I adore Christmas, it’s one of my favourite times of the year. I meant to get this one out before Christmas, but to be honest, I was too busy having family time. For those of us working or looking for some fun reading between Christmas and New Year I thought this one might still be of interest.
Every year the British Medical Journal have a wonderful tradition. They post some free to access journal article. Now, these aren’t just any journal articles. They apply serious scientific processes to brilliant topics, such as the disappearance rates hard vs soft centred chocolates in ward environments presented as an observational study.
These articles always bring a smile to my face, and if you’re looking at an entertaining way to learn more about scientific processes or scientific writing these are a great place to start. I hope you’ll feel the same when you have a read of some of the ones linked to below, and know that there are more out there if you want to journey down this particular rabbit hole.
Merry Christmas, and thank you so much for spending another year in the company of the Girlymicro blog!

From 2005
The case of the disappearing teaspoons: longitudinal cohort study of the displacement of teaspoons in an Australian research institute BMJ 2005;331:1498
Abstract
Objectives To determine the overall rate of loss of workplace teaspoons and whether attrition and displacement are correlated with the relative value of the teaspoons or type of tearoom.
Design Longitudinal cohort study.
Setting Research institute employing about 140 people.
Subjects 70 discreetly numbered teaspoons placed in tearooms around the institute and observed weekly over five months.
Main outcome measures Incidence of teaspoon loss per 100 teaspoon years and teaspoon half life.
Results 56 (80%) of the 70 teaspoons disappeared during the study. The half life of the teaspoons was 81 days. The half life of teaspoons in communal tearooms (42 days) was significantly shorter than for those in rooms associated with particular research groups (77 days). The rate of loss was not influenced by the teaspoons’ value. The incidence of teaspoon loss over the period of observation was 360.62 per 100 teaspoon years. At this rate, an estimated 250 teaspoons would need to be purchased annually to maintain a practical institute-wide population of 70 teaspoons.
Conclusions The loss of workplace teaspoons was rapid, showing that their availability, and hence office culture in general, is constantly threatened.

From 2010
Beauty sleep: experimental study on the perceived health and attractiveness of sleep deprived people BMJ 2010;341:c6614
Abstract
Objective To investigate whether sleep deprived people are perceived as less healthy, less attractive, and more tired than after a normal night’s sleep.
Design Experimental study.
Setting Sleep laboratory in Stockholm, Sweden.
Participants 23 healthy, sleep deprived adults (age 18-31) who were photographed and 65 untrained observers (age 18-61) who rated the photographs.
Intervention Participants were photographed after a normal night’s sleep (eight hours) and after sleep deprivation (31 hours of wakefulness after a night of reduced sleep). The photographs were presented in a randomised order and rated by untrained observers.
Main outcome measure Difference in observer ratings of perceived health, attractiveness, and tiredness between sleep deprived and well rested participants using a visual analogue scale (100 mm).
Results Sleep deprived people were rated as less healthy (visual analogue scale scores, mean 63 (SE 2) v 68 (SE 2), P<0.001), more tired (53 (SE 3) v 44 (SE 3), P<0.001), and less attractive (38 (SE 2) v 40 (SE 2), P<0.001) than after a normal night’s sleep. The decrease in rated health was associated with ratings of increased tiredness and decreased attractiveness.
Conclusion Our findings show that sleep deprived people appear less healthy, less attractive, and more tired compared with when they are well rested. This suggests that humans are sensitive to sleep related facial cues, with potential implications for social and clinical judgments and behaviour. Studies are warranted for understanding how these effects may affect clinical decision making and can add knowledge with direct implications in a medical context.
From 2013
The survival time of chocolates on hospital wards: covert observational study BMJ 2013;347:f7198
Abstract
Objective To quantify the consumption of chocolates in a hospital ward environment.
Design Multicentre, prospective, covert observational study.
Setting Four wards at three hospitals (where the authors worked) within the United Kingdom.
Participants Boxes of Quality Street (Nestlé) and Roses (Cadbury) on the ward and anyone eating these chocolates.
Intervention Observers covertly placed two 350 g boxes of Quality Street and Roses chocolates on each ward (eight boxes were used in the study containing a total of 258 individual chocolates). These boxes were kept under continuous covert surveillance, with the time recorded when each chocolate was eaten.
Main outcome measure Median survival time of a chocolate.
Results 191 out of 258 (74%) chocolates were observed being eaten. The mean total observation period was 254 minutes (95% confidence interval 179 to 329). The median survival time of a chocolate was 51 minutes (39 to 63). The model of chocolate consumption was non-linear, with an initial rapid rate of consumption that slowed with time. An exponential decay model best fitted these findings (model R2=0.844, P<0.001), with a survival half life (time taken for 50% of the chocolates to be eaten) of 99 minutes. The mean time taken to open a box of chocolates from first appearance on the ward was 12 minutes (95% confidence interval 0 to 24). Quality Street chocolates survived longer than Roses chocolates (hazard ratio for survival of Roses v Quality Street 0.70, 95% confidence interval 0.53 to 0.93, P=0.014). The highest percentages of chocolates were consumed by healthcare assistants (28%) and nurses (28%), followed by doctors (15%).
Conclusions From our observational study, chocolate survival in a hospital ward was relatively short, and was modelled well by an exponential decay model. Roses chocolates were preferentially consumed to Quality Street chocolates in a ward setting. Chocolates were consumed primarily by healthcare assistants and nurses, followed by doctors. Further practical studies are needed.

