I must admit I shed a bit of a happy tear when this arrived unsolicited in my inbox, it’s been a bit of a week. My next thought was that there is no way I could share it, as it would be the epitome of self promotion, and that’s never considered to be a good look. Then I sat and thought, what would I advise a friend to do if they were in the same situation and I decided something. I decided to be proud of what I’d achieved. To be proud of the hours spent to achieve the output earned, and to be proud to have someone so invested they would take the time to write an unsolicited review for this blog. I know that is what I would advise and hope that all of you would do, and so this is my moment I decided to model the advice I would give. We all have the right to own our achievements and not make ourselves small to avoid the commentary of others.
Dr Walker is a paid up member of the Dream Team since 2013, token immunologist and occasional defector from the Immunology Mafia. Registered Clinical Scientist in Immunology with a background in genetics (PhD), microbiology and immunology (MSc), biological sciences (mBiolSci), education (PgCert) and indecisiveness (everything else). Now a Senior Lecturer in Immunology at University of Lincoln. She has previously written many great guest blogs for The Girlymicrobiologist, including one on turning criticism into a catalyst for change.
Full disclosure: I wasn’t invited to write this review, I insisted. I also haven’t been paid for it; quite the opposite, in fact. I went out and bought two copies of Professor Elaine Cloutman-Green’s book with my own money: one for me and one for my PhD students to share (or squabble over). And yes, I did get her to sign them. What can I say? I’m a lifelong fangirl.
Professor Cloutman-Green’s It Shouldn’t Happen to a PhD Student is a rare gem in academic literature a compassionate, wise, and profoundly practical guide that feels like a conversation with the mentor every research student wishes they had. Written with warmth, humour, and candour, the book demystifies the PhD journey from start to finish, transforming what can often be an isolating experience into one filled with clarity, community, and hope.
Elaine, known affectionately as my favourite Professor or the GirlyMicrobiologist, draws upon two decades of experience as both scientist and supervisor to craft a guide that balances rigour with humanity. Structured in three accessible sections; getting onto a PhD programme, surviving and thriving during it, and using it as a springboard for the future. The book serves as both a roadmap and a reassuring companion. Each chapter blends actionable advice with reflections that acknowledge the emotional highs and lows of research life, creating a tone that is both authoritative and deeply empathetic.
From the very first chapter, “Knowing Your Why,” Elaine invites readers to pause and reflect on their motivations, an exercise that sets the tone for the entire book. Rather than treating doctoral study as a mechanical career step, she frames it as a personal journey of purpose and growth. As she writes, “A PhD should be a step towards delivering on your aspirations, not just a title to put in front of your name.” It’s a line that perfectly encapsulates her philosophy that research is not about prestige, but about purpose.
What truly elevates this book above other graduate-school guides is its inclusivity and warmth. Elaine writes as a mentor who has seen it all: the sleepless nights, the imposter syndrome, the joy of a successful experiment, and the power of perseverance. Her anecdotes and checklists are peppered with practical wisdom not the vague “work harder” platitudes found elsewhere, but concrete steps to manage deadlines, develop professional skills, and build meaningful academic networks. The inclusion of “Top Tips” sections at the end of each stage provides digestible summaries that make the book easy to dip in and out of throughout the PhD journey.
And it’s not just students who need this book. Supervisors – myself included – will find plenty here that resonates. Elaine reminds us, gently but firmly, that supervisors are people too: flawed, human, and still learning alongside our students. Her reflections on empathy, communication, and shared growth are as valuable for those guiding PhDs as for those undertaking them. Every research group could benefit from having this guide on their shelf, it’s as much a manual for mentorship as it is for PhD survival.
Of course I must acknowledge my own bias, Elaine was my mentor during my own PhD, and many of the insights in this book feel like familiar echoes of the advice that got me through my hardest days. She taught me so much about science but more importantly that research, like life, is all about surrounding yourself with people who lift you up when you falter. It Shouldn’t Happen to a PhD Student captures that same generous spirit, showing that the best kind of academic success is shared success: when mentors and students grow together, celebrate each other’s wins, and keep curiosity at the heart of everything they do. Everyone deserves a mentor like Elaine someone who reminds you that with compassion, courage, and community, the PhD journey can be one of the most transformative experiences of your life. Oh, and she provides the most excellent of snacks, the occasional much needed gin and tonic, and a rousing rendition of ‘Drop it like it’s hot!’… but that’s a story for another time.
I am currently in the middle of secret project, which I hope to announce more about in late August/early September. I’m really excited about it but it’s taking a bunch of my time. I’m hoping that you will be just as excited when I can share more details. The wonderful Dr Claire Walker is helping me deliver my passion project by curating the Girlymicrobiologist blog for a few weeks. This means that I hope you all enjoy getting some great guest blogs from a range of topics. Girlymicrobiologist is a community, and all of the wonderful authors stepping up, sharing their thoughts and projects, to support me in mine means the world. I hope you enjoy this guest blog series. Drop me a line if you too would be interested in joining this community by writing a guest blog.
Dr Walker who is a paid up member of the Dream Team since 2013, token immunologist and occasional defector from the Immunology Mafia. Registered Clinical Scientist in Immunology with a background in genetics (PhD), microbiology and immunology (MSc), biological sciences (mBiolSci), education (PgCert) and indecisiveness (everything else). Now a Senior Lecturer in Immunology at University of Lincoln. She has previously written many great guest blogs for the Girlymicrobiologist, including The Clinical Academic Path – From the Lab to the Lectern.
This weeks blog post is from Dr Shayda Karimi, who is a medical doctor and self published author, discussing how important creativity is in science.
Blog by Shayda Karimi
Hello! My name is Shayda.
I’m a medical doctor, specialising in anaesthesia and pre-hospital emergency care. Medicine has always been considered one of the ‘softer’ sciences, but never the less is more of a science than a humanity, and the subject takes pride in adhering to evidence based practice. Creativity lies at the heart of problem solving, and problem solving is key to providing high quality, innovative medical care, especially in dynamic specialities like emergency care. For example, I was recently faced with the dilemma of a man impaled on a large segment of aluminium ladder. The metal couldn’t be removed without a CT scan to determine which structures it had damaged, and due to the angle of penetration, the patient couldn’t fit through the scanner with it in place. The creative solution was to put a 999 call out to the fire service, who with specialist cutting equipment were able to reduce the size on the metal segment. The patient safely had his scan.
Creativity in science should be encouraged. Through my time at medical school, opportunities to be creative were very limited- most lectures were on never changing topics- anatomy and physiology. I took a student component module called ‘medicine in literature’- even that was factual. To resolve this gap in my undergraduate education, in my F3 year (a common point for junior doctors to take a year out of training, having completed two foundation years and before commencing higher specialist training) I decided to complete a masters degree in creative writing. I was the only person on my course with a ‘science’ background.
The dissertation for this course was a long piece of writing. Which for the first time in my post primary school life, could be completely and utterly false. This dissertation turned into my first novel. Writing fiction develops problem solving skills- characters must resolve the obstacles put into their path, and this must be believable with the rules they are living in. I learned about how language can be used to invoke emotions and atmosphere- this is of vital importance when speaking to patients and colleagues. Or even when writing emails! I developed an appreciation that though creativity is not fact- it can also be to a certain degree taught and developed.
The dissertation turned into my first published novel ‘Heirs’, set in a future dystopian London, conjoined twins are born next in line to the throne. They end up separated and in a fight for power. This was fun experience; taking the science I knew as fact, and adding a whole load of fiction to turn it into a familiar but bizarre future.
Creativity and science go hand in hand. We should all endeavour to leave the cold hard world of facts every once in a while and dive into something purely imaginative; an art class or high fantasy novel.
