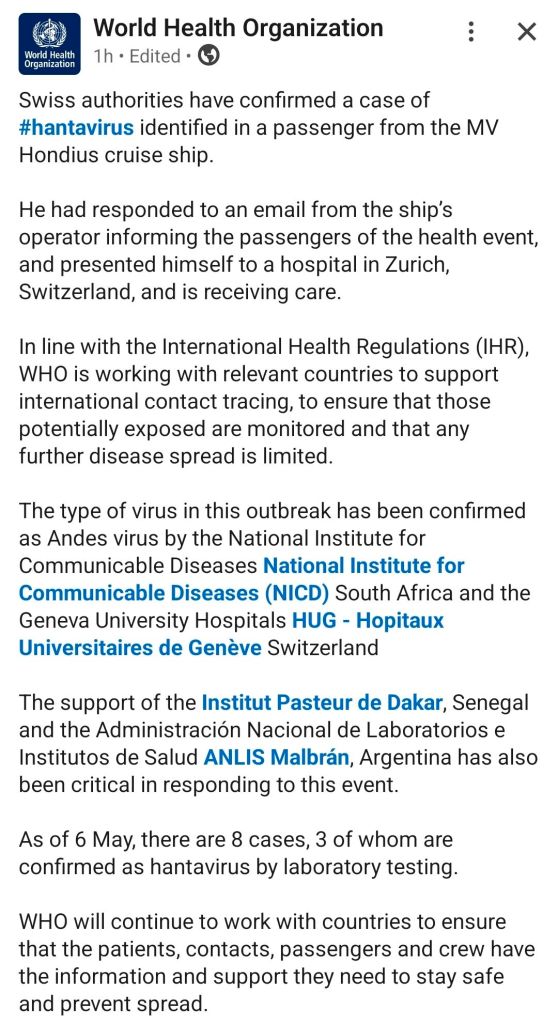
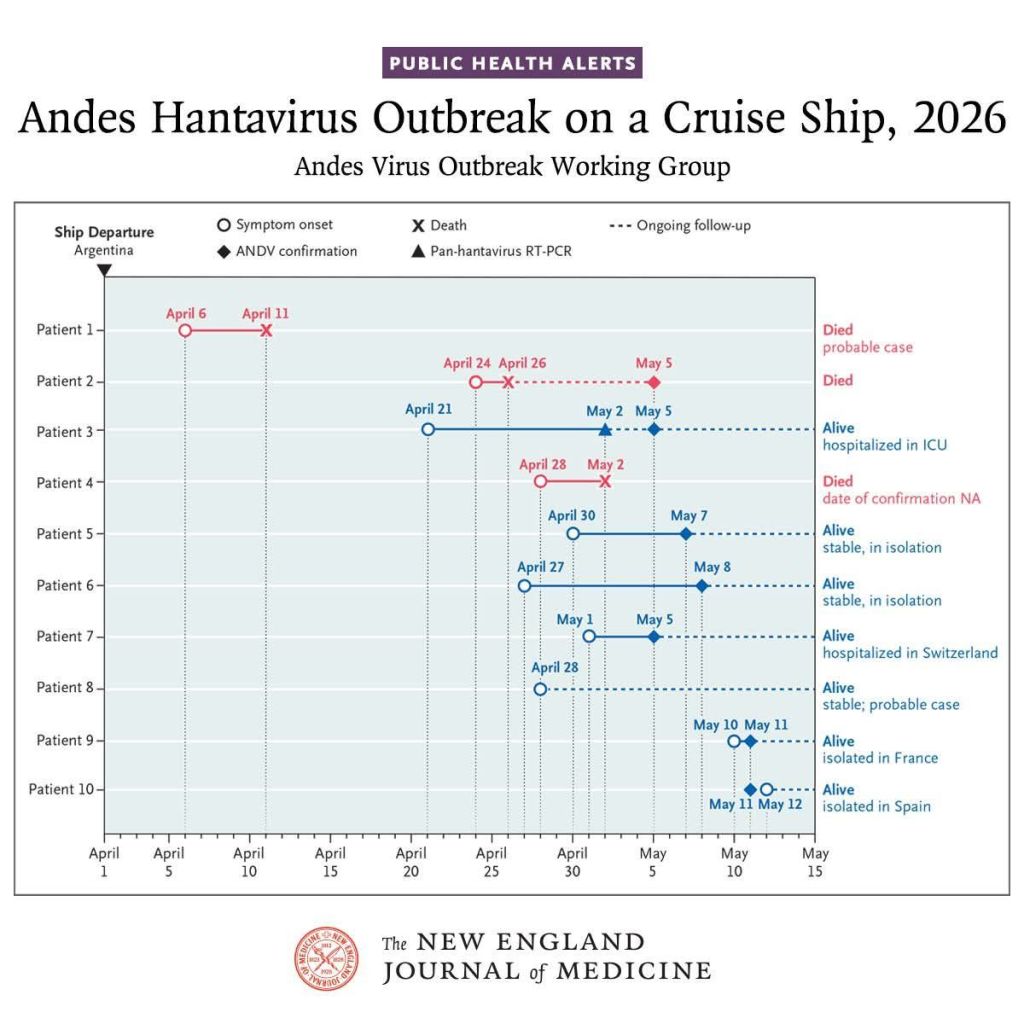
The cruise ship (MV Hondius) that is making headlines departed from Ushuaia, Argentina, on April 1, 2026, and traveled across the South Atlantic Ocean, stopping at several remote locations that including excursions and the opportunity for passengers to get off the ship, standard cruise fare but with more unusual destinations. These included Antarctica, South Georgia Island, Tristan da Cunha, Saint Helena, and Ascension Island.
