You may have noticed that I’ve been a little poor at keeping up with the Girlymicrobiologist site admin, and missing the odd weekly blog post. This isn’t because I’ve been slacking, honest, it’s more because I may have become a little distracted by a new project. I promise to get back on top of things soon, but in the meantime I thought I owed you an update.
Many of you have been kind enough to support last years project, which was a book aimed at supporting people to engage with research and research degrees, and I couldn’t be more grateful for your cheer leading. This new project, however, in the words of Monty Python could be described as ‘and now for something completely different’. It couldn’t be further from a book about academic study. This one is all about something else I love passionately, movies and TV.
I finished and launched the last book last October, and to be honest it hadn’t occurred to me, prior to letting it go into the wild, that I would write anything else till my retirement – when I’m planning to write some pathology based murder mysteries. It was never the plan to do something again, at least so soon. Frankly though, my brain tends to disrupt all my best laid plans, and ideas come meaning I just can’t help myself but get swept up. I’m blaming Ian McKellen inspiring me to ‘practice any art’.
Despite having no plans to do more, I have to say that I really enjoyed writing the first book, and I found the process of being able to write in a different way very fulfilling. I love writing this blog, and the first book is based on a lot of the pieces I have written for here, but it was nice to see them come together and take on a new and different life of their own. I also enjoyed mixing up the writing of something on a single theme with writing blogs on different topics for here, although I did rely a lot on Dr Claire Walker bringing together many guest blogs to allow me some writing time. It was lovely to see what those guest blogs brought to the site, and I really enjoyed seeing how including those voices really makes this feel even more like a community space. Without realising it, I think I caught ‘the bug’. Now, I’ve always enjoyed writing, this is my happy space, but I had never seen myself as an author, having held a book I’d written in my hands though, I can see how it could become a little addictive.
As I was sitting watching horror movies as part of my post release recovery, and researching for my 2025 Halloween post, I suddenly realised what I’d like to do next. I really wanted to write about some duel loves of mine, movies and TV plus infection.
Without any expectation of writing another book, all of a sudden I had a structure in my mind, and Don’t Open That Door had began…
You all know how much I am a movie and TV buff, everything from guilty pleasure reality TV, like The Secret Lives of Mormon Wives, to documentaries, and all genre of film (with the exception of torture porn horror movies, I’m a Blumhouse girlie). Whilst enjoying some down time with Mr Girlymicro, I realised how widely infection is featured in all kinds of different genera settings, some of it was actually pretty good, whilst some of it was really poor. So the first step was to do a whole bunch of research about what kind of examples were out there, by hitting up a bunch of different lists that have been collated by others, internet searches, and sourcing opinions from my movie loving friends. All of which led to the creation of a list of 138 options that needed a review to see if if they were actually linked to infection, and if they were infection based….was the infection content any good.
If you follow me (Girlymicro) on Instagram, you will have probably seen a number of stories that I’ve posted recently linked to movies I’ve been watching with some Infection Prevention and Control/micro commentary:
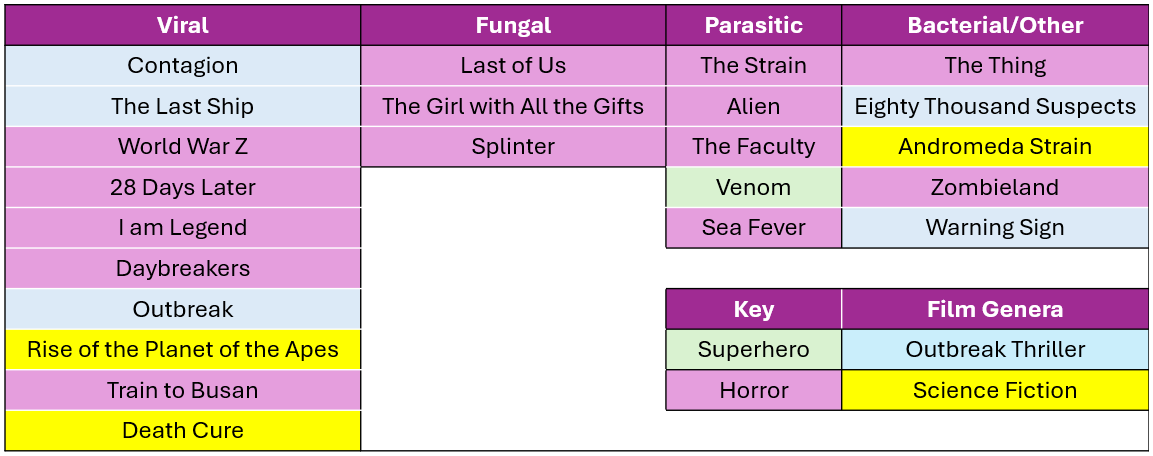
These have come about whilst I’ve been watching the 138 films/series with Mr Girlymicro to decide which ones make the cut to be included. I’ve watched some awesome films, some like Sinners, weren’t based on infection so couldn’t be included. I have also watched some truly bad movies, I even gave Resident Evil another go, and have spared you all by making sure that it is not included on the list. One of the considerations was that, even if the science wasn’t dreadful, I haven’t included anything that I or Rotten Tomatoes include as being truly horrible. I’m not just saving you on this, but also myself, as I’m having to watch included examples many times as part of the writing. I also felt it was really important to cover infections linked to viral, fungal, parasitic, and bacterial causes, just because they behave so differently and the interventions needed are so different. So the final list for inclusion involves movies and TV series that sit across infectious agents, although viruses are more represented than any other cause.
There are plenty of horror movies on the list, purely because they represent A LOT of the infection genera, but I was surprised at how many options there were outside of horror movies. I also tried to mix up certifications where I could, so that there are some options that everyone might enjoy.
Not everything could be included however, and there were also some exclusion criteria that impacted what I could include. Exclusion criteria included factors such as availability – no point including things that people can’t access, language options – I sadly only speak English so it needed at least English subtitles, and most importantly not based on real life events – this is about fiction.
For inclusion examples also needed to have infection as a central theme. This meant that health dramas could not be included as they only feature infection in some episodes, but at some point I do really want to write something that compares different medical dramas (House, New Amsterdam, Holby City etc) and maybe do a ranking scale….let me know if you think that would be a fun blog post.
Image credit The Red Dress
The reason it felt timely to talk about this today, is that the Biomedical Scientist magazine has been kind enough to do a whole feature on what the new book will look like, with a bit more detail, and some examples of what chapters will look like. It dropped on the 27th March and you can check it out the link here: https://thebiomedicalscientist.net/2026/03/24/infections-films. Also, how awesome is the art work they’ve done, can’t say enough how awesome The Red Dress are.
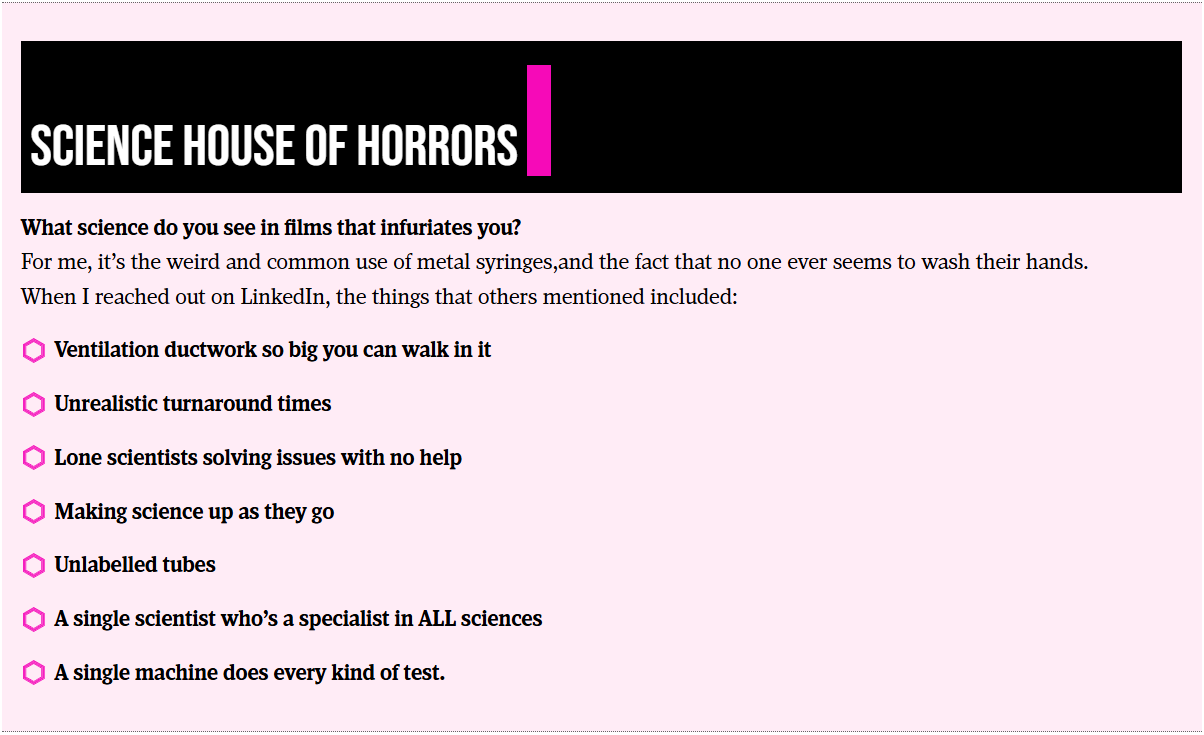
Whilst writing the article for the Biomedical Scientist and watching the example movies, I couldn’t happen but note how many weird and wonderful things are included as part of the science representation. Things that in my scientific career I rarely if ever encounter, but seem to crop up time and time again in Hollywood depictions of scientific life. I’m collating these for one of the final chapters in the book called ‘Science House of Horrors’ as I find them a bit fascinating. I’ve included some of the ones in the Biomedical Scientist article that I noticed, as well as those sent through as responses from social media, but I’d love to know if you have any others that I should include.
There are other opportunities to get involved though, I have 23 films and series examples, but there is room in the book to cover 25. I’m really keen to get other examples that include fungi, but if there is just something brilliant I haven’t included please let me know. There will also be a chapter called ‘Hall of Fame’ that covers both amazing movies that just don’t have enough infection in them to be included, or ones that were great but not quite as good an example of an infection characteristic as the ones already included. There is also the ‘Hall of Shame’ for examples, such as the TV series The Rain and Resident Evil, where the science is so bad that it is note worthy in itself.
Anyone who drops me an email to elaine@girlymicrobiologist.com and inputs into the House of Horrors, volunteers film examples I’ve missed, or suggests contenders for the ‘Hall of Fame’ or ‘Hall of Shame’, will get their name included in the list of contributors at the back of the book. Science takes a village, so does pulling together a book, and I’m really keen that this feels like it comes from our community. I hope you enjoy the article and I can’t wait to hear from you about your suggestions.
I am not a big Halloween girly, to be honest I can take it or leave it because I’m mostly excited about the build up to Christmas. That said, what I do love are movies and TV, and despite never being someone who can tolerate a lot of slasher or gore based horror movies, I love a good vampire movie.
A lot of this may be because I enjoy the world building and lore that seems to be more integral to vampire movies and series. This is because, although they share some of the same rules, depending on how the world is built they always need to explain which of the nuance comes into play in that particular setting. It felt fun this Halloween therefore, to write a blog post that talks about some of those tropes when vampirism is linked to infection, and how those rules compare to the real world.
Common vampire tropes to be aware of and to bear in mind as you read on:
Experiencing pain or physical damage in relation to sunlight
Needing to consume blood as a protein source
Inability to eat or digest food other than blood
Avoidance of animals
Ability to influence humans to undertake acts that may be against their will
Violent reactions to garlic
Inability to see themselves in mirrors or via cameras
Death only by beheading
Death by wooden stakes
Damage linked to holy water
Aversion to signs of faith
Aversion to alcohol or drug use
Not all of these are present in every piece of world building, hence why I find the variety of vampire mythos so interesting. The choice of which ones go together combined with different origin stories and creation processes enable a pretty large tapestry to be created from some similar thematic components.
Mystical, infections or something else?
The place to start I guess is by discussing whether all vampire world building includes infectious transmission? And the answer is a definitive no. Sometimes the way that the creation of new vampires works isn’t discussed. Sometimes the rules about the underlying process is unclear. That said, the fear of becoming something new is a frequently used trope for dramatic purposes and so the process by which a human is turned into or by which vampires exist is discussed pretty frequently as part of world building, and from what I can see there are three main routes:
Mystical – some form of occult/magic/cause not routed in science
Genetic – vampires are born and exist as a stand alone species
Infection – transmission via blood or other infectious transfer, even if the agent is unclear or unspecified
Now, I’m not going to cover the mystical/magically as that’s not anything based in science and the science is what I’m here for. The other two, however, are often based (sometimes loosely) in science as they are often inspired by things that actually exist and so I’m going to talk about both of those in a bit more details.
Genetic
I’m going to kick off by talking all things genetics. There are an increasingly large number of vampire movies and TV series where the vampires that featured were born vampires. This includes movies like Abigail, Perfect Creatures, the finale of the Twilight series, but also TV series such as A Discovery of Witches, First Kill and Vampire Academy. Sometimes within these there are vampires that are made through other means (discussed below) in the same world. Often these genetic vampires exist as a separate species to their Homo sapien neighbours either openly or in hiding.
There is often much discussion about where the vampire myth comes from, and in many way these stories of genetic vampires who are birthed through a similar route to standard human deliveries, links in most with what is considered to be a real world inspiration for many vampire myths. The origin is thought to be linked to a rare inherited condition known as Porphyria, the presentation for which may account for for some of the common components of vampire portrayals.
Porphyria is a rare, inherited blood disorder that occurs when the body can’t convert porphyrins into haeme, a vital component of haemoglobin. The resulting symptoms vary depending on the type of porphyria. Acute porphyria presentations include symptoms such as gastro intestinal pain and symptoms like nausea and vomiting – symptoms that are often portrayed linked to vampires attempting to eat normal food. Whilst cutaneous porphyria symptoms include pain, burning and swelling in response to sunlight, skin fragility and a tendency towards skin blistering – all of which are frequently included as vampire responses to exposure to sunlight.
Porphyria D. Montgomery Bissell, M.D., Karl E. Anderson, M.D., and Herbert L. Bonkovsky, N Engl J Med 2017;377:862-872 VOL. 377 NO. 9
Interestingly, in some of the genetic origin vampire stories, the impact of some of the limitations of the lifestyle limitation of traditional vampires are not so extreme. In some of these cases they can be seen in daylight, although not for long and don’t enjoy it, and they may be able to tolerate some, if not all, of human food. They are possibly therefore most aligned to their real world inspirations. I could write pages and pages on this, but infection is where my heart lies so I’m going to crack on.
Virus, parasitic, others?
Now we’ve covered off those born vampires, let’s move onto the most common version of vampirism outside of the traditional Dracula more mystical inspiration, that is vampires who are created linked to transfer of infection by blood or other means.
There are three main ways that this commonly comes into play:
Viral causes
Parasitic routes
Bacteria intoxication
I’m still trying to find a vampire movie where the main infectious agent is fungal, but it seems that most of the movies based on fungi are linked to zombie outbreaks. That makes a lot of sense, due to the fact that fungi are eukaryotes (like us) rather than prokaryotes (like bacteria), and so fungi tend to be linked to changing behaviour linked to interfering with the human nervous system. If you’ve seen a vampire version though please do let me know as I’m collating a list of where different organisms might come into play.
By far the most common route depicted is where the causative agent is a virus. Viruses are featured in movies such as Blade and Daybreakers and TV series such as Ultraviolet. This is because viral transmission in general is associated with transfer of bodily fluids, be that faecal-oral, respiratory via saliva, bodily fluids such as breast milk, or in the case of vampire movies via blood.
The most uncommon causative agent I’ve discovered is the parasitic cause of vampirism as shown in The Strain TV series. During the series transmission of the virus to create a full vampire is via something known as ‘The White’ that contains parasitic worms. These then lead to anatomical changes, including the growth of a proboscis that enables the biting and transmission of the parasite to others.
Bacterial coverage is mostly linked to potential methods of intoxication that supports the control over humans by vampires. Rather than being a direct cause of the vampirism, this seems to be about how transfer of the bacteria releases, or causes anatomical change, which then changes behaviour via things like hormonal or neurological changes. I’ve talked before about why bacteria may feature less in horror movies than other causes, but this can mostly be summed up by the fact that audiences tend to know more about bacteria and therefore it is less tempting for writers, but also horror tends to sit better in ‘the possible but not too close to us’.
Transmission
Obviously it’s not just the infectious agent that is important, but the mode of transmission for that agent. This being all about vampires the biggest mode of transmission is by bite, but it’s not always so straight forward. In mystical vampire movies, there’s usually a whole lot of removing of the original human blood and then transfer of the vampire blood, leading to a mystical baptism and rebirth. Infectious causes are much more one way, any bite could lead to someone turning into a vampire and the most important thing is load related. If someone is in contact for longer, if more blood is drunk and therefore more saliva and fluids exchanged, then the chances of conversion are much higher.
It’s not just blood as a bodily fluid that features in conversion during vampire movies. There are also films, such as Requiem for a Vampire and Trouble Every Day, where vampirism is treated more like a sexually transmitted disease, rather than transfer occurring during feeding on the blood of their victims. It seems that these films have increased since the 1980s, maybe as a result of fear processing linked to the HIV/AIDS pandemic during that time period or maybe because our knowledge about and ability to detect infections has increased and therefore there are a larger part of the collective public awareness. It will be interesting to see how the SAR CoV2 pandemic will impact this further.
The most unusual transmission, and one that aligns most highly with blood borne transmission is the presence of congenital transmission as featured in Blade. Where the main character Blade becomes a vampire hybrid by acquiring the vampire virus at birth, due to his mother being bitten and placental crossing of the virus into his blood stream. As a result, he exhibits some of the characteristics of a vampire due to the virus, but the effects are attenuated linked to his exposure route. It can often be that congenital infection presents differently to primary infection via other causes, and it appears vampirism is no different.
The other variable is linked to the time to turning once the infection has been introduced. I would speculate that this too is load related, as well as the infectious agent behind the symptoms. Viruses, for instance, are likely to reproduce and induce change at a much higher rate than anything linked to bacteria or parasites. This is partly due to their reproductive rate, but also linked to the level of dose that tends to be available. The exception to viruses resulting in the fastest change is likely to be bacterial intoxication and influencing. As the toxin acts immediately, when this is present in media and TV the change is almost instantaneous, but also time limited and therefore requires top up or re-application. Not all impacts are until beheading, some require a more time boundaried set of interventions.
Interventions
Once your characters are aware that vampires exist within their mist, then they will want to look for actions in order to protect themselves. One of the classic ones as featured in many movies, including the classic Lost Boys, is garlic.
In some ways the impact of garlic makes even more sense if you think of vampirism through an infectious transmission route, as garlic has been considered to have anti-infective properties for a long time, although warning you may have to ingest a LOT of it!
Another common feature in vampire movies is the roles that animals play as protectors. For instance, in 30 Days of Night, the vampires kill all of the dogs before they launch their main attack. This kind of thing also often happens in films and TV where vampires are hiding in plain sight. It could be that they are taking out animals as they don’t want to be found, and animals are easier than humans, but I have another proposition. There are a number of infections where animals can be used to sniff out and identify infected individuals. Therefore, if animals could detect vampires they are much more likely to be a risk and warrant removal. Animals could therefore act as a front line of diagnostic defence to enable you to tell friend from foe.
Having determine that a common weakness of vampires is their damage response to ultraviolet light (UV), films such as Underworld weaponise light against the vampire protagonists. Light, and especially UV-C (200 – 280nm), has been known to impact viruses and bacteria for well over 100 years. When light is in this frequency is can damage both RNA and DNA, resulting in cell death, and it is possible that if the infectious agent is the only thing that is keeping your body moving the damage would be more pronounced. We’ve also discussed how the lack of some biochemical pathways can lead to UV-C causing much larger amounts of pain an damage.
Normally, penetration of the light to cause damage might be an issue, but if you are using bullets or other means this may not impact. The most important thing I have to say here is, that despite what is shown in Blade 2, light does not bend around corners. This is also important for when you are considering using UV-C in hospitals to support cleaning, it doesn’t have good penetration and doesn’t go around corners of work in shadows. Using UV-C may work against your vampires but you are going to need to think carefully about where you use it so it does what you think it can.
Vampire movies have amazing world building and are often my favourite genera in terms of their string internal logic. I love the fact that so many types of infection and route of transmission that reflect real world cases are present as part of these pieces of entertainment. They can actually teach us a lot, even when we don’t realise it, and so much of it has origins in real world knowledge, even if only loosely. So, this Halloween evening find one you haven’t seen before and let me know which intervention you would use to stop your town being turned into creatures of the night!
Before I go, I thought I would share a few of the previous years Halloween blog posts in case you are looking for some more spooky season and infection reading:
For my birthday in 2014, I celebrated by submitted by PhD thesis for printing. I ripped off the band aid and committed.
For this birthday, 11 years later, I’m taking another leap of faith, and once more rolling the dice on myself. This time it’s still PhD related, but rather different. This time it’s to let you all know that I have written a book, which will hopefully go live on Amazon on Friday the 17th October.
It feels like birthday launches could become a tradition.
I’ve been talking about a super secret project for a while now, and the wonderful Dr Claire Walker has been taking on some heavy lifting in terms of arranging some guest blogs, so that I could write a book on my weekends rather than writing a blog. But what is the book, and why did it come about?
The Book
The book is entitled ‘It Shouldn’t Happen to a PhD Student: How to thrive, not just survive, during your PhD’. It has 40 chapters that take you all the way through from deciding you want to do to PhD, and thinking about where and what type, to submitting your thesis, and what kind of skills you may need to develop during your PhD to maximise your career success after it is done.
Professor Elaine Cloutman-Green, otherwise known as “The Girlymicrobiologist”, is a clinical academic with over 2 decades of experience leading research projects and supporting students at all levels, including PhDs. She also runs the popular Girlymicrobiologist blog, which aims to de-mystify science and support those wanting to engage with academic careers from A-level all the way through to career enrichment.
In this book, Girlymicro talks about the reality of what it is like to study for a PhD, what gateways you may need to pass through, and how to manage key relationships in order to achieve success.
This book starts at the very beginning, with why you might want to do a PhD, how you might decide what route to PhD is right for you, and what a successful application might look like.
It then takes you through your PhD journey, year by year, with tips about how to approach and succeed during significant moments, such as attending your first conference, or writing your first academic paper.
Finally, you will discover what other skills you need to develop during your PhD to give you the best route to success after your viva. All of this supported by links to activities on the Girlymicrobiologist blog, to help you with practical exercises in order to apply what you have learned.
Whether you’re planning your PhD, a healthcare professional looking to develop, or simply curious to know about how the world of academia works, The Girlymicrobiologist offers a refreshing blend of knowledge and relatable experiences. Get ready to laugh, learn, and be inspired to find a way into, what she describes as the best job on the planet.
This is the book I wish that someone had given me when I started on my PhD. I was pretty clueless and spent a lot of time finding my way, and making heaps of mistakes. It seemed only fair to write all of my learning down so that I can share it, not just with my own students but more widely, so that everyone is free to make their own new mistakes, not just repeat ones I’ve already made.
The Why
I’ve been talking about writing a book for ages, and I still have the original Girlymicro book I’d planned going on in the background. I was prompted to do this book now though, after spending an afternoon at an awards event and realising that I could tell you every person who was going to win in every category before the dinner even started. It made me think a lot about access and privilege. That night I came home and I was really glum, and I couldn’t quite process why I was feeling that way.
I slept on it and spent some time speaking to Mr Girlymicro the next day to process my thoughts. I talked about how much access to healthcare professions and even academic training schemes are now based on who you know, to describe the best way to get through gateways like applications and interviews. How, even once you are in them, to feel like you understand how things work and the undisclosed boxes that need ticking, you need to have someone who will let you in and tell you the unwritten rules, and frankly not all supervisors see that as their role. This means that I really feel like we are missing out on some amazing talent. People who would make wonderful PhD students, or academics, because they can’t get across the threshold or see themselves in the role.
Not everyone has strong connections with a university. Still fewer people know someone who has a PhD. The way the system currently feels is that if you can access information you really have such an advantage over those that don’t. I therefore see a lot of my medical colleagues getting access to PhD funding, and yet fewer and fewer of my nursing and scientific colleagues. I increasingly encounter more and more undergraduates who are reaching out because they need help to know why they aren’t being successful, because they don’t know what is expected of them. It has always been hard to get onto PhD programmes, and it should be. What it shouldn’t be is hard because you don’t have access to the right people to give you the knowledge you need to level the playing field.
I realised that was why I was feeling upset and unsettled. I don’t like unfairness. I don’t like inequity. I don’t like realising that I’m part of the problem. Mr Girlymicro commented, as I was off loading, that I had plenty of blog posts that talk about how to apply for and do a PhD, and so why didn’t I take the way I was feeling and turn it into something positive. A book. So, this book concept was born. A book where I set out to play my role in fixing the disparities as I see them.
The Vision
That conversation happened right at the end of May. I gave myself 3 months to take some content form this blog, as well as creating new content, to come up with a book of ~80,000 words that captures the advice I give to my PhD students, and those approaching me floating the concept of applying for a PhD.
Why 3 months? Well, if I allowed myself a year, I would take a year, and remember that other book? I still want that to happen at some point. The other thing was that I wanted it finished as close to the start of the academic year as possible, so that it could start benefiting people right away. We all also know that I have no patience, and so using my birthday as a cut off always felt right.
The book was finished at the end of August, and I’m in final edits before upload at the end of the month. I want it to be the kind of resource that people can dip in and out of, whether they are doing a PhD or not. Chapters, such as developing goals, or on public speaking, should stand alone to benefit even those who are not in academic study. The activities that can be accessed alongside the book, to help things like developing your elevator pitch, should only grow in number over time, and hopefully will be a good general resource for anyone that finds them, not just for those who are studying for a PhD.
My main hope however, is that people who are on a PhD will find it not only helpful, but something that will help them feel a little less alone in the process. There were times, as I was doing my PhD outside of a standard academic department, that I felt really lonely, and sometimes even very lost. Not everyone has a super supportive supervisor, not everyone finds those peers that keep you going. I was lucky that I had great colleagues who picked me, not everyone has that. I hope that this book can act a little like the friend you need, who you can turn to for advice, and to know that others have been there before and found a way to succeed.
What to Expect
I don’t know what to expect to be honest. I’ve never written a book entirely alone before, with thanks to Dr Helen Rickard and Dr Sam Watkin who have contributed text. I know why I needed to write this book, and as I say in the first chapter, knowing your why is the most important thing. I don’t expect it to be perfect, nothing is, but as I say to my students, the main thing is that it is done.
The book should go live on Amazon (depending on their turn around time) on Friday 17th October. It should be purchasable in 3 forms:
Ebook for £2.99 or included in your ebook subscription if you have one and free to download
Paperback for £9.99
Hardback for £15.99
None of this is about making money for me, but Amazon have minimum costs, especially if you want it to be available widely, so there we go.