“The true sign of intelligence is not knowledge, but imagination” – Albert Einstein
I am currently in the middle of secret project, which I hope to announce more about in late August/early September. I’m really excited about it but it’s taking a bunch of my time. I’m hoping that you will be just as excited when I can share more details. The wonderful Dr Claire Walker is helping me deliver my passion project by curating the Girlymicrobiologist blog for a few weeks. This means that I hope you all enjoy getting some great guest blogs from a range of topics. Girlymicrobiologist is a community, and all of the wonderful authors stepping up, sharing their thoughts and projects, to support me in mine means the world. I hope you enjoy this guest blog series. Drop me a line if you too would be interested in joining this community by writing a guest blog.
Callum is a disciple of the biomedical sciences, current master’s student creating a more authentic lab experience for those after me, aspiring consultant microbiologist (the best discipline, sorry Claire – you see he understands, like me, that micro will always trump immunology).
Callum is supervised by Dr Walker who is a paid up member of the Dream Team since 2013, token immunologist and occasional defector from the Immunology Mafia. Registered Clinical Scientist in Immunology with a background in genetics (PhD), microbiology and immunology (MSc), biological sciences (mBiolSci), education (PgCert) and indecisiveness (everything else). Now a Senior Lecturer in Immunology at University of Lincoln. She has previously written many great guest blogs for the Girlymicrobiologist, including Exome Sequencing and the Hunt for New Genetic Diseases.
Blog by Callum Barnes
Hello again everyone! It certainly feels weird to be writing another one of these, but my supervisor the lovely Dr Claire Walker thought it would be a great idea considering the outcome of my research that I discussed here.
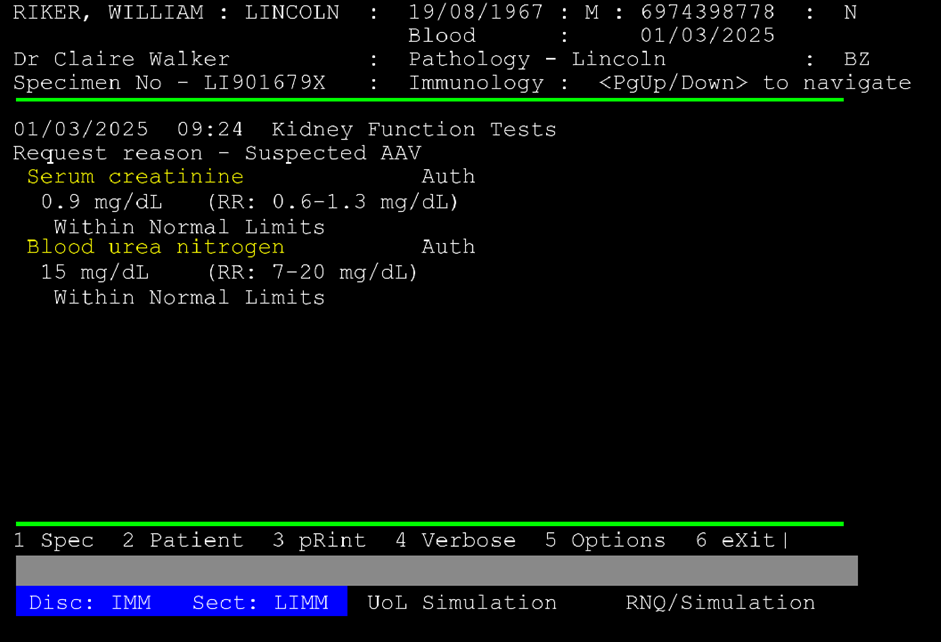
A small recap for those that don’t want to read two blogposts – I am an Mbio Biomedical Science student at the University of Lincoln and completed my portfolio on a placement year in a local microbiology lab. It was great and I became so much more confident in both my practical and theoretical work, which really showed me the value of clinical placements. The problem is that these placements are too few and too competitive nationwide, and only a fraction of those that want to join the biomedical workforce get to experience them despite their value. Long story short, we created a clinical simulation that was as authentic to a real pathology lab as possible, with patient request cards and a functioning (front-end) LIMS, both seen below:
Can you believe no one got the Star Trek references? Anyway. The results were honestly incredible, with basically everyone that participated getting value out of it. I can’t share too much as we are yet to publish, but here are some quotes that really highlight how the clinical simulation increased confidence and was effective as a learning tool.
“Getting hands on experience in the lab. It gave me the confidence to continue in the lab setting.”
“Overall, the lab practicals have been helpful. I think my lab skills have drastically improved, especially my microscopy skills and interpreting my lab results.”
“I like the opportunity we had to practice new skills and learn about it in the contrast of a case study.”
These results were really good, but during my background research I came to realise that other medical disciplines are ahead of us in utilising learning tools to teach university students – like really ahead. Trainee doctors have actors, manikins, and in the last decade have extensively integrated VR/AR/XR technologies into their teachings. We are left with a couple of practical sessions per discipline to cover the hundreds of different diagnostic processes that biomedical scientists go through. And this is almost entirely down to cost, practicals cost a fortune after all. They take setting up, and time, which staff don’t have enough of as is. Which brings us back to virtual reality…
Virtual reality (can be) cheap, accessible, and most importantly repeatable. Other medical disciplines have already identified this, and there is good data to back up the use of VR in those disciplines. But none in biomedical science, because clinical simulation is only just being recognised as a worthy endeavour.
And so, this is going to be my goal. I am going to develop software to train biomedical scientists in virtual reality. It’s going to be tough, but I do truly believe that this is a sorely neglected part of training the next generation of pathologists here in the UK, and honestly hopefully the world too. And if everything goes well (and even if it doesn’t), I’ll be back here in a year to let you all know how it went.
Following on from the wonderful fungal post on fungal toxins (mycotoxins) last week from Dr Sam Watkin, I wanted to follow up with a post on the latest fungi of interest from a clinical perspective, Candidozyma auris. This fungi is getting more and more coverage, as well as becoming more important in healthcare, so I thought I would take a moment to talk about what it is, what it does, how to find it, and what to do when you do.
In a pre-pandemic world, which feels like a long time ago, Professor Lena Ciric was working at a media fellowship, and as part of that work wrote an article for the BBC on Candida auris, which has subsequently been renamed to Candidozyma auris.
This article came out in 2019, so maybe C. auris is not so new but in terms of the numbers of cases we are seeing within the NHS, and the changing prevalence out in healthcare systems more widely, it is definitely more of a feature and a concern than it was back then. Reflecting this change the UKHSA guidance Candidozyma auris (formerly Candida auris): guidance for acute healthcare settings which was originally published in 2016, has been updated recently (19th March 2025). It feels timely therefore to put something out in order to raise awareness of this organism and the unique challenges it presents.
NB I can neither spell nor pronounce Candidozyma auris and so we’re sticking to C. auris from this point out.
Yeast are a type of fungus, and Candida species are often associated with colonisation (present without causing infection or symptoms) on skin, in the mouth or within the vagina. If they grow up to high levels they can cause an infection called candidiasis, which often causes symptoms like itching or discharge. Common infections include Thrush and nappy rash. Candida albicans is one of the most common yeast infections seen within the healthcare setting, and in this kind of environment more serious infections can be seen, especially those linked to the blood stream, and occasionally serious organ infections.
C. auris was originally believed to be a relatively new species of genus Candida, as it often behaves in a similar way to the other Candida species. The reason for the name change to Candidozyma auris, was because, although in many ways it behaves similarly to its Candida cousins, it does have some differences in the way it behaves. These include features such as intrinsic antifungal resistance and growth conditions, that make it useful to characterise in a way that acknowledges it as a novel genus in its own right.