The ship itself carried 147 people (86 passengers and 61 crew) from 23 different countries, so small for a cruise but still a sizable mix of people to have in one space.
The extent of their contact with wildlife before or during the expedition is either unknown or disputed, although there are plenty of rumours linked to bird watching etc. The importance of all of which will become apparent when we talk more about the virus and it’s standard transmission routes.
It is also worth noting, that unlike many cruises which have a curcular route with all passengers embarking and disembarking at the same point, with this cruise a number of passengers departed at various points as part of planned departures, therefore dissemination of some people involved had already occurred before any clinical symptoms were understood.
Headlines began to appear linked to a possible outbreak onboard in early May, with the outbreak developing, and more information gradually becoming available, as so often happens during any outbreak situation.
What are Hantaviruses?
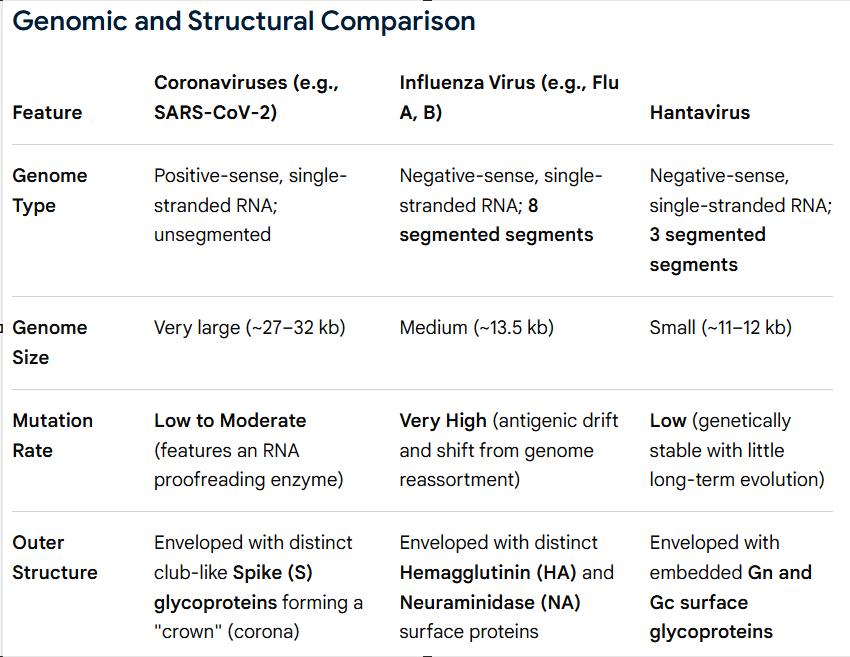
First let’s start with the fact that Hantaviruses are very different from the viruses that we have seen causing pandemics over the last century. Although all three are RNA viruses, Hantaviruses are different in structure, transmission and disease presentation to both coronaviruses and influenza viruses. They demonstrates low comparative rates of mutation and very limited person to person spread, so the same epidemiological principles do not apply.
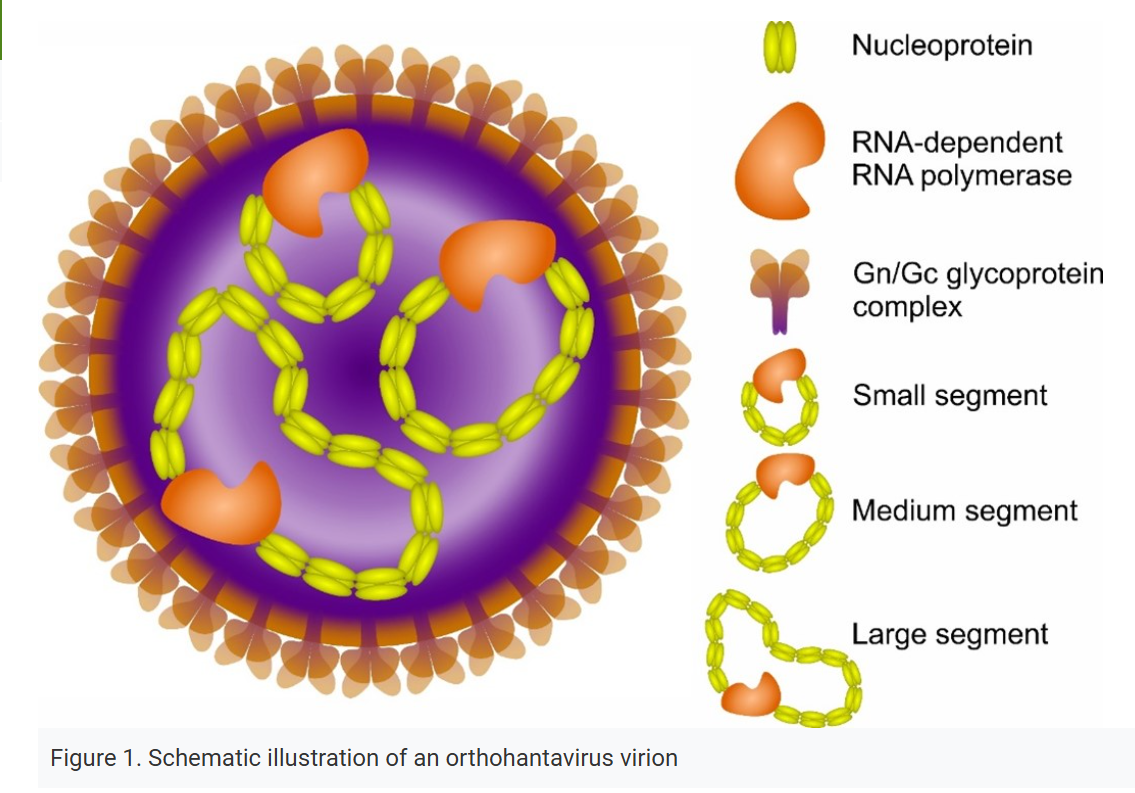
Hantaviruses are RNA viruses that are part of the genus Orthohantavirus. They were named after the Hanta river in South Korea in 1978 (originally called the Hantaan virus) and consist of a family of viruses rather than one single disease, with over 20 species known. As a viral group they have since been split into Old World Hantaviruses and New World Hantaviruses, with viruses found to circulate not just within rodents but also within moles, shrews and other animals. They circulate asymptomatically within their natural zoonotic reservoirs without causing symptomatic infection. When humans are exposed, and infection caused, it is typically due to spread from their normal reservoir with exposure due to interaction with bodily fluids, such as dried urine and droppings.