To mark the occasion, although it is terrifying me at the moment, I’m holding a small book launch event at UCL on the same night. If you fancy, come and join me. After all, we should all do a little something that scares us, and I’m hoping if I feed you wine you will forgive any deficiencies knowing the reasons why this book came into being in the first place.
If you like, I’m kinda hoping you might also tell your friends…
I am currently in the middle of secret project, which I hope to announce more about in late August/early September. I’m really excited about it but it’s taking a bunch of my time. I’m hoping that you will be just as excited when I can share more details. The wonderful Dr Claire Walker is helping me deliver my passion project by curating the Girlymicrobiologist blog for a few weeks. This means that I hope you all enjoy getting some great guest blogs from a range of topics. Girlymicrobiologist is a community, and all of the wonderful authors stepping up, sharing their thoughts and projects, to support me in mine means the world. I hope you enjoy this guest blog series. Drop me a line if you too would be interested in joining this community by writing a guest blog.
Previous mycology posts have covered how fungal mycotoxins can cause us harm, and how the new yeast on the block, C. auris, is causing problems in healthcare, but the next two posts will talk about how beneficial fungi can be in our every day lives.
The blog posts will look at how certain yeasts can be used in something that brings me a lot of joy, bread. Many of you will know I’m dairy free, and although I know I should cut down on carbs, you can take my bread from my cold dead hands. It’s one of the few things I can eat without fear and makes me happy. In celebration of this oft overlooked area of microbiology we shall be talking all things baking over the next two weeks.
The first of these posts is written by Dr Walker who is a paid up member of the Dream Team since 2013, token immunologist and occasional defector from the Immunology Mafia. Registered Clinical Scientist in Immunology with a background in genetics (PhD), microbiology and immunology (MSc), biological sciences (mBiolSci), education (PgCert) and indecisiveness (everything else). Now a Senior Lecturer in Immunology at University of Lincoln. She has previously written many great guest blogs for the Girlymicrobiologist, including Exome Sequencing and the Hunt for New Genetic Diseases.
Before I hand over to Claire though, I thought I would talk a little about baking and fermentation. About 50% of all the PhD students I speak to have dreamt at some point of throwing their research out the window, running away and starting a bakery. This may be because baking has a surprising amount of science within it when compared to some other forms of cooking, hence the need to closely align to a recipe. A lot of this is actually because you are working with yeast, a living organism, hence the fact that we are talking about this on the Girlymicro blog, as micro is just cool in so many ways
Fermentation is an anaerobic (occurs without the presence of oxygen) process where microorganisms, like bacteria and yeast, convert sugars into energy and various byproducts, like acids, gases, or alcohol. In baking, it causes yeast and bacteria to convert sugars into carbon dioxide, among other things. This is what causes the dough to rise, as well as adding flavour, and is therefore essential to all things yummy and bread related. The most commonly used yeast is Saccharomyces cerevisiae, and this is one of the reason baking can behave so variably on times of the day or seasons, as both temperature and pH can impact on how well the fermentation process works. It can also mean, if you are impatient like me, you add water at far too high a temperature and effectively kill off your yeast so it doesn’t work at all. Fermentation, and its use in food production, is one of the many examples of how microbiology and microbes impact our every day lives, and of how much poorer our lives would be without them. So I hope you’ll enjoy the next couple of blogs about how baking has both microbiological and immunological links.
Blog by Dr Claire Walker
As I’ve confessed on this blog before,I am, what I like to call, a ‘failed microbiologist’. Many moons ago I completed a master’s qualification in environmental microbiology and dreamed of a career tracking pathogens through our water systems guaranteeing safe water for all. However, I graduated during a recession and started applying for any job that would have me. As luck would have it, I ended up on the immunology clinical scientist training scheme (the story of that fateful application I will save for a later date), and the rest is history. However, I’ve always loved a bit of microbiology and my fascination with all things fermented has taken me on many adventures. Including baking afternoon tea for a GirlyMicro special event!
My treat for finishing my marking this year was a fermentation course at the Welbeck School of Artisanal food learning all about the transformation of food by microorganisms. The word fermentation comes from the Latin fervere meaning ‘to boil’ after Romans watched the bubbles forming when they fermented grapes into wine. Name a scientist who doesn’t love a bit of Latin? There are several biological processes occurring when we ferment foods like grapes, but essentially it is a process by which large chains of molecules are broken down by enzymes into their smaller, tastier, more nutritious, and more easily digestible parts.
The area of fermentation about which I am really passionate is sourdough. Yes, I lived in East London for many years, and yes, I owned a banneton before it was cool. Sourdough doesn’t just indulge my microbiology side project; it became unexpectedly personal. After picking up a particularly unpleasant microbe while travelling in India, I developed amoebic dysentery, and my gut never fully bounced back. I couldn’t tolerate shop-bought bread or much of anything, really. It wasn’t until I began incorporating fermented foods, especially sourdough, into my diet that I noticed slow but steady improvement. (Though let me be clear: this is my experience, not medical advice – if you’re unwell, definitely speak to your clinician!)
For the uninitiated, a sourdough mother, or starter, is a living culture of wild yeast and lactic acid bacteria that needs regular feeding with flour and water to stay active. As a failed microbiologist, I found something oddly fulfilling about sustaining a microbial ecosystem especially one that produces bread with real health benefits. What’s not to love about a culture that feeds you back?
Of course, I’m a dyed in the wool clinical immunologist so I can’t finish up this post without waxing lyrical about the immunology of sourdough. What makes sourdough really special, from an immunologists perspective, is how it supports our gut, which is home to about 70% of our immune cells. By encouraging a healthy mix of gut bacteria, sourdough helps produce bioactive compounds that keep our immune system balanced, strengthening our defenses without overreacting. This means it can help protect us from infections while calming down low-grade chronic inflammation that might otherwise cause problems. So, sourdough isn’t just tasty, it’s a simple, natural way to support a well-regulated immune response. Of course, sourdough isn’t for everyone, especially not for coeliacs. After all, even the most dedicated immunologist moonlighting as a microbiologist hasn’t yet figured out how to turn gluten into something completely safe. Guess some mysteries are still off the menu!
I’m so excited by this weeks guest blog post. I’m a massive murder mystery fan, and from Agatha Christie onwards there have been multiple books where mushrooms and mushroom toxins (mycotoxins) have been used, either deliberately or accidently, as a pivotal component of the plot. In recent months however, mycotoxins have been in the news in a real world sense, as the case of Erin Patterson has been heard and the jury are deliberating as I write. Erin Patterson is accused of 3 charges of murder, and one of attempted murder, linked to feeding guests a poisonous dish of Beef Wellington at a dinner party.
This led me to speak to my go to guy for mushroom (mycological) based questions. Sam is in love with all things shroom, and even has a mushroom foraging based Instagram. Who better to go to with a request to write a blog post on mycotoxins and to learn more about this intriguing topic?
Blog by Dr Sam Watkin
Hello Girlymicro blog readers! I’m Sam, a previous PhD student of Elaine’s with research focused on investigating trends in microbial dissemination in hospitals. I’m taking the blog astray from the world of IPC however with this post, and instead will focus in on one of my other interests. As people who know me have probably come to realise, I’m a big fan of mushroom foraging. There is something so rewarding to me about finding excellent edible mushrooms that you just can’t buy in shops and exploring the different flavours they can add to food. My partner had to put up with me having a Cauliflower fungus (Sparassis crispa) the size of a football in our freezer for well over a year. We would break bits off and make fantastic soups and stew bases with it – it has a really unique nutty flavour. More than just the pursuit of a free dinner though, I find it very enjoyable finding fungi that I haven’t seen before, or that are particularly rare. I imagine it is similar to the enjoyment a twitcher gets from sighting a rare bird, although mushrooms tend to stay put so there is less pressure on being constantly focussed. Having said that, searching for fungi does often devolve into a game of looking at the brown forest floor trying to spot the slightly-different-brown mushroom. More than once have I run over to a promising shade of brown or yellow, only to be disappointed by a frustratingly deceptive leaf. It is nevertheless a pursuit I thoroughly enjoy, despite the frequent soakings in rain showers and occasional run-ins with brambles.
One aspect of foraging (and indeed looking to identify fungi) is being aware of what ones you can eat and what ones are to be avoided. The old adage “All fungi are edible, some fungi are only edible once” absolutely holds true. While my professional life involves researching microbial transmission and how best to prevent infection, I am fascinated by the toxic nature of fungi. I did consider becoming a toxicologist in my teens, but rapidly realised that the amount of chemistry required was simply not my idea of joy. I do find it very interesting however how fungi are capable of producing some of the most unpleasant, and also strangest, toxins that can be found in the natural world (or at least I think so). So here I am going to run through a few of the fungi that I find most fascinating when it comes to their chemical makeup and the influence they have had on humans through history.
A fairytale classic – Amanita muscaria
Few fungi are more iconic than A. muscaria (known in English as the Fly Agaric). Their characteristic red caps and white flakes are often illustrated in children’s books and are probably what comes to mind when one pictures a ‘toadstool’. They are in every respect the archetypal fungus. This being said; however, you absolutely would not want to eat one. If someone were unfortunate enough to eat a specimen on A. muscaria, they would most likely experience a range of unpleasant neurological symptoms. Confusion, dizziness, ataxia, hallucinations, muscle twitching are often reported, as well as nausea and vomiting. In severe cases, a loss of consciousness and dangerous decreases in blood pressure can occur. These unpleasant effects are due to the makeup of alkaloids present in the fungus, with ibotenic acid and muscimol being predominantly responsible for these effects. Muscimol has a similar molecular structure to GABA-A – the most abundant inhibitory neurotransmitter in the human brain. Ingesting a chemical which mimics such an important neurotransmitter as part of your supper is unlikely to be good news. It acts as an agonist for GABA-A receptors, causing a reduction in the excitability of neurons, causing the range of neurological symptoms. Muscimol is by no means alone here however – A. muscaria also contains ibotenic acid which further acts as an agonist of a host of neurotransmitter receptors (for instance metabotropic glutamate receptors – another widespread neurotransmitter receptor class. Oh, and ibotenic acid is metabolically converted to muscimol in the body. More fun to go around!
It’s not only the alkaloid balance or popular culture appearance of A. muscaria that makes it interesting however – it has had significant historical and cultural influences. It has been traditionally consumed by shaman in northern Europe as a part of winter solstice celebrations. This is due to the intoxicating effects of consumption, where the experience was likened to flying. Part of the rituals would involve the fungi being collected while wearing ceremonial red robes. The fungi were also often fed to reindeer before ingestion to metabolise out some of the more toxic components, with the hallucinatory agents collected in the reindeer’s urine which was then consumed. I’ll pass. But, an association with winter and red robes, feelings of flying and reindeer… these rituals have indeed been credited as a potential origin of the popular imagery of Santa Claus. I guess everything must start somewhere!
An explosive pufferfish – Gyromitra esculenta
I find this to be one of the most fascinating fungi in existence. Partly fuelled by the fact that I still am yet to find this species growing wild (one day my persistence will pay off) and partly by how unique these fungi are both in shape, cultural perceptions and toxicity. Looking like mini brains, they can be found under pine trees on sandy soil in autumn (or so I’m told… maybe they are deliberately avoiding me). They are found in Europe and certain parts of North America, and are called False Morels due to their relation and similarity to the delicious Morels.
Despite being well known as a poisonous fungus their name would suggest otherwise, with “esculenta” being Latin for “edible”. And these fungi are indeed eaten in large quantities! When prepared correctly. As such, they have been likened to the pufferfish of the fungal world, which is quite the title! Appropriately prepared they are supposed to be a delicacy – I can’t speak from experience on this one, my adventures into free fungal food doesn’t quite stretch this far – however raw or improperly cooked they can be fatal. This toxicity is down to the presence of a volatile toxin called gyromitrin. When ingested, gyromitrin is metabolised to monomethyl hydrazine. This goes on to wreak havoc on a wide range of enzymes and processes, inhibiting cytochrome P450, amine oxidases and preventing the formation of pyridoxal 5-phosphate. This compound is a key cofactor in the synthesis of our old friend GABA. This causes a reduction of GABA present, preventing neuronal inhibition and causing to a prolonged excitatory state in the brain – almost the opposite of the effect seen in A. muscaria. This is still not good news however, with symptoms including severe gastrointestinal distress, kidney and liver damage and seizures and death in severe cases. Interestingly, the toxic metabolite produced here is used amongst other chemicals as a rocket propellant. I can’t but help imagine a future where we have spacecraft fuelled by fungi (albeit from a poisonous metabolite of a mycotoxin). Somehow, I doubt it.
Building up to it – Paxillus involutus
Following on from the theme of the last fungus, P. involutus is no stranger to gastronomic controversies. This very common, fairly non-descript fungus is a rather boring shade of brown (sorry if this is your favourite fungus!), although its cap does have a uniquely rolled-over rim (hence the imaginative English name – Brown Roll-Rim). It has historically been considered to be an edible mushroom, with many guidebooks simply stating that once cooked, it was safe to consume. Needless to say, these guidebooks are now firmly out of date and it is now recognised as a deadly poisonous fungus. Unlike the previous two fungi I’ve described here, this fungus does not contain any psychoactive alkaloids or toxic rocket fuel precursors. Instead, this species contains some rather unpleasant irritants which, upon consumption of raw specimens, result in severe gastroenteritis. These toxins however are degraded on heating, hence why it used to be considered edible after cooking. No, the real toxins are much more sinister in this fungus.
True to the weird nature of fungi, this species rebels against the “only edible once” saying quoted earlier. This fungus can actually be edible quite a few times before it poisons you. Unlike other toxins which you may expect to have a rapid onset after consumption (maybe a few days after ingestion at the most), the compounds responsible for the fatal poisonings attributed to P. involutus can take months to manifest. This is because the toxic effects often become apparent after repeated exposure, usually through the repeated consumption of the fungus. This is because the toxic compound here is in fact an antigen, which the body becomes sensitised to over time. Once enough meals of P. involutus have been eaten, the antigen present stimulates a rare autoimmune response where the body produces antibodies which attach to and disrupt red blood cells (autoimmune haemolytic anaemia). This causes life-threatening reductions in red blood cell counts, kidney damage and multi-organ failure. There is no antidote. If in doubt…
So, there are three of the fungi that I find most interesting in terms of their toxicity. This only scratches the surface of the wild world that is mycotoxins – there are hundreds of others. From St Anthony’s Fire (a range of medieval diseases attributed to Ergot (Claviceps purpurea) to the near-certain fatality after consumption of Amanita phalloides or Amanita virosa (named the Death Cap and Destroying Angel respectively – foreboding!), mycotoxins are truly fascinating. These show the massive variety of toxins out there and how they influence both our health but our culture and relationship with wild foods. From a foraging perspective, the range of dangerous fungi out there clearly shows the importance of only foraging with an experienced guide and only collecting what you can identify with 100% confidence. If in doubt, leave it out!
NB from Girlymicro – Whilst we’re delving into some mycological (fungal) joy over a couple of blog posts I thought I would take the opportunity to re-share this four part article series on the fungi of The Last of Us, which was a real joy to be involved with, and a clinical article that may surprise you:
This month I’ve been honouring of World DNA day 2025 by publishing a number of posts linked to what DNA is, how we look for it, and what it means to send it away.
Today I’m talking about Upgrade by Blake Crouch. In the story explored in this world, DNA based technology, although very obviously rooted in present day science, has evolved and so has the impact and access to this technology for both individuals and society. In this post I thought it might be interesting to explore ow much of this book is science, and how much of it is fiction? Before I get onto that however, here’s a reminder of the other posts that have been available in the DNA blog series:
One of the reasons I picked Upgrade for the final book review is that I thought it would be interesting, after discussing the current usage of DNA for testing and therapies in previous posts, to explore a book that covers a slightly further future, based in 2060, and what impact the use of DNA technologies could have on humanity in the future.
‘You are the next step in human evolution . . .’
What if you were capable of more?
Your concentration was better, you could multitask quicker, read faster, memorize more, sleep deeper.
For Logan Ramsay, it’s happening. He’s beginning to see the world around him, even those he loves the most, in whole new ways.
He knows that it’s not natural, that his genes have been hacked. He has been targeted for an upgrade.
Logan’s family legacy is one he has been trying to escape for decades and it has left him vulnerable to attack. But with a terrifying plan in place to replicate his upgrade throughout the world’s population, he may be the only person capable of stopping what has already been set in motion.
To win this war against humanity Logan will now have to become something other than himself . . .
In this world, DNA based technology, although very obviously rooted in present day science, has evolved and so has the impact and access to this technology for both individuals and society. It raises some interesting questions about what it means to be human. In this post I thought I would explore some of the science that is included, and what questions the use of this science brings into play.
Are visions of a world where DNA controls our lives unique?
Before I get into the science of the book however, I wanted to flag that visions of a world where the use of DNA testing, evaluation or modification, are not new. GATTACA (did you see what they did there……they are all DNA bases) have been around since the 90’s, when the technology we use clinically now was only in its infancy. Fear of how science could be used in the future is a pretty constant feature of this type of creative content, as it provides a safe way to explore these fears and ethical challenges. I suppose what I’m saying is that just because something is included in these kinds of visioning pieces does not make it bad, wrong or scary. It just means that we also need to think and reflect on what checks and balances are included as part of their introduction in order to make sure the world we create and influence based upon them is the one that we are aiming for, and we have taken steps that include the law of unexpected consequences rather than ignoring it. DNA editing is an amazing, technically complex and powerful tool that has the potential to be positively life changing, so please keep that in mind when you read the rest of this post.
The world of upgrade
In the world of Upgrade the impacts of climate change have really been felt. Entire cities have been flooded as the seas rise and access to food has become a real issue for vast portions of the worlds population. Logan, our protagonist is the son of a genius, a woman changing the face of science. Being the child of a world famous geneticist makes Logan feel the reality of being a normal person surrounding by an extraordinary vision.
I had extraordinary dreams but had been gifted only an ordinary mind
Sadly, as is often the case in these tales, his mothers (Miriam Ramsay) drive for change comes with a fair amount of hubris. In an attempt to address the food shortages Miriam, with Logan supporting as a junior scientist, develops a new gene editing tool called Scythe in an attempt to genetically enhance rice crops. The process goes wrong, and results in The Great Starvation that leads to the deaths of 200 million people.
As a result of the mass deaths, genetic manipulation using Scythe or related tools originating from CRISPR, are outlawed and their use results in a mandatory 30 year minimum jail term. Thus making the field of genetics either outlawed or suspect, and to the birth of the Gene Protection Agency, a police force which aims to track down those undertaking illegal manipulations or research.
Logan ends up going to prison for his work with his mother’s research, and his mother commits suicide. After serving his time Logan is released and joins the very agency that has been set up to prevent a repeat of the genetic manipulation that changed the world. At the start of the book Logan is investigating a scene where an explosion happens, his body is hit by shards of ice, and his life changes again…..forever.
My mother had tried to edit a few rice paddies and ended up killing two hundred million people. What havoc could she wreak—intentionally or through unintended consequences—by attempting to change something as fundamental as how Homo sapiens think?
So, what is gene editing?
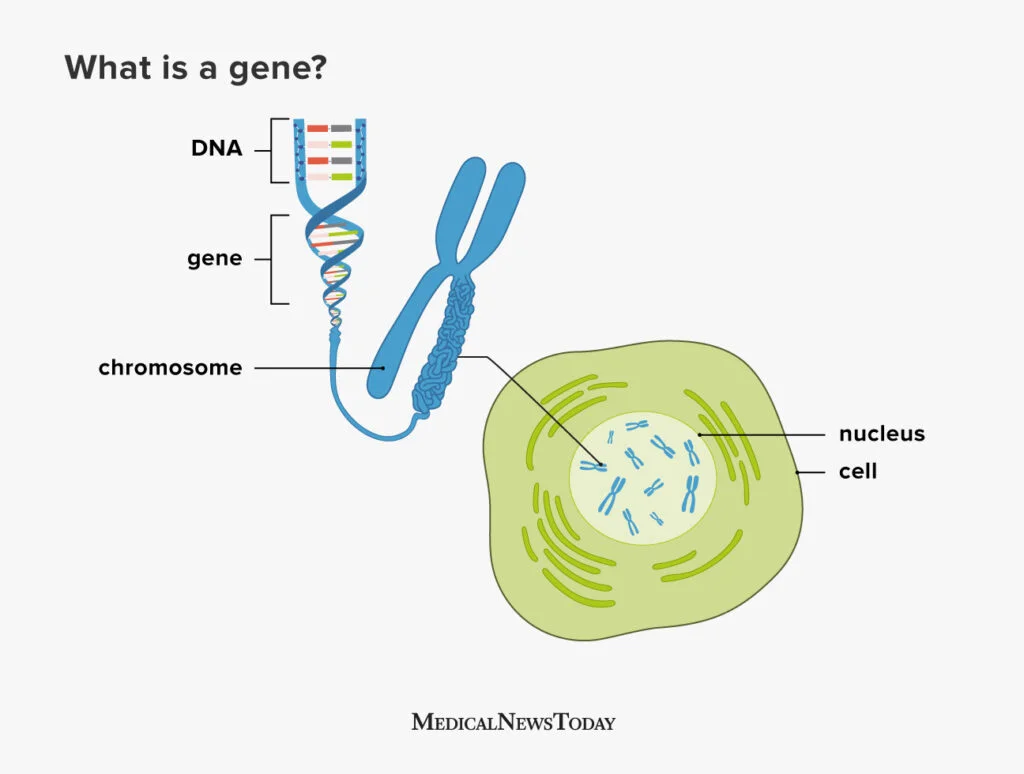
I’ve already mentioned CRISPR but I’ve not described what it or gene editing actually are. Gene editing as defined by the World Health Organisation is:
A method for making specific changes to the DNA of a cell or organism. It can be used to add, remove or alter DNA in the genome. Human genome editing technologies can be used on somatic cells (non-heritable), germline cells (not for reproduction) and germline cells (for reproduction).
Before I go further I should probably talk about how CRISPR works and what it is used for. Tools like CRISPR/Cas9 are tools for gene editing, and are the present day origins behind the futuristic tools present in Upgrade. Emmanuelle Charpentier and Jennifer Doudna were awarded the Nobel Prize in Chemistry in 2020 for the development of CRISPR, commonly referred to as genetic scissors.
CRISPR allows you to design a targeted way of manipulating a gene section that you are interested in, and in some cases then replace it with an alternative gene section, which enables the gene to function in a different way. Being able to target and replace, or inactivate genes, in this way opens up a whole new world of possibilities, from health to industrial applications. There are three main approaches to gene manipulation:
Replacing a disease-causing gene with a healthy copy of the gene
Inactivating a disease-causing gene that is not functioning properly
Introducing a new or modified gene into the body to help treat a disease
Now, wearing my geek credentials on my sleeve, I wanted to share with you a music video that describes how CRISPR works. It’s set to the music of ‘Mr Sandman, bring me a dream’ and is retitled ‘CRISPR/Cas9 bring me a gene’. I love this as it I think it describes the history of the process really well. I will tell you now though, that when I made Mr Girlymicro watch this for the 5th time he could not get out the room fast enough, so this may just be a me thing.
Where is the science rooted in the present?
Having talked about the fact that gene editing isn’t the work of science fiction, I thought it would be useful to talk about how and where it is actually being used right now.
According to the Federal Drug Administration there are a variety of types of gene therapy products, i.e. products that manipulate genes, currently available:
Plasmid DNA: Circular DNA molecules can be genetically engineered to carry therapeutic genes into human cells.
Viral vectors: Viruses have a natural ability to deliver genetic material into cells, and therefore some gene therapy products are derived from viruses. Once viruses have been modified to remove their ability to cause infectious disease, these modified viruses can be used as vectors (vehicles) to carry therapeutic genes into human cells.
Bacterial vectors: Bacteria can be modified to prevent them from causing infectious disease and then used as vectors (vehicles) to carry therapeutic genes into human tissues.
Human gene editing technology: The goals of gene editing are to disrupt harmful genes or to repair mutated genes.
Patient-derived cellular gene therapy products: Cells are removed from the patient, genetically modified (often using a viral vector) and then returned to the patient.
There are a number of ways that gene therapy products are already being used for the clinical management of patients, including for patients with conditions such as HIV and sickle-cell disease. One big change that has occured during my clinical career is the use of CAR-T cell therapy for tackling some types of cancer. CAR-T cell therapy is a type of immunotherapy where a patients own T cells (type of white blood cell) are taken from a patient who has cancer, and the cells are then modified in order to better recognise and attack cancer cells within the patients body when they are then given back. So gene editing is already saving lives and in every day use, even if its roll out is currently limited.
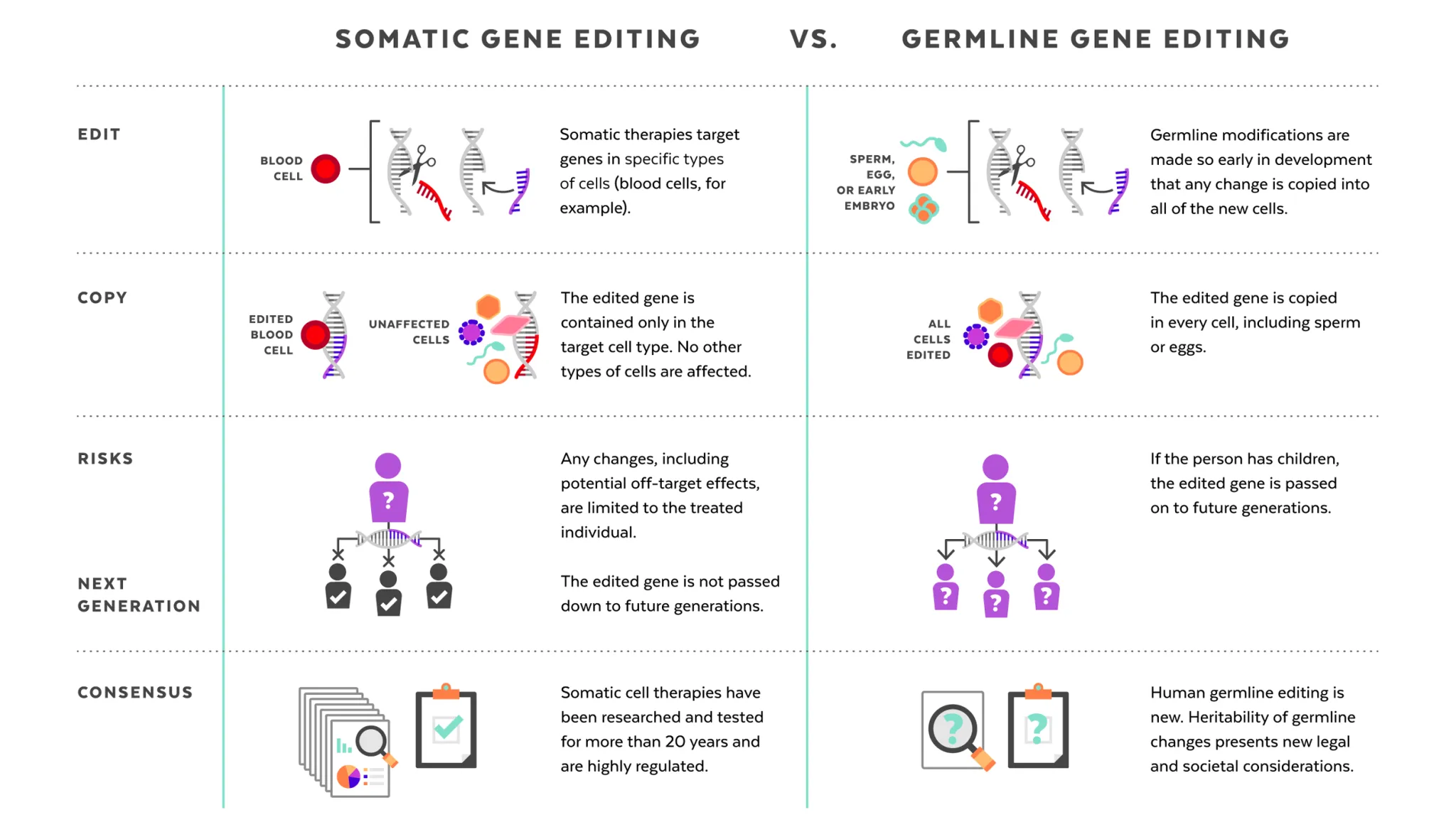
Having established that gene editing is very much the next frontier for expansion in healthcare, it’s probably important to consider how stable these changes will be within the wider the gene pool. It’s worth noting that the human genome editing techniques that are being introduced in healthcare are linked to somatic cells, where changes would be non-heritable, rather than within germline cells, which are involved in reproduction, where any changes would be inherited by future generations. Most of the changes that are currently being targeted for gene therapy would not therefore cause the changes to be established within the gene pool. There is a question about whether the target genes, even for somatic changes, may become more established as some of those carrying them may not have previously survived to reproductive age, but to be honest this feels like the impact will be minimal and a price worth paying as a society for improving both quality and length of life in those impacted. Changing future generations of children is however a whole different ball game.