What is the difference between C. auris and the other Candida species that you know?
Many Candida species can cause severe infections within specific settings, however C. auris has been known to not only cause a wide variety of infections (bloodstream, intra-abdominal, bone and cerebrospinal fluid (CSF) infections), but ones which lead to significant mortality rates, with an estimated rate of 30 – 72% in severe infection reported in the literature.
Infections can occur in any patient group, although UK outbreaks have been most frequent associated with adult settings. Augmented care settings (such as intensive care and transplant settings) are at highest risk due to the vulnerable, long stay nature of many of their patients. Management of any infection occurring is complicated by the fact that C. auris has developed resistance to many available classes of antifungals, with emergence of pan-resistant strains, which add to the mortality risk.
C. auris also appears able to both easily transmit and colonise the skin of patients, with most patients being colonised before they go on to develop any subsequent infection. These colonised patients can then contaminate their healthcare environments, and unlike other yeast species, C. auris is able to survive and represent a continued risk within the environment for prolonged periods, all of which contributes to outbreak risk.
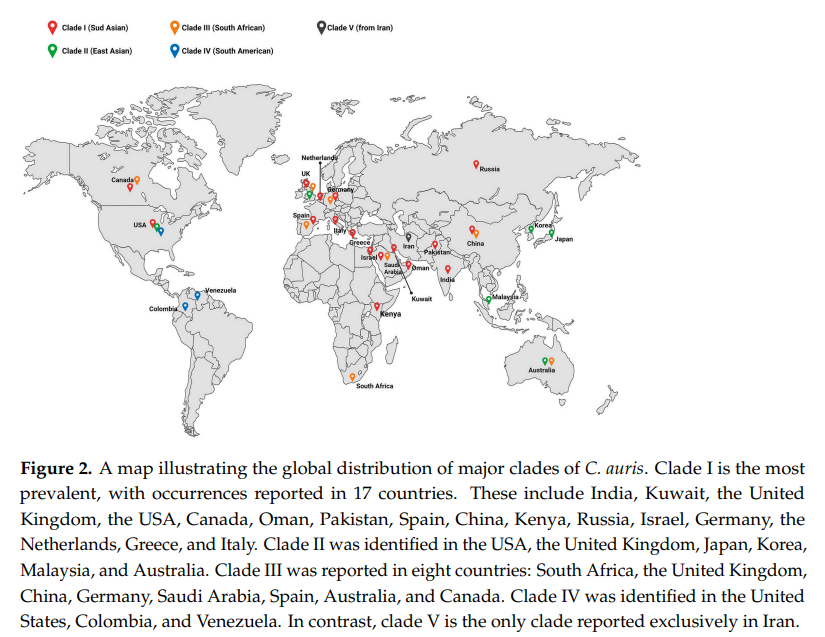
It was first identified in the ear canal of a patient in Japan in 2009, but has since been found globally, and is now separated into six genetically distinct clades:
Clade I = the South Asian clade, first detected in India and Pakistan
Clade II = the East Asian clade, first detected in Japan
Clade III = the South African clade, first detected in South Africa
Clade IV = the South American clade, first detected in Venezuela
Within the UK from January 2013 – December 2024, 637 C. auris isolates were reported through laboratory surveillance in England, with 59 (9.3%) isolated from blood culture specimens. It should be noted that not all labs report, and for some time many labs could not accurately identify C. auris, or actively screened for it, and so this may represent under reporting. A routine whole genome sequencing service is not currently available for typing, although it can be undertaken linked to specific outbreaks. Hopefully this will be up and running soon to better understand how the different clades discussed above are represented in the UK, and whether any of them are linked to more challenging outcomes than others.
Due to its global distribution, overseas patients may also be at increased risk of introducing C. auris into UK healthcare settings, with one centre reported 1.6% of their overseas admission detected as colonised, with patients coming from the Middle East, India and Pakistan, showing higher levels of recovery.
UKHSA guidance suggests we should screen any patient who has had an overnight stay in a healthcare facility outside of the UK in the previous year, as well as patients patients coming from affected units in the UK. This sounds relatively straight forward, but it can be challenging to identify patients who have had an overnight stay overseas on admission if they are not being admitted from overseas. It also relies on clear communication from other centres that they have an issue, if we are to screen patients from impacted units. Many centres have therefore decided to screen all patients on high-risk wards, such as intensive care, to address some of this unknown risk.
Risk factors for developing C. auris colonisation or infection should be considered when deciding on screening strategies and the list within the UKHSA guidance includes patients who have experience:
healthcare abroad, including repatriations or international patient transfers to UK hospitals for medical care, especially from countries with ongoing transmissions
recent surgery, including vascular surgery within 30 days
prolonged stay in critical care
severe underlying disease with immunosuppression, such as HIV and bone marrow transplantation
corticosteroid therapy
neutropenia
malignancy
chronic kidney disease or diabetes mellitus
mechanical ventilation
presence of a central-venous catheter or urinary catheter
extra-ventricular CSF drainage device
prolonged exposure to broad-spectrum antibiotic or antifungal use
Screening is undertaken by taking swabs from the axilla (armpit), groin and nose, although different patient groups may require additional screening. Patient surveillance is important for two reasons:
1) to understand which patients are colonised in order to introduce additional precautions to limit risk of transmission to other patients or the environment
2) to support improved patient management but allowing patients to be put on the most effective antifungal if they go on to develop any signs of yeast infection, in order to improve outcomes
If a patient is detected as positive, other screening sites can help manage individual patients and so UKHSA say additional site screening should be considered:
urine (especially if there is a urinary catheter in-situ, including intermittent self-catheterisation)
throat swab
perineal swab
rectal swab (in paediatrics we would consider a stool sample instead)
low vaginal swab
sputum or endotracheal secretions
drain fluid (abdominal, pelvic or mediastinal)
vascular access sites
wounds or broken skin
ear
umbilical area (neonates)
Swabs should ideally be processed on chromogenic media (colour changing agar plates) and fungal colonies confirmed using MALDI ToF or a validated PCR (my previous post on PCR may help with this). It can also be helpful to incubate plates at 40oC, as C. auris can grow as much higher temperatures than its Candida cousins, which can help with identification. If grown then the yeast should be stored in case you need them for future typing to help in understanding transmissions or outbreaks.
Why should we care about it?
Due to the high mortality rates for patients who develop infections, and the issues with choosing antifungals that work, it is really important that we know when we have patients who are colonised with C. auris. Controlling spread, even if patients don’t become infected, is incredibly important for the individual. This is because if a patient is detected as positive they won’t be de-alerted (have IPC precautions stopped) at any point and so it will impact them for months, if not years. These IPC precautions include isolation (keeping separate from other patients), and sometimes only being nursed by specific members of staff. These patient and staff impacts are so significant they’ve even been acknowledged in popular media, with a three episode arch covering C. auris in The Resident on Netflix (season three, episodes 18, 19 and 20).
Are there differences in how you might treat?