From 2015
Evidence of a Christmas spirit network in the brain: functional MRI study BMJ 2015;351:h6266
Abstract
Objective To detect and localise the Christmas spirit in the human brain.
Design Single blinded, cross cultural group study with functional magnetic resonance imaging (fMRI).
Setting Functional imaging unit and department of clinical physiology, nuclear medicine and PET in Denmark.
Participants 10 healthy people from the Copenhagen area who routinely celebrate Christmas and 10 healthy people living in the same area who have no Christmas traditions.
Main outcome measures Brain activation unique to the group with Christmas traditions during visual stimulation with images with a Christmas theme.
Methods Functional brain scans optimised for detection of the blood oxygen level dependent (BOLD) response were performed while participants viewed a series of images with Christmas themes interleaved with neutral images having similar characteristics but containing nothing that symbolises Christmas. After scanning, participants answered a questionnaire about their Christmas traditions and the associations they have with Christmas. Brain activation maps from scanning were analysed for Christmas related activation in the “Christmas” and “non-Christmas” groups individually. Subsequently, differences between the two groups were calculated to determine Christmas specific brain activation.
Results Significant clusters of increased BOLD activation in the sensory motor cortex, the premotor and primary motor cortex, and the parietal lobule (inferior and superior) were found in scans of people who celebrate Christmas with positive associations compared with scans in a group having no Christmas traditions and neutral associations. These cerebral areas have been associated with spirituality, somatic senses, and recognition of facial emotion among many other functions.
Conclusions There is a “Christmas spirit network” in the human brain comprising several cortical areas. This network had a significantly higher activation in a people who celebrate Christmas with positive associations as opposed to a people who have no Christmas traditions and neutral associations. Further research is necessary to understand this and other potential holiday circuits in the brain. Although merry and intriguing, these findings should be interpreted with caution.