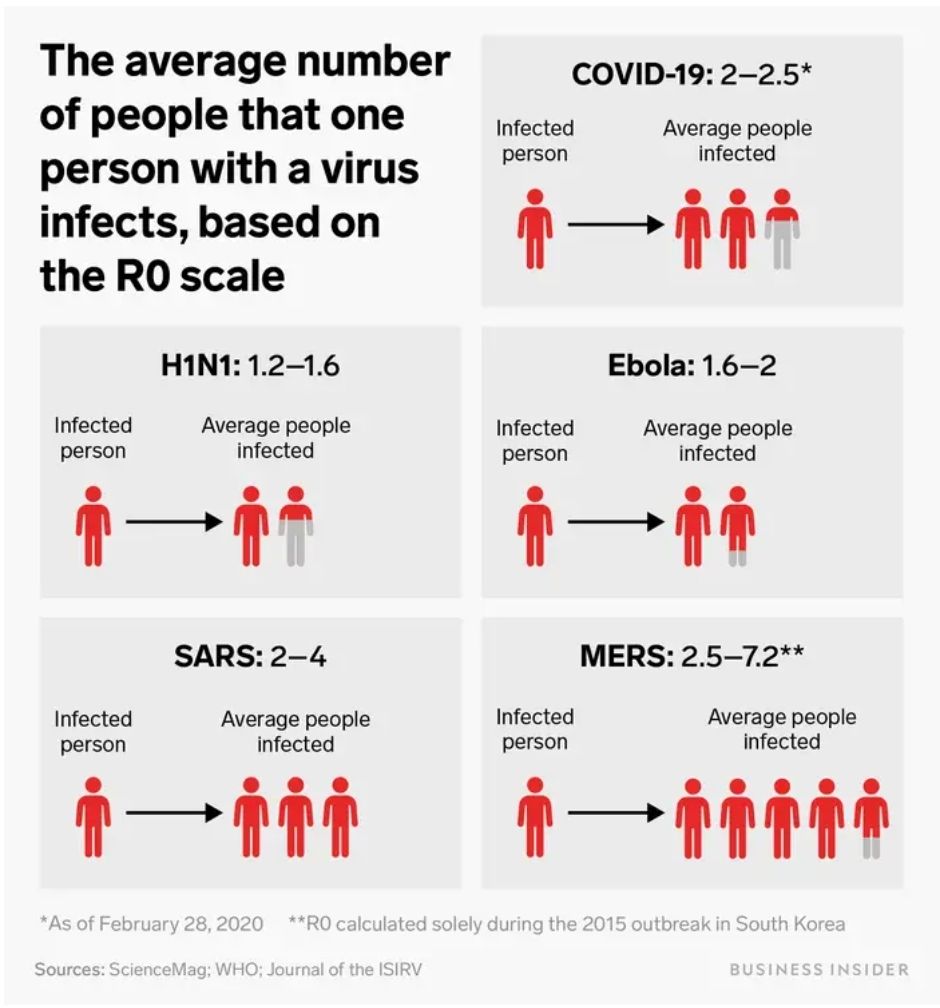
The technology discussed within Upgrade has moved on somewhat from CRISPR. It retains some features of current technology however, as the delivery of Scythe is via viral vector. The interesting thing about this form of delivery is that, in the world of Upgrade, the viruses have been modified and use their standard invasion routes to deliver the genetic material into cells, but, unlike the way that this is being undertaken as part of gene therapy in current healthcare, the viruses do not appear to have been fully modified to remove their ability to cause infectious disease. Some of the plot, therefore, is driven by the fact that it is possible to undertake wide spread indiscriminate gene editing within the human population. The modified viral cells retain their transmissibility alongside their gene editing functionality, and so a gene manipulation can spread in a similar way to any respiratory viral infection. The R0 within Upgrade is 8, which means that every person infected will infect, on average, 8 other people, which means the potential for spread within the population is massive. (If you want to know more about what an R0 is, I’ve covered it in a previous post here). It is not clear to me whether the gene targets within Upgrade are targeting just somatic changes, or a combination of somatic and germ line, but when you can spread so widely so quickly that is probably not the main consideration.
What questions does Upgrade raise?
Within the world of Upgrade, the gene editing doesn’t just target a single gene, but a whole suite of different genes for large scale changed. The problem with using gene manipulation that changes multiple gene targets, that are non-personalised to the condition/individual, and are highly transmissible, is that it is highly likely that the changes won’t work for everyone’s genome. There are going to be side effects or potentially significant impacts. Within Upgrade these are seen through errors that then occur in the brain due to protein mis-folding, very similar to how prion diseases work. The change in some people is catastrophic and there is no intervention available to reverse it. Using indiscriminate gene manipulation has the power to create mass disruption and change societies. It is this power for change that is the jeopardy that drives the novel. Is the cost worth the outcome, and who gets to decide? How much collateral damage would we be prepared to accept, even if the wider benefit to society is a positive one?
Prion diseases: A rare group of neurodegenerative disorders October 2022 In book: Viral, Parasitic, Bacterial, and Fungal Infections Antimicrobial, Host Defense, and Therapeutic Strategies (pp.651-662) Edition:1 Chapter: 53 Publisher: Elsevier: Academic Press
What does it mean to be human?
As part of this risk/benefit consideration, Upgrade asks a lot of questions of the reader, the main one of which, for me, is what does it actually mean to be human?
There is a genetic definition of what it means to be human, but the gene modifications within humans causes our protagonist Logan to ask some very valid questions about what it actually means to be human. Is it just about genetics? How much can we change not only our genes, but our outlook/perceptions, as people and still remain human?
The ‘upgrades’ received cause different characters in the book to judge humanity in general, and other human beings, in very different ways. Do genetic changes make you superior? Does being intellectually smarter permit you to make decisions for others for their benefit, as determined by the smarter individual? In many ways this brought to mind, for me, the old approach to clinical decision making, which was very paternalistic and the role of the person/people impacted was highly passive. I’d like to think we are now moving towards a much more patient focus decision making process, but this book made me think about what would happen if this model was used, not just for one to one interactions, but for the future of humanity.
The question about decision making is an interesting one however. There is plenty of data that demonstrates improved decision making in small groups, and if time is of the essence how would you engage with enough people for a decision to be valid? Especially a global decision? How many people would you need to interact with for a choice about changing the DNA of your species to be valid? How would you manage a lack of consensus? Would you let the world burn whilst the choice was being made, or would you accept that at some point someone would need to step in and lead the way forward? It’s the uncomfortable space between ethics and pragmatism, and definitely not something that is easy to answer, even conceptually.
Is intelligence the problem?
As discussed above, a lot of the plot driven by the counter to our protagonist in Upgrade, is based on the concept that if humans were smarter they would make better decisions. Therefore, by improving how people think and removing some of the emotional component the human race would be improved and therefore ‘saved’. This is especially important in the world of Upgrade, as because of the damage that is being done linked to climate change and other damage caused by humanity, the clock is ticking and Logan is very aware in his upgraded state that there is only 100 years left to save mankind.
The problem, as it plays out to me, is that it is very much not about intellect however, it’s about the ability of individual humans to care enough for others. For one person to make decisions that costs them rather than benefits them for the sake of someone that they do not know well if at all. This is especially true for problems that are going to impact future generations, like climate change, where the people most impacted have yet to be born. By the time we ‘meet’ those who will be most affected it will be too late to save them. Even for a present day context it raises questions, we all think of ourselves as having empathy and caring for others, so why does that not play out and allow us to care for the migrants that are dying trying to join us and share in our safety? Why is our compassion so limited?
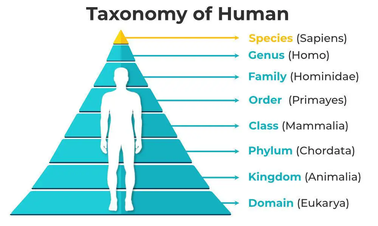
One of the reasons for this has nothing to do with intellect, and would in no way be altered no matter how smart we become. It’s based on a theory known as the Dunbar number, which predicts that we can only empathise with a maximum number of 150 people, the number of people that would likely to have been the maximum size of our primate tribe. More than this, we can only truly care, to the point we may want to sacrifice, about a much smaller number of people. The book therefore postulates that we aren’t held back due to a lack of intelligence or innovation, we’re held back by a lack of compassion and the ability to truly care about people we don’t know and will never meet. If we are to change anything about ourselves in order to save mankind therefore, it’s not intellect we need more of, we need to find a way to increase our capacity for compassion and therefore change our Dunbar number, to adapt for the world we now find ourselves in. So maybe the answer to the problem is to become more ‘human’ rather than less.
Where do all of these questions leave today’s gene editing technology?
Gene editing technologies are making massive strides, saving lives, and positively helping people who have serious health conditions.
Somatic gene editing is well established, and has been developed over the last 20 years so that regulation is in place, and it being more and more routine rolled out in countries that have access to advanced scientific technologies. The problem is just that however, these interventions are technologically challenging and incredibly expensive, and therefore not universally available. This means that they also do not necessarily take into account the diversity of the human genetic population or the lived experience within different cultural communities. Regulation is also not present universally, with some people forced to access these therapies through the use of rogue clinics, or by undertaking medical tourism, which brings with it increased risk. There is also the potential for illegal, unregistered, unethical or unsafe research and other activities, including the offer of unproven so-called therapeutic interventions, as with any emergent technologies. Ensuring equity of access and appropriate regulation will be essential to ensure a safe global adoption of these therapies.
Germline gene editing is however in a very different place, as this would lead to the editing of DNA in a way that may be heritable across generations. There is an intense debate linked to its use as the the future generations that would be impacted would have no capacity to consent to the changes, and or risks, that are being made. There could be possible risks and consequences for offspring and for society in general, and once that genie is released it will not be possible to put it back in the bottle. Discussing what circumstances it would ever be appropriate to undertake these changes requires us all to be actively engaged in these discussions.
I hope you’ve enjoyed these series of blogs linked World DNA Day and taken some to celebrate the miraculous nature of just being you. I’ve really enjoying sharing some of the technical information, but also diving into some fictional worlds and discussing the thoughts that they provoke. With summer coming up I hope you may even pick up a copy of these great novels and dive into their worlds yourself. If you find any others in your reading adventures, return the favour and let me know. I may even include them in a future review. Happy reading.
This month I’ve been honouring World DNA day 2025 by publishing a number of posts linked to what DNA is, how we look for it, and what it means to send it away.
Having spent some time covering what is the current state of science in this area however, I thought I would follow up with a couple of book reviews whose fictional worlds focus on how the world of DNA, DNA editing and DNA interpretation could change the lives of everyone involved. The first of these is The One by John Marrs.
This book is set in the near future in a world very much like ours. It’s nice for me to review a book that is set in London, where I can also do a bit of location tourism and spot similarities between this fictional london and the London in which I live. The tech and the science in this book are very much just one step further open than some of the modern day science I covered, especially in part 2 of this blog collection. All this being said, this book is also a thriller and so not necessarily like life as we know it.
How far would you go to find The One?
A simple DNA test is all it takes. Just a quick mouth swab and soon you’ll be matched with your perfect partner–the one you’re genetically made for.
That’s the promise made by Match Your DNA. A decade ago, the company announced that they had found the gene that pairs each of us with our soul mate. Since then, millions of people around the world have been matched. But the discovery has its downsides: test results have led to the breakup of countless relationships and upended the traditional ideas of dating, romance and love.
Now five very different people have received the notification that they’ve been “Matched.” They’re each about to meet their one true love. But “happily ever after” isn’t guaranteed for everyone. Because even soul mates have secrets. And some are more shocking than others…
The One is set in a world where, instead of just sending off your DNA to find relatives or health characteristics, there has been a gene discovered that can be used to link you up to your one true biological match. The person you are supposed to fall in love with. This is because the discovered variant of this gene causes physiological changes and the production of a pheromone that is unique to you, and which is particularly attractive to (statistically) one other person, who has a complimentary version of this gene. Production of the pheromone means that when you encounter each other you immediately physiologically react, and experience a biological ‘love’ match. Within the setting of the novel, a company called Match You DNA, has been marketing a product where you send a swab and can be matched with the person you are genetically made for. Sending away for matching has become common, with over 1 million matches, but is neither universally undertaken or universally accepted as a good thing. The book starts with a number of characters taking their DNA tests, for various reasons, in the hopes of being matched with their soul mate. Five couples are then matched and the novel follows them through their matching journeys.
MatchYourDNA.com thanks you for choosing Match Your DNA the world 1st scientifically proven test 100% guaranteed to match you with the one and only person you are genetically designed to fall in love with. With 1.7 million people either matched or are already on our register, your perfect match is only 3 steps away:
1) Sign up here for free
2) Receive your free DNA test kit. Just send us the mouth swab in the provided container and we’ll use your DNA to find your match in our database
3) As soon as we’ve found your match we’ll contact you. For a one off fee of $9.99 we’ll put you in touch with each other. 82% of customers are matched within 7 days. If you don’t currently have a match do not worry. Thousands of new customers join match your DNA each week and 98% of matches are identified with 6 months of registering
Match Your DNA cannot be held responsible for any direct, indirect or consequential harm related to using this service including but no limited to dissolution of existing relationships, personal injury or death not resulting from.match your DNA negligence or misconduct
What about the science?
The world of The One includes science and technical details that bring up a heap of both scientific and ethical questions that I think are really important for us to think about, whether we work in science or not. Science impacts all aspects of our everyday lives, and so the more we know and think about how it impacts us, the better prepared we will be, both as individuals and as a wider society. I really enjoyed exploring this world and so wanted to share what questions the setting triggered for me, and how it relates to the world in which we currently live. If you have already read/listened to the book, or if this blog prompts you to do so, I would love to hear what it triggered for you.
How much can anyone own a gene?
The founding premise of the world building in The One is that a single company would have sole access to this form of specific DNA matching technology, I posit via some form of patent for the gene, although this isn’t really discussed. A gene patent is the exclusive rights to a specific sequence of DNA (a gene) given by a government to the individual, organization, or corporation who claims to have first identified the gene.
So can someone own a gene? It may surprise you that the answer is both yes and no. A company can patent specific DNA sequences, such as DNA sequences that have been manipulated and altered in a lab, making them different from naturally occurring DNA. This wouldn’t help in the case of The One, as the company cannot patent naturally occurring genes, such as the genes they would need to target, as they exist already in the human body. However, patents can, and have been granted, for specific uses of genes, such as diagnostic tests or therapies, even if the gene itself is not patentable. This has happened for diagnostic tests including those for the BRCA1 and BRCA2 genes, which are linked to hereditary breast and ovarian cancer, and for the area of the Staphylococcus aureus genome where the SCCmec gene cassette inserts, leading to S. aureus displaying resistance to methicillin (MRSA). It is therefore possible that a single company would be able to corner the market, for a period of time, and be the sole provider of this kind of service, and therefore have the kind of societal influence demonstrated within the novel.
Can there really only be one true gene match?
This book is very much based on an advancement of the kind of DNA sequencing that people can currently use to check on their ancestry and relatedness, as discussed in parts one and two of this blog series. How realistic is it that there is only one copy of a gene variant in the world for each of us however?
While the human genome is highly similar across individuals (99.8-99.9%), small differences do exist, totaling 3 – 5 million variations, some of which can have profound impacts. Studies like the All of Us Study, funded by the National Institutes of Health, have discovered over 275 million previously unreported genetic variants, showcasing the immense diversity within human genomes. Whether this variation would be localised to a specific gene with each variant being present at just the right kind of frequency that there would only one person in the world for us is yet to be mathematically modelled 🙂
It is also unclear exactly how the translation of this gene variation into physical expression via pheromones, which are chemical messengers that can influence attraction, would work. The extent of their impact would need to be the topic of further research. Pheromones are known to play a crucial role in mate selection and social behavior in many animals, but the evidence for their direct influence on human attraction is less conclusive. So this bit of the world building that is inspired by science, but definitely science fiction at this point.
How does nature vs nurture work?
The nature vs. nurture debate explores how much of an individual’s characteristics are determined by genetics (nature) versus environmental factors and life experiences (nurture)
At it’s very core, much of The One is about whether nature always trumps nurture. Are we slaves to our genes? Is the development of a loving relationship with someone who is not your genetic match, developed over years, always going to be trumped by a brief encounter driven by genetics?
One of the big dilemmas that some of the couples face, and a central theme discussed in the book, links to this debate and examines how the revelation of being matched impacts on characters pre-existing, as well as their new relationships. What if those who were already married and in happy relationships from before the existence of matching, decide to swab themselves and are not in fact each others matches? What if you run into your match as part of your normal life but are already dating, is cheating then OK? Are those with relationships that have not been validated by Match Your DNA of less value, both to individuals and society, than those that are biologically prescribed? Does nature automatically trump nurture?
If you start to extrapolate even further than this, does it mean if you can’t find a match that you default into being considered a second class citizen? A short step on from that, could you be compelled to take part in matching even if you don’t want to? These are some of the future possibilities hinted at during The One. Although these conundrums are very much science fiction, they are definitely rooted in other types of discussions that are happening even now, such as whether we should sequence the genome of every baby at birth in order to provide better preventative healthcare? In fact, it is a threat that is developed in another novel within the same world, called The Marriage Act, which points a lens at the role of government in handling these issues and how once individual decisions can suddenly be adopted by society as embedded behaviours, resulting in the loss of individual freedom to decide.
One of the other interesting threads, for me, is the question of is it OK to breach other societal norms because of a DNA match? Should an 18 year old (minimum age for matching) suddenly feel like they need to date a 90 year old? Should you leave behind all of your connections and stability to fly across the globe to be with someone you don’t know on the basis of a single gene? If your match dies, does that mean you will never find another true love?
On a wider societal scale the book triggered a number of other considerations for me. Such as, what would be the consequence of people no longer going through the dating process and leaping straight to a formulated relationship? Would it impact social skill and other development? What opportunities would we take away from people to learn about others, but also to learn lessons about themselves? How can impacts that appear to be at the individual level completely change the way society as a whole begins to function?
What about giving up on self determination?
Building on the above, one of the very interesting themes for me is what happens if the person you are matched with is just not a very nice person? Does you biological compunction overwhelm your personal choice? In other words, if nature trumps nurture, what happens to self determination?
Self determination theory includes three key components. The first is that of competence, where people need to gain the skills to control their lives. Second is autonomy, where people need to feel they have control over their choices, and finally, relatedness, where people need to feel connection and belonging.
The One raises interesting questions about which of these drivers may be the strongest. Finding your DNA Match leads to intense feelings of belonging and enhances feelings of security, as you’ve found your One, and it is not supposed to be reversible. It removes doubt, but does it also remove effort? Relatedness is definitely enhanced by the concepts of gene matching. However, the concept of DNA matching also directly reduces any sense of autonomy, as you are seeding control of a key relationship to your genetics, which you have no control over at all. The sense in the book is that this causes an understandable level of conflict and cognitive dissonance* that runs within all of the characters present.
*the psychological discomfort experienced when we hold two or more conflicting beliefs, attitudes, or values simultaneously
Another question that struck me linked to this is….which biological compunctions are the strongest? The bond with a child or the instinct to reproduce are both strong biological imperatives, so if these are placed up against a link with a DNA match, which would win out? For instance, would you walk away from your child and never see them again for the love of your life? Having spent a while pondering it, my thoughts on this are that these discussions are not as binary as I have perhaps presented them and that everything is likely to be combination of nature and nurture, and it is how these unique combinations come together that drive us and make each of us even more unique than we are on a genetic level. Still, I am intrigued about whether there would be a hierarchical determinant to some of these drivers, that is if they were all real.
What about informed consent?
Not to spoil the story but there seems to be a strong temptation for people in the world of The One to not only send swabs from people other than themselves, but to also access the results of other people and therefore control access to information that doesn’t belong to them. Now, I’ve already covered in part two why taking the DNA from other people for testing could have legal consequences, but why else could it be considered wrong?
I thought it might be important here to talk about the importance of informed consent, and why some of the consent gained could perhaps not be considered to be truly informed.
Informed consent has a number of key components to it, but some of the big ones are linked to open disclosure of both the benefits and risks of any test/procedure, alongside discussion of whether there are any alternative options, so that the person deciding whether to go ahead is making that decision with access to all of the best information, i.e. the decision is informed.
Now, obviously how much informed consent is needed does vary widely depending on what is being undertaken. As I said in part two, most of the common DNA tests to send away are not considered medical tests and are not therefore subject to these kinds of gate keeping. If the world changed so that this form of testing had such impacts on lives, then should that be reconsidered so individuals truly knew what they were signing up to? Would just ticking a box on an Internet form really provide sufficient levels of understanding that the consent could be considered informed?
There are also interesting questions raised in the book about the consent linked to use of data. Is it acceptable to collect data for one thing and then use it to develop a test that wasn’t part of the acceptable use criteria for that data? Is it OK to gather a whole heap of human genomes and then utilise them for research purposes if that wasn’t part of the consent for which they were collected? Is it OK as long as it is all anonymised? All of these things depend upon the type of consent that is given.
In part two I talked about the data that is being collected for current DNA testing for non-medical testing and that the resulting sewuences are likely to be used for other purposes, and that use is probably included in the terms and conditions you sign when you send off for testing. How obvious this is will probably vary between companies. As these are non-medical devices though, the consent is unlikely to need to be informed. Most people think about the swab, but not the DNA sequence that results. If you are making an entire business based on those sequences, such as in this book however, you probably need to be certain that their use is legitimate, and covered within the purpose for which they were collected. #nospoilers
Is a single company having so much power dangerous?
In a previous book review I wrote about the Theranos scandal and the impact of a single company with massive influence who didn’t follow good scientific practice had on the lives of the people they tested. Obviously the Theranos scandal is real life, real people were hurt, and real people went to prison. The One on the other hand is a work of fiction, and a space where some of these more ethical concerns about the impacts of scientific developments on the the life of people can be somewhat more safely explored. It does call into focus whether one company should have so much capacity to influence the lives of so many. It made me think, if this were to happen right now what kind of oversight would be required? How could lobbying and other practices mean that some of the neutrality of that oversight could be impacted? Also, how much oversight would be appropriate? How do we ensure quality without negatively impacting innovation? How do we allow the good whilst minimising the bad? This is something science is constantly struggling with and there are no easy answers, but the capacity for harm if you get it wrong should be something that all scientists should live with and actively reflect on.
Hopefully this blog, and going on to read the book, will help us all to take some time to think about some of the ethical considerations that this fictional world raises, and encourage us all to think a bit more about our own and societies role in DNA testing moving forward.
One last note, if you prefer your content as visual media, The One has also been made into a TV series which is currently on Netflix. Full disclosure, I’ve only seen a couple of episodes. The feel of the series seems pretty similar to the book but the actual plot lines seem to have been changed quite a lot. Pro of this is that you can quite happily enjoy both as the series gives new aspects to new enjoy. However you decide to explore it I would definitely recommend a dive into this world and enjoying the surprises that it brings and the thoughts that it provokes.
Friday just gone, 25th April, was World DNA Day. I’ve had a series of blogs that I’ve been playing around with linked to both DNA in our everyday lives and two book reviews where the world changes because of genetic testing and genetic manipulation. I thought I would write these posts, because as much as artificial intelligence could change the way we live and is frequently discussed, we are all accessing DNA based testing more and more, with many of us not really thinking about how this too is changing the world in which we live. Depending on how you feel about science and needing to have a refresher on what DNA and how we look for it and interpret it, you may want to hit up part one of this blog series first.
In part one I also introduced the kind of testing that DNA and DNA sequencing can be utilised for, not just in a accredited healthcare laboratories, but also linked to private companies who offer information on things like ancestry. In today’s blog I wanted to go a bit more into what can be the less thought about results of sending away your DNA, and also what kinds of things you might want to think about, or have in place, before you do.
Thinking unexpected consequences?
In part one I used this quote from a recent article:
As stated in a recent Independent article:
As they’re based on estimates, I suggest treating home DNA tests as a fun investigation to get to know your family history a little better rather than a to-the-letter representation of everything that’s ever happened in your gene pool – Ella Duggan Friday 28 March 2025
It describes sending away of your DNA as a fun investigation, and recommends not taking the results too seriously. This is definitely the right attitude in many ways, as you wouldn’t take key health guidance from a magazine quiz, you’d want to speak to a healthcare professional who can put your results in context. The problem with not taking the tests themselves too seriously is that we don’t really think about the consequences of taking them or where the results might lead. My family have been given these for Christmas, for instance, and it was seen as a fun piece of science that could be done after lunch. Taking and sending away your DNA, the thing that makes you you, however, should always be done with a little more consideration that that. So I thought it might be useful to use just a couple of examples of why.
Health services
Sending away DNA for health reasons to private companies has been controversial ever since it was introduced into the UK and there are a few reasons why this is the case.
Firstly, if you have health concerns, then really you should be accessing medical care through healthcare professionals who you’ll be able questions, and who can put your results into a risk context for you based on your own medical history, rather than just getting a list of genes in isolation.