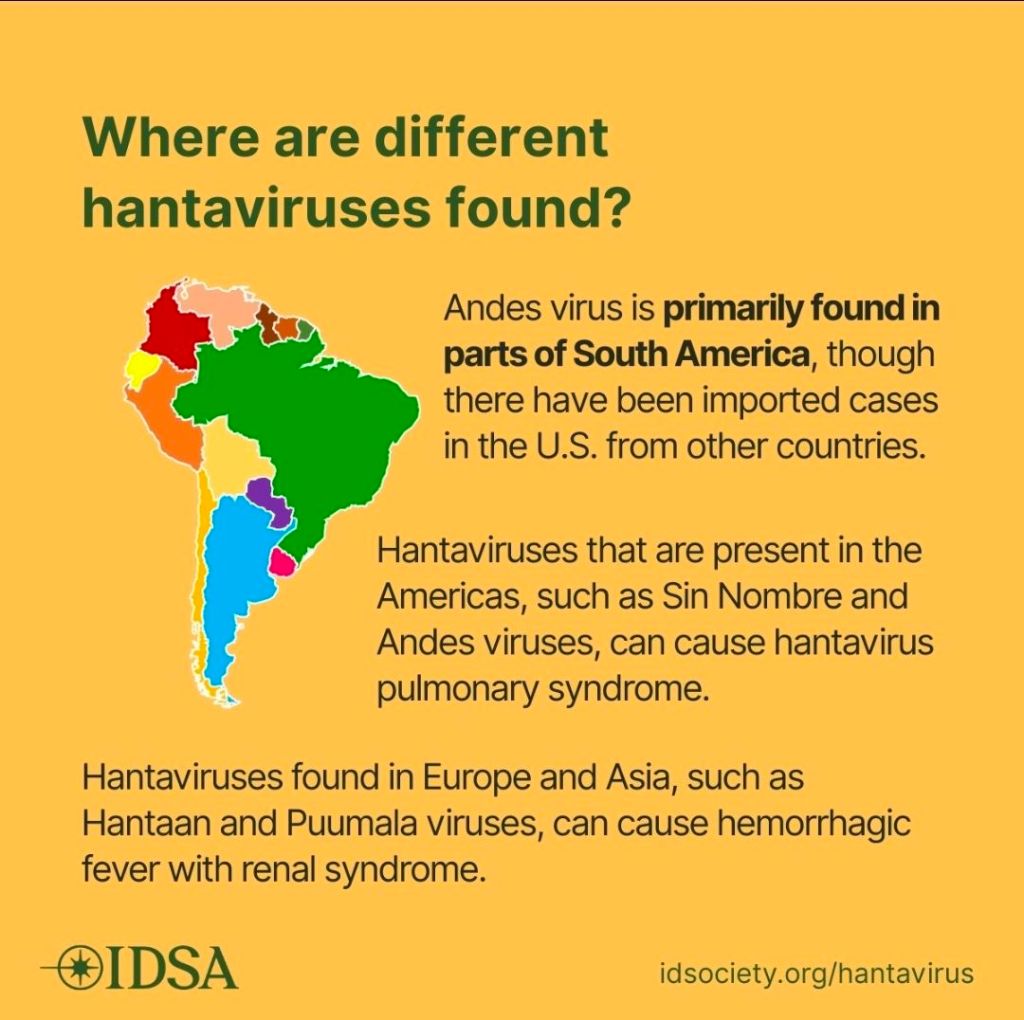
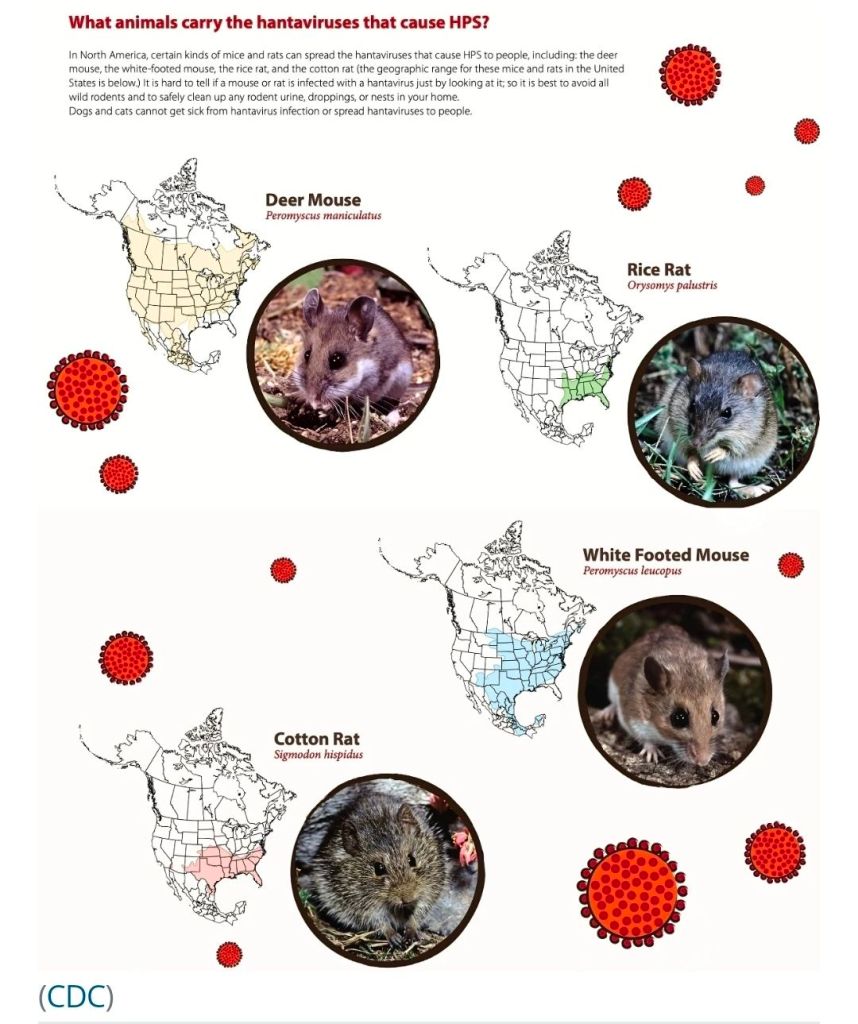
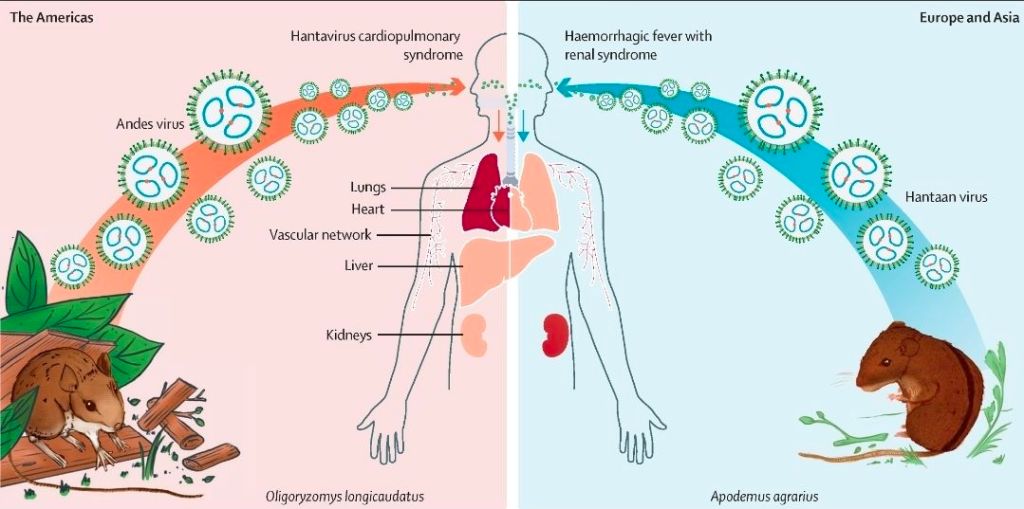
Different Hantavirus species are associated with different animal reservoirs and their associated geographical territories, as well as leading to different clinical presentations in human infection. Old World Hantaviruses are linked with hemorrhagic fever with renal syndrome (HFRS) and are geographically associated with Africa, Asia, and Europe. New World Hantaviruses are associated with hantavirus cardiopulmonary syndrome (HCPS) have a geographical and have a distribution across the Americas, sometimes also called hantavirus pulmonary syndrome (HPS). As the cruise exposure focus is mostly linked to South America, due to both cruise stops and clinical HCPS presentation, the main animal reservoirs of interest are:
Long-tailed Pygmy Rice Rat (Oligoryzomys longicaudatus)
Pygmy Rice Rats (Oligoryzomys species)
Vesper Mice (Calomys species)
Although there have been a number of cases in the current cluster confirmed as positive for the Andes virus, for context, in Europe (according to ECDC), just under 1,900 cases were recorded in 2023 across all different strains/species of Hantavirus. In the Americas, 8 countries reported 229 cases in 2025. There are, therefore, cases of Hantavirus infection detected annually across the globe, and although not huge numbers the impacts on individuals can be significant. The number of cases that are currently being observed linked to the cruise are therefore considered to be an outbreak, but the risk is mainly due to how individuals that will need to be repatriated to their native countries will be managed and how to ensure the best possible outcomes for those exposed.
What are Zoonotic infections?