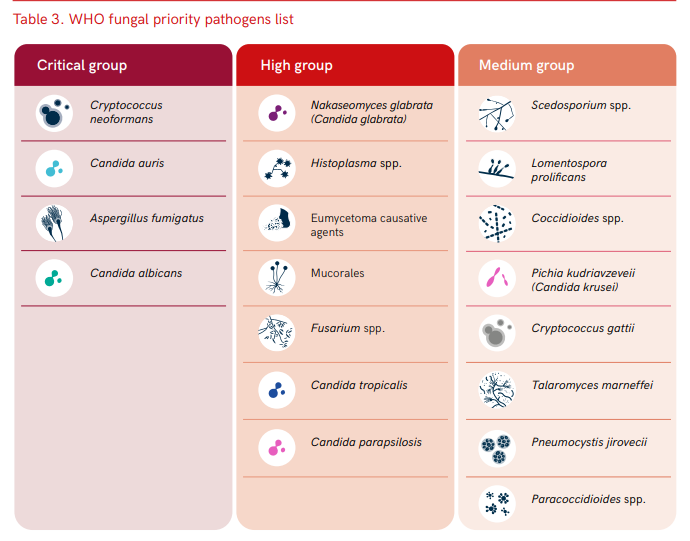
As I’ve already said, C. auris is pretty resistant to treatment compared to its Candida cousins. UK data indicates that isolates are resistant (don’t respond to) to the normal first line treatment of fluconazole, and often to other antifungals within the azole class. Some isolates have been resistant to other commonly used antifungals, such as amphotericin B (20%) and echinocandins (10%). Resistance to other antifungals can also occur whilst infections are being treated, and so it is important to monitor sensitivities (whether the drug works) and send to reference labs in order to understand the most appropriate therapy. Its resistance profile is one of the reasons the WHO have highlighted C. auris as a priority fungal pathogen for further research and to highlight clinical risk.
Its not just antifungals that are important however, antimicrobial stewardship is important in general, as prolonged exposure to broad-spectrum antibiotics and antifungal agents are risk factors for both C. auris colonisation and infection (again this links back to the high risk patient groups impacted). Therefore, doing a better job of monitoring and controlling antimicrobials in general is likely to have a beneficial impact on C. auris risk.
Challenges with environmental control
One of the many things I love about the new C. auris guidance is its focus on multidisciplinary input ‘Healthcare workers are encouraged to work in multi-disciplinary teams, including Clinical Infection Specialists and IPC teams, to risk assess and support the management of patients infected or colonised with C. auris‘. I think this is so important, especially with an organism that is so challenging and can present such a high risk.
Environmental control is a particular issue for C. auris as we know it’s ability to survive and can grow at higher temperatures than many other fungi, means that it is likely to survive well in the environment. It also has the ability to form environmental biofilms, which can mean it is difficult to impact effectively using standard cleaning techniques, and once within the environment has been been detected for 4 weeks.
Within the UKHSA documentation, environmental contamination for C. auris has been found on the following surfaces during outbreaks:
beds, bedside equipment, bedding materials including mattresses, bed sheets and pillows
ventilation grilles and air conditioning units
radiators
windowsills and other horizontal surfaces
hand wash basins, sink drains and taps
floors
bathrooms doors and walls
disposable and reusable equipment such as ventilators, skin-surface temperature probes, blood pressure cuffs, electrocardiogram leads, stethoscopes, pulse oximeters and cloth lanyards
Basically most of your healthcare environment, whether fixed or movable features. In order to help stop the transfer from patients to the environment, via staff, the use of personal protective equipment is really important. Therefore the use of gowns and gloves is suggested. Single use and disposable equipment should also be used whenever possible, and patients should be kept in single, ensuite rooms, to minimise the risk of C. auris escaping from within the bed space to adjacent clinical environments. Any items within the space should either be cleanable with a disinfectant, or disposed of after a patient leaves. One thousand ppm of available chlorine should be used for cleaning, but needs to be used in concert with an appropriate contact time if it is to be effective.
WHO fungal priority pathogens list to guide research, development and public health action 2022
Outbreaks
Most detections of C. auris cases detected are colonisation rather than infection (though colonisations can lead to subsequent infections). Within the UK there have been 5 significant outbreak of C. auris, each with over 50 cases, in addition to many sporadic introductions of single cases, frequently from overseas. Many of these have been in London or the South of England, and have resulted in considerable disruption to services over a prolonged period of time. This disruption can, in itself, be a risk to patients as it can result in delayed access to care. Outbreaks are also financially significant, with outbreaks reported as costing over £1 million for a service impacted for 7 months.
Although outbreak numbers are currently small, they are becoming more frequent, and even if infrequent have significant impacts. The need to control this risk before it becomes endemic within the UK health system is therefore significant. It is crucial therefore to collect more data and understand transmission routes of C. auris better.
Despite probable under reporting, it is clear that C. auris is becoming more common within UK healthcare settings, and has the ability to both cause significant issues for both individual patients and for services, due to outbreak impacts. Although fairly new on the scene there is increasing recognition of how C. auris could change fungal risks within healthcare, and even long stay residential settings. If we are going to adjust approaches in order to react to the new risks C. auris represents we need to both update our current practices, and invest in research, in order to learn how to do things even better. This is the reason that it feels important to share a post that is a little more technical than normal, both to help myself by learning more, but also to ensure that we are having conversations about an organism that has the ability to impact us all.
Dr Claire Walker has been a paid up member of the Dream Team since 2013, token immunologist and occasional defector from the Immunology Mafia. Registered Clinical Scientist in Immunology with a background in genetics (PhD), microbiology and immunology (MSc), biological sciences (mBiolSci), education (PgCert) and indecisiveness (everything else). Now a Senior Lecturer in Immunology at University of Lincoln. She has previously written many great guest blogs for The Girlymicrobiologist, including one on turning criticism into a catalyst for change.
What may be less well known, even to regular readers of this blog, is that she did her PhD on finding genetic diseases, and as this ties in so well with the recent blog series I’ve been doing on DNA I thought having a guest blog from Claire might be the cherry on top of this particular ice cream sunday!
If you’ve missed any of the blog series of posts, especially if you want a refresher on how DNA works before reading about Claire’s work, I’ve included links to all the posts the below:
Having spent some time covering what is however, I thought I would follow up with a couple of book reviews that focus on how the world of DNA, DNA editing and DNA interpretation could change the lives of everyone involved.
When I was 26 I finished my Clinical Scientist training and was offered a full-time position at the hospital I trained in, with a good pay increase and a view to becoming a laboratory manager in the next few years. It was a great gig with a lovely team, good earning potential and support to further my clinical training. Unfortunately for them, I had just completed a secondment to a famous children’s hospital and had my mind absolutely blown. I had seen how immunology was being influenced by the study of human genetics, at the forefront of the field with cutting edge techniques which seemed, frankly, indistinguishable from magic. Suddenly, working in adult rheumatology and learning how to manage NHS laboratory budgets just didn’t seem so interesting anymore. So I turned down the job, went home, looked my husband in the eye, and said the words he’d been quietly dreading ever since I’d first jumped from environmental microbiology to human immunology: ‘I think I want to retrain… again.’
I applied for a PhD in genetics and immunology at University College London Institute of Child Health. Specifically, I focused on children with rare syndromes that didn’t have a clear diagnosis often called “syndromes without a name.” These kids and their families had often been on a long and frustrating diagnostic journey, seeing specialist after specialist, with no real answers. That’s where exome sequencing came in. By reading the protein-coding parts of the genome — the exome — we hoped to find clues hidden deep in their DNA that could point to the cause of their symptoms. Think of it like a high-stakes game of genetic detective work. Each patient’s exome was a puzzle, and sometimes, we’d find that one variant that explained it all. Other times, we discovered new candidate genes that had never been linked to disease before. Conversely, we found that some quite well-known genetic diseases could have highly unusual presentations – what we call expanding the clinical phenotype of a condition.