One of the other reasons you should manage this form of testing through health providers is that you can then be linked into any medication or further testing that is required. The presence of a gene alone can be pretty meaningless, you need to then look for whether that gene is being expressed (see part one) in order to really understand it’s impact, and so there are likely to be follow up requirements to any results received.
If you are going through genetic testing, especially if it has impacts on decision such as reproduction, you would normally be supported through the process ahead of the testing, and when the testing is returned, through professionals such as genetic councillors. If you get your results by sending your DNA away you may get completely shocked and surprised by the results that you can get back, and may make some decisions based on the findings that may not be correct for you and require better input from someone more used to interpreting the results. It could feel like a really lonely way to hear bad news.
Finally, these tests are being sent off to laboratories that don’t require accreditation. They are acting as medical tests, without going through the rigor that is required for the equivalent tests in healthcare, and yet are interpreted, by some, in the same way, and therefore effectively out of context. They may also not have the required levels of validation linked to the information and interpretive guidance that is issued with a result, so that you know what being present or absent for gene X or Y actually means for you. It also means that there may be less processes in place to ensure that you get the result that is actually meant for you and not for Professor X down the road. If you are processing hundreds of samples this kind of error, without safety checks, can be easier than you’d think. Knowing the quality of the result you are receiving may be less than obvious.
Ancestry services
OK, OK, I can hear you say. I wouldn’t send my DNA off for medical testing, but surely sending it off for ancestry services is ‘no harm, no foul’ and just a bit of fun. My first caveat here is that not all ancestry services are the same and not all of them look at the same sections of your genome. Some will look at your mitochondrial DNA (which will always come from your mother and your maternal line) in order to give a view of where your ancestral DNA comes from over generations. This is often referred to ancestral origins, and is much less likely to hit you with real time life dilemmas. Many kits are also paired with items that look at wider genomic matches, or DNA matches, and so you may get back more than you bargained for if you didn’t look closely at what was going to be provided.
I’ve included just a couple of, extreme, examples of how these kinds of unexpected consequences can play out in real life. The first is a BBC News story that came about because a woman was contacted by a stranger after sending off her DNA via an ancestry site. From the results it eventually became apparent that she had been accidentally swapped as a baby in a hospital in her 50’s with another child. Thus having dramatic and rather unexpected consequences for her and her family.
The other example I’ve included links to a couple of documentaries where the use of DNA matching platforms has uncovered serious misdemeanors or crimes, including IVF undertaken using the sperm of medical professionals without the knowledge or consent of the parents involved, and sperm donors being involved in the insemination of more couples than disclosed, thus increasing the risk of their children potentially interacting/dating/mating in later life without knowledge of their genetic linkage. This is obviously not the fault of the DNA matching service, and is something that is beneficial to uncover and stop, but has hugely dramatic impacts on those involved without any prior warning or support in place. It certainly wasn’t what they expected when they sent away their swab.
Is it just human DNA that counts?
Finally, to follow up on the takes of the unexpected, and because infections are fascinating, I wanted to share a link to a video that I think is really great about the first time DNA testing of HIV was actually used to convict someone of a crime. This one isn’t a word of warning, as I suspect that none of us are going to decide to deliberately inject someone with HIV contaminated blood, but I wanted to end this section with something where the use of DNA testing in the hands of people who really know what they are doing is a powerful tool for good. Also, because I wanted to give a non-human example of where I think some of this may go in the future.
What do we need to know before we start to send our DNA away?
Having laid out my warning stall, I wanted to go through some things I think you should actively think about before sending your DNA away.
What is the legal situation?
First and foremost, the sending of DNA away for processing is covered under something called the Human Tissue Act or HTA (in England). I’m flagging this as the first thing as, unlike what you see on TV, you should not be taking DNA from other people and sending it off to see what it says, and especially not for any form of DNA match testing. In the UK, if you do take anyone’s DNA sample without them being aware of it, it is considered a violation and you are liable to prosecution which can result in up to 3 years imprisonment. It is not OK to steal someone else’s DNA without their consent! There’s a lot to this one and I’m not a legal expert, but it seems to be something that many people are not aware of and now you know.
What level of information will be gathered?
All of the different tests offered will do things, and companies interpret the results slightly differently. It’s incredibly important to know what you are sending your DNA away to be tested for, how it will be tested and what kind of information you can expect back.
The main types of DNA tests and the areas they analyse are:
Autosomal DNA Tests = examine the 22 pairs of autosomes and the X chromosome. Commonly used for ancestry testing and can help determine ethnic origins, identify genetic predispositions, and find relatives. Utilise single nucleotide polymorphisms (SNPs), which are variations in a single DNA base pair
Y-DNA Tests = analyze the Y chromosome, which is passed down from father to son. Used for tracing paternal lineage and can be helpful in genealogical research
Mitochondrial DNA (mtDNA) Tests = use mitochondrial DNA, which is inherited maternally (from your mother) used for tracing maternal lineage and can be helpful in genealogical research
Paternity Tests = examines specific regions (loci) on the chromosomes to look at parental relationships
Health-Related Genetic Tests = looks for specific genes or regions of the genome that are associated with certain health conditions to try to identify genetic risks, diagnose genetic disorders, or assess treatment options
You may need to read the small print to really understand how the testing will be undertaken and to manage your expectations. If you can, make sure you look up examples of what the results you will receive will look like, and if there would be any follow up support given. Also, crucially see if there will be additional funding required to get access to the full data set you are expecting so you don’t get hit by any unexpected requirements.
How will data be used?
The next few sections are all linked to what happens to the results of your testing that you are sending away.
The first thing to check before you send off your test is how long will your data be stored for once. This is important for you in terms of being able to access reports, but also about how long your legacy data will be available. Will you have access to wider information if you request it to be passed to your healthcare provider? Is there any information on the data analysis tools used? Are you even allowed to ask questions or is all patented and under intellectual property rules, which is reasonable but you should know what the boundaries are. Most healthcare reports should be kept for at least 10 years, but as these are covered under different guidance, will you only have access to download your data for a set period of time? Will it be possible to get your own local back up of your data? Once you know the answers to these questions you can then make active choices and comparisons about which aspects are important for you.
The article below is a little old, as it’s from 2018, but many of the questions still stand. How carefully will your data be ring fenced? You may not think about it much, as your DNA may hold little financial value to you, but DNA databases are one of the main assets that companies who process your DNA have, and why the testing is actually relatively cheap. Having access to thousands of DNA sequences, along with medical histories sometimes, means that data is incredibly value for scientific and commercial development. This is OK, we need sequences to develop new testing. Pharmacy companies also need access to sequences to develop and model new medicine. Therefore, it is likely that your data monetised and used for other purposes, which may or may not be OK with you. The big question to ask is whether it will be anonymised and how it will be used. Knowing this information before you commit allows you make informed choices, as not all companies are likely to be identical in how they handle things.
Another aspect that you might not think about is data security. If your data is of value to the company, and therefore is a potential asset, then it may be of interest to others. This can make data security to prevent things, such as hacking, important. This could be especially true if your DNA reveals linkages of significance, or things that you might not wish disclosed, such as cancer risk. Doing some research to ensure the security of any data that is held is important, but not often high on the list of questions that people ask.
Who can data be released to without my knowledge?
I’ve talked above about who will have access to your data, but mostly I talked about your anonymised data. It may not just be anonymised data that you are concerned about by however. If you are sending off for testing that relates to cardiac, cancer, diabetes or other risks, than this can have much wider impacts if shared. The legal landscape in relation to this is very much changing and catching up with the concept of genetic information as a protected asset is slow. Also, warning, I’m no expert in this. However, when sending away for this kind of testing it is important to know that it is often not covered by medical confidentiality, as it’s not considered a medical test when conducted via private companies. Being aware of how this impacts the rules around your data and what the company will or will not release is key. Why is it key? Well, it can impact all kinds of insurance schemes, from requirements to declare for holiday insurance if you are seen as ‘knowing’ a risk, to life insurance changes in cost or profile if released directly to the company. Knowing whether your personal, non-anonymised data can or will be released is essential before choosing whether or to whom you’re prepared to send you swab away to.
I suspect that this last point will probably impact those of you reading this blog less, but for to complete this list…….your DNA can also be released to law enforcement, depending on the country, so if you’ve secretly been a mass murderer then maybe don’t send your swab away and get your DNA added to a mass database.
What will happen if the company is sold?
As I said earlier, one of the biggest assets these companies hold is the databases of DNA sequences which we provide them. When something happens to the company therefore, it is this asset that many of those interested in the company might be after, and they may have nothing to do with the purpose you sent your testing for. Reading the small print before you send away your sample may not be able to prepare you for what happens when those rules change and you are no longer dealing with your original commercial provider. The one thing you can do in these circumstances in understand what access and rights you have to request that your data is deleted, or to delete it yourself, in the case that circumstances change.
I’m aware that the section above on what you might need to think about is pretty heavy and so I wanted to finish part 2 on something a little more population level and upbeat in relation to why having access to this testing is a good thing for science in general. For instance, we know that the ability to undertake ancestral testing was a reason that the bones of Richard III were identified and confirmed, which had big impacts for history buffs. It show that the use of wider availability of testing has all kinds of benefits, and not just to science. In terms of wider science, being able to look at bones using DNA testing has supported identification of Mycobacterium tuberculosis as present in Egyptian mummies which has helped us understand the evolution of this infection over centuries. More recently, looking at the development of Homo sapiens and how we became the human beings we are today has been forever changed by wider applications of these methods. Use of these technologies can therefore impact all aspects of our lives moving forward, and it really is up to us, both as individuals and as a society, about where they work for us.
Parts three and four of this blog series will be linked to book reviews that explore what those futures could looks like if the use of DNA testing and genetic manipulation change how we look at ourselves and others. So join me in continuing to explore the power of DNA.
This weekend I’m off to Torquay for the Agatha Christie Spring Literary Festival. It will involve talks, a statue unveiling and even a ball! Some of you will know that I’m a massive Agatha Christie fan and love a good murder mystery. It’s part of the reason my ambition for when I retire is to finally have time to write some of the pathology murder mysteries that I have drafted out. I’m planning a three book series called The Murder Manuals. Anyway, that’s some way off but I still love to indulge in a bit of Agatha joy.
Whilst thinking about it this weekend, when I should have really been packing instead, it occurred to me that maybe one of the reasons that I love my job so much is because, in many ways, working in Infection Prevention and Control (IPC) is like working to solve real life mysteries and challenges on a daily basis. You come into work every day not really knowing what the future will hold and spend your days trying to uncover who the criminals (microorganisms) are and how to prevent future ‘crimes’, in the form of infections. This feels even more true having recently posted about how a forensic science lecture I went to looked at solving crimes. So, whilst my head is all linked to the detective process (I suspect I’m more Miss Marple than Hercule Poirot, although really I’d love Mr Girlymicro and I to be Tommy and Tuppence) I thought I would write about why I believe IPC professionals make the best healthcare detectives.
Beginning at the end
Like most good crime dramas, we in IPC, often make our entrance towards the end of a story when we things have already happened. We then have to work backwards to understand what’s happened as well as working forward to prevent any future risk (‘crimes’). Now, the point we get involved can range a bit. Just like in detective dramas, if the crime is obvious the police get involved early. Sometimes however, Miss Marple suspects a crime has occurred (think Sleeping Murder) but everyone else can be slow to get onboard.
In the world of IPC sometimes there are very clear events that need to be looked into. An outbreak for instance is traditionally described as 2 cases linked in person, place and time, or a single case of a significant infection, such as Ebola. This works pretty well most of the time but there are circumstances where using this definition can mean it takes you longer to identify an outbreak, or ‘crime’, has occurred. An example of this is when outbreaks are linked to an intermediate environmental source. This means that you may have low level numbers of cases which don’t appear to be linked in time, or even person, but are just linked to location. I’ve written about the importance of environmental IPC before, but this is one of the reasons it can be particularly tricky.
Need to understand the rules
In every detective story there are rules. If you’re in a Christie novel there will be a denouement, if you’re watching Columbo you will always see the murder at the start, and if the murderer is a female she will always be the person Morse tries to flirt with badly at least once. Infection Prevention and Control is no different. There are unwritten rules that you need to learn and which will help guide you on your way. Vancomycin Resistant Enterococci outbreaks will often have an environmental component. Norovirus outbreaks within staff often have a secret staff member who vomited in the toilet and told nobody. Pseudomonas aeruginosa outbreaks make people ask ‘have you checked your water?’ All of these things give you a way to start investigating and a set of questions to begin with.
Now, here comes the word of warning. Just like The Murder of Roger Ackroyd broke the rules, so do bacteria and other outbreak causes not always behave the way they are supposed to. Just like any good police drama with a rebellious detective, you need to know the rules but also know when to ignore them. Know when to switch tack and think that your MRSA outbreak may actually be linked to your ventilation system, not direct hand to patient transmission. Be neutral enough when looking at your data to not ignore the clues that are there. Red herrings will be present and distract you, so know when to call a fish a fish.
Start broad and narrow down
One of the best ways, with any investigation, is to start broad and narrow down. This enables you to avoid diving down rabbit holes and missing other pathways that should be investigated. Very rarely can you turn up to a country house murder and exclude most of those present, and as Hercule Poirot famously states “it is always wise to suspect everybody”, and the same is true with IPC investigations.
Ask yourself, why do I think that there’s something happening? How do I know that cases occurring at the same time are actually linked? How are my surveillance systems set up to support identification of low levels of cases over prolonged periods? How sure am I then that a ‘crime’ has actually been committed? Once the body as been found, in terms of looking for sources, where do I get my information from? Do I consider just other patients, or patients and families, or patients, families and the environment, or even patients, families, environment and staff. This, all before you even start to consider how different organisms behave in different types of patients. In a country house murder you need to consider those above stairs as well as those below, and in stories like the A.B.C. Murders, you even need to consider those who came and rang your doorbell.
There are so many moving parts within healthcare and we need to ensure that we are capturing as much of that landscape as possible when we start our investigations. Starting broad supports this, but you also then need to know the key moments to start excluding options so that you can eventually get to the depth needed to support interventions and change. Eventually you have to have the scene where you commit and name the murderer. Within IPC, events such as outbreak meetings can really help with this, as unlike our favourite detectives, we can’t keep all the information to ourselves right to the very end. These meetings bring people together to both help gathering information but also to decide on how to focus next steps.
A plethora of unreliable witnesses
In A Murder is AnnouncedMiss Marple states, ‘Please don’t be too prejudiced against the poor thing because she’s a liar. I do really believe that, like so many liars, there is a real substratum of truth behind her lies’. One of the things that is often quite difficult to pin down during IPC investigations is….what is the truth? Truth is often seen as definitive but in reality truth relates back to the lens through which the individual sees the world. For instance, if you asked me what I was doing at 7am last Wednesday I wouldn’t lie, but I would have to offer some form supposition as I can’t actually remember precisely. The other complication is that those directly involved may be even less able to recall their own roles. If I’m sick in hospital days can merge into one and I’m focussed on my physical reality rather than taking in my environment. This is all before we take into consideration the fact that we may be providing sedatives and other medications that could impact recall. Would I remember that one of my visitors mentioned my niece had diarrhoea……..probably not.
Within IPC investigations no one is likely to remember every physical action, which is why audit can be a helpful addition, in order to have an external person capture trends. In other scenarios the actual witnesses to the event can’t speak, for instance ventilation gauges that may have fluctuated or alarmed (is that a voice?) to an event that no one wrote down or reported. This is especially challenging when you are trying to get to the bottom of grumbling outbreaks that have been going for some time, but also is a particular challenge linked to infections with organisms that may not become apparent for months, such as some surgical site infections or infections with pathogens like Aspergillus. Memory can make individuals particularly poor witnesses in these scenarios and good record keeping and notes are essential to support look back investigations (investigations where you are looking back to capture risks and event detail).
Need to know which tools to use
If you only interview half of the witnesses in your case, you’ll be lucky to get even half of the story, as it will all depend on which people hold the information. On some occasions you will luck onto all the answers with the first witness, but is this a risk you want to take? The same can be true in IPC investigations if you don’t think about the tools or sampling methods you want to access from your toolkit. Is your main focus on using bacterial culture? Do you have a method that will work even if the patient is on antibiotics? If you are looking for a viral cause, what method is best? PCR is not PCR is not PCR. You can look for RNA, or DNA, you can extract from different volumes and different types of samples. The pros and cons of all of which need to be considered. Putting together a sampling strategy in response to an investigation is like choosing the pieces of a jigsaw puzzle whilst knowing that you are not going to have all of the bits. You want to choose pieces that give you the best chance of accurately guessing what the picture is.
In IPC there are various pieces of documentation that will help with thinking in this area. Documents like the UK Standards for Microbiology Investigations (UK SMIs) can help guide thinking linked to which samples might be useful to take. UKHSA also has various documentation linked to outbreak investigation with specific organisms and interpretation criteria, such as measles, C auris, and TB. At the end of the day however, just like your detective walking into a murder scene, you will need to work out how to apply that guidance to what you see in front of you.
It’s all about the clues
Once you have investigated and questioned your witnesses then you need to be able to work out from your clues which pieces are useful and which are your red herrings and may lead you astray. Like all investigations the most important thing is to be methodical but you then need to make time to be able to think and reflect. Poirot famously once solved a case without leaving his front room, just by being able to sit and question those involved. I’m not saying that this is something we should try in terms of IPC, but I do think it holds some lessons for us about the power of thinking time. Especially when you are in the midst of an outbreak there is often a real drive to be seen to be doing something, responding to everything, and constantly doing more. After 20 odd years in micro/IPC I think I’m beginning to think that Poirot may have been onto something.
If you are constantly changing or adding in responses it can be really difficult, even if you reach resolution, to know which thing you did made the difference. Early on in an outbreak it can be easy to rush into making recommendations prior to having gathered all the information you need. It sometimes feels good to call an exposure meeting the minute you get the information that an event has happened. For instance, you may have days to respond in the case of something like a chickenpox (incubation period 8 – 21 days), before those patients become a risk to anyone else. Therefore waiting to call a meeting until you have gathered all the clues, until you know everyone’s immune status, levels of exposure etc, can mean that your meeting is so much more effective in managing any risk. Waiting until you have a decent action plan for where you might search for clues, i.e. sample, may mean you find the answer so much more quickly then having to go in for multiple attempts. Taking a breath and putting thought before action may mean you get to the final result so much faster. So utilise those Little Grey Cells!
Not everyone takes kindly to be investigated
IPC should not be about blame, but just like the house guests in a country house murder may not take kindly to a visit from Inspector Japp, some occupants of your ward may be less than happy to see IPC walking up to the nurses station. Although I talk about the similarities between IPC and detectives, we should not be feared and act like police, or worse than that judiciary. Often the reason why Jessica Fletcher gets further faster in finding the murder than the police at the scene is because she is seen as just another friendly visitor rather than someone looking to find fault. Her focus is on building and utilising relationships in order to gather information. She is often seen by the other witnesses involved as being part of their team, and the outputs of her investigations are often linked to co-production of outcomes by sharing information, rather than going it alone.
In general, as in many areas of working life, relationship building is key. You see Jessica all the time in Cabot Cove, not just when there’s been a murder. That means that by the time she finds the body she already knows most of the players and has built up relationship capital with those involved. This enables her to sometimes ask the challenging questions. I believe the same needs to be true for IPC. If clinical teams only see us when things go wrong, they are automatically going to be somewhat defensive. If they see and work with us when times are going well, as well as less well, they are more likely to feel we’re in it together with shared ownership. All of which means we may also get to the source that much faster when we need to.
Sometimes there’s a twist in the tail
There are a number of famous Agatha Christie stories where the murder victim turns out to not actually be dead, I won’t spoil them here. The same can be true for IPC cases. There are certain organisms, of which Adenovirus is my personal favourite, that can both cause primary infection and then go latent and reactivate later. Often this reactivation is linked to immune status, and of course many patients in hospital have immune systems that are doing less well. These present challenges as you can look like you have a cluster of cases but, due to the type of patient, they can all be independent findings that happen to cluster together. So, without the right investigations you can call ‘murder’ when actually there is no corpse. Being happy to hold your hands up and step down when you have new information is an important trait, but knowing to get the testing done to enable you to do so is even more so.
The other scenario that can happen is, as Sherlock Holmes famously said, “When you have eliminated the impossible, whatever remains, however improbable, must be the truth“. There will be things that have been done, behaviour that has occured, that you would never imagine or predict. Over the years I’ve found a lizard in a bathtub, olive oil used as skin care by parents, and all kinds of things in fridges and freezers, just as the tip of this iceberg. Things that out in the real world would probably not be a risk, but in the healthcare world can lead to all kinds of issues, none of which would be on my primary list of questions when trying to identify a source. The world continues to surprise me, and therefore in the world of IPC keeping enough of an open mind to to respond to the unexpected is essential.
It’s a team sport
Poirot has Hastings. Morse has Lewis. Sherlock has Watson. Tuppence has Tommy, and Jessica has most of the population of Cabot Cove. Solving crimes benefits from teamwork and IPC is no different. I’ve spoken about the importance of relationship building but doing IPC investigations well benefits from more than even that. One of the key ways these partnerships work is by creating the space where the discussion and reflection we’ve already talked about can happen. In healthcare, which is far from a contained setting with only a handful of key players, being part of a team can also provide vastly more eyes and insight into what happens in reality.
The Hawthorne effect is a type of human behaviour reactivity in which individuals modify an aspect of their behaviour in response to their awareness of being observed
One of the reasons that it’s important to undertake a team response within IPC is that if I turn up, a stranger or less frequent visitor on the ward, then those on the unit may behave differently because I’m there. If you see IPC hanging around a sink, for instance, then you may suddenly focus way more on your hand hygiene efficacy then you would otherwise. If I go to speak to a family, they may say different things to me than they would to the bed space nurse they see everyday. In order to get the full picture I may not always be the right person to ask the questions. Being fully integrated, being seen as part of the team, or having relationships with people that are, can make all the difference in terms of the success of your activity. Everyone benefits from having a Hastings to send in to ask questions from time to time.
No greater satisfaction than being part of the denouement
I don’t know about you but I just love the moment that everyone gathers at the end of a Christie novel and detective starts the process of walking everyone through all of the different clues, red herrings, and witness statements. The moment when you discover if you’ve picked up on everything that was on offer to you, and even more than that, the anticipating of waiting to hear if you’ve put it all together in a way that a) works and was b) actually correct.
I feel the same way when I finally have that moment when I crack the case, when I find the source, or even just get to the point where I understand a tricky result. The hallelujah moment when you look down at the jigsaw pieces you have and you can finally see the full picture. It’s the reason that some of our favourite investigative successes live on for years in teaching and case studies. I will talk about the case of the Norovirus and Biscuit Tin to anyone who will listen even now. The settings may be different but every detective, whether in a novel or in healthcare, loves to regale others with their exploits. We just can’t help ourselves. My excuse is that sharing the learning helps is all. That said I’m off to attend a talk called ‘How to kill people for profit’. I’m assuming it will give me all the tips I need to be the next cozy murder success and maybe even weave in the odd IPC detective drama moment into the mix.
There’s been a bit of a delay posting this one, as it was supposed to come out a couple of weeks ago, but I ended up needing to take a bit of a well-being break. Healthcare Science week was a brilliant blur but full on and, for once, when I went on leave I decided that all work, yes even this blog, needed to be put on hold so I could have a complete break. I hope absence has made the heart grow all the fonder……
Now, onto the science
At the start of Healthcare Science week, my family and I, because they love me, went for a night out to experience a different type of science…..forensic science. I wanted to go to see ‘Walking into a Murder Scene: an evening with Simon Fowler‘ by First Forensic Events for 3 reasons:
The first is that I think it is really helpful to engage with science beyond your discipline for inspiration and ideas. In this case, I’m not a big true crime fan or anything like that, but I was interested in how they deal with technical challenges we both share, such as low volume detection of targets by PCR amplification from human blood, as this could help with sepsis detection in clinical settings.
The second is that I have a long-term plan to write some pathology murder mysteries, by long term, I mean it’s my retirement plan, and so I also thought making some science notes could be helpful as success is mostly in the preparation.
Finally, I try to engage with science outreach wherever I can, no matter what the topic. I wrote a blog here last year about aviation outreach at a massive airshow known as RIAT and what learning that triggered for me. I really believe in seeking out and engaging with these opportunities, firstly because they do a lot to inspire me as to what more I can do. Secondly, because why reinvent the wheel? Learn from others about what works well and how I could switch up what I do. Last and by no means least, if we don’t support these people and these events, they may cease to happen. Finances are tight everywhere, and outreach is increasingly seen as a ‘nice to have’. Numbers talk, and so taking some time out of my day to be there to support others talking science is the least I can do.
The event was the first ones from a group known as First Forensic Events and was, in many ways, a trial run. The house was packed, though, and there was an obvious interest from those attending to just find out more about a world that most do not have access to. It got me thinking and as a result I thought I would focus this blog on what I took away in terms of how we, as scientists and Infection Prevention and Control professionals, could do more in terms of reaching out to a different audience and shedding some light on what we do to lift the veil in a similar way. I often think we don’t talk enough about the fascinating aspects of what it is we do for a living and this event made me realise that we are in position to share that with others and there are people out there who may want to learn more.
Location location location
The first thing I want to talk about is location. This event took place at the Royal Gunpowder Mills, which was objectively brilliant. One, it is not a place that is open that much to access, and so to be able to attend for an event already felt special. Two, it’s a place that’s interesting and quirky, and so even if people aren’t leaving and talking about how great your content is, they are likely to still be talking about what an interesting night they have had. I get pushed all the time to have events in cheaper and less interesting spaces because the costs need to be justified. The truth is, as much as we may dismiss them, locations can make or break events. Therefore, investing in them makes complete sense to me.
One of the reasons that location choice is so important is that it gives you the opportunity to really demonstrate that you have thought about the comfort and experience of your audience. Are there drinks available? What about food? How will people find their way to seats etc? Attendees will focus better on the content if they are not distracted by feeling hungry or thirsty or trying to understand where they need to be. They are also more likely to linger and talk to each other, which is key to both creating a buzz about the event and to permit natural network creation which will encourage future support.
A clear sense of identity
All things tend to be easier or work better if you have a clear sense of identity or what you want to achieve. This works for everything from advertising events and getting people into the room, to how people respond to the event itself. It is therefore worth investing a lot of time in both thought and planning in order to get this right, before diving deep into the practicalities and details.
When we spoke after the session it was clear that Simon’s focus was linked to training. His unique selling point (USP) for the session was to demonstrate not only some of the interesting cases he’d been involved in but also why and how he got into the work he did. He was also very clear that, in the same way we always want to focus on the patient, he wanted to make his sessions about the victims. Simon started off his session by talking about his core values and where he came from, in his case it was that he wanted a military career but that life turned out somewhat differently. He was diagnosed with Perthe’s disease which meant he was no longer eligible for military service, and so he then had to re-focus and choose a different life path. He built the start of his session up around his personal journey into science.