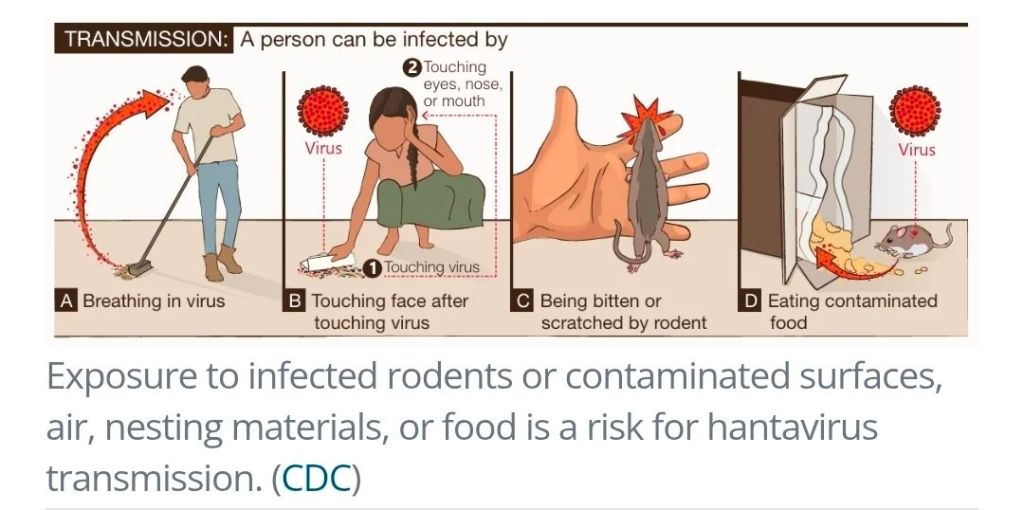
A zoonosis (or zoonotic infection) is an infectious disease that can jump from a non-human animal to humans. Traditionally it will have no, or limited, ongoing human to human spread. Transmission can be:
Direct – touching, petting, biting, leading to direct contamination by saliva, blood, urine, or other bodily fluids
Indirect – exposure to saliva, blood, urine, or other bodily fluids via indirect routes such as contamination linked to food, contaminated environments where animal reservoirs live (soil, water etc), contaminated objects
Vector borne – not linked to Hantaviruses, but for other organisms can be spread linked to insect carriage and transmission via insect bites
I’ve talked about the fact that Hantaviruses have animal reservoirs. But which animal, depends on the Hantavirus species, which then impacts where there is a risk of acquisition, as you can’t be exposed if the animal doesn’t live there.
The cruise had been visiting remote wildlife areas, so a passenger could have come into contact with the virus then, or before boarding the ship, as the incubation period is prolongued. This can make contact tracing and understanding the epidemiology more challenging, at least initially, and it is possible that the initial transmission event will never be well understood. The animal reservoir associated with the identified Andes virus, the causative agent of the outbreak, long-tailed pygmy rice rat (Oligoryzomys longicaudatus) and Pygmy Rice Rats (Oligoryzomys species) which can help to pin down broad areas, but not precise transmission route.
Transmission
Transmission linked to zoonotic infection happens in two main ways, transmission within the animal reservoir where infection is usually without any symptoms (asymptomatic), and exposure to humans to the virus circulating within the animal reservoir.
Within the animal reservoir transmission can be linked to moments like aggressive acts, such as biting and scratching where saliva or bodily fluids may be transferred. This is probably one of the primary mechanisms. Animals may also share environments leading to close contact, such as sharing nests, and viral transmission can be linked to exposure in close quarters.
This transmission linked to close contact is also an unusual feature of the Andes Hantavirus and can occur in humans and not just within the animal reservoir. Even so, human to human transmission is relatively rare, but can occur when individuals have prolongued close contact with someone who is symptomatic, especially if exchange of bodily fluids can occur via kissing or other close contact. There is also believed to be an airborne transmission route for the Andes virus, although the route by which this occurs is not well understood. This is addition to the transmission routes from the animal reservoirs that can be due to a number of exposure routes:
The initial clinical presentation of the 70-year-old Dutch passenger, who developed a fever, headache, and diarrhea day 6 of the cruise, five full days after boarding, and who then died on day 11. This timeline means the passenger is unlikely to have acquired Hantavirus onboard as the minimum Hantavirus incubation is believed to be 7 days, meaning that the exposure was likely to have occurred before the passengers even boarded the ship. Ongoing transmission onboard is therefore unlikely to have been point source from an animal exposure, and is more likely to have been linked to close contact of human passengers.
