
Last week I wrote about the challenges of the current Ebola virus outbreak, talking about some details linked to the virus itself, and also some challenges that mean this outbreak may be more challenging to manage. I was involved in previous outbreaks, but definitely in a peripheral support capacity, because of my underlying autoimmune condition I did not travel to Sierra Leone. Context and learning from previous events is important however, so I tapped my good friend and colleague Ant De Souza, who was directly involved in supporting diagnostics, to write me a guest blog of his experiences.
Anthony De Souza is an award-winning Healthcare Science educator with over a decade of experience as Biomedical Scientist in microbiology. He was the first Healthcare Scientist to gain a permanent Practice Educator post, a post he has only continued to develop and expand since its inception. Ant’s transition into strategic education leadership has empowered the Healthcare Science workforce to improve patient outcomes based on his approach; which links strengthening multidisciplinary collaboration, expanding clinical capabilities, and elevating the profile of the healthcare science workforce to ensure they are invited to have a seat at the table. The impact of this has been recognised not just by me, but by him being named on The Pathologist’s Power List for his outstanding contributions to the field.

Ebola Deployment, Sierra Leone – A Personal Reflection
In 2015, when an urgent appeal was issued by Public Health England (now UKHSA) for scientists to support the Ebola crisis in West Africa, I didn’t hesitate—I knew I had to go.
In the past, I’d seen similar calls for volunteers and questioned whether my skills were enough to make a meaningful contribution. The last thing I would ever want was to become a burden on a mission of such importance. But this time felt different. For the first time, my experience, confidence, and mindset aligned with what was needed. I was working as a Band 6 Biomedical Scientist at Watford General Hospital, in a busy microbiology department delivering a 24/7 service. I was used to working under pressure, and I felt ready to contribute.
Before committing, I spoke with my colleagues. A five-week deployment would mean they would take on additional workload, and it was important to me that I had their full support. With their encouragement, I signed up.

Preparation and training
Preparation for deployment was thorough and, at times, intense. I travelled to Porton Down in Salisbury for specialist training, where we learned how to work safely with high-risk pathogens such as Ebola. This included simulation exercises in a laboratory environment designed to mirror the Kerrytown facility, where we practised managing realistic scenarios, including equipment failures and power outages.
We also completed security awareness and hostage survival training, alongside a series of vaccinations for diseases such as yellow fever, cholera, and typhoid. Anti-malarial medication was essential. The preparation highlighted not only the scientific challenges ahead, but also the environmental and personal risks we would face.
The journey
Getting to Sierra Leone was a journey in itself. We travelled by plane, transferred in Morocco, then boarded another flight to Freetown. From there, the journey continued by minibus to a port, a boat crossing, and finally another minibus to the site.
It was a strange experience travelling with a group of people I had never met—yet over the course of five weeks, these individuals would become a close-knit team.

Arrival and first impressions
On arrival, small behavioural changes immediately became part of daily life. Handshakes were replaced with elbow taps, a simple but important measure to reduce transmission risk. Regular temperature checks became routine, particularly at checkpoints when travelling to and from the treatment centre.
We were based at the Ebola Treatment Centre (ETC) in Kerrytown, outside of Freetown—a facility built by the British Army Royal Engineers and funded by the Department for International Development. The scale of the operation was impressive, and there was a strong sense of shared purpose. People from different organisations and backgrounds worked together with a single goal.
The ETC was divided into zones based on risk, from green (low-risk areas) to red (high-risk patient areas). Full personal protective equipment (PPE) was mandatory in higher-risk areas.