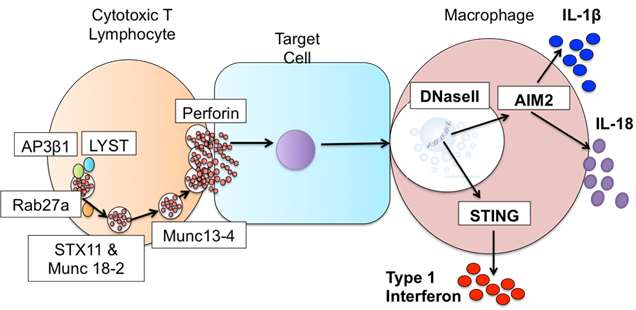
The disease I was assigned to work on was the oh-so-easy to pronounce and explain, Haemophagocytic Lymphohistiocytosis (HLH). HLH is a rare but serious condition where the immune system goes into overdrive and won’t switch off. Instead of protecting the body, it causes severe inflammation and can damage organs including the liver, brain, and bone marrow. It can look like a really bad infection, but it’s actually the immune system attacking the body from within. Some cases are triggered by infections or cancer, but others are caused by inherited defects in genes like UNC13D or PRF1. The children in my student were amongst the big chunk of patients where none of the usual suspects showed up on molecular testing.
But finding a genetic change through exome sequencing was only the beginning — I still had to figure out if it actually meant anything. Not all changes in our DNA cause disease, so we looked for the presence of the mutation in healthy controls and used predictive software like PolyPhen2 to solve the first clue: what would this mutation do to the protein the gene encoded? Then came the hard part — proving it. I had to design and run experiments to test how the genetic fault affected the protein’s job in the immune system, and whether that could explain the symptoms we were seeing in the child.
The hard work paid off, in my study we found: one case that was UNC13D protein defective HLH, but only affected the brain; one that turned out to be a totally different (and very rare) immune disorder; and one that revealed a brand-new genetic disease caused by defects in DNaseII resulting in something akin to HLH and another inflammatory condition. In all of these cases what this really gave us was the opportunity to get these kids an answer and onto treatment that could actually work for them.
Figure 3. Defects in DNaseII sit downstream of defects known to cause HLH. Image credit – Claire Walker, thesis.
For me what’s really fascinating about genetics is that what took me years of research is fast becoming a routine test – an incredible reminder of how quickly genetic technologies can evolve. What was once a complex puzzle of genetic mysteries is now providing families with the answers they’ve long needed, turning uncertainty into hope and paving the way for more personalized, effective care in the future. I think that alone was worth putting my husband through yet another ‘re-training’ episode, who knows what I’ll come up with next?
I hope this addition has given you an insight into why working to learn more about how our genes impact us is so important, but also how needed specialists like Claire are for us to do this safely and make the difference we want to make. Sometimes all patients need is an answer, a name to put to what they are going through, something that can provide a route forward even if it doesn’t provide a complete fix. Something so simple can be so difficult to achieve, but just because something is hard doesn’t mean that we shouldn’t try.
Friday just gone, 25th April, was World DNA Day. I’ve had a series of blogs that I’ve been playing around with linked to both DNA in our everyday lives and two book reviews where the world changes because of genetic testing and genetic manipulation. I thought I would write these posts, because as much as artificial intelligence could change the way we live and is frequently discussed, we are all accessing DNA based testing more and more, with many of us not really thinking about how this too is changing the world in which we live. Depending on how you feel about science and needing to have a refresher on what DNA and how we look for it and interpret it, you may want to hit up part one of this blog series first.
In part one I also introduced the kind of testing that DNA and DNA sequencing can be utilised for, not just in a accredited healthcare laboratories, but also linked to private companies who offer information on things like ancestry. In today’s blog I wanted to go a bit more into what can be the less thought about results of sending away your DNA, and also what kinds of things you might want to think about, or have in place, before you do.
Thinking unexpected consequences?
In part one I used this quote from a recent article:
As stated in a recent Independent article:
As they’re based on estimates, I suggest treating home DNA tests as a fun investigation to get to know your family history a little better rather than a to-the-letter representation of everything that’s ever happened in your gene pool – Ella Duggan Friday 28 March 2025
It describes sending away of your DNA as a fun investigation, and recommends not taking the results too seriously. This is definitely the right attitude in many ways, as you wouldn’t take key health guidance from a magazine quiz, you’d want to speak to a healthcare professional who can put your results in context. The problem with not taking the tests themselves too seriously is that we don’t really think about the consequences of taking them or where the results might lead. My family have been given these for Christmas, for instance, and it was seen as a fun piece of science that could be done after lunch. Taking and sending away your DNA, the thing that makes you you, however, should always be done with a little more consideration that that. So I thought it might be useful to use just a couple of examples of why.
Health services
Sending away DNA for health reasons to private companies has been controversial ever since it was introduced into the UK and there are a few reasons why this is the case.
Firstly, if you have health concerns, then really you should be accessing medical care through healthcare professionals who you’ll be able questions, and who can put your results into a risk context for you based on your own medical history, rather than just getting a list of genes in isolation.
One of the other reasons you should manage this form of testing through health providers is that you can then be linked into any medication or further testing that is required. The presence of a gene alone can be pretty meaningless, you need to then look for whether that gene is being expressed (see part one) in order to really understand it’s impact, and so there are likely to be follow up requirements to any results received.
If you are going through genetic testing, especially if it has impacts on decision such as reproduction, you would normally be supported through the process ahead of the testing, and when the testing is returned, through professionals such as genetic councillors. If you get your results by sending your DNA away you may get completely shocked and surprised by the results that you can get back, and may make some decisions based on the findings that may not be correct for you and require better input from someone more used to interpreting the results. It could feel like a really lonely way to hear bad news.
Finally, these tests are being sent off to laboratories that don’t require accreditation. They are acting as medical tests, without going through the rigor that is required for the equivalent tests in healthcare, and yet are interpreted, by some, in the same way, and therefore effectively out of context. They may also not have the required levels of validation linked to the information and interpretive guidance that is issued with a result, so that you know what being present or absent for gene X or Y actually means for you. It also means that there may be less processes in place to ensure that you get the result that is actually meant for you and not for Professor X down the road. If you are processing hundreds of samples this kind of error, without safety checks, can be easier than you’d think. Knowing the quality of the result you are receiving may be less than obvious.
Ancestry services
OK, OK, I can hear you say. I wouldn’t send my DNA off for medical testing, but surely sending it off for ancestry services is ‘no harm, no foul’ and just a bit of fun. My first caveat here is that not all ancestry services are the same and not all of them look at the same sections of your genome. Some will look at your mitochondrial DNA (which will always come from your mother and your maternal line) in order to give a view of where your ancestral DNA comes from over generations. This is often referred to ancestral origins, and is much less likely to hit you with real time life dilemmas. Many kits are also paired with items that look at wider genomic matches, or DNA matches, and so you may get back more than you bargained for if you didn’t look closely at what was going to be provided.
I’ve included just a couple of, extreme, examples of how these kinds of unexpected consequences can play out in real life. The first is a BBC News story that came about because a woman was contacted by a stranger after sending off her DNA via an ancestry site. From the results it eventually became apparent that she had been accidentally swapped as a baby in a hospital in her 50’s with another child. Thus having dramatic and rather unexpected consequences for her and her family.
The other example I’ve included links to a couple of documentaries where the use of DNA matching platforms has uncovered serious misdemeanors or crimes, including IVF undertaken using the sperm of medical professionals without the knowledge or consent of the parents involved, and sperm donors being involved in the insemination of more couples than disclosed, thus increasing the risk of their children potentially interacting/dating/mating in later life without knowledge of their genetic linkage. This is obviously not the fault of the DNA matching service, and is something that is beneficial to uncover and stop, but has hugely dramatic impacts on those involved without any prior warning or support in place. It certainly wasn’t what they expected when they sent away their swab.