Clinical presentation
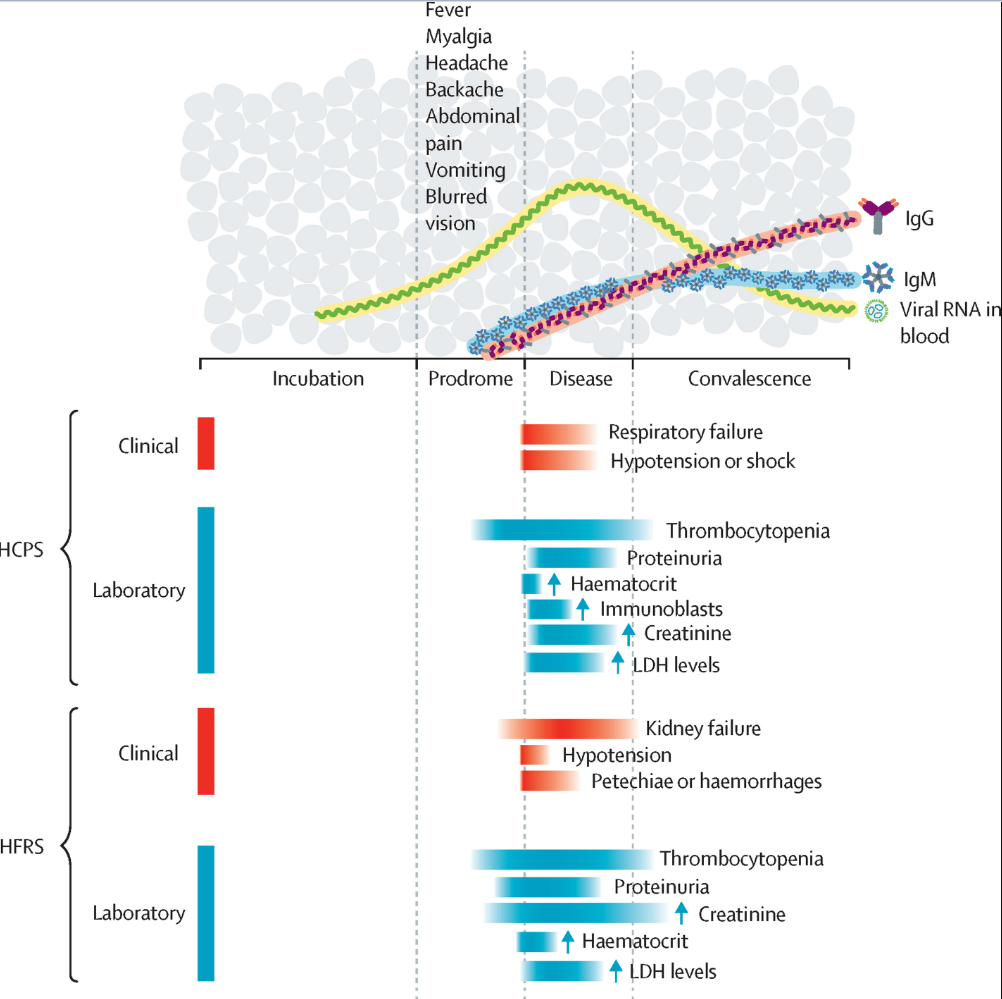
Initial presentation of HCPS is pretty generic, and could easily be hard to recognise as Hantavirus infection without a string travel or exposure history. The prodrome phase, or early onset phase is usually 1 – 5 days long and can occur 4-42 days after exposure. Symptoms can be confused with many other viral illnesses and include:
High fever, chills, and profound fatigue
Severe myalgia (muscle aches), particularly in large muscle groups like the thighs and back
Prominent gastrointestinal symptoms: nausea, vomiting, diarrhea, and abdominal pain
Headaches and dizziness
One to two days after the initial phase patients can enter a cardiopulmonary phase where patients can become critically unwell:
Rapidly progressive dyspnea (shortness of breath) and hypoxia
Noncardiogenic pulmonary edema (fluid in the lungs) and coughing
Hypotension, tachycardia, and cardiogenic shock
Potential myocardial depression and acute metabolic acidosis
Vial P, Ferrés M, Vial C et al. Hantavirus in humans: a review of clinical aspects and management The Lancet Infectious Diseases, 2023; 23, e371-e382
This is different to the progression of HFRS, which typically has five phases:
Febrile Phase (3–7 Days)
Hypotensive Phase (Hours to 2 Days)
Oliguric Phase (3–7 Days)
Diuretic / Polyuric Phase (Days to Weeks)
Convalescent Phase (Weeks to 6 Months)
The initial febrile phase is still pretty non-specific in terms of presentation, but tends to include high fever, chills, intense headache, severe backache, and abdominal pain. Mortality rates vary by causative species, but range from 1 – 15%.
Vial P, Ferrés M, Vial C et al. Hantavirus in humans: a review of clinical aspects and management The Lancet Infectious Diseases, 2023; 23, e371-e382
Transmission control
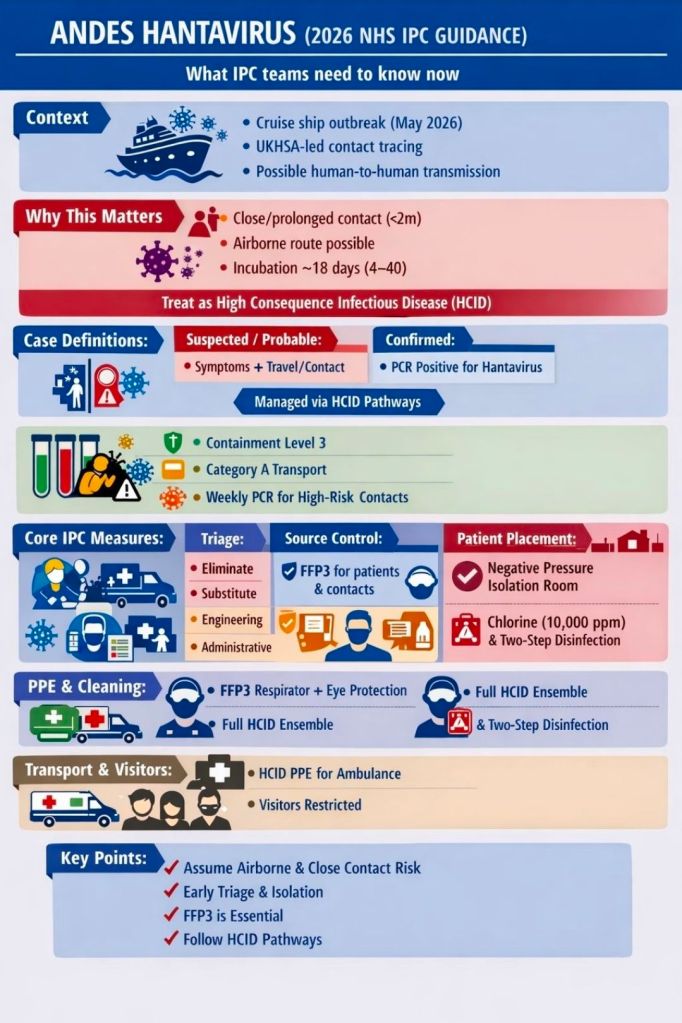
Within the UK, Hantavirus infection caused by Andes virus is classified as a high consequence infectious disease (HCID). HCIDs are defined based on the following criteria:
Requires an enhanced individual, population and system response to ensure it is managed effectively, efficiently and safely
Acute infectious disease
Typically has a high case-fatality rate
May not have effective prophylaxis or treatment
Often difficult to recognise and detect rapidly