If we were to do something similar for health I think the need to be clear about our USP holds true, and for me, the things that seemed to engage the audience most were a focus on clear story telling with outcomes to show your role and it impacts i.e. what did you do and how did it change things? The other thing that seemed to really fascinate those present was discussion about prioritisation, outcomes and decision making. How do you decide what to do, in what order? How do you make decisions and how did those choices impact the end result? I suppose I’m talking about making thought processes an object of active discussion and raising awareness, rather than maintaining mystery or focusing purely on events. The stuff someone can’t find out by reading up about something on the internet and can only be got from a more intimate discussion based setting.
Back to the fundamentals
Keeping to the basics and planning, lets talk set up. Location is important but so is the staging. Everything from what you are planning to wear, to props and the tech that you will use. Is your outfit comfortable and accessible? Are you going super smart/business, that could be seen as hierarchical? Will you go branded or display your geek like tendencies with, for instance, a CSI T-shirt? All options are fine but they need to fit with your USP. Who are you selling up on that stage? Choose an outfit that fits with deliberation rather than as an accident.
Making the staging visually interesting is useful, especially if people are sitting for a while before everything kicks off. Offering an intriguing set up means that people will engage before you even start, as well as allowing people to speculate what might happen later. Having props that you will use draws your audience in.
It is important at the planning stage to also be considering accessibility. Too many people believe they have a loud enough voice that they don’t need mics etc. That works for some people but there will be people in the audience who you don’t reach and who will find it a barrier to engagement. Mics also allow nuance in terms of being able to go both loud and quiet as needed, rather than focusing constantly on projection. The same with slides if you are using them. Will they be accessible to people who are colour blind? What level of text is appropriate? What fonts may permit engagement? Should you be image heavy? In the case of something linked to criminal cases or health, how much do you show? Gore, surgery, infection etc can be triggering, so consider what level may be needed/appropriate. If you are recording (pictures, video etc) think how this might impact your staging and movement and if it will change your lighting requirements.
During the show itself, when we attended, there were some technical issues as the laptop running the slides stopped working. I think this is everyones worst nightmare, but has also happened to us all at some point. It reinforced for me that if you are relying on tech as part of your staging, you always need to have a plan B about how you will handle things if something happens to that tech. How you will you pivot? Having a plan means that you will be less flustered and therefore impact the experience less for those attending.
Selling credibility
Credibility is everything, whether we realise it or not. Setting up and selling your credentials is an important thing to do both before the event and early on during the establishment phase. Why should we listen? What do you know? What’s your experience….really? There are multiple ways that you can both do this and embed it. Thinking about how you are going to both establish and sell your credibility is something we don’t often consider and may take for granted, but if you are trying to speak to new people, especially outside of your field, it is something to really think about.
One of the great ways that it was done at the First Forensic Event was that someone else whom people may be familiar with, in this case Donal Macintyre, introduced Simon linked to both the event and by covering his skills and expertise. We all use testimonials in every day life and this setting was no different. I’d heard of Macintyre Investigates but as someone who doesn’t engage with a lot of true crime work the name didn’t mean much. It did however mean something to most others there, and he also talked about the TV work and others things Simon had been involved with in order to try to establish wider credentials. This is no different really to someone reading out your bio at a conference, but re-pitched to make it useful to a different crowd, and still well worth doing.
The other thing that Simon did was to acknowledge the other members of his crew. This was important for two reasons. One, because we should acknowledge that we are not single person armies and the work and support provided by others. It makes you not only more approachable but also acknowledges the work undertaken by other people to get us to where we are. In this particular case however there was another important purpose in acknowledging the other people who were involved, and that was to enhance the credibility of the event itself. The other people involved in First Forensic Events are other forensic scientists and police detectives, which aid to further establish credibility by inclusion in networks and experience. If others are willing to add their names to your events then it also demonstrates their backing and investment in your undertaking.
A story in three acts
We’ve reached the nitty gritty. How will you actually structure your event to achieve your outcomes? What are you trying to achieve? Simon was clear that it wasn’t just about factual presentation, but about him and his journey as a scientist. I think that was a really good decision and something that many of us as scientists should consider when working up our presentations. We are not science in isolation from ourselves, and so bringing your full self to these events is bound to be more impactful, and also helps to engage your audience more. For this purpose the session was structured around stories, stories about self, stories about action, and stories about impact. This kind of story based structure enabled the audience to really engage as the human ability to engage with oral tradition goes back to us sitting around campfires and learning through listening to tales.
The first third was based around learning who Simon was, what drove him and how he got into his work as a scientist. Fundamentally this section is about building of rapport as well credential building. It also enables the audience to settle in and for an expectation setting phase to be undertaken. The second third was a practical session. This is where Simon demonstrated some practical aspects of what a bludgeoning event could cause in terms of blood splatter, and scene investigation. This enabled a change in pace and energy, which breaks things up for people as they will have been sitting for some time at this point and changes it from being a didactic slide presentation. It also means people go into the break with a level of introduction of what may be discussed in more detail post break and therefore your audience can choose how much information they are comfortable with, and gives an exit opportunity if needed. This gives detail without inclusion of people or actual harm, and therefore allows engagement without emotional risk. The final section, post interval, was based on actual cases, still rooted in technical discussion, which supports focus on facts rather than emotion. This type of structure supports engagement and gradual submersion rather than attempting to shock.
Speaking to the room
This brings us onto the audience. How do we speak in a way that allows the audience to truly engage. I’ve talked about structure but there are other things that can help. The first thing we can do is do some scene setting. Making sure at the start of the session that everyone know how the event is going to work and what the rules are. This includes some basic things like telling people that there will be an interval, what time it will be and how long it will run for, so everyone can make sure they know how long they’ll need to engage. In the case of this particular event it also included scene setting around what might be shown and discussed, making clear the level of imagery etc in order to reassure and expectation manage. It also included being very clear that it was completely OK for people to leave and return at any point, as people may be triggered by different things, different memories, in order to reduce distraction by discomfort or concern about whether removing yourself would be acceptable. It also included the fact that there would be a Q and A, and that Simon and his team would be available for questions both within the event and during the breaks.
As with any science event it is worth doing what you can to avoid exclusion of your audience by thinking about how you will use technical terms and being weary of abbreviations. Many of us use abbreviations without even thinking about it as part of our engagement (I used the term PCR earlier) as it is part of our language. Those in the audience are less likely to have the same shared language however, especially if you are reaching out to a new audience. Making sure you allow time to explain any technical terms you are going to utilise is a key thing to practice. When you think you have explained enough you are likely to need to explain even further. As someone who doesn’t work in law enforcement some of the terms and abbreviations used in this event didn’t mean anything to me. That didn’t really impact my understanding or get in the way of the outcomes however, but made me remember how healthcare is filled with exactly the same barriers to full understanding, and that I need to be more careful about how I talk about my job also.
One way to make sure that you get feedback on how to improve and make tweaks on things like language is by making sure that the first time you do anything you add plenty of cheer leaders/critical friends into your audience. These people can flag and help you improve for future events, as well as providing some reassurance and friendly faces in the room to help alleviate your anxiety.
Maintaining accessibility
I’ve talked about accessibility already in terms of supporting your audience to logistically engage, but now I’m talking about connection. How do we make sure that we allow participants to connect with us, feel engaged with us, and fully share in the event. There are some key ways that I think this can be done, although sometimes it can be scary. I think the key one for me is allowing yourself to show vulnerability. Sharing enough of yourself that others can start to see you as a person. This includes sharing things such as values and drivers, but also sharing failure and things that did not go so well. Allowing people to see you as a person and not just a role.
The other part of this is being open and able to laugh at yourself, and allowing others to join you in that moment. All of this can be really shown in less structured moments. Moments where you make yourself available to engage 1:1 in breaks etc. Also, in a more open way by including moments where audience members can fully participate in things like Q and A’s. I always find it helpful to set parameters for these. Being open about the fact that there is nothing off limits, especially with kids. So they can ask what my favourite colour, is or how much I earn, or what I find the hardest, without restricting them to the science. Setting boundaries and expectations in general means that everyone knows what the rules are. Can you use your phone? Can people take pictures? Can people leave? All of which enables people to focus on engagement rather than attempting to predict what’s in or out of scope.
Pitching your future
How does it end? You’ve made it through, you’ve shown your full self. Hopefully you’ve felt that the audience engaged. You’ve made it through the Q and A. What do you do now? You need to make sure that you provide another opportunity to engage in the future whilst everyone is still paying attention. This is the moment to link to other opportunities, but this means you need to have those other opportunities set up and ready to share. What I’m saying is, as much as it’s crucial to focus on the right now, to make a real success out of events like these you need to be able to provide the next thing. So making sure you’ve planned ahead and have something else to sign post to is a key stepping stone to success.
Even if you don’t have another event planned you need to make sure you are thinking about marketing. What is your social media? Do you have a web page? Where can people go to find out more, either about you or about your future planning? Making sure that you have these things set up so that people can continue the engagement that they’ve started means that this is less likely to be a one off and more something that will be a stepping stone to future engagement. Having shown who you are and having brought people into your world, the logical thing is to make sure you have a plan for showing people what’s next.
So much that links us
So after all that, what did I think of forensic science. When I go to any of these things, what always strikes me is that we have so much that links us. Whether we are acting as detectives in finding an infection or a criminal linked to a crime scene, we are actually following very similar thinking and processes. We even use some similar techniques. I walked away thinking that I had been involved in a super cool event, but also struck by how brilliant it would be to do something similar for healthcare, and whether there would be anyone out there interested in setting something up. I left, as I almost always do, with my mind on fire with ideas and inspiration, and I wish to do so much more than I currently do. It reminded me how much we need to put ourselves out there and be brave. More than that even, it reminded me of how much the work we do is fascinating, and how interesting it would probably be to those that have never traveled in our footsteps. Perhaps even more so after the pandemic. So step up and step out, your audience awaits you!
This post was supposed to be something quite different. It was supposed to be about One Heath and a great podcast created by Beckman Coulter I was involved with in 2024, alongside some really inspiring people. In some ways it still is that, but because of the cruel reality of life it is actually also something quite different.
”Going Macro on Micro” is a podcast that Dr Simon Doherty and I were involved with that explores emerging themes and pressing issues in the world of microbiology. As the host, Dr Lough, says the podcast covers everything from investigating the global challenges of infection control to unveiling the future of diagnostic technologies.
The week the final episode of the podcast dropped, before Christmas, I got some pretty devastating news. Sadly Simon has passed away. Now, I didn’t know Simon well. We’d emailed since doing the podcase together and I kept an eye on the awards he received and his really interesting posts. In this limited contact though, he still managed to inspire. Recording the series with him was such a privilege. He was kind, open and funny. More than that he was so knowledgeable and I came away feeling like I’d learnt so much. I am so sad that I won’t be able to build on the foundation we laid to continue to learn from him and talk about the challenges/opportunities that face us in the fascinating world we both inhabited. I thought about not sharing these episodes when I heard the news, but then decided that I don’t want you to lose out on the honour I had of learning from him direct. I hope that you will hear both his wisdom and his challenge, and also aspire to do better, as I do, as a result. Thank you Simon.
I’ve decided to keep the focus on Simon and just put some graphics and links here that might supporting learning more about antimicrobial resistance and One Health. At some point when the loss of Simon has had a little more time to be processed I will think about writing something in a little more depth reflecting on his comments and the overlap between human health and veterinary medicine. Until then, the links to the episodes are below:
Ahmad Nayeem , Joji Ronni Mol , Shahid Mohammad. (2023). Evolution and implementation of One Health to control the dissemination of antibiotic-resistant bacteria and resistance genes: A review. Frontiers in Cellular and Infection Microbiology
Episode One
Rhouma, M., Soufi, L., Cenatus, S., Archambault, M., & Butaye, P. (2022). Current Insights Regarding the Role of Farm Animals in the Spread of Antimicrobial Resistance from a One Health Perspective. Veterinary Sciences, 9(9), 480. https://doi.org/10.3390/vetsci9090480
Episode Two
Sanseverino, Isabella & Navarro, Anna & Loos, Robert & Marinov, Dimitar & Lettieri, Teresa. (2018). State of the Art on the Contribution of Water to Antimicrobial Resistance. 10.2760/771124
Episode Three
Sanseverino, Isabella & Navarro, Anna & Loos, Robert & Marinov, Dimitar & Lettieri, Teresa. (2018). State of the Art on the Contribution of Water to Antimicrobial Resistance. 10.2760/771124
Episode Four
Sanseverino, Isabella & Navarro, Anna & Loos, Robert & Marinov, Dimitar & Lettieri, Teresa. (2018). State of the Art on the Contribution of Water to Antimicrobial Resistance. 10.2760/771124
Episode Five
Sanseverino, Isabella & Navarro, Anna & Loos, Robert & Marinov, Dimitar & Lettieri, Teresa. (2018). State of the Art on the Contribution of Water to Antimicrobial Resistance. 10.2760/771124
Episode Six
Sanseverino, Isabella & Navarro, Anna & Loos, Robert & Marinov, Dimitar & Lettieri, Teresa. (2018). State of the Art on the Contribution of Water to Antimicrobial Resistance. 10.2760/771124
The World Health Organisation (WHO) talks about it like this:
Antimicrobial Resistance (AMR) occurs when bacteria, viruses, fungi and parasites no longer respond to antimicrobial medicines. As a result of drug resistance, antibiotics and other antimicrobial medicines become ineffective and infections become difficult or impossible to treat, increasing the risk of disease spread, severe illness, disability and death.
I think it’s easy to forget that although AMR is a big part of the professional life of most Infection Control and microbiology professionals, even for other healthcare professionals it features less often, let alone for members of the public. It can be surprising therefore when you do go out and about, or even just talk to friends and family, to hear some of the ways that non infection professionals think about how AMR works and who it impacts.
Common misconceptions I hear when talking to people about AMR:
It’s the body that becomes resistant to antibiotics
I have never taken antibiotics so I cannot get a resistant infection
Antibiotics treat all types of infection
Antibiotics can be stopped when the symptoms stop
Only infected patients can transmit antimicrobial resistance
If you reflect on some of these myths, it’s actually pretty easy to understand how they come about. Most people are focused on themselves and act from a human centric point of view. Many people give little, if any, thought to the multitudes of living bacteria that co-exist in their bodies. Once you accept this as the starting point, most of these myths are actually based on pretty small mental leaps. If, however, you don’t switch your point of view before you start having conversations about AMR, you can unwittingly end up reinforcing the very misconceptions you were aiming to address.
One of the reasons that I think this post is timely right now, is that I am already seeing more posts linked to how we should not be putting artificial medications into our bodies, alongside the back lash against vaccines, and so it seems to me a good time to remember what a difference these, now common, medical interventions have made to the lives of individuals and public health in general.
Let’s start with a little bit of context
Hardly any of us will have living memory of life without access to antibiotics and what life was like in a world without vaccination. One way to really get a feel for the impact these common interventions have made is to look at the impact in the last 30 years on reducing child mortality (death). Even in this recent time period, massive progress has been made due to advances such as the rota virus vaccine, but also in getting more global access to antimicrobial therapy where it is most needed.
Public health is multi factorial, with impacts being cumulative and made by more than just one thing, so not all of these impacts are made by antibiotic and vaccine availability. Other steps to reduce death linked to infectious disease include everything from clean water and sewer systems to pasteurisation and other means of food safety controls. The impact of these combined approaches is massive, but as the UN sustainable development goals show us, those of us who are access to clean water are not actually in the majority and more is yet to be done to ensure equality of access.
To aim to undo some if not all of this century plus of progress is something I find pretty hard to process. If you’ll forgive the momentary indulgence, I have to state that I think the current anti-vaccine and general anti medical stance that is being seen within some groups and communities is ultimately an act of extreme privilege It’s a privilege to be able to choose not to access something that is readily available to you and not available to others. It is a privilege not to have to live first hand the consequences of what the alternative might hold. It’s also a privilege to be able to change your mind and choose to access something later. Thinking of things in this light doesn’t necessarily help with having conversations in a supportive and open way when some of the underlying thinking may be so different, but it may mean we can flip the dialogue from one of imposition to one about the power of choice, and supporting evidenced based decision making for all.
Where does AMR come into this?
There’s a big stat that everyone quotes about more people dying from AMR than cancer by 2050, with an estimated 10 million deaths. As a scientist, I get the need to quantify and use numbers, as a human being however, I find that numbers that are so big can just be off-putting. They are so large it can make us, as individuals, feel powerless to impact them.
For me, the reason this conversation is so important to have in the right way, and pitched to the right communities, is because if we are going through a period of global push back against the common interventions, such as vaccination, that have successfully reduced mortality and provided first line protection, then our final line of defence in terms of treatment is now even more vital. 2050 isn’t that far away, and we are already seeing consequences linked to more resistant organisms being identified in severe infections. Therefore, the time to be having conversations and really raising awareness to impact decision-making is now. Sadly, this is coinciding with a period of time when trust in healthcare professionals and science in general feels very low. Instead of being defeated by this, however, we need to use it a driver to really focus on how we can do it better.
One of the other reasons that AMR is both important and challenging to communicate is that it is always in constant flux. You can’t just learn about it and move on. The mechanisms change, the diagnostics change, and the interplay of all of these factors within the bacterial host interactions can make it even more complex and hard to engage with. To exemplify this, the figure below was something I saw posted on Bluesky and fell in love with, as I adore the fact that it lists all kinds of routes to AMR in a single image, thus capturing the complexity of what we’re dealing with.
That said, you don’t have to understand all or any of this image to understand the core of why AMR is going to be a problem moving forward. The main thing to take away from it is that AMR is complicated, and as a result you will hear many different messages linked to it, and those messages will continue to change as we learn more and the impacts are felt differently. As a result, it can then sound like we don’t know what we’re doing, or just end up really off putting, as there isn’t one clear message we are getting out there for people to cling onto. We, therefore, need to build this flexibility into messages and link around core themes rather than trying to talk in absolutes. Otherwise, we risk losing more of the public confidence than has already occurred.
What is being done nationally?
This year, a new version of the UKs National Action Plan for confronting AMR has been released and within it there is a strong focus on the acknowledged need to educate both members of the public and healthcare professionals on AMR.
There is also plenty in there about increasing equitable access to antimicrobials, the need to improve diagnostics to help support both diagnostic and antimicrobial stewardship, and something that pleased me greatly, a special mention of the role of the built environment in managing AMR.
The thing is, top-down approaches will only ever get us so far. At some point, those of us involved in all things infection also need to be consciously including some of these drivers in our own every day practice.
No one can do everything, but whether you are collaborating with industry, undertaking research, or working in clinical practice, we have to embed AMR based action into our encounters. Do you include an AMR slide into all of your teaching? No matter the audience? Do you take the moment when it comes up with friends and family to just talk about the fact that this issue exists? Can you free up some capacity and undertake some public engagement?
Recognising there is a need is not the same thing as addressing that need, and we also have to be there to hold strategic partners and organisations to account in order to make sure action happens. So, let’s consciously match that top-down approach with a bottom-up drive for change.
What resources are there to help talk about AMR to other professionals
Having talked a lot about the need to talk to other healthcare professionals and seeing so much about #WAAW this year, it does really feel progress is being made to support us all to do this better.
Those of you who are UK based have probably heard of and support the Antibiotic Guardian programme (https://antibioticguardian.com/). This programme has lots of resources and supports personal action by asking you make a specific pledge about what you will undertake linked to addressing AMR.
Every year, new infographics come out that talk about different aspects of AMR. Some of these, like the one above, link AMR into commonly known components of healthcare practice, such as hand hygiene, in order to support individuals to feel empowered to act. Others focus more on messaging about antibiotic courses, or as we heard a lot about at the FIS/HIS conference last week, things like IV to oral switches, and sending the right samples to enable a switch from broad to narrow spectrum antibiotics. There’s plenty of ones out there now that can be really useful to embed in talks or laminate and put up on walls. The UKHSA especially have recently released a lot for WAAW, and because there are so many, you can keep them on rotation so that they don’t just become invisible as people see them too frequently.
I’ve also been involved in creating various content this year, as have many others, including webinars and podcasts to explore some of the issues linked to AMR and provide different routes via which healthcare professionals can engage with information and CPD on this topic. I’ve included a link to just one of these below in case it’s of interest, but a quick internet search will provide you with all kinds of others.
The main thing to remember is that we all like to receive our learning in different ways, and so ensuring that we remember that when we’re designing our education strategies is one of the best ways to be impactful.
What resources are there to help talk about AMR to members of the public
The resources you might want to use linked to AMR will vary greatly based on your target audience. It’s important to remember that even if someone is a healthcare worker they are also a member of the public, and depending on their personal background or setting they work in, utilising content created for the general public may serve both purposes.
There is some really great video, podcast, infographic, blog, and other content aimed at public outreach on AMR. There’s even a musical called The Mold that Changed the World, about Fleming and Penicillin, as the first antibiotic.
There are lots of different entry points when you are thinking about content that might be appropriate, and you’re likely to go to different depths depending on whether you are doing a one off encounter or a more prolonged piece of relationship building.
The post that is linked to at the start of this article on AMR as a Super Wicked Problem may help with choosing your content. You may also want to consciously address some of the myths mentioned at the start or even start your conversation with the fact that many antibiotics actually started as products identified in nature, and so are not as far from natural compounds as may be frequently thought.
Some of you who have been reading this blog for a while will know how proud and passionate I am about The Nosocomial Project, which aims to use a science, technology, engineering, arts and mathematics (STEAM) approach to talk about infection and infection risks.
As part of this work, we organised a two part festival linked to AMR entitled Rise of the Resistance Festival. All of the content is split across YouTube and the website. I’ve included linked here in case any of it is useful in your own settings when you are looking for inspiration or planning content. The content covered in the festival included everything from a play aimed at pre-school aged children entitled Sock the Puppet, who is a hand puppet who is scared of germs, expert panels, comedy sets, and Klebsiella as a drag queen. I still have so much fun rediscovering this content, and I hope you’ll feel the same way.
I would make a plea that we all work together on this one to do some myth busting and get messages about AMR out there, but also find a way to get messages across that are entertaining/joyous and filled with hope for what we can achieve, rather than focusing on the horrors of what happens if we don’t get our act sorted. I think all of us, including healthcare professionals, have had our fill of trauma in the last few years. So, let’s focus on empowerment and positivity to make this change happen, rather than following in the footsteps of those who want a world of decisions driven by fear.
I’m off to the Federation of Infection Societies (FIS) conference this week. I’m involved in 3 sessions over 2 days, and in many ways, these types of events are a complete highlight for me. I get to be inspired by hearing new science, I get to catch up with wonderful colleagues who I don’t get time to see very often, and I get to immerse myself in all things microbiology without the distraction.
There is another side to this coin, however, and that is both the anxiety that builds before I go, and that can last throughout the whole event. The ever-present spirals of ‘do I know anything?’, ‘will I say something stupid?’, ‘will I know anyone?’, and the classic ‘do any of these people actually like me?’.
The combination of this social anxiety with the, sometimes long, very peopley days, can mean that I hit spirals pretty easily and the lack of solo recovery time means that I can find it pretty exhausting by the end.
Now, I’m obviously not talking about extreme cases of social anxiety that may require informed medical or long-term support. I’m talking about situational anxiety that most of us may find ourselves in from time to time.
Just in case there is anyone out there in a similar boat, I thought I might put together some things I’ve learnt along the way that help manage some of my anxiety traits and enable me to actually enjoy the experience rather than dreading it.
Do your prep work ahead of time
The first thing I’ve had to learn is that I can’t just pretend that doesn’t happen. I can’t wish it away. What I can do is be prepared and make sure that I have made the process as trigger free as possible.
For me, this is about simple things, like getting a hotel as close to the venue as possible. It means that if I just need a 30-minute alone break, I can take one. It removes anxiety about getting lost or forgetting something crucial and not having time to go back for it, which, although minor, can be the final straw. It’s also about making sure that I have pre-found all the rooms I need to locate ahead of time, so I know where I’m going, and that ahead of multi-day meetings I have a plan for which sessions I’m going to before I even travel to the event.
Know your triggers
I know that I have a few things that really lead to anxiety, but perhaps more unique to me, is the fear that I was have an auto immune attack and won’t be with people who understand what is needed. I learnt early that the best way to cover this one off is that I very rarely travel alone, especially over seas. I often travel with my mum or one of a very small list of truly trusted people, who I know would understand how to get me help if required.
Something that is more likely to strike a cord with others, is that I am also the girl who has walked into conference rooms, spent 15 minutes and walked out, as I knew no one and was just overwhelmed. I’m not proud of these moments, but I think it’s important to acknowledge that they have occurred. Although, to be honest, when they’ve happened, I mostly felt invisible, so I doubt anyone noticed.
I have discovered that I need to know that the space is one where I feel welcome for me to perform at my best. This sense of welcome can be either intellectual, because of the topics covered, or because of feeling a sense of community, as the room contains people within my field or in strong alignment with my values. I’ve found the overwhelming feeling hits most strongly when I’ve been in very large political or strategic sessions, where I felt out of my comfort zone on both intellectual and community counts.
That said, I’m not too bad in the sessions themselves, I’m there to learn something new, and learning excites me even now. It’s the breaks that are my nemesis, especially when large groups all surge into a space at the same time, and the weight of expectation that you must now network lands. The seconds that feel like hours of desperately searching for faces you recognise and being forced to face the fact that yes, you really should go up and speak to that absolute stranger, as it’s the right thing to do. It’s these moments that can cause me to bolt for the nearest bathroom.
Carve out time for yourself
One of the key mechanisms I’ve identified to help with my triggers is that I make sure I have enough time to myself, be that eating food away from the venue so I feel more certain what it contains and less at risk, to making sure I have evenings to myself to process and unwind.
I usually come over as really social, and really into spending time with people, and I am both of those things. I also only have a limited amount of social battery, and so in order to maintain that extrovert part of myself I have to have recharge time. I love talking to people about this blog, I love hearing about and responding to other peoples work, but at a certain point I need to sit down with an audio book and a cup of tea in order to do it well. This means that when I go through the brochure ahead of time, and plan my sessions, I make sure that I have enough blocks of time to enable me to be my best self when I’m in the space with others. Sometimes all you need is a walk to a local coffee shop and back to give you the perspective you need.
The wonderful thing about having hit my 20th year as a Healthcare Scientist, is that I now also know quite a few people, some of whom I’ve known for well over a decade. This means that at most events, there are also people who I count not only as colleagues but as friends. People that I can just go and spend time with that doesn’t include social commitment. Those friends you have that you can just be in the same space without any demands being made. If I’m at an event where these people are also attending, then I know that I have someone I can just excuse myself to catch up with if I’m having a moment. It’s also the great thing about ensuring that you have a hotel room nearby. Your safe bolt hole is only minutes away.
Make an agreement with yourself about how much is enough
The fact that you have social anxiety does not provide a free pass to escape one of the fundamental purposes of attending conferences, networking. It’s key to your career, it’s key to your development, it needs to happen. The thing is that there are varying degrees of what networking can be, and before you’re in the space, you need to decide what level you are aiming for and will therefore achieve. For me, my deal is that I will, on each day, speak to one person I don’t know. I am not allowed to finish my day without this happening, but once I have had that one daily interaction, then any further moments are a bonus. Once that one challenging moment is over with the pressure is off, and then I almost always over achieve on my goal.