Is it just human DNA that counts?
Finally, to follow up on the takes of the unexpected, and because infections are fascinating, I wanted to share a link to a video that I think is really great about the first time DNA testing of HIV was actually used to convict someone of a crime. This one isn’t a word of warning, as I suspect that none of us are going to decide to deliberately inject someone with HIV contaminated blood, but I wanted to end this section with something where the use of DNA testing in the hands of people who really know what they are doing is a powerful tool for good. Also, because I wanted to give a non-human example of where I think some of this may go in the future.
What do we need to know before we start to send our DNA away?
Having laid out my warning stall, I wanted to go through some things I think you should actively think about before sending your DNA away.
What is the legal situation?
First and foremost, the sending of DNA away for processing is covered under something called the Human Tissue Act or HTA (in England). I’m flagging this as the first thing as, unlike what you see on TV, you should not be taking DNA from other people and sending it off to see what it says, and especially not for any form of DNA match testing. In the UK, if you do take anyone’s DNA sample without them being aware of it, it is considered a violation and you are liable to prosecution which can result in up to 3 years imprisonment. It is not OK to steal someone else’s DNA without their consent! There’s a lot to this one and I’m not a legal expert, but it seems to be something that many people are not aware of and now you know.
What level of information will be gathered?
All of the different tests offered will do things, and companies interpret the results slightly differently. It’s incredibly important to know what you are sending your DNA away to be tested for, how it will be tested and what kind of information you can expect back.
The main types of DNA tests and the areas they analyse are:
Autosomal DNA Tests = examine the 22 pairs of autosomes and the X chromosome. Commonly used for ancestry testing and can help determine ethnic origins, identify genetic predispositions, and find relatives. Utilise single nucleotide polymorphisms (SNPs), which are variations in a single DNA base pair
Y-DNA Tests = analyze the Y chromosome, which is passed down from father to son. Used for tracing paternal lineage and can be helpful in genealogical research
Mitochondrial DNA (mtDNA) Tests = use mitochondrial DNA, which is inherited maternally (from your mother) used for tracing maternal lineage and can be helpful in genealogical research
Paternity Tests = examines specific regions (loci) on the chromosomes to look at parental relationships
Health-Related Genetic Tests = looks for specific genes or regions of the genome that are associated with certain health conditions to try to identify genetic risks, diagnose genetic disorders, or assess treatment options
You may need to read the small print to really understand how the testing will be undertaken and to manage your expectations. If you can, make sure you look up examples of what the results you will receive will look like, and if there would be any follow up support given. Also, crucially see if there will be additional funding required to get access to the full data set you are expecting so you don’t get hit by any unexpected requirements.
How will data be used?
The next few sections are all linked to what happens to the results of your testing that you are sending away.
The first thing to check before you send off your test is how long will your data be stored for once. This is important for you in terms of being able to access reports, but also about how long your legacy data will be available. Will you have access to wider information if you request it to be passed to your healthcare provider? Is there any information on the data analysis tools used? Are you even allowed to ask questions or is all patented and under intellectual property rules, which is reasonable but you should know what the boundaries are. Most healthcare reports should be kept for at least 10 years, but as these are covered under different guidance, will you only have access to download your data for a set period of time? Will it be possible to get your own local back up of your data? Once you know the answers to these questions you can then make active choices and comparisons about which aspects are important for you.
The article below is a little old, as it’s from 2018, but many of the questions still stand. How carefully will your data be ring fenced? You may not think about it much, as your DNA may hold little financial value to you, but DNA databases are one of the main assets that companies who process your DNA have, and why the testing is actually relatively cheap. Having access to thousands of DNA sequences, along with medical histories sometimes, means that data is incredibly value for scientific and commercial development. This is OK, we need sequences to develop new testing. Pharmacy companies also need access to sequences to develop and model new medicine. Therefore, it is likely that your data monetised and used for other purposes, which may or may not be OK with you. The big question to ask is whether it will be anonymised and how it will be used. Knowing this information before you commit allows you make informed choices, as not all companies are likely to be identical in how they handle things.
Another aspect that you might not think about is data security. If your data is of value to the company, and therefore is a potential asset, then it may be of interest to others. This can make data security to prevent things, such as hacking, important. This could be especially true if your DNA reveals linkages of significance, or things that you might not wish disclosed, such as cancer risk. Doing some research to ensure the security of any data that is held is important, but not often high on the list of questions that people ask.
Who can data be released to without my knowledge?
I’ve talked above about who will have access to your data, but mostly I talked about your anonymised data. It may not just be anonymised data that you are concerned about by however. If you are sending off for testing that relates to cardiac, cancer, diabetes or other risks, than this can have much wider impacts if shared. The legal landscape in relation to this is very much changing and catching up with the concept of genetic information as a protected asset is slow. Also, warning, I’m no expert in this. However, when sending away for this kind of testing it is important to know that it is often not covered by medical confidentiality, as it’s not considered a medical test when conducted via private companies. Being aware of how this impacts the rules around your data and what the company will or will not release is key. Why is it key? Well, it can impact all kinds of insurance schemes, from requirements to declare for holiday insurance if you are seen as ‘knowing’ a risk, to life insurance changes in cost or profile if released directly to the company. Knowing whether your personal, non-anonymised data can or will be released is essential before choosing whether or to whom you’re prepared to send you swab away to.
I suspect that this last point will probably impact those of you reading this blog less, but for to complete this list…….your DNA can also be released to law enforcement, depending on the country, so if you’ve secretly been a mass murderer then maybe don’t send your swab away and get your DNA added to a mass database.
What will happen if the company is sold?
As I said earlier, one of the biggest assets these companies hold is the databases of DNA sequences which we provide them. When something happens to the company therefore, it is this asset that many of those interested in the company might be after, and they may have nothing to do with the purpose you sent your testing for. Reading the small print before you send away your sample may not be able to prepare you for what happens when those rules change and you are no longer dealing with your original commercial provider. The one thing you can do in these circumstances in understand what access and rights you have to request that your data is deleted, or to delete it yourself, in the case that circumstances change.
I’m aware that the section above on what you might need to think about is pretty heavy and so I wanted to finish part 2 on something a little more population level and upbeat in relation to why having access to this testing is a good thing for science in general. For instance, we know that the ability to undertake ancestral testing was a reason that the bones of Richard III were identified and confirmed, which had big impacts for history buffs. It show that the use of wider availability of testing has all kinds of benefits, and not just to science. In terms of wider science, being able to look at bones using DNA testing has supported identification of Mycobacterium tuberculosis as present in Egyptian mummies which has helped us understand the evolution of this infection over centuries. More recently, looking at the development of Homo sapiens and how we became the human beings we are today has been forever changed by wider applications of these methods. Use of these technologies can therefore impact all aspects of our lives moving forward, and it really is up to us, both as individuals and as a society, about where they work for us.
Parts three and four of this blog series will be linked to book reviews that explore what those futures could looks like if the use of DNA testing and genetic manipulation change how we look at ourselves and others. So join me in continuing to explore the power of DNA.
Friday just gone, 25th April, was World DNA Day. I’ve had a series of blogs that I’ve been playing around with linked to what DNA is, how we look for and investigate it and how we are exploring DNA in our everyday lives. Linked to this I’ve also got two book reviews coming where the world changes because of genetic testing and genetic manipulation. So this is the first of four part DNA bonanza.
I thought I would write these posts, because as much as artificial intelligence could change the way we live and is frequently discussed, we are all accessing DNA based testing more and more, with many of us not really thinking about how this too is changing the world in which we live.