Ability to spread in the community and within healthcare settings
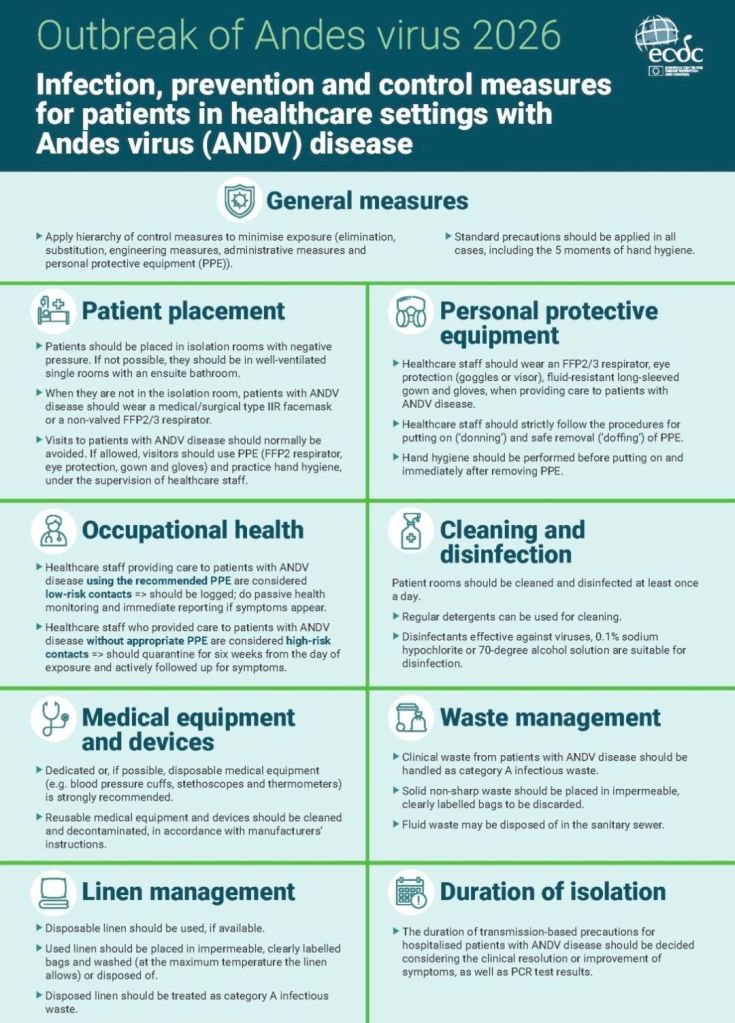
Interestingly, only the Andes Hantavirus is listed as a HCID, due to the risk of airborne human to human transmission. Once an HCID is confirmed or highly probable based on a combination of exposure history, symptoms, and diagnostic testing outcomes, the patient will be transferred by specialist transport teams to a designated HCID Treatment Center or High-Level Isolation Unit (HLIU). There are 7 adult and 5 paediatric Airborne HCID Treatment Centres in England, all of whom will hold specialist isolation facilities.
Early diagnosis of Hantavirus infection can be difficult, especially within the first 72 hours of symptoms, before the virus can be accurately detected in body secretions and excretions. Repeat diagnostic testing is often done 72 hours after symptom onset. As the initial presentation is fairly generic, it can take some time to realise what additional testing is required, and a good travel and activity history is key to informing diagnostic steps.
Within the UK, diagnostic testing options include:
Serology (Blood Tests): This is the primary diagnostic method. Laboratories use Enzyme-Linked Immunosorbent Assays (ELISA) or immunoblot assays to detect hantavirus-specific Immunoglobulin M (IgM) which looks for recent infection and IgG antibodies which looks for more established immune response, both by testing blood serum samples.
Molecular Testing (RT-PCR): Reverse transcription-polymerase chain reaction (RT-PCR) is used to detect hantavirus viral RNA in acute blood or blood samples during the viraemic phase, when the virus is present within the blood stream.
WHO update 6th May 2026
Internationally, one of the challenges for control in this specific outbreak, was that this wasn’t a point source exposure where everyone is incubating according to the same time frame, as people left the ship at different times, and were also isolating onboard the ship over different time periods based on the level of contact with the initially cases. This made initial components of contact tracing challenging, which then led to further possible exposures as some of the initial passengers returned to their home countries before the extent of the outbreak was understood.