Be realistic about how much you can expect of yourself
The key thing I’ve learnt is that I have to realistic when I’m making that deal with myself and deciding on achievable targets. For me, there is not point is saying I will speak to five people I haven’t met before, as I’ll just be setting myself up for failure. You will also find that I rarely sign up for conference dinners, as I have over the years found that if I’m in a space with other people from 08:00 – 18:00 I will really struggle to then spend yet more time with other people, no matter how lovely or interesting those people are. All I will want at that point is room service, tea, and a movie in my room.
Everyone will have their own tolerances and lines. The important thing is to have enough self reflection to know what yours are. Otherwise, you just add guilt into the anxiety mix, which is not much fun for anyone.
Learn how to work a room using tools you are comfortable with
One of the other things that I’ve learnt about myself, is that although I get super anxious standing in a room trying to approach someone at the coffee table, I am much much more comfortable moving around the exhibitor stands. The guys at the exhibitor stands are motivated to speak to those who approach, and there are usually science based discussions that I am eager to have. This, for me, is a match made in heaven, as it breaks me into the speaking to people I don’t know in a very gentle way. If I’m lucky, I will also meet others when I’m wandering around, which will allow me to tick my ‘speak to one stranger box’ as exhibitors do not count on that front. The added bonus is that I also often manage to find cool new stuff I’m interested in or develop collaborations whilst this is happening, so it’s a no lose scenario for me.
The other thing that having worked for 20 years has given me is the opportunity to be asked to be involved with sessions. For this girl with social anxiety, this is actually a great thing, despite the fact that it sounds like it should be stressful. I’ve never minded public speaking in the same way as I worry about 1:1 interactions. When I speak, all I can do is put my best foot forward and hope that others will be interested in what I have to say. For the most part, if people don’t engage they will just leave and not give it another thought. On the positive side though, if people find what you say interesting enough to want to speak to you afterwards, this a great way to tick the ‘speak to one person you don’t know box’ and as they are approaching you all you have to do is respond. I find this so rewarding, but I also appreciate how fortunate I am to have this type of opportunity and how much it helps me manage to get the most out of events.
Prepare your exit strategy
One of the important things to bear in mind, and which I often forget, is that others do not necessarily feel the same way about social requirements. I struggle when people arrange evening meals at meetings when you’re already booked to spend a full day together. I understand the purpose, it’s lovely to build bonds and memories, and logistically it’s easier. I rarely, if ever, hit the end of the meeting day and wish to spend the few hours downtime I have with others, over reading in the bath however. There are frequently times I can’t opt out of these moments, but where I can, I will often have a pre planned reason to excuse myself. Often, this is work related, as I will always genuinely need to do some email catch up, and doing this after dinner means working till midnight. I don’t lie but I may pre-plan my rationale for not being available to support both my work load and my mental well being. I will never not pre-inform, as that is rude. People will have budgeted and made arrangements, so I will never last minute drop, but if the option arises I may flag unavailability at the planning stage.
Don’t succumb to expectations and pressure
People are amazing and much more welcoming than you expect. I’m always counting myself as so fortunate is be asked to unexpected drinks, meals and catch ups at conferences. I have learnt that I need to not get caught up in the moment and end up crossing the carefully curated boundaries I have put together, in order to ensure that I can last the social distance of the conference. I’m a planner for a reason and I don’t riff off the plan well. I also struggle with saying no. This means that there have been multiple times when I’ve said yes to that dinner, or those drinks, and have then suffered the consequences afterwards. Now, I work hard to keep to my boundaries so that I don’t make life harder for myself. This can be surprisingly difficult as all these invites are inclusive and well intended, I just have to remind myself to make the sensible choice to enjoy the entire event, rather than burning out after a single evening.
Know that this is an essential part of the job, so invest in coping strategies early in your career
The truth is that networking and attending these kinds of events is essential. They are a fundamental way of hearing the latest science and expanding your knowledge. They are also key for collaboration and building your networks, as well as dissemination of your work. No matter what anyone says, I have found that science fields tend not to be meritocracies, there’s plenty of ‘who you know’ involved, and the only way to address that is to get yourself out there. So you will need to learn how to navigate these settings, and the earlier in your career you manage that, the more rewards you will reap.
I’ve talked about some of my own pitfalls and things that I’ve implemented to help me, but you will have your own triggers, and each response will need to be customised to yoi and your needs. What is true for all of us is that you are not alone, and if you are in need of someone to speak to during the horror of a break, then I am always happy to be your person. This is what I look like and I will never turn you away.
Know that it gets easier
The longer you hang on in there, the easier it gets, honestly. I haven’t walked out on an event in a decade, although the toilet hiding is still a little more frequent 🤣
Pre manage your expectations of yourself and make sure they are reasonable
Book with a group or a friend if you can to take the edge of socialising with strangers
Join a social network, as you can use it to find like-minded people, and it can give you a virtual introduction rather than the cold approach
Similarly, join a society. Societies often have small meet-ups either before events or at meetings, and so you can make connections in a smaller, less intimidating space
Submit work. It’s much less intimidating if people come and speak to you rather than the other way around
Know it’s absolutely OK to need to tap out and have your own space, but make sure this is pre-planned so you don’t miss the reason you came to the event
Right, well, having talked about the need to be prepared. I haven’t even packed yet, so I’d better get on that. If any of you are Liverpool bound, make sure you come and say hi. I’m there Wednesday and Thursday.
All opinions in this blog are my own
If you would like more tips and advice linked to your PhD journey then the first every Girlymicrobiologist book is here to help!
This book goes beyond the typical academic handbook, acknowledging the unique challenges and triumphs faced by PhD students and offering relatable, real-world advice to help you:
Master the art of effective research and time management to stay organized and on track.
Build a supportive network of peers, mentors, and supervisors to overcome challenges and foster collaboration.
Maintain a healthy work-life balance by prioritizing self-care and avoiding burnout.
Embrace the unexpected and view setbacks as opportunities for growth and innovation.
Navigate the complexities of academia with confidence and build a strong professional network
This book starts at the very beginning, with why you might want to do a PhD, how you might decide what route to PhD is right for you, and what a successful application might look like.
It then takes you through your PhD journey, year by year, with tips about how to approach and succeed during significant moments, such as attending your first conference, or writing your first academic paper.
Finally, you will discover what other skills you need to develop during your PhD to give you the best route to success after your viva. All of this supported by links to activities on The Girlymicrobiologist blog, to help you with practical exercises in order to apply what you have learned.
It has not been a great week for science, with many of us being concerned about how the presence of a vaccine denier on the successful ticket to the white house will impact public health initiatives and the quality of science communication in general. I’ve been thinking a lot about how we got here and how, even more than previously, embedding good science into mediums that are routinely accessed by the majority, will be crucial in ensuring the reach of accurate science communication when some of the more standard public health routes are bound to suffer in the coming years.
I think it will be a surprise to none of you that I am a bit of a lover of TV and movies, we’ve also covered a number of book reviews linked to this blog, and I like nothing better than snuggling down with a good book and a cup of Darjeeling. What does any of this have to do with anything? Infection, infection control, and science in general is a huge chunk of my every day, but this isn’t the case for everyone, or even most people. Many people are passive absorbers, meaning that they may not search out information but take on board when they encounter it when going about their lives. This means that the quality of what they encounter may be hugely variable, depending on how and where this happens. I’ve previously talked about the quality of the science in some of the books I enjoy, including the News Flesh series, as well as posting last week about how infection control is represented the Alien movies for Halloween. These are fun posts to do, but it made me think of the most popular movies that are linked to infection out there. How good is the science they represent? and by doing this better, could we support science literacy in general?
IMDB list of Top 25 Virus/Pandemic/Epidemic/Infection Movies
In order to think about this more detail I hit the Internet Movie Database (IMDB) which contains all kinds of lists, including a top 25 of Virus/Pandemic/Epidemic/Infection Movies (https://www.imdb.com/list/ls094715071/)
A Quiet Place (2018) (Girlymicro comment – I don’t know that this should count as it’s an alien invasion film)
Bird Box (2018) (Girlymicro comment – I don’t know that this should count as it’s an unknown enemy film that does not appear to be linked to infection)
Now, I have only seen 16/25 of these, Mr Girlymicro has seen 22/25, so between us we have most of these, so hopefully I’ll be to comment from a position of knowledge on a fair few of these. Before we even start however, as you can see from my commentary on this list, the poor science starts early during the classification of some of these as infection movies, even before we start to talk about the science content of the movie/show itself. Firstly, let’s look at the name of the list = Top 25 Virus/Pandemic/Epidemic/Infection Movies and how it related to the actual definition.
An increase, often sudden, in the number of cases of a disease above what is normally expected in a specific population and area.
An outbreak, which carries the same definition as an epidemic, but is often used for a more limited geographic area.
The CDC suggests epidemics occur when an agent and susceptible hosts are present in adequate numbers, and the agent can be effectively conveyed from a source to the susceptible hosts. Whereas a pandemic refers to an epidemic that has spread over several countries or continents, usually affecting a large number of people. The starting epidemic is usually due to a combination of factors including:
A recent increase in amount or virulence of the agent,
The recent introduction of the agent into a setting where it has not been before,
An enhanced mode of transmission so that more susceptible persons are exposed,
A change in the susceptibility of the host response to the agent, and/or
Factors that increase host exposure or involve introduction through new portals of entry
So you can see from the above that a number of movies on this list don’t actually count under the terms linked with to the title. Some of them are alien invasion, some of them are climate change related, and one is even on the topic of bioremediation. Yet there they are on the list.
For some of the others, I’ve already covered their concept during my Zombie post, so I’m not going to go through these in this blog, but focus instead on the ones that fulfill the epidemic based criteria. That said, give me a shout if you’d like a more in-depth zombie comparison post as Train to Busan is an awesome movie, and I’ll accept any excuse to re-watch it.
Let’s start at the very beginning
The first film on the list is Outbreak, a film that came out in 1995, with a description of ‘A team of Army doctors struggle to find a cure for the deadly Motaba virus that was transported from Africa to North America by a white-headed Capuchin monkey and is now spreading quickly throughout a small California town.’
This movie has an amazing cast, but I have to say I don’t want any of them in my team if it came to trying to lock down a high risk infection from an unknown source (vector). In terms of the escape monkey component. You’d think that it is far fetched, and if you’d asked me yesterday I would have said just that, but just today on BBC News there was a story on 43 escaped monkeys from a research lab in the US. So far fetched it may be, but not unheard of, in the case of vector escape.
Even if the vector component may not be quite as unlikely as I’d previously thought, I’d like to say that the rest of the practice in this is highly suspect at times. That said, I do have to admit, that I once went to a talk by a scientist who was looking for viral transmission sources of haemorrhagic fevers in Africa. They showed pictures of the table where they performed autopsies on found deceased animals in the jungle, under the same canopy as the table where they then sat down for dinner. So, as much as the way that high consequence infectious diseases (Ebola etc) are not portrayed as accurately as I’d like, maybe this is a movie of its time, as was that lecture. I really want to enjoy this movie, as it so defined how many of us had our first introduction to outbreaks and what they could mean, but almost 30 years on I don’t think I could recommend the scientific accuracy it portrays. The fact that this is still the top rated movie does not bode well for our scientific literacy hopes.
What a difference a decade makes
Almost 15 years after Outbreak, Contagion was released in 2011. This was the first of the infection movies on this list that I saw after I’d started working within Infection Prevention and Control. Contagion is described as ‘Healthcare professionals, government officials and everyday people find themselves in the midst of a pandemic as the CDC works to find a cure.’ I remember going to see this with a scientist friend and whooping out loud at the explanation of an R0, it gave me so much joy I was shushed by someone else in the cinema, to my ongoing shame.
The CDC defines an R0 as ‘The basic reproduction number (R 0), also called the basic reproduction ratio or rate or the basic reproductive rate, is an epidemiological metric used to describe the contagiousness or transmissibility of infectious agents.’ So, see if you share my joy at how the movie explains what this is, in a way that is so much more approachable than the CDC definition:
This film is not perfect, I clearly remember losing my mind about the glove use at one point, and SPOILER ALERT, it was that poor glove use that meant I was OK with one of the characters dying, but the underlying science is well explained and some of the approaches to containment and vaccination are definitely well routed in evidence. The differences in the quality of embedded science between Outbreak and Contagion are highly noticeable. Part of me wonders if some of the drivers for this heightened quality is linked to awareness of the topic due to the 2009 Swine Flu pandemic, or whether this was part of a wider shift towards improved factual grounding in these kinds of movies.
When talking to Mr Girlymicro about this movie, whilst writing this post, he has pointed out that despite my enjoyment he found it an act of ultimate depression which he will not be watching again, and that was when he watched it before the pandemic. It may therefore be, something that triggered my science joy may, in fact, be too depressing or triggering for other reasons to equate to true enjoyment for the general public. This may be an example of something that could risk being dis-engaging by being too close to the truth, despite being second on the IMDB list. Especially in a post pandemic world, this is a line that may prove difficult to walk and prove to be a barrier to movies and TV on this topic being commissioned in the short to medium term.
A completely different movie about primates
Still on viruses and re-visiting our primate theme from Outbreak comes Rise of the Planet of the Apes , which was also a 2011 release. It came out the same year as Contagion, and in the same discussion as Mr Girlymicro stated he would not re-watch that movie, for all the accuracy of it’s science, he would watch Rise repeatedly, and I can testify that in fact he has. Rise has the following description ‘A substance designed to help the brain repair itself gives advanced intelligence to a chimpanzee who leads an ape uprising.’ This is a really interesting addition to the category, as the pandemic aspects of it are mainly actually addressed in the closing credits which demonstrate how a pandemic can spread across the globe, with the film very much focused on the human (and primate) story behind the build up.
This film utilises a viral vector to try to address and revert brain abnormalities linked to Alzheimer’s, with a scientist desperately trying to find a cure for his father, whilst undertaking clinical trials on primates. Now, the clinical trial aspects of this film could not be further from the reality, and any scientist caught undertaking clinical trials and then sneaking the medication to treat their father would at best be fired and at worst been imprisoned. Somehow, because of the focus on the relationships rather than the science, the bad science in this movie bothers me significantly less than that represented in Outbreak, possibly because it feels deliberately portrayed as more like science fiction than science fact. There are some aspects of science to this one that I find interesting and like. The idea of a vaccine or medication behaving differently across species barriers is something that is interesting and could be deeply seated in evidence based plot-lines. I am aware, in this age of post truth and vaccine denial, having a film that focuses on how a vaccine or treatment could end life as we know it may not play into the goals I’m wishing to achieve using popular culture.
Let’s not forget about fungi
In recent years there’s been a rise in the quality of TV and the amount of choice has exploded, especially on streaming and other services. The switch to being able to film big budget TV over shorter film equivalents has provided storytellers with the capacity to really explore bigger and more complex tales that may not have been possible in under 3 hours.
This is last and most recent entry onto the IMDB list and is also the only TV entrant. It is our first step away from the world of viruses, into the world of mycology and all things fungal. The Last of Us came out in 2023, although it’s based on a computer game that was released in 2013. The series is set ‘after a global pandemic destroys civilization, a hardened survivor takes charge of a 14-year-old girl who may be humanity’s last hope.’ This is therefore a great combination of the way different mediums impact popular culture. The plot asks big questions about how far you would go to get a cure for the world, how much is one persons life versus the possible saving of mankind. It’s a real homage to the power that vaccination could hold to impact the world, and how when one isn’t available how desperately people might act in the search for a cure. This is the only entry on the list that came about post pandemic, and I think it is because of that (despite being a parallel to the game) that really resonates on where that desperation comes from, and despite the current vaccine back lash, shows how different outcomes could be.
The very first scenes of the series are a flashback interview from before the pandemic where a scientist talks about what they think the next bit pandemic will be, and I have to say the whole scene brings me unacceptable levels of science joy.
Anyway, this one played so much into my particular ball park that I worked with Liv Gaskill at ID Transmission on a series of articles that talked about the science behind both the Last of Us computer game and the resulting TV series, which pretty closely followed the same plot. This four part series was a real joy to be involved with and so I’m hoping that you might enjoy them too:
I wonder if fungi will be increasingly represented in this genre a) due to the success of The Last of Us and b) as viruses feel a little too close to home these days and so the fungal world might feel like a safer sand box to play around in. This could provide a safe way to have accurate science portrayal, alongside entertainment, as the real prospect of a fungal pandemic is thankfully pretty small.
A shocking oversight
We’ve reached the end of the list, but not the end of the blog post as I want to address an appalling over sight on the IMDB list, and that is the omission of The Strain on the list. This is also a TV series, where season 1 was released in 2014, covered a series of 3 books, and ran for 4 seasons. The series is described as ‘A mysterious viral outbreak with hallmarks of an ancient and evil strain of vampirism ravages the city of New York.’
The strain – episode one, season one
There are many reasons why I love this series (and at some point I should do a vampirism and infection blog to include things like Ultraviolet) is that some of the main characters are epidemiologists linked to the CDC and so some of the science exposition as part of the job based discussions is very pleasing. The other reason I like this series is there is a definite bait and switch, in terms of the causative agent, with all the initial dialogue being linked to your standard viral outbreak, with a gradual reveal that the culprit is actually a parasite. This adds a layer of interest as the approaches to dealing with transmission really start to reflect this, and provide an interesting change as the characters are also forced to pivot and discuss the differences. So, the use of a non-viral infection is not as unique as some of the coverage of The Last of Us may imply. That said, the general science outside of the epidemiology in this definitely becomes more to serve the horror plot than feasibility as time progresses.
Where are the bacteria?
You’ve survived ~3000 words of outbreak talk, covering viruses, fungi and even parasites. You may however be struck by the lack of bacterial cause in any of these listings. I’ve been thinking about this whilst I’ve been writing this blog and I’ve come up with a few thoughts as to why this might be the case:
Too close to home – many people have experienced bacterial infections themselves in their loved ones, sometimes with tragic consequences. It may be hard to therefore suspend belief enough to enjoy the offering. I wonder if this will be true to an extent for viruses now, or whether popular culture will be a safe way to explore collective trauma linked to the pandemic
Too slow – one of the features of many of the scenarios in these movies and shows is that the impact to fast and significant. This an important aspect of making events have real risk and in raising tensions. If accurately portrayed bacterial infections may be too slow in their impact OR the deterioration is so quick there is insufficient time for viewer engagement
Not dramatic enough – bacterial transmission (as described by R0) are not going to be as dramatic as their viral counterparts, so if you subscribe to ‘go big or go home’ this transmission route is probably not the one to drive a sprawling plot-line forward
Too commonly encountered – there are 101 medical shows which have bacterial infections and their consequences featured and so they may be too close to a different genre
The science is pretty hard to get right – as people are more familiar with the topic the less story flexibility there is and the greater the need to not be too jarring for those you are trying to engage. At least in the UK, many people will have been taught about Typhoid Mary and the John Snow Cholera outbreak, and so may have some familiarity. It may also be that these also make people think of the past, and this is not the feel many of these properties are trying to evoke.
So maybe bacteria are a harder sell, although I’d be intrigued to throw a little antibiotic resistance into the mix, or some bacterial toxin related drama and then see what cool things could be done as a result. Maybe that might be my future project 🙂 Let me know if you think that there is a bacterial based film/series that I’ve missed.
It’s Halloween weekend, and in previous years I’ve talked about all things Zombie and infection transmission. This year, though, I thought we talked about something a little different, infection control precautions through the lens of the Alien movie series. Most importantly, I’m going to talk about those initial interactions with the unknown that we frequently see in both these movies and in infection prevention and control (IPC), and whether we too would open the door when someone presents at the air lock?
Spoiler warning! This post is going to mention things that happen in various Alien movies. If you haven’t seen them it may, therefore, contain spoilers – the best way to deal with this oversight in your viewing (if you are concerned) is to just get out there and watch them as Alien is the same age as me 😁
This post was inspired by watching Alien Romulus again this weekend, which, if you haven’t seen it is the best Alien movie in forever.
In preparation for the cinema release I also did a re-watch of a number of the movies in the franchise. Just in case you are less familiar, and inspired to do the same, the list includes a variety of films in different sub-genres as listed below:
Whilst watching these I was struck by a number of moments that made me think about behaviours during the pandemic, but also tales of heard of some activities that occurred during the response to the Ebola pandemic and other high risk clinical settings. Not all of these moments would have been massively out of place, in terms of parallels with these films, and demonstrate that both risk assessment and clarity of thinking can be impacted and lead to responses outside of what would be normally expected.
The thing to remember is that there are usually protocols for just about everything, so most of the decision-making should occur and have been thought out long before the situation ever arises. The problems are almost always linked to human factors in the way we respond to stress and unexpected situations, and when the protocols appear to go out the window. So, just like every character and every space ship in the Alien franchise has a protocol for how to behave when they encounter new life, strange situations or sick crew members, every healthcare facility also has protocols to help deal with illnesses we see less often or that get issued when new diseases are encountered. Healthcare facilities may not have air locks, but they do have labs and isolation facilities, so the parallels may be more present than you’d imagine.
Infection is not always obvious
One of the first themes that recurs throughout all the movies is that infection is not always obvious, either to those on the other side of the air lock, or to the individuals outside waiting to come in. Infection with the parasite sometimes occurs when the stars of our show are unconscious, be that due to trauma or medical interventions, and so they are unaware of the Facehugger on character action that has occurred.
In terms of IPC the same if frequently true, both for viruses and bacteria. Some viruses have what is known as a pre-symptomatic phase, where you are infectious to others before you even know you are sick. This was a big problem in the early stages of the SARS CoV2 pandemic. Even for bacteria, when we talk about antibiotic resistant bacteria, most people are colonised and have the potential to act as silent sources without even knowing it, with only small numbers going on to develop infections.
The truth is not always apparent
Even when an individual knows that something has happened, and are aware of their close encounter with Alien kind, the truth of their scenario may still not be apparent to either them or to others. If you look at the Facehugger situation, surely once the terrifying creature has dropped off without apparent poor consequences, then everyone breaths a sign of relief and is grateful for the near miss, not knowing that this is only the beginning. When you combine this with the fact that some people will determine this to be a low risk event and therefore not want to disclose, as they are aware of the inconvenience that will result, you end up in situations where not all the information is available.
This can also be true in real life clinical situations. Patients may not know they have been exposed. Patients may also present with symptoms that they haven’t recognised as significant, or that they have risk assessed themselves and decided they aren’t concerned about and so don’t disclose. This can happen more easily they you think, especially at the start of something, where patients don’t feel particularly unwell, or they just have a couple of vesicles/small rash. In the latter stages, when patients are presenting because they feel unwell, they may be confused or not always able to accurately disclose what’s happened. Occasionally, this may be a deliberate attempt to withhold personal details, but most often it’s because they are rightly focussed on how they are feeling in the moment. Plus, if you asked me to accurately recall everyone I met and everything I ate a week ago, I’m not sure I could, even when well.
By the time you realise the condition is a threat it may already be a risk/out of control
One of the consistent themes across all of the movies is that situations get out of control before anyone truly understands the situation and the risks. It’s only when the person that you breached protocol for suddenly starts to writhe and the horror stands before you in all its glory do you truly understand the implications of the decisions you’ve made. At that point you are trapped in your glass med bay with a growing Alien and your self recriminations are not going to save your life.
This one is a rather more dramatic version of some of the conversations that happen amongst healthcare workers when you phone to give results and have conversations about whether patients had been in the right precautions and the staff member was wearing the right personal protective equipment (PPE). There have definitely been times when staff have made a risk assessment and not followed the protocols about what PPE to wear and have then responded to these phone calls with ‘what can you do?’ in relation to the exposure. Sadly, in some cases there is nothing that can be done once the guidance has been bypassed but to wait and see, which is the reason for the guidance in the first place. Fortunately, for most scenario’s in the real world, the consequence isn’t bloody horror, death and an alien threat to mankind.
Risk assessment is linked to risk management
One of the reasons that protocols are in place in the Alien movies is that someone, somewhere, has obviously recognised the risk of infection in a small contained community where everyone interacts and lives on top of each other. Even in Aliens, when you’re talking about somewhere the size of a colony, this principle stands. This is because you are unlikely to be able to access a clinical trial on a mining ship, or develop a novel antiviral on terraforming mission, even if what you’re importing is a more traditional style of infection, versus an Alien parasite. The extent of the risk mitigations needed will always align to the risk itself. If you are concerned about an introducing something that is untreatable, then your measures are going to be much more extreme than if your infection is likely to just mean someone goes to bed and takes paracetamol for a weekend. If you can’t treat, then prevention is your only option. After 9 movies there doesn’t appear to be a Xenomorph (Alien) cure and so measures taken to prevent allowing one into your space need to match the risk they present.
This approach is definitely seen in response to infection in IPC. If you have a condition that spreads easily, rapidly and can be incapacitating for a period (i.e. norovirus) then you will use a different set of precautions to those that you use to manage something which may not be as transmittable but is untreatable or has life threatening consequences such as a haemorrhagic fever. Having conversations and being open with people about the risks of getting things wrong and ensuring that individuals understand why responses are different in different circumstances are a key requirement for people working in IPC, and something I think we should all endeavour to do better at. I think the days of asking people to blindly follow protocols should probably be behind us, as I think the Alien movies demonstrate that if people don’t get the why, they often ignore some of the core components based on external drivers
So, what lessons can we learn?
Beware of acting on incomplete information
Decisions are consistently made in these movies based on incomplete information, which leads them to underestimate both risk and consequences. A great example of this is the way people use information related to the black goo, especially in Alien Romulus, maybe don’t inject yourself with a substance that doesn’t have a proper name let alone a full data set for you to understand what it does. The other thing is that information is often treated as static, and so there is very little rapid inclusion of new info, rather than being mindful of an iterative response to new data, so help constantly inform and improve your risk assessment. It’s always worth being conscious of when is enough is enough when it comes to information and decision making.
Emotions get in the way of logic
During the movie Covenant, the entire crew is made up of couples. I get this in terms of colonisation, but in terms of good decision making, and in relation to risk this is just a one way route to bad outcomes. There’s a reason that in a certain Zombie series husbands have kept their zombie wives locked in basements rather than removing the risk to them and others. There’s a reason medical professionals should not manage their loved ones. Emotions interfere with logic, and there is no way under this setting you are managing to make decisions without your emotions getting in the way. It’s a reminder that if we become aware that we are in an emotive place, it may be the time to step away and take a deep breath, before making that judgement call or even tap out entirely and allow someone more removed to take our place.
The contrast between human emotional decision making and evidence based decision making, usually undertaken by the android cast, is beautifully explored during Romulus via Andys story arch and is one of the highlights for me in terms of enjoyment.
Science doesn’t change based on how much you wish the outcome to be different
One of the reasons that emotional involvement in decision making can be so challenging is that it can interfere with perspective and accurate interpretation of risk, thus impacting risk perception. Sadly the truth that wishing does not impact outcomes is hard to argue with, but it is human to try to persuade ourselves we have more control and ability to influence the outcome than we do. Under stress, our natural tendencies towards pessimism or optimism are definitely amplified. All of this means that when there is someone at the door banging and begging to be admitted, it is easy to persuade ourselves there is a) enough time to manage to open the door safely and b) the consequences of opening said door will not be as bad as we fear. Emotions don’t change outcomes but we are almost programmed to hope that they can.