I remember really clearly the first time I actively came across the concept of DNA, DNA testing and DNA manipulation. It was in Jurassic Park, when Mr DNA pops up at the start of the film to talk you through how they used DNA and cloning in order to make the dinosaurs. This film came out in 1993, I was 13 and I just remember how all of my class were queuing up to get tickets. It was the first film I really remember there being hype about, well that and Aladdin which was a different kind of seminal moment. It was the first film I remember watching and thinking just how cool science and scientists were.
In fact I talk about Mr DNA so much that the wonderful Mr Girlymicro brought me a Mr DNA Funko pop which lives on my desk at work and reminds me that the impression we make on people stays with them.
What does all this have to do with how we use DNA now? Well, in 1990 when Jurassic Park came out, the routine use of DNA, even in research, was still pretty much science fiction. The structure of DNA had only been described in 1953. Polymerase Chain Reaction (PCR), which is the main way we investigate DNA, had only been developed in 1983, and was only starting to become more widely available in the 1990’s. When I started working within healthcare in 2004, we were only really just starting to move from PCR being something that was used in research to something that was common place in clinical diagnostics. The leap from there, to a world where thousands of us can swab ourselves at home and post samples off to be diagnosed with SARS CoV2 during the pandemic, or to get information on our genetic heritage, would have sounded like something that would only occur in a science fiction novel if you’d mentioned to me back theb.
Just a flag, this part one post has a lot of the technical stuff linked to what DNA is and how we investigate it. You may want to skip this post and head directly for part two if you don’t want to be reminded of secondary school science, but if you can bear with me I think it will help some of the context.
What is DNA?
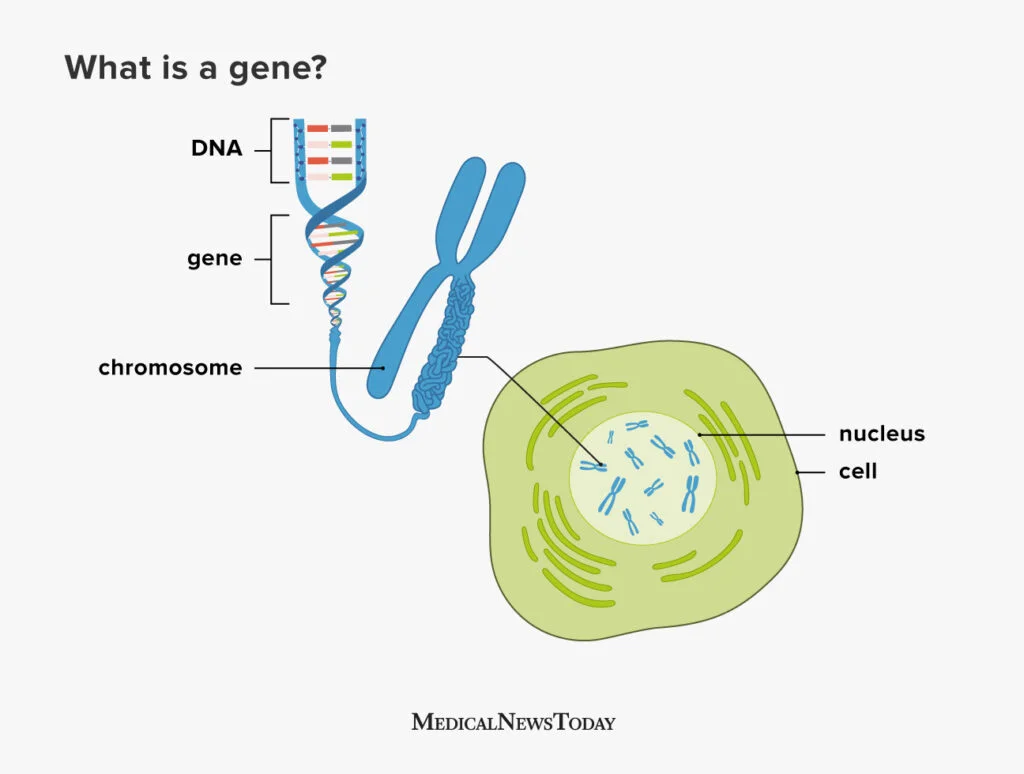
DNA, or to give it its full name Deoxyribonucleic acid, is commonly referred to as the building block of life. The structure of DNA consists of a double-stranded helix held together by complementary base pairs. The nucleotides that form the base pairs are adenine, thymine, guanine or cytosine. These nucleotides act to link the two strands together via hydrogen bonds, with thymine always pairing with adenine (T-A) and guanine always pairing with cytosine (G-C).
Sections of DNA then combine together together to code for genes, which are sections of DNA that work together in order to code for proteins, that then permits the expression of our DNA in physical form.
Genes are organised into chromosomes or packages of DNA. Each chromosome is formed from a single, enormously long DNA molecule that contains a strand of many genes, with the human genome containing 3.2 × 109 DNA (3,200,000,000) nucleotide pairs, divided into 46 chromosomes formed from 23 pairs (22 pairs of different autosomes and a pair sex chromosomes).
So how do we get from DNA to proteins? The specific sequences of nucleotides that form our DNA are arranged in triplets (groups of three). To turn DNA into protein, it gets transcribed into RNA (ribonucleic acid) within cells, with each of these triplets coding (translating) into an amino acid, which then get combined together to form proteins. The amino acids combined dictate what form and function the resulting proteins takes. Proteins then serve as structural support, biochemical catalysts, hormones, enzymes, and building blocks for all the processes we need to survive as humans.
Long and short, everything comes from your DNA, it’s super important, and is unique to you, but it’s structure is complex and there’s a lot of it in each of us.
How do we investigate DNA?
Now that we know about what DNA is, and how important it is for life, not just for humans but for all living things, it makes sense why so much time and energy has been deployed into understanding more about what it means for us as a species, as well as for us as individuals.
I’ve mentioned that PCR was first developed in the 80’s but didn’t really come into routine clinical testing until the 2000’s. What is PCR though and how does it work?
I often describe PCR as a way to look for DNA that is similar to looking for a needle in a 25 story block of flats sized haystack. The human genome is 3.2 billion base pairs, and we are often looking for a fragment of DNA about 150 base pairs in length, 1/21 millionth of the genome. It’s quite the technical challenge and you can see why it took quite a while to be able to move from theoretically possible to every day use. What makes it even more complicated is that you need to know what that 150 nucleotide fragment is likely to contain or where it is likely to be positioned within those 3.2 billion base pairs to really do it well. The human genome was not fully sequenced, and therefore available to us to design against, until the year before I started my training at GOSH, 2003. The progress therefore in the last 20 years has been extraordinary, and I can only imagine what will happen in the next 20 years. Hence the book reviews that will be coming as parts 3 and 4 of this blog.
So, how does PCR work? Well the first thing to say is that there are actually a number of different types of PCR, although the basic principles are the same. For example, there are some types of PCR that target RNA. There are also types of PCR that are used more frequently within clinical settings for things like SARS CoV2 testing, that are called Real Time PCR, called that as results become available in real time rather than waiting for the end of the process. It is for Real Time PCR that the small ~150 nucleotide fragment length is an issue. So all of these processes have their own pros and cons. Like many things in science, you have to use the right process to answer the right question.
The basic principles shared between types of PCR are as follows:
Designing your primers:
Primers are the pieces of DNA that you design and make that will stick to your target piece of DNA you are interested in. The reason this works is because of the fact that the nucleotides that make up DNA are complimentary and so A binds to T, C binds to G. As DNA is double stranded you can design your primers (your equivalent to the magnets to find you needle in your haystack) so that they will bind to your specific target (the piece of DNA you are interest in). If you want to have your primer stick to a piece of DNA sequence that reads AAG CTC TTG, you would design a primer that ran TTC GAG AAC using the complementary bases, make sense?