Clinical management
There is no specific antiviral treatment option for Hantavirus so management focuses on supportive therapy, respiratory support (often in intensive care), fluid management, and for HFRS dialysis. Among patients who have severe respiratory symptoms as part of HCPS, the case fatality rate has been estimated to be approximately 38%.
As part of the follow up for this current outbreak, UK nationals, once repatriated have been taken to an isolation facility where they will be kept for up to 72 hours and initial clinical review and testing will be undertaken. As part of this clinical teams will then assess whether contacts who are not displaying symptoms can isolate at home or at another suitable location based on their living arrangements. Exposed individuals are generally being advised to self-isolate for up to 45 days from their last known exposure, but this self-isolation is voluntary. During the isolation period clinical networks will maintain daily contact to check for potential symptoms and undertake regular testing.
The World Health Organization (WHO) has recommended a 42-day quarantine period for the cruise passengers from their last exposure, although within the UK this has been extended to 45 days. Cases are managed, if symptoms develop using the following case definitions:
Confirmed Case: A patient with positive PCR testing for hantavirus in clinical samples, combined with travel on the MV Hondius from 1 April 2026 or contact with a passenger within 45 days of symptom onset.
Probable Case: A patient with compatible symptoms (e.g., fever, respiratory distress) and no other identified pathogen, linked by travel or close contact to the MV Hondius outbreak.
Possible/Suspected Case: A patient with compatible symptoms and no other identified pathogen, who had contact with a MV Hondius passenger within 45 days of symptom onset.
Previous outbreaks
Although all of this information seems rather intense and it is easy to see why the new media are trying to make a big story out of it, apart from those exposed we do need to put this outbreak into context. Outbreaks of Hantavirus happen with relative frequency, probably more than we know as diagnosis can be difficult identification may be underestimated, and some local outbreaks are probably under reported. To help demonstrate this I’ve put together a list of previous, easy to find, outbreaks along with their case numbers:
Argentina Regional Outbreak (Late 2025 – Early 2026)
Cases: A spike in localized regional cases with the NEJM reporting 34 cases from a single event.
Deaths: Up to 20 deaths.
Germany Voles-Linked Surge (2025)
Cases: 55 cases in the first half of the year (predominantly in Bavaria)
Driven by an ecological spike in the local bank vole population.
Brazil Farmland Outbreak (September 2022)
Cases: 22 cases.
Deaths: 10 deaths.
Traced to wood and rice mice exposure on agricultural properties.
Episodic Outbreaks in Los Santos, Panama (2022)
Cases: 29 cases recorded over nine months.
16 manifested as severe HCPS; no fatalities reported.
Argentina Andes Outbreak (2018)
Cases: 34 confirmed cases.
Deaths: 11 deaths.
Someone sick with ANDV attended a birthday party with 100 people; 5 people who were seated close to the individual later developed symptoms
Yosemite National Park, USA (2012)
Cases: 10 confirmed cases.
Deaths: 3 deaths.
Contracted by visitors staying in signature tent cabins infested with deer mice.
Chili (1997 – 1998)
Cases: 25 cases were officially recognized as part of the primary outbreak wave from July 1997 to January 1998.
When expanding the surveillance period from October 1995 through January 22, 1998, a total of 33 cases were confirmed nationwide
Epidemiologists verified human-to-human transmission across two out of three family clusters identified during the outbreak
The Korean War Epidemic (1950–1953)
Cases: 3,000+ UN soldiers infected.
The landmark historical event that first clinically defined Hantavirus Hemorrhagic Fever with Renal Syndrome (HFRS)
What is currently happening with this outbreak?
As this post has taken me a couple of weeks to pull together, I thought it was worth ending with the latest update I have available from the European Centre for Disease Prevention and Control (ECDC) on 24 May. At this point 12 cases have been reported in total, including 10 confirmed and 2 probable cases. One new case and no new deaths have been reported since the previous update (unclear when the last update was).
ECDC update on 24th May
The cruise ship M/V Hondius has had all passengers and crew disembarked and is currently docked in Rotterdam, the Netherlands, undergoing sanitation procedure.
The short answer is no, I don’t believe so and neither do many people who are far more expert than I that you will hear write and talk on this subject. This scenario has got me thinking though, if this outbreak hadn’t impacted European and US passengers whether we would have even heard about this outbreak at all. As you’ve seen in the outbreak section, Hantavirus outbreaks are not that uncommon. Was it because of passenger social media that it made headlines, because the cruise industry is big business, or because it impacted audiences because they saw passengers as being ‘like them’ and worrying that they too could be impacted on a holiday?
I think, whatever the reason, that this should be used as a wake up call for all of us to realise that infection diseases are global, and that we ignore infections that we don’t consider to impact ‘us’ at our risk. With global travel, with climate change, with changes in health surveillance due to certain US policies, the old way of looking at infectious diseases may not be fit for purpose. Too much of the world is in pandemic denial, and just doesn’t want to think about infection risk. We either experience coverage that induces panic, or ostriching where we don’t talk about it at all. Neither of these approaches are going to lead to the best outcomes or knowledge sharing in the face of a changing infection landscape. What needs to happen is for global networks to be built, for infrastructure to be invested in, and for communication to occur in a way that supports surveillance and knowledge acquisition. I don’t believe that Hantavirus is a risk for developing a new pandemic, but if we don’t take the time we have available to invest in planning, we won’t be as prepared for the next outbreak that could be.