Working in the laboratory
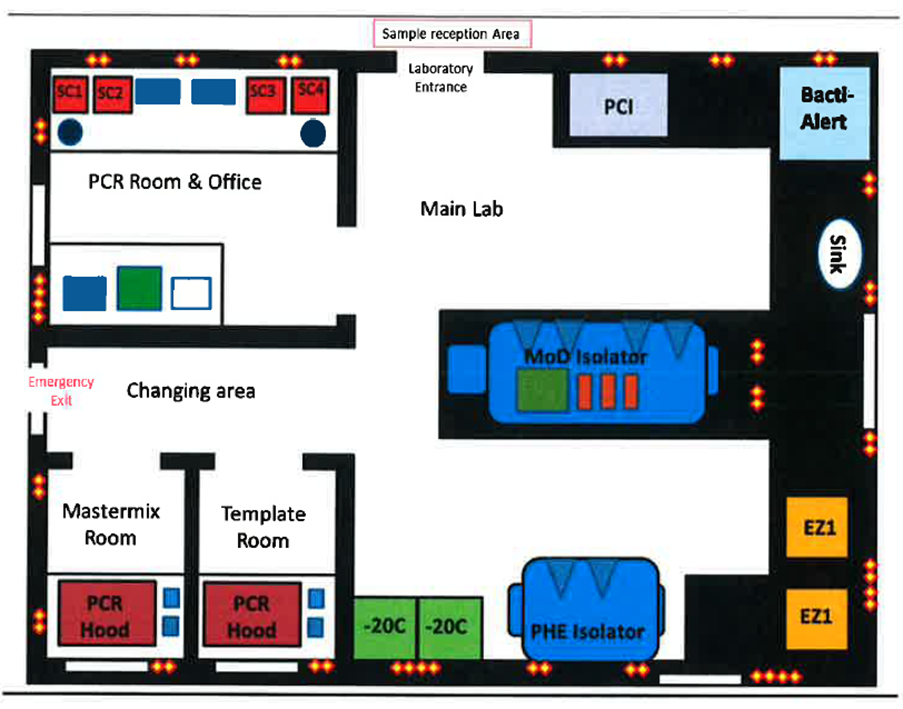
Our laboratory was located centrally within the site, shared with the Ministry of Defence. After donning PPE, we met the outgoing team and received a rapid but essential handover. For a few days, we worked alongside them before taking full responsibility.
Our role was to test blood and swab samples from individuals suspected of having Ebola. We operated six days a week, with two teams of six covering shifts from 06:00 to 22:00.
Many samples came from community settings, including remote villages. A significant proportion were post-mortem samples, taken to determine whether Ebola had caused the death. The high number of samples from children and infants was particularly difficult to process emotionally.
Specimen reception took place outside the lab. Samples were placed into chlorine solution for decontamination before being handled further. Wearing full PPE in the heat of the sun was physically exhausting, and the need for constant vigilance—checking for incorrectly packaged samples or hidden sharps—added to the pressure.
Inside the lab, resources were basic but functional. The space had sealed cement benches, limited air conditioning, and no negative pressure system. Testing was carried out using PCR techniques for Ebola, alongside POCT testing for malaria. A flexible film isolator was used to safely inactivate the virus before analysis.
Life beyond the lab
Outside of the laboratory, the scale of the public health response was visible everywhere. Posters, radio messages, and community outreach efforts aimed to educate people about Ebola transmission, safe burial practices, and how to protect themselves.
Strict measures were in place:
- Large gatherings were prohibited
- Schools and religious services were disrupted
- Curfews were enforced
- Checkpoints monitored movement and health status
- Movement restrictions between districts
Daily life, as it once was, had largely come to a standstill.
Cultural challenges and adaptation
One of the most striking aspects of the outbreak was its impact on traditional burial practices.
In Sierra Leone, burial rituals are deeply rooted in cultural and religious beliefs. Traditionally, families wash, dress, and physically say goodbye to loved ones. However, in the context of Ebola, these practices posed a significant risk, as the virus remains highly infectious after death.
To reduce transmission, specially trained burial teams were introduced. These teams worked closely with communities and religious leaders to adapt traditions safely. While physical contact was removed, efforts were made to preserve dignity—allowing families to view the body from a distance, limiting attendees, and involving community leaders in the process.
This collaboration was essential. Without it, there was a real risk that families would carry out burials in secret, increasing the spread of the virus.

Reflections
There is much I could say about my time in Sierra Leone—far more than can fit into a single blog. The work was challenging, both physically and emotionally. There were moments of exhaustion, uncertainty, and sadness.
But above all, what stays with me is the resilience of the people.
In the face of immense hardship, communities adapted their traditions, supported one another, and worked alongside international teams to combat the outbreak. It was a powerful reminder that effective public health is not just about science or medicine—it is about trust, collaboration, and cultural understanding.
This experience reshaped my perspective on global health, teamwork, and the role we each play in times of crisis. It remains one of the most challenging and meaningful periods of my career.
All opinions in this blog are my own