An individual will always want to be the 1 in a million
The reason someone opens the door is the same reason that when one character looks at another and utters the fateful and true words ‘it’s too late’, and it almost definitely is, neither one acts before everything gets out of control. Humans are not good at dealing with numbers and risk when they are actively involved in the situation. One of the reasons we aren’t in that we throw sentences around saying it is a 1/million chance. We, as humans, have a tendency to focus the fact that, although it is a long shot, there is a chance that things can go your way. Sadly, as someone who has experienced the opposite, where my sister died in a 1/10,000 pregnancy, someone always need to be the one. The stats work both ways, whereas most of us survive in the world by only focussing on one side of the equation. This therefore impacts our capacity to evaluate any risk in situations we are involved with. Somebody always bears the cost and few of us can bear the vulnerability of acknowledging that that somebody could be us.
The people with the most experience are not always the ones making the decisions
One of the other main themes in these movies is that decisions, when not being made by friend and loved ones, are often being made by people in positions of power, not necessarily based on knowledge or even accepting of prior experience. This works well or not so well based on how well they listen to those who do have the information to help improve their decision making. Chains of command, especially in high stakes scenarios, are not necessarily bad, as we’ve already talked about the risks linked to emotional decision making, but so much depends on how well they work and how they place value on evidence based choices rather than hierarchy.
The other theme here is the trusting of unknown sources, especially ones with no evidence of expertise, over those who have either lived experience or expertise. I think this one resonates a lot right now, when there are so many sources of misinformation out there, and so many conspiracy theories that rely on speculation and rumour. Fact checking is key, be that on a space ship or deciding on your vaccination options.
Not everyone has the same thought processes
One of the other reasons decision making goes astray in these movies is because those involved in that decision making often have undisclosed values, beliefs or drivers that are impacting their choices, and this process is not always obvious to those others involved. This is true from androids that may or may not be obviously androids and who will have programmed ‘primary directive’, as well those working for the corporation. This is interesting as they often have more complete information than the others involved, as well as seeing the situation through a different lens because of how they view the world. This means that they can see others as disposable or views risks different, as they have a set of criteria that they wish to achieve which is more than just survival. Although in clinical life the juxtaposition is rarely so extreme, the challenge of reaching alignment when people come with different world views can definitely impact shared decision making.
Smart people can do stupid things
Having said all of that, smart people can in general do stupid things, even without all of these complications. Even when the experts are the ones making the decisions they can still make the wrong ones, especially when tired, stressed, or lacking all the information. This is the reason why protocols are key, drawn up and decided upon when all of the confounders to good decision making are not present.
You need to follow the standard operation procedures
In the end this entire post has been a very very long way of saying ‘JUST FOLLOW THE SOP!’
Many of these movies but have been much shorter with a much reduced body count, if those involved had just followed the pre-established procedures laid down for their safety. Obviously, we don’t have so many Xenomorphs as a daily risk factor in healthcare, but the same is true for us. SOPs are rarely there for the sake of it, they are there to support decision making so that in times of stress or information overload, you are not having to seek extra information to support good decision making, you have it freely pre-digested and available to you. So the next time you think twice about donning that PPE or the closing that isolation room door, ask yourself ‘would you open the airlock door?’, think twice and do the right thing.
And now for something completely different
Finally, because this is something that has amused me whilst watching these films and is probably not something that I can talk about in general down the pub. The computer in the Alien movies is usually referred to as Muthur, pronounced Mother. I just want to share my joy that the analysis software that is used to help analyse 16S rDNA runs, to give you microbiome analysis i.e. tell you what bacteria are present in your sample, is called Mothur, and also pronounced Mother. I’m sure the two things have nothing to do with each other, but allow me my scientific joy that something which was so ‘other world’ when it came out to me as a scientist has the same name as something imagined from ‘another world’.
Also, if anyone needs a science advisor on their next project, give me a shout as this post has brought me much joy and I think I may have missed my calling 🙂
Many of us are coming up against a lot of challenge when we are talking to patients and the public about science right now. Post pandemic, so many people just respond that they are ‘done’ and that everything is over now. The thing is, nothing is ‘done’, we are in another SARS CoV2 wave, measles is everywhere, and Bordetella pertussis (whooping cough) has already killed a number of previously healthy children this year. Sadly, infectious diseases don’t go away when we have had enough of them impacting our lives. So what can we do? How can we have these conversations differently?
I was at RIAT (Royal International Air Tattoo) last weekend for Mr Girlymicros’ birthday, and like the scientist I am, I couldn’t help but make some time to see what their STEM (science, technology, engineering and mathematics) offering was, and I was pleased to find it was so so much larger than I had expected.
The first thing they had was an entire interactive STEM tent, called the Tech Zone, which also included an area called the Inspire Stage. This stage had full days of talks and interactive sessions covering a large range of ways to talk and engage audiences about STEM using an aviation focus.
In addition to the talks and activities, they had something I’ve never had access to before, an entire area dedicated to science planes!!!!
Spending time attending activities, talks and walking around the planes has got me thinking, what things do you need to think about if you are running an event like this? Why do they offer advantages over standard school based teaching? What could we learn in order to think about how we talk about some of our big science challenges differently, and how could this be relevant to infection prevention and control (IPC) and microbiology?
Designing your day
During an event like this, you need to know that attendance will ebb and flow. It’s before 9 and I’m the only person here at this point, but it will get really busy as the day goes on. It is important therefore to be able to flex your expectations and approaches based on who ends up in the room in front of you. You may also need to bear in mind, when designing your session, that people may turn up late or leave early to see something else, and therefore your session needs to make sense to someone who hasn’t seen it from start to finish.
Because of this drop in and out set up, you are unlikely to get to keep people’s attention for long, so you need to plan short activities or sessions. What they may look like will depend if you have a stall with people who are walking by, where you may get them for 5 minutes, or a talk with seating where you might get 20 minutes. Making any session consist of small blocks of no more than 5 minutes, will probably stand you in good stead to be able to engage whomever is there in the moment. Either way what you are planning needs to be fun, well pitched and ideally interactive, so that the audience feel like they are part of what is going on. They have a lot of options about other places they could be after all.
You need to bring people in
It’s important to acknowledge that different people are likely to want different things and ensure that you have a spread of different sessions that will appeal across different types of audiences. The Inspire stage had everything from the Red Arrows to knitting in space, and so serviced a wide audience. They also had a range of very interactive sessions, to ones that were more like interviews, and the interaction was therefore limited to asking questions. When choosing how to put together an agenda like this one, it’s worth thinking about what is going on elsewhere. The sessions with an England international rugby player and a pop star were scheduled when a lot of display teams were flying. Display teams are a big draw and so you may need an equally big draw to keep people in your tent when they could be elsewhere. You may also be less likely to schedule your interactive kids activities over a lunch time slot, as children are more likely to need to eat at a regular time and so are less likely to be available and may be less settled even if they are.
You need to know who you are trying to speak to
The other thing you need to decide when you are putting together your agenda is who you are actually trying to speak to? The age range, interests, and backgrounds at events like this are broad, and so you need to decide are you trying to appeal to everyone? In which case you will need different sessions that speak to different groups. You could decide instead to only target families, children, or students. All of these decisions are completely valid, but they need to be consciously made, as they impact on the content and level of embedded interaction which will be required.
I was speaking to Fran from Great Scott! Productions afterwards about the challenges of this, and she talked about how important it is to also allow the audience to always feel like they are slightly ahead of you. This enables them to feel comfortable and can give them the confidence to engage with interactions and ask questions. No one wants to sit through a session where they don’t feel like they know what is going on or be made to feel stupid for not following. Pitching your content correctly is super important.
Invisible or hard to understand concepts
Keeping your audience on board and following your train of thought is key. One of the great ways they did this over the weekend was by having segments that enabled the audience to visualise usually invisible concepts, such as energy use. One example of how they did this, was by using thermal detection from a plug socket using a camera to show energy in the form of heat. This is a great way to bring theory to life and an approach we can think about in terms of how it is applicable to infection. So many of our challenges are invisible and, therefore, hard to cognitively tackle. Making the invisible visible is a great starting point when talking about topics such as antimicrobial resistance or vaccination.
Demonstrate diversity and break down stereotypes
Many children are put off engaging in STEM topics because they don’t see reflections of themselves in the people they see talking about these subjects on TV or in the movies. Historically, there have been a lot of white men occupying this space. Events like this are a great chance to break down some of these stereotypes in order to show that anyone can undertake any of these careers. To allow people to feel seen.
My two minor niggles with the agenda for this event were that the main pull was occupied by interviews between white men. I get why. I get that you need your big ticket numbers to compete with the outside draw. I do think they could have sandwiched a session demonstrating diversity and inclusion between them. This would have meant this session may have had a bigger audience than might have been achieved otherwise, and therefore supported impact. My other comment was that, although gender diversity felt well represented, I’m not sure other diversity aspects were. That being said, I know how hard it is to get this balancing act right, and some of your speakers are always based on your networks, so it is not easy to achieve.
Engage parents as well as kids
Running events, like Reach Out for Healthcare Science, has made me aware that even when targeting events at children, it is so important to include parents in the conversation. Parental influence on career choices are really strong, and you can inspire someone, but if their parent doesn’t know what that career looks like, it can lead to nothing. Having interactive areas that include careers information to also get parents onboard can mean that you impact in a longer term way.
To a certain extent, at an air show, you probably have a lot of low hanging fruit to talk about careers in aviation, but they can also lead to wider conversations about engineering in general, or other sciences. It is a great place to have the ‘have you thought about’ conversation in order to expand horizons. It is a good idea that you have hand out material that can also be engaged with by the adults, as well as those aimed at students or different age groups attending.
Provide an idea of a day in the life
One of the great ways that RIAT helped with discussion linked to careers was in the science planes area. They not only had the planes to look at, but they had signage and stands where you could talk to scientists and pilots about what a career in this area actually entailed. They used a super cool draw to get people in and then offered them the level of detail they were happy to engage with.
I think this is so important as there are a lot of misconceptions about what a career in STEM actually looks like, and there are limited opportunities for many people to actually sit down and talk to someone who does it for a living. This informal setting means that people can ask any questions they want without having to put their hand up in front of a lot of other people or deal with a scrum to get to the front of an activities queue.
Photo credit Jon Cloutman-Green
So, RIAT had a lot of cool ideas that we can use to think about designing our activities and agendas in order to talk to people about STEM, but what does it engagement on this scale offer that we can learn about in terms of thinking about the benefits with partnering our STEM offerings with large scale events?
Provides access to non-standard audiences
RIAT has a massive attendance with 80,000+ people on the day I was there, and over 200,000 over the weekend. There are very few face to face events with the possible level of reach that RIAT offers, although there are others like Glastonbury, where STEM can be and sometimes is embedded. The advantage of these events is not just numbers, it’s the fact that some of this audiences may not engage with other types of STEM engagement, such as visits to science museums or festivals. This means there is a massive opportunity to raise awareness and engage with audiences that may not normally feel like these events would be ‘for them’ or something they would seek out. It gives opportunities to drop by taster experiences without requiring any huge amount of commitment or pre-existing level of interest. Yet these small encounters can really alter individual trajectories and change lives.
Photo credit Jon Cloutman-Green
Routes to talk about the big issues
One of the other things these kinds of events can enable is access to conversations about pretty big issues. Climate change was a big topic of discussion at RIAT because of the fact that it was linked to aviation. This led to lots of interesting talk about how bio fuels are a scientific and engineering solution to a number of aviation associated climate change issues. One thing that I found really interesting was the use of virtual flight and simulation training as an alternative to standard ‘in air’ flight training for the RAF. It was quoted that 50% of the flights taken by the RAF are training flights, and so the ability to use non-airborne alternatives provides great opportunities to reduce carbon emissions and impact climate change risk.
I think there is so much that could be taken away from the way these interactions were undertaken to think about how we could discuss big issues in IPC and microbiology, issues such as antimicrobial resistance. My main takeaways from those activities I attended included:
embedding discussion of the big issues within wider activities
make references present but not preachy
ensure that message is about empowerment and change, rather than catastrophe and fear
discuss how individual actions can be taken
focus on how STEM can change things for the better
spring board from subjects that you know the audience are already interested in
I would love us all to be inspired by these offerings and really start to think of other spaces we occupy in our non professional lives where we might be able to talk about bringing STEM in, either as part of collaborations or driven as individuals. So, if you have any ideas, or places where I could help, please please reach out and talk about how we can bring our whole selves to these spaces with the aim to inspire and help others to feel seen. To help the next generation access careers that we know are exciting, creative and impactful. To create an inclusive legacy and safe space where stereotypes don’t define who gets to access STEM professions. To leave the profession that much better than we found it.
In the mean time, whilst I cogitate on how to do all of this better, one the other great things about attending these events is that you also get to partake in the wider wonderful offering, and even when it rains, there’s are plenty of planes and tea to bring you joy. Here’s to more STEM activities on the big stages and sharing the joy of embracing science as part of your life!
It’s not something that comes up in conversation on this blog very often, but I’m a bit of a swifty. Watching the Taylor Swift in the Reputation concert video is a happy place for me, I often watch it on my commute when I’ve had a challenging day, and the music forms a staple of my ‘get psyched’ mixes, along with a fair share of rock and big band music.
Now, for those of you who have yet to discover this particular joy, there is a speech she makes linked to why we worry about how we are perceived and the impact of having a ‘bad’ reputation that really lands with me:
“For example, having a bad reputation in our mind could get in the way of finding real friendship, real love, real acceptance, people you really fit in with because you think what if they have heard something about me that isn’t true, what if they’ve got these preconceived notions about me that they heard from gossip and then they never want to meet me and then we’ll never know what could’ve happened,” she continued. “And I think that’s why some of us…meaning if not most or all of us are sort of afraid of having a bad reputation because we’re so scared of something fake, like gossip, or a rumor about you or a name you got called getting in the way of you finding something real. And so, when it comes down to that fear and that anxiety, it’s just all really delicate,”
Taylor Swift – Reputation Tour 2018
There are many forms of reputation:
Personal
Professional
Organisational
I think there are a couple of reasons why anything that impacts reputation is so powerful. The first one is that both trust and reputations take a long time to build and can be destroyed in the blink of an eye, depending on the scenario. Another is that, I believe, at the core of our being most of us want to be liked, and having someone affecting how we are perceived can directly impact on that. Finally, it is difficult to know how to respond to situations that influence our reputations. We say ‘stick and stones may break my bones, but words shall never hurt me’, implying we should rise above it, but we also say ‘no smoke without fire’, implying there is a burden of proof upon us to correct what is being said.
I think, depending on who you are and the circumstances, the impacts on different types of reputation may not feel equal. Now, I went to a girls school, and one of the reasons I’m glad to no longer be a teen or in my twenties is because I’ve learnt and grown so that personal reputational attacks in general have a lesser impact on me. I would love for everyone to like me, but I know the reality is that this will never be the case. Although often highly impactful, personal reputation attacks can often be dealt with by removing the individual from your social circle. You often have the choice to interact or not, and the other members of your circle often know you well enough to not listen too closely.
What I have found more challenging are circumstances that impact my professional reputation. For a self declared people pleaser, like me, the thought that someone could lead you to be a scenario where you were perceived to be difficult, mean, or destructive, is particularly stressful. This is doubly so when you have a very particular set of values, about being collaborative, supporting others, opening doors, and being patient focused, and the commentary indicates you are anything but.
There’s a movie I love called Gossip, most people have never heard of it. It starts with a group of college students running an experiment where they create some untrue gossip and then track how far it spreads, how it evolves, and the impact. Needless to say, it doesn’t end well. Now, I’m as guilty of gossip as the next person. We all want to feel in the know and to almost feel special by knowing something others do not. There’s a bunch of research about why this is. Gossip in real life, just as in fiction, isn’t harmless however.
Although gossip is bad enough, I feel there is also a significant difference between gossip and the escalation to deliberate character assassination or attempts to damage the reputation of another person. The weaponisation of reputational attacks, or even the threat of them to gain leverage, can be one of the most stressful things I’ve encountered in my professional career. Partly because they tend to come as a complete surprise to those targeted, but also because it’s difficult to know how to respond whilst in the midst of it. I’ve seen this happen to others and been a (somewhat) minor victim myself. Having hopefully come out the other side, I wanted to capture my thoughts for anyone caught in a similar situation in the future.
You may not escape the fallout
The first thing to say is that I am always a fan of taking the high ground and not engaging. Engagement can just end up adding energy to the situation rather than letting it burn out. It is important to note that taking this sensible higher ground approach may not mean you escape reputational damage, however, at least in the short term. You need to be aware of the fact that a time may come when you do have to address what is happening, and you may need to have a plan for how you will do so. Hopefully, it will never get to that point, but like with many things in life, preparation is key.
You have to remember the long game
One of the reasons to start out with a policy of none engagement is that most of the time, this will just turn out to be a blip and nothing more. Something you will look back on in a few years, possibly sigh, but see as a learning experience and nothing more. Professional careers span decades. Sometimes, it’s very easy to be caught up in the now rather than seeing it in that context. No matter how bad it feels in the moment, you need to ask yourself: how will this feel in 6 weeks, 6 months or 6 years? Very often, with the distance of time, it won’t feel anywhere near as bad, and that is the context you need to hang onto.
You have to faith in those that know you
It can be pretty shocking when you first hear reports of things being said that could impact how you are seen by others. It can be easy to feel like you should rush in and respond, but as I’ve said, for many reasons that is unlikely to be the best option. During what can be an unsettling time, it is important to remember that nothing really has changed. You have had professional relationships with many people ahead of this moment, relationships built on mutual trust and respect. These relationships haven’t changed, and you have to have faith in those people who know you and know the value you hold. Never let a single moment devalue everything you have already built.
You have to believe in the system
We work within systems, systems that provide individuals with routes for escalation and complaint. It’s incredibly important that everyone has the opportunity to feel heard. Everyone has their own perception that is unique to them, and those perceptions are real, even if they don’t match our own. This can be hard to accept when that variance in perception means that we feel attacked, or worse than that, if it feels that there are other drivers behind the responses that mean they are less genuine. The harsh truth is that it doesn’t matter. The system is set up, crucially, so that individuals can pursue making complaints, and this is an essential part of parity and fairness. If actions are taken that are erroneous, you have to believe that the requirement for evidence and facts count. That truth will out. Even if it takes a little time.
You have to try and not get sucked into the whirlpool
Whilst rumours/gossip/complaints are swirling it can be easy to get sucked into the drama and the emotions of it. It can be easy for those voices to be the voices that you carry with you and for you to only hear them in your head, not the ones of those that support you. To focus on the negative, the stress and the fear that comes from a lack of control. It’s hard, but none of this is useful to you. If you can’t find a way to put it in a box and distance yourself from it, it will be all you see and experience. This can really start to impact how your interact with the rest of your working life, or even how you feel outside of work. You need to make a deliberate effort to not engage with the whirlpool and to maintain your sense of self.
You have to control your own responses
Part of not engaging is making sure you retain what control of the situation you can. In the end, the only thing we can ever truly control is how we respond. You have no control over how others perceive you, you have no control over their actions, or what they say. You can absolutely decide how you react to that stimuli. It is all too easy to let the fear associated with being unsettled lead to responses that are seated within that fear, or to appear angry and let that drive our interactions. Those kinds of responses aren’t helpful however, in fact they just add fuel to the fire. You have to be aware, that if not careful, you can end up with a self fulfilling prophecy if you lose control, becoming what you are accused of.
You have to keep being authentic
For me, some of the worst reputational attacks, are those that attack us around those values that we use to define ourselves. Calling us self interested, when our focus is on parity and fairness, calling us unsupportive, when we believe in lifting others. These may not seem so significant in the scheme of things, but when those things you prioritise and use to define yourself, are the things that are under attack, it can feel incredibly personal. From what I’ve seen, responses to this tend to go one of two ways. First, people stop undertaking some of the associated activities, as they fear further attacks or putting their head above the parapet. Or, second, they change the way they do it, through anxiety or fear. Now, I’m not saying changing is bad, but I think it needs to be based on genuine reflection, rather than in response to negative emotions. I think stopping, in some circumstances as a temporary measure, is a wise choice, but it shouldn’t be the long term solution. It’s important to not allow circumstances to change who you are and your values.
You have to find your support systems
All of these aspects can be highly challenging, and to be honest you are not going to be able to navigate this on your own. You will need support, you will need help to undertake reflection, you will need an external view point to aid you to sense check and evaluate responses. Feeling personally attacked can really throw off your sense of inner balance, and you will need other people to help you find and retain the sense of self that you need to traverse what is happening. I think you need to find people from your professional context, as well as your personal, so that you have people who know you, all of you, as well as people who know the players and the landscape in which this is all playing out. It can be easy to want to ostrich, whereas, in reality, what you need to do is use those connections and networks you have to be able to understand what is really going on. Word of warning here, I am not suggesting you go out and start talking to everyone about what is happening, or the person who is doing the talking, that would be as bad as the initial reputational attack. I’m talking about having a few key supports where you can safely and openly talk about how you feel and what’s going on.
You have to make the sensible choices
I’ve said to not engage, but I’m not saying to be foolish and ignore what it happening. I’ve already talked about the fact that you function within a system, with processes and requirements. The first thing you should do is really learn about what those processes look like. What are the requirements upon you, what kind of evidence may be required. Have you encouraged reporting/escalation? Have you referred to occupational health? Have you offered alternative lines of reporting/management? Have you spoken to your line management or HR to confidentially gain advice? You may not need to do anything complex, it could be as simple as recording meeting content in emails, or not meeting 1:1. Seeking advice however is key, as these scenarios can also be complex, dependent on whether the person is in your organisation, a direct report, a peer, all of which impacts the information you need. You need to know enough to make sure you are making sensible choices to protect yourself and that you are acting proportionately and appropriately.
You have to check what is perception and what is reality
It can be easy, when you feel like the rug has been pulled from under you, to lose your sense of what is real. The resulting self doubt can make you question every interaction you have. Paranoia can set in and it can colour the way that you see the world. It can also colour your perceptions of your interactions with those associated with the commentary that is currently ongoing. You can’t let this happen. You need to find strategies to manage this, otherwise you will read negativity into everything. This is another reason why being sensible and not having 1:1s, or having email confirmation of any discussions, can be helpful. You can get a neutral opinion that gives context to interactions, and written communication can be helpful to ensuring shared understanding. As the emotions can spill over into other spaces, you also have to check yourself more widely. If you are like me, you can be sent into a spiral of being hyper critical about yourself, and this can colour your perceptions. Awareness is part of the challenge, and if you can become aware of how you are responding, and how that might impact on the lens through which you are seeing your interactions, you can start making proactive steps to adjust appropriately.
When it is over you have to let it go
You will get through this situation, you will come out the other side. No matter what the outcome, this isn’t forever. It can leave you with a certain amount of trauma, or a changed view of the world, or level of trust. That’s understandable, I get it, depending on what has happened the personal cost can be significant, even in just emotional impact. The thing is, despite recognising this, you have to let it go. You need to take the learning, and grow, without letting it fundamentally change who you are. You can’t become less trusting, or have less faith in people, there wasn’t enough of both of those to start off with and the world can’t afford for us to have less. You have to move on, wiser, but fundamentally unchanged. So deep breaths, take one day, one hour, or if needed one minute at a time. Keep the faith, and the world will turn out OK.
I was presenting at my first conference of the year last week, which is a sign that conference season is soon to well and truly kick off. I know that this often puts many of us in a state of anxiety. We know that conference presentations are important for both getting our work out there and also for personal and career development. Presenting however, can feel like quite a high stakes manoeuvre, especially if you are not comfortable with public speaking. With this in mind I thought it might be useful to share some tips that I have learnt, in the hopes that it might help with your next upcoming session.
1 – Know your audience
The first thing to realise is that we often make presentations about us, when actually they aren’t really about us at all, they are about the audience and what we are trying to achieve on their behalf. We are often given a fairly generic topic to speak on, or have submitted an abstract of what we wish to present. That’s great but actually probably doesn’t have enough clarity to start putting together the session. My first step whenever I’m asked to speak is to think about the learning objectives for the session. What might benefit the audience most? What are they expecting? Learning objectives act as a guidepost, and I will usually include them with the blurb I’m asked to write for the agenda. This means that people selecting their sessions will be able to make an informed decision about whether your session will work for them. Are you pitching an introduction level session or an update on the latest research that assumes pre-existing knowledge? You want to match your pitch to the audience that you are expecting.
It is also worth thinking about what kind of atmosphere is likely to be present? Is it a fairly informal setting where the session will be more discursive or is it a formal conference session where you may need to prepare for possible confrontational questions? Prepare for questions and queries whilst you’re preparing your session, try to think about the rabbit holes that the audience might want to go down and for any potential pitfalls where you will need to have a pre-prepared strategic response. If you’ve been clear about what the session covers and audience pitch this should be less of an issue, but it’s always worth being prepared.
2 – Be prepared to bring your authentic self
One of the things I’ve come to truly believe is that, no matter how formal the session, you should bring your whole self to it. I’ve written previously about how we should feel free to wear clothes that empower us, and conference sessions are no different. This can be something as simple as wearing your favourite colour, but whatever it is, delivering talks is easier when you feel good and empowered so do whatever you need to feel that way. My top tip is that whatever you decide to wear, ensure that it’s comfortable. I used to wear heels to speak but now I always wear flats, as I’ve decided that the pain isn’t worth it for me, especially when you consider how long you will be networking after your session.
The other place were I try to ensure that I also include something that is a little bit me, is within the presentation itself. Again, this can be levelled dependent on setting, sometimes I just choose a colour scheme or icon that speaks to me. Other things you can include are quotes or images that are meaningful to you. Again, it doesn’t have to be something big or in the face of your audience, but something that centres you and makes you feel more like you own the space you are presenting in. Sometimes however going big is the way forward, sometimes making something memorable is the right approach, it all depends on your confidence level and the setting.
3 – Judge your session
I’ve talked up above about thinking about how informal/formal the setting you are presenting in and how this can impact on your content. There are however other things that are beneficial to think about in terms of expectations for your setting. The type of session will dictate a number of things, as will time slot and room allocation. If you know the venue you are going to you may be able to predict numbers of attendees for instance, if you are allocated a room you may be able to find out whether its for 15 people versus 1500. High numbers of attendees will limit your options for interactions, as will being given a 15 minute time slot.
Common types of sessions include:
Debates
Research presentations
Topic presentations
Workshop
Plenary or keynote
Speed presenting
Poster presentation
Careers presentations
Panel sessions
There are obviously others but these are the main ones that spring to mind. Just from looking at the list you’ll be able to see how different ones will attract people with different levels of pre-existing knowledge or interest. There are some key questions that are worth asking to help you support judging your session when the email comes in. First, always confirm length of session and whether or not this will include time for questions. Second, ask about number and types of attendees both for your session and the target audience for the conference/meeting itself. Finally, as this will impact your options for engagement with large audiences, will there be free Wi-Fi available for attendees so they can access voting apps? Don’t feel like this information should confine your creativity and what you want to undertake but build any limitations into your thinking in order find solutions ahead of time. Finally, please please please never be the person that delivers a 40+ minute talk despite being given a 30 minute slot.