From 2021
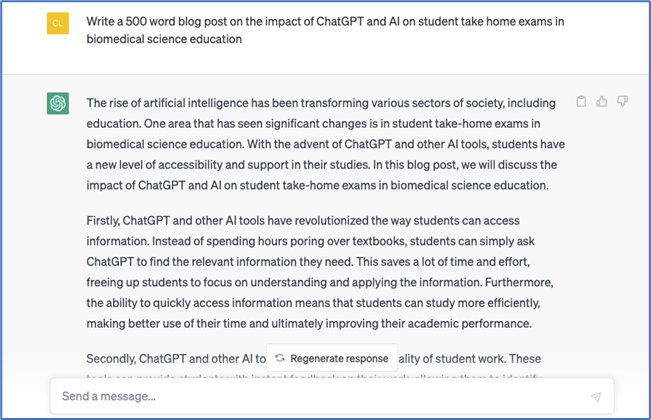
Ghost in the machine or monkey with a typewriter—generating titles for Christmas research articles in The BMJ using artificial intelligence: observational study BMJ 2021;375:e067732
Abstract
Objective To determine whether artificial intelligence (AI) can generate plausible and engaging titles for potential Christmas research articles in The BMJ.
Design Observational study.
Setting Europe, Australia, and Africa.
Participants 1 AI technology (Generative Pre-trained Transformer 3, GPT-3) and 25 humans.
Main outcome measures Plausibility, attractiveness, enjoyability, and educational value of titles for potential Christmas research articles in The BMJ generated by GPT-3 compared with historical controls.
Results AI generated titles were rated at least as enjoyable (159/250 responses (64%) v 346/500 responses (69%); odds ratio 0.9, 95% confidence interval 0.7 to 1.2) and attractive (176/250 (70%) v 342/500 (68%); 1.1, 0.8 to 1.4) as real control titles, although the real titles were rated as more plausible (182/250 (73%) v 238/500 (48%); 3.1, 2.3 to 4.1). The AI generated titles overall were rated as having less scientific or educational merit than the real controls (146/250 (58%) v 193/500 (39%); 2.0, 1.5 to 2.6); this difference, however, became non-significant when humans curated the AI output (146/250 (58%) v 123/250 (49%); 1.3, 1.0 to 1.8). Of the AI generated titles, the most plausible was “The association between belief in conspiracy theories and the willingness to receive vaccinations,” and the highest rated was “The effects of free gourmet coffee on emergency department waiting times: an observational study.”
Conclusions AI can generate plausible, entertaining, and scientifically interesting titles for potential Christmas research articles in The BMJ; as in other areas of medicine, performance was enhanced by human intervention.
From 2023
As a special Christmas gift there were 2 from 2023 that made me exceptionally happy!
Effect of a doctor working during the festive period on population health: natural experiment using 60 years of Doctor Who episodes (the TARDIS study) BMJ 2023;383:e077143
Abstract
Objective To examine the effect of a (fictional) doctor working during the festive period on population health.
Design Natural experiment.
Setting England, Wales, and the UK.
Main outcome measures Age standardised annual mortality rates in England, Wales, and the UK from 1963, when the BBC first broadcast Doctor Who, a fictional programme with a character called the Doctor who fights villains and intervenes to save others while travelling through space and time. Mortality rates were modelled in a time series analysis accounting for non-linear trends over time, and associations were estimated in relation to a new Doctor Who episode broadcast during the previous festive period, 24 December to 1 January. An interrupted time series analysis modelled the shift in mortality rates from 2005, when festive episodes of Doctor Who could be classed as a yearly Christmas intervention.
Results 31 festive periods from 1963 have featured a new Doctor Who episode, including 14 broadcast on Christmas Day. In time series analyses, an association was found between broadcasts during the festive period and subsequent lower annual mortality rates. In particular, episodes shown on Christmas Day were associated with 0.60 fewer deaths per 1000 person years (95% confidence interval 0.21 to 0.99; P=0.003) in England and Wales and 0.40 fewer deaths per 1000 person years (0.08 to 0.73; P=0.02) in the UK. The interrupted time series analysis showed a strong shift (reduction) in mortality rates from 2005 onwards in association with the Doctor Who Christmas intervention, with a mean 0.73 fewer deaths per 1000 person years (0.21 to 1.26; P=0.01) in England and Wales and a mean 0.62 fewer deaths per 1000 person years (0.16 to 1.09; P=0.01) in the UK.
Conclusions A new Doctor Who episode shown every festive period, especially on Christmas Day, was associated with reduced mortality rates in England, Wales, and the UK, suggesting that a doctor working over the festive period could lower mortality rates. This finding reinforces why healthcare provision should not be taken for granted and may prompt the BBC and Disney+ to televise new episodes of Doctor Who every festive period, ideally on Christmas Day.

Analysis of Barbie medical and science career dolls: descriptive quantitative study BMJ 2023;383:e077276
Abstract
Objectives To identify Barbie brand dolls that had medicine and science themed professions in comparison with other career dolls and to determine their accuracy in meeting clinical and laboratory safety standards.
Design Descriptive quantitative study.
Setting Visual and data analysis of web searches.
Main outcome measures To identify the kinds of medical and scientific subspecialties that the Barbie dolls (and a comparison doll group) worked in; and to determine whether these medical professional and scientist dolls met laboratory and clinical safety standards. Additional data about doll demographics (ie, age, ethnic group, and sex) were also collected.
Participants 92 Barbie brand dolls were analyzed: doctor (n=53), scientist (n=10), science educator (n=2), nurse (n=15), dentist (n=11), and paramedic (n=1). 65 non-Barbie brand dolls were also analyzed for comparison purposes: doctor (n=26), scientist (n=27), nurse (n=7), dentist (n=2), engineer (n=2), and magnetic resonance imaging (MRI) technician (n=1) dolls.
Results Barbie brand medical professional dolls (n=80) largely treated children (66%, n=53/80), with only three (4%) medical professional dolls being directly depicted working with adults. Of the 12 scientist Barbie brand dolls, none met all proper personal protective equipment requirements related to hair and clothing. Barbie brand dolls often came with items, such as laboratory coats, microscopes, stethoscopes, and glasses, that children stereotypically associate with doctors and scientists. While comparison dolls offered a wider range of age and ethnic groups than the Barbie doll group did, the dolls similarly struggled to portray a wide range of medical and scientific subfields and most comparison dolls did not wear proper personal protective equipment.
Conclusions Medicine and science themed dolls help to inspire tomorrow’s medical professionals and scientists. All toy companies should ensure that future medical professional and scientist dolls meet clinical and laboratory safety standards and diversify the types of medical and scientific professions represented (especially among male dominated fields). For young girls’ sakes as much as her own, Barbie must keep shattering glass ceilings.

All opinions on this blog are my own