4 – Use the agenda to guide you
Once the agenda is released and you’ve starting to build the content of your session you can also use it to help in your preparation. Your timing and position on the agenda can influence the build of your talk. If you are directly after lunch, you might want to think harder about the engagement side to wake everyone up and get them back into the flow. If you are just pre lunch, you might want to stack some of your more exciting parts towards the end and build towards them to ensure you keep the audiences attention. If you are going first or last you probably need to start and finish with a bang.
The other area where the agenda can really help you is to see what others are covering, especially if they’ve listed any focuses or learning objectives in their descriptions. This may mean you can get valuable slides back if someone is talking on a similar topic ahead of you, and will therefore have given a lot of similar introductory slides, thus giving you more time to build on the subject in your slot. It can also give you ideas of areas to avoid, so that you don’t give too much overlap. One of the things to not do is be intimidated by anyone else on the agenda. If you are speaking/presenting you have earned the right to do so, it doesn’t matter if the person before you is Dame X or Professor Y, acknowledge what that might do to the atmosphere in the room (i.e. may mean you have a larger audience) and then plan as if they were any other speaker.
5 – Have a plan on how to engage attendees
Engagement can start before the event even begins. If you have a poster session for instance, you might want to share a picture of your poster and it’s location on social media. Sometimes I also find running polls can help with working out pitching your session, and also in building engagement so that you are more likely to get an audience. This can be especially important if your session is at an event where there are multiple sessions running at the same time and therefore you almost need to sell why someone should comes to yours when there is so much choice available. Taking some time to raise awareness via social media using the event # can be really beneficial under these circumstances.
Depending on the availability of Wi-Fi and session details you may also want to consider using tools or apps to support interaction with the audience during your session. You can use tools such as Mentimeter and Slido to build voting or other forms of interaction into your session. This approach is especially important if you are asked to do a workshop session. It’s also worth asking additional questions during the prep phase, such as the type of seating, to see whether it would support group discussions.
Even if you are giving a standard presentation without interactive tools you still need to think about how to engage your audience. There obviously many different ways of doing this, starting from basics like pitching correctly so you bring your audience with you. If you can bringing yourself to your session by using framing such as story telling it can really help, alongside the use of humour. You can even think if there are props that would be appropriate to support what you’re talking about, although you also don’t want to make it gimmicky. Whatever tool you feel comfortable with, practice using it as it will make sure your session is more memorable.
6 – Make sure you have a plan B
Things go wrong, they do, despite your very best endeavours. Having a plan B in your pocket never hurts. This can be as simple as having a USB with your slides on it with you in case they haven’t managed to load it before you arrive. If I’ve included videos or anything else ‘fancy’ in my presentation I will always have a plan B and C. Plan B is an extra copy of my talk without the ‘fancy’ bit in it in case it doesn’t work when I test with the AV tech ahead of my talk. Plan C is a script in my head that I can use to describe the video in case it worked on test and suddenly fails during the real thing. If I’m doing a smaller session, I will also sometimes arrive with print outs of my slides so that I can approach it old school if needed.
Having a plan B is especially important if you are using voting or something tech related. If your entire session is going to be based on audience participation you need to have a plan if no one there can get signal or access to Wi-Fi. It’s worth building this flexibility in when you are developing the session so you will not need to entirely wing it if the unexpected happens to you.
7 – Be prepared to push yourself
I’m just throwing this out there. You should be prepared to push yourself into a space where you feel uncomfortable. Growing your skills is a never ending task, even if you feel like you are a pretty good public speaker, there are always things to learn, improve and do better. Sometimes the very act of speaking is a sufficient push because it’s not an area in which you feel comfortable. If you are comfortable talking ‘science’ maybe also stretch yourself by bringing more of yourself into the session. Embrace the creative possibilities and strive to have more impact, build better engagement, be more memorable. Read and research on the topic of how to present better in the same way that you would read and research your content and find inspiration about the next thing you could try.
8 – Facilitate a relaxed state of mind
Having just encouraged you to step out of your comfort zone by planning your presentation I also now want to encourage you to remove the stress that can be present outside of the speaking component itself. I speak from experience. I once agreed to speak at 2 conferences on the same day, on different topics and in different cities. This was beyond foolish. There simply wasn’t enough time to get from point A to point B and I arrived to land on stage for the second session with 1 minute to spare. I’ve also learnt that travelling up on the day of a session doesn’t work for me, it just makes me too stressed. I now will always travel up the night before, even if I arrive really late, because then I can go to sleep knowing that I’m where I need to be rather than lying awake all night stressing about whether an act of god will stop me making it to my session.
I also comfort myself by reading up on the areas that I have identified during my gap analysis that I might get questions linked to, or to reassure myself – even if it’s a topic I know really well – that I have up to date information and references. Feeling like you are walking up to a podium prepared is the best way I have to remove any of my stress linked to presenting.
9 – Plan to do your own timing
This is one I have learnt the hard way. I don’t like clocks present in the corner of a screen when I’m presenting as I want to be looking out at the audience and connecting when I’m speaking not constantly looking down at a monitor, probably slightly influenced by the fact that I don’t use notes as it enables me to feel more organic. I know some of you will feel differently. I’ve learnt to manage this by having a phone with a big clock (on silent) with me when I present so I can see it as I move around. I know that there will often be Chairs or speakers who will signal when you have 5 minutes left. I personally find that I need to pace my session throughout, as otherwise at 5 minutes I could be left with waaaay too much to cover, and so I like to time check myself. The final reason I do this is that I have been caught out. I’ve turned up and started a presentation and realised there was no clock or timing device visible anywhere. The panic, for me, at that point is real people, it’s a real stressor for me. You may have a different thing that triggers you, but once you identify what it is, do your best to have a plan to redress it so it doesn’t distract you from the moment you are in.
10 – Use the opportunity to build your networks
This last one I think is really important, if you are given the opportunity to have a platform use it! No matter how nerve racking it is, no matter how much you may not like presenting. In fact, if this is not your naturally comfort zone all the better, go out and seek opportunities that enable you to do it more. With practice comes familiarity and skill development. Don’t feel alone in your discomfort, but do know that there will be something in you that can inspire and give confidence to others. The world needs to see more people like you, whomever you are, especially if you have the courage to bring some of yourself to the podium. There is not enough diversity present on agendas and that is something that needs to change, and we need to have the courage to do that together as a collective.
The other thing to bear in mind is that so much within health and science is dependent on who you know. It’s probably not fair but it is true. Connections and networks are where you gain invites and opportunities, and presenting and meeting people is a big way to build these relationships. Whether you do this by following the hashtags for the event on social media, by speaking to those presenting or partaking in networking and social events at the meeting, networking is key. For those of you, who like me, find networking challenging I’ve previously written a post which I hope might help, but presenting is often an easy way to do it as people will come to you and you already have a shared interest through the topic. Whatever your level of networking comfort it’s worth putting in some time ahead of the event to think what your strategy might be, and who you might want to catch up with.
I really hope that this post will help support you, no matter how many presentations you’ve done, to bring a little bit more of who you are to the room you are presenting in and to be a little bit braver in some of the choices you make when developing sessions. I also hope that by sharing some of the learning I’ve gained by making mistakes, or making life harder for myself, that you won’t make the same ones. If you have any other top tips that you’ve gained to support presentation preparation then please do add them in the comments. See you at the podium!
All opinions in this blog are my own
If you would like more tips and advice linked to your PhD journey then the first every Girlymicrobiologist book is here to help!
This book goes beyond the typical academic handbook, acknowledging the unique challenges and triumphs faced by PhD students and offering relatable, real-world advice to help you:
Master the art of effective research and time management to stay organized and on track.
Build a supportive network of peers, mentors, and supervisors to overcome challenges and foster collaboration.
Maintain a healthy work-life balance by prioritizing self-care and avoiding burnout.
Embrace the unexpected and view setbacks as opportunities for growth and innovation.
Navigate the complexities of academia with confidence and build a strong professional network
This book starts at the very beginning, with why you might want to do a PhD, how you might decide what route to PhD is right for you, and what a successful application might look like.
It then takes you through your PhD journey, year by year, with tips about how to approach and succeed during significant moments, such as attending your first conference, or writing your first academic paper.
Finally, you will discover what other skills you need to develop during your PhD to give you the best route to success after your viva. All of this supported by links to activities on The Girlymicrobiologist blog, to help you with practical exercises in order to apply what you have learned.
I adore Christmas, it’s one of my favourite times of the year. I meant to get this one out before Christmas, but to be honest, I was too busy having family time. For those of us working or looking for some fun reading between Christmas and New Year I thought this one might still be of interest.
Every year the British Medical Journal have a wonderful tradition. They post some free to access journal article. Now, these aren’t just any journal articles. They apply serious scientific processes to brilliant topics, such as the disappearance rates hard vs soft centred chocolates in ward environments presented as an observational study.
These articles always bring a smile to my face, and if you’re looking at an entertaining way to learn more about scientific processes or scientific writing these are a great place to start. I hope you’ll feel the same when you have a read of some of the ones linked to below, and know that there are more out there if you want to journey down this particular rabbit hole.
Merry Christmas, and thank you so much for spending another year in the company of the Girlymicro blog!
Objectives To determine the overall rate of loss of workplace teaspoons and whether attrition and displacement are correlated with the relative value of the teaspoons or type of tearoom. Design Longitudinal cohort study. Setting Research institute employing about 140 people. Subjects 70 discreetly numbered teaspoons placed in tearooms around the institute and observed weekly over five months. Main outcome measures Incidence of teaspoon loss per 100 teaspoon years and teaspoon half life.
Results 56 (80%) of the 70 teaspoons disappeared during the study. The half life of the teaspoons was 81 days. The half life of teaspoons in communal tearooms (42 days) was significantly shorter than for those in rooms associated with particular research groups (77 days). The rate of loss was not influenced by the teaspoons’ value. The incidence of teaspoon loss over the period of observation was 360.62 per 100 teaspoon years. At this rate, an estimated 250 teaspoons would need to be purchased annually to maintain a practical institute-wide population of 70 teaspoons.
Conclusions The loss of workplace teaspoons was rapid, showing that their availability, and hence office culture in general, is constantly threatened.
Objective To investigate whether sleep deprived people are perceived as less healthy, less attractive, and more tired than after a normal night’s sleep. Design Experimental study. Setting Sleep laboratory in Stockholm, Sweden. Participants 23 healthy, sleep deprived adults (age 18-31) who were photographed and 65 untrained observers (age 18-61) who rated the photographs. Intervention Participants were photographed after a normal night’s sleep (eight hours) and after sleep deprivation (31 hours of wakefulness after a night of reduced sleep). The photographs were presented in a randomised order and rated by untrained observers. Main outcome measure Difference in observer ratings of perceived health, attractiveness, and tiredness between sleep deprived and well rested participants using a visual analogue scale (100 mm).
Results Sleep deprived people were rated as less healthy (visual analogue scale scores, mean 63 (SE 2) v 68 (SE 2), P<0.001), more tired (53 (SE 3) v 44 (SE 3), P<0.001), and less attractive (38 (SE 2) v 40 (SE 2), P<0.001) than after a normal night’s sleep. The decrease in rated health was associated with ratings of increased tiredness and decreased attractiveness.
Conclusion Our findings show that sleep deprived people appear less healthy, less attractive, and more tired compared with when they are well rested. This suggests that humans are sensitive to sleep related facial cues, with potential implications for social and clinical judgments and behaviour. Studies are warranted for understanding how these effects may affect clinical decision making and can add knowledge with direct implications in a medical context.
Objective To quantify the consumption of chocolates in a hospital ward environment. Design Multicentre, prospective, covert observational study. Setting Four wards at three hospitals (where the authors worked) within the United Kingdom. Participants Boxes of Quality Street (Nestlé) and Roses (Cadbury) on the ward and anyone eating these chocolates. Intervention Observers covertly placed two 350 g boxes of Quality Street and Roses chocolates on each ward (eight boxes were used in the study containing a total of 258 individual chocolates). These boxes were kept under continuous covert surveillance, with the time recorded when each chocolate was eaten. Main outcome measure Median survival time of a chocolate.
Results 191 out of 258 (74%) chocolates were observed being eaten. The mean total observation period was 254 minutes (95% confidence interval 179 to 329). The median survival time of a chocolate was 51 minutes (39 to 63). The model of chocolate consumption was non-linear, with an initial rapid rate of consumption that slowed with time. An exponential decay model best fitted these findings (model R2=0.844, P<0.001), with a survival half life (time taken for 50% of the chocolates to be eaten) of 99 minutes. The mean time taken to open a box of chocolates from first appearance on the ward was 12 minutes (95% confidence interval 0 to 24). Quality Street chocolates survived longer than Roses chocolates (hazard ratio for survival of Roses v Quality Street 0.70, 95% confidence interval 0.53 to 0.93, P=0.014). The highest percentages of chocolates were consumed by healthcare assistants (28%) and nurses (28%), followed by doctors (15%).
Conclusions From our observational study, chocolate survival in a hospital ward was relatively short, and was modelled well by an exponential decay model. Roses chocolates were preferentially consumed to Quality Street chocolates in a ward setting. Chocolates were consumed primarily by healthcare assistants and nurses, followed by doctors. Further practical studies are needed.
Objective To detect and localise the Christmas spirit in the human brain. Design Single blinded, cross cultural group study with functional magnetic resonance imaging (fMRI). Setting Functional imaging unit and department of clinical physiology, nuclear medicine and PET in Denmark. Participants 10 healthy people from the Copenhagen area who routinely celebrate Christmas and 10 healthy people living in the same area who have no Christmas traditions. Main outcome measures Brain activation unique to the group with Christmas traditions during visual stimulation with images with a Christmas theme.
Methods Functional brain scans optimised for detection of the blood oxygen level dependent (BOLD) response were performed while participants viewed a series of images with Christmas themes interleaved with neutral images having similar characteristics but containing nothing that symbolises Christmas. After scanning, participants answered a questionnaire about their Christmas traditions and the associations they have with Christmas. Brain activation maps from scanning were analysed for Christmas related activation in the “Christmas” and “non-Christmas” groups individually. Subsequently, differences between the two groups were calculated to determine Christmas specific brain activation.
Results Significant clusters of increased BOLD activation in the sensory motor cortex, the premotor and primary motor cortex, and the parietal lobule (inferior and superior) were found in scans of people who celebrate Christmas with positive associations compared with scans in a group having no Christmas traditions and neutral associations. These cerebral areas have been associated with spirituality, somatic senses, and recognition of facial emotion among many other functions.
Conclusions There is a “Christmas spirit network” in the human brain comprising several cortical areas. This network had a significantly higher activation in a people who celebrate Christmas with positive associations as opposed to a people who have no Christmas traditions and neutral associations. Further research is necessary to understand this and other potential holiday circuits in the brain. Although merry and intriguing, these findings should be interpreted with caution.
Objective To determine whether artificial intelligence (AI) can generate plausible and engaging titles for potential Christmas research articles in The BMJ. Design Observational study. Setting Europe, Australia, and Africa. Participants 1 AI technology (Generative Pre-trained Transformer 3, GPT-3) and 25 humans. Main outcome measures Plausibility, attractiveness, enjoyability, and educational value of titles for potential Christmas research articles in The BMJ generated by GPT-3 compared with historical controls.
Results AI generated titles were rated at least as enjoyable (159/250 responses (64%) v 346/500 responses (69%); odds ratio 0.9, 95% confidence interval 0.7 to 1.2) and attractive (176/250 (70%) v 342/500 (68%); 1.1, 0.8 to 1.4) as real control titles, although the real titles were rated as more plausible (182/250 (73%) v 238/500 (48%); 3.1, 2.3 to 4.1). The AI generated titles overall were rated as having less scientific or educational merit than the real controls (146/250 (58%) v 193/500 (39%); 2.0, 1.5 to 2.6); this difference, however, became non-significant when humans curated the AI output (146/250 (58%) v 123/250 (49%); 1.3, 1.0 to 1.8). Of the AI generated titles, the most plausible was “The association between belief in conspiracy theories and the willingness to receive vaccinations,” and the highest rated was “The effects of free gourmet coffee on emergency department waiting times: an observational study.”
Conclusions AI can generate plausible, entertaining, and scientifically interesting titles for potential Christmas research articles in The BMJ; as in other areas of medicine, performance was enhanced by human intervention.
Objective To examine the effect of a (fictional) doctor working during the festive period on population health. Design Natural experiment. Setting England, Wales, and the UK.
Main outcome measures Age standardised annual mortality rates in England, Wales, and the UK from 1963, when the BBC first broadcast Doctor Who, a fictional programme with a character called the Doctor who fights villains and intervenes to save others while travelling through space and time. Mortality rates were modelled in a time series analysis accounting for non-linear trends over time, and associations were estimated in relation to a new Doctor Who episode broadcast during the previous festive period, 24 December to 1 January. An interrupted time series analysis modelled the shift in mortality rates from 2005, when festive episodes of Doctor Who could be classed as a yearly Christmas intervention.
Results 31 festive periods from 1963 have featured a new Doctor Who episode, including 14 broadcast on Christmas Day. In time series analyses, an association was found between broadcasts during the festive period and subsequent lower annual mortality rates. In particular, episodes shown on Christmas Day were associated with 0.60 fewer deaths per 1000 person years (95% confidence interval 0.21 to 0.99; P=0.003) in England and Wales and 0.40 fewer deaths per 1000 person years (0.08 to 0.73; P=0.02) in the UK. The interrupted time series analysis showed a strong shift (reduction) in mortality rates from 2005 onwards in association with the Doctor Who Christmas intervention, with a mean 0.73 fewer deaths per 1000 person years (0.21 to 1.26; P=0.01) in England and Wales and a mean 0.62 fewer deaths per 1000 person years (0.16 to 1.09; P=0.01) in the UK.
Conclusions A new Doctor Who episode shown every festive period, especially on Christmas Day, was associated with reduced mortality rates in England, Wales, and the UK, suggesting that a doctor working over the festive period could lower mortality rates. This finding reinforces why healthcare provision should not be taken for granted and may prompt the BBC and Disney+ to televise new episodes of Doctor Who every festive period, ideally on Christmas Day.
Objectives To identify Barbie brand dolls that had medicine and science themed professions in comparison with other career dolls and to determine their accuracy in meeting clinical and laboratory safety standards. Design Descriptive quantitative study. Setting Visual and data analysis of web searches.
Main outcome measures To identify the kinds of medical and scientific subspecialties that the Barbie dolls (and a comparison doll group) worked in; and to determine whether these medical professional and scientist dolls met laboratory and clinical safety standards. Additional data about doll demographics (ie, age, ethnic group, and sex) were also collected.
Participants 92 Barbie brand dolls were analyzed: doctor (n=53), scientist (n=10), science educator (n=2), nurse (n=15), dentist (n=11), and paramedic (n=1). 65 non-Barbie brand dolls were also analyzed for comparison purposes: doctor (n=26), scientist (n=27), nurse (n=7), dentist (n=2), engineer (n=2), and magnetic resonance imaging (MRI) technician (n=1) dolls.
Results Barbie brand medical professional dolls (n=80) largely treated children (66%, n=53/80), with only three (4%) medical professional dolls being directly depicted working with adults. Of the 12 scientist Barbie brand dolls, none met all proper personal protective equipment requirements related to hair and clothing. Barbie brand dolls often came with items, such as laboratory coats, microscopes, stethoscopes, and glasses, that children stereotypically associate with doctors and scientists. While comparison dolls offered a wider range of age and ethnic groups than the Barbie doll group did, the dolls similarly struggled to portray a wide range of medical and scientific subfields and most comparison dolls did not wear proper personal protective equipment.
Conclusions Medicine and science themed dolls help to inspire tomorrow’s medical professionals and scientists. All toy companies should ensure that future medical professional and scientist dolls meet clinical and laboratory safety standards and diversify the types of medical and scientific professions represented (especially among male dominated fields). For young girls’ sakes as much as her own, Barbie must keep shattering glass ceilings.
It’s the end of November and we’ve just come to the end of World Antimicrobial Awareness Week 2023 #waaw. I have previously posted about some of the challenges linked to antimicrobial resistance and this year I’ve been really impressed by the amount of information on social media. I also know of some face to face events (more on that later) linked to speaking to school children and healthcare staff. Many of us are involved with an engagement push linked to this week, and one-off events are both valuable and have strength of purpose. I wonder though how many of us have really thought about how we design or put these events together in a chain for greater impact or in the wider context of the challenge?
What do we normally do?
It is sometimes tempting, especially if we’re doing a one off event, to focus on the activity or engagement first. This means that we will often come up with the cool fun idea of what we are going to do, focussing on the science, and how to break that down. This means that sometimes we start towards the end of the process, rather than starting off spending time thinking about what it is we want to achieve and then building everything based around that.
Even when you have the objectives nailed there are a number of different ways and factors that may impact your messaging and how that message is co-created/received, and your audience is a key component of the design process. Factors to consider can include aspects such as:
Social and cultural norms (beliefs or religious practices)
Different objectives lend themselves to different things, and to different audiences. Infographics are a very common way of communicating. They are easy to share and have great longevity, as they can be used in social media, but can also be utilised in print form for posters and leaflets to allow a different form of targeted spread. They can work better with some groups than others, and depending on the content are more likely to appeal to individuals with pre-existing knowledge or interest.
One of the challenges with a lot of the way that we communicate is that some of the facts can come across as pretty scary. The classic message that often gets used is modelling data that more people will die from antimicrobial resistance (AMR) than cancer by 2050. The problem with using these kind of shock statistics is that it runs the risk of turning general members of the public off the message as it’s both a scary and a big problem, which they can’t face engaging with as they don’t feel they have the capacity to influence it. This is especially true for those who see themselves as rarely interacting with healthcare, who might go to the GP every other winter for a course of antibiotics, but don’t see themselves as getting sick.
Another challenge is balancing some of the messaging, the message that everyone is responsible can sometimes read that no one is actually responsible. When I’m out and about having conversations about this right now, the pandemic has definitely had an impact. There is a lot of compassion and other fatigue post SARS CoV2, where people feel like they have given up a lot for the ‘greater good’ and don’t want to feel like more is being asked of them, in terms of personal sacrifice.
It is also hard to get both your ‘what’ and your ‘why’ into a single infographic. Messages linked to action are very powerful, but they tend to work better for audiences who already have a strong grasp of why the message is important and how it relates to a specific issue.
Great programmes, such as the Antibiotic Guardian programme, are already doing great work and position themselves linked to a behaviour change by encouraging individuals to sign up to behaviour pledges. They tend to appeal to people who have some pre-existing baseline knowledge, with pledges acting as re-enforcement. For instance, images, like the one below, are great and super easy to interpret, if you already have an understanding of antimicrobial resistance being a One Health issue. This is valuable, especially if your target audience is those using large amounts of antibiotics in daily life, such as farming, or antimicrobial prescribers, such as medics and vet.
Other types of engagement options enable you to tackle some of the frequent mis-conceptions, such as the fact that it is the person and not the organism that becomes resistant. Face to face encounters allow you to get a greater feel for where any of the knowledge gaps or pre-conceptions lie, in a way that is harder when you are just sending messaging out into the world. The limitation of this approach is always going to be the number of people who can be engaged. So the choice of objective really does impact which approach would be best, alongside whether you are aiming for knowledge/awareness raising or whether you are aiming to impact or change behaviour.
One of the other challenges with designing content or activities without having first defined your audience is that the language pitch can be particularly challenging. Words like diagnostics work really well when talking to healthcare professionals, but may resonate with the wider public. The things are also not static, the wider public may be more comfortable with certain terms post pandemic than they were before, this may or may not be maintained as part of common language as the years past. Therefore language options that may be appropriate in 2023 may not be appropriate in 2027, and undertaking a conscious review of pitch and language is required every time.
What does the literature tell us?
We recently published a paper focussing on some of these issues and processes linked to designing outreach or engagement for AMR, and it really made me think about some of the steps that might be helpful. It also made me realise how we should be using other tools and options when designing both our activities and evaluations linked to social behavioural models (Participatory learning and action approaches (PLA), Information-Motivation-Behavioural (IMB), Transtheoretical approaches) taking the learning and understanding from other areas to maximise our success in this area. Some of the key prompts for me included:
How many of us really take the time to define our target populations and think about what would work for the group we are going to target?
How many of us really define the single simple message we want that target audience to take away from our interaction and think about whether we are looking at knowledge/awareness increase or behaviour change?
How many of us design evaluation strategies based on population and target message/change in order to understand whether we have achieved our aims and how to improve it next time?
Without really embedding a rationale, design, and evaluation process, are we ever going to achieve what we want to achieve within a highly complex landscape? Because of the ‘super wicked’ nature of communicating about AMR unless we take a co-productive approach, will any of our interactions lead to long-term impacts? Are we really going to reach the groups that could most influence that change?
How can we approach things differently?
It takes a lot of time to design activities and I for one am always tempted to re-use and re-purpose as I’m time resource limited. One of the main things that came out of writing the paper, for me, was being very conscious of picking of the right tool for the job, and that one size doesn’t fit all because of the different reasons we might be undertaking the work in the first place.
Another thing that really struck me when reading the literature in this area is how much the power of telling stories can really address some of the issues that are linked to fear or the complexity of the challenge. It offers a route into the topic for people who are not necessarily already engaged by offering entertainment, and also to describe scenarios in a way to allow people to not feel so judged about personal actions whilst raising knowledge/awareness. It can provide a safe way to engage with a topic on an emotional level with reduced risk.
We’ve tried some of these concepts as part of The Project Nosocomial, with different approaches, from drag Klebsiella and panel discussions, to complete plays aimed at different audiences.
It is not just us that have tried this approach, there have been films such as Catch and musicals such as The Mould that Changed the World.
Not everyone is going to write a full on play however in order to engage others. Despite this I think there are things that we can still learn as scientists, like feeling empowered to tell our stories and our whys, that can support connections and innovation in this area. These approaches can be embedded in a low key way in all of our activity planning in order to enrich them. This type of experience, just like with Ted and others talks, can be really valuable in helping us improve our wider communication skills, and therefore also help with our wider professional practice.
One of the big challenges can be feeling secure enough to bring yourself, as well as the scientist, to your activity. By doing so, by sharing our stories and our why, you can engage in a deeper way than by just being the expert in the room. It adds depth and the ability to respond during engagement that hopefully leads to improved longevity of impact, and inspiration of intellectual curiosity of those involved. It also provides a route for us to learn as scientists, not just about communication, but also about how lived experience can impact patient choices.
I suppose, my point in this article is that I hope we can all be a bit braver, both in acknowledging the challenges we face in addressing an issue of this complexity, but also the steps we take in designing our responses to those challenges. I’d love to hear what other people are doing, so if you want to let me know that would be great, or you could even write a guest blog on your experiences of what you are up to in this area.