You design one set of primers for one strand, this is called your forward primer (moving from 5′ to 3′), and then you design your reverse primer at the other end of your target for the opposite DNA strand (moving from 3′ to 5′). Doing it this way means that when you start your PCR process you end up with complete copies of your target. You will then successfully have pulled the needle from your haystack using you targeted magnets.
Undertaking the PCR:
Once you’ve got your primers (which you can just order in once designed) you can then get onto the process of the PCR itself. You combine your sample that you think might contain the DNA target you are looking for (be that human, bacterial, environmental etc) with the reagents (chemicals) that you need to make the process work all in a single small tube. This tends to be a delicate process that needs to be undertaken at controlled temperatures as the protein that runs the process (Taq polymerase) is delicate and expensive. To do this we combine:
DNA Template: This is the sample that contains the DNA target you want to amplify
DNA Polymerase: Almost always this is Taq polymerase which is used due to its heat-stability as it originates from a bacteria that lives it deep sea vents. This allows it to function at the high temperatures required for PCR and is used to make the new DNA copies
Primers: These are the short, synthetic DNA sequences that you design to attach to either end of your target DNA region. These then allow the DNA polymerase to add nucleotides to create the new DNA strands
Nucleotides (dNTPs): These are single nucleotides (bases) that are then used to build the new DNA strands (adenine, thymine, guanine, and cytosine)
Buffer Solution: This solution provides the optimal conditions (pH, salt concentration) for the enzyme to function properly
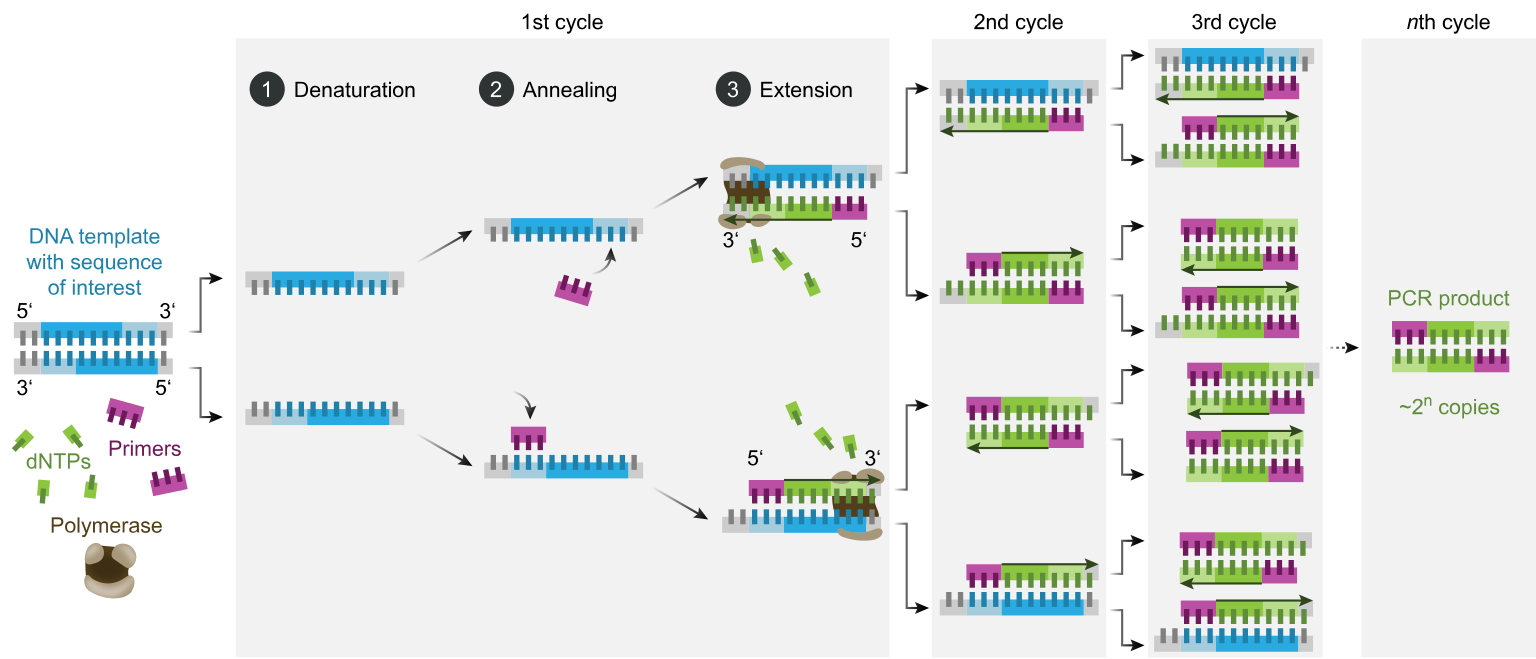
Once you have your reagents you then put them on a platform that heats and cools for different steps to allow the enzymes to work and for the new DNA strands to be created:
Denaturation: The double-stranded DNA template is heated (typically to 95°C) to separate it into two single strands. This step ensures that the primers can access the DNA sequence of interest
Annealing: The temperature is lowered (typically to 50-60°C) to allow primers to bind to their complementary sequences on the single-stranded DNA. This is the step where your magnets find their needle
Extension: The temperature is raised again (usually to somewhere around 72°C, the optimal temperature for Taq polymerase activity). Taq polymerase extends the primers by adding complementary nucleotides based on the DNA sequence to create new copies of the original DNA target
These three stages are repeated in cycles, typically 20-40 times, which results in thousands and thousands of copies of the original target to be created, so that eventually your 25 storey haystack is made up of more needles than it is hay, and therefore it is easy to find what you are looking for.
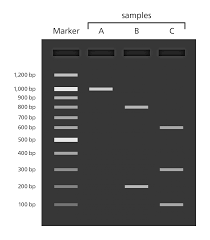
Interpreting your results:
At the end of your PCR step, if you are using traditional PCR, you run what is now called your PCR product or amplicon (the things you’ve made) through something called a gel. This is just a flat jelly made of agarose (or seaweed) which also contains a dye that binds to DNA and allows to separate your DNA based on size. This allows you pick out where you have samples that have the massive amplification you are looking for, as you can see it as a band within the gel. If a band is there and the right size (as you know how big your target was supposed to be) this is a PCR positive.
If you need to know more detail than whether something is present or absent, for instance if you need to know not just that a gene is there but which variant of a gene is present, you need to be able to tell what the nucleotides that were added between your two primers actually were. To do this, you will follow up PCR with a process called sequencing.
You take your target PCR’d section and then put it through a process to work out what the nucleotides added were. This involves doing the PCR process again, to make even more copies, but the nucleotides added into the reagent mix have fluorescence attached so you can tell which ones have been added during the PCR process. G’s often produce a black colour when hit by light, A’s green, T’s red and C’s blue.
For our original sequence we talked about, AAG CTC TTG, the sequence would read Green, Green, Black then Blue, Red, Blue followed by Red Red Black. Colours are then back interpreted into a DNA sequence (a series of letters) and there you have it, you know what the DNA is between your primers and you can then interpret your sequencing result. If you have large fragments of DNA you are interested in, you may have to do this in overlapping segments and put it back together, something like a jigsaw, before you can get your answer, but the basic process is the same.
What can DNA tell us?
As I’ve said, the search for DNA and specific genes has become an increasingly normal part of providing diagnostics in healthcare. Most of us will have sent off a swab for a PCR at least once during the COVID-19 pandemic. PCRs are frequently used in my world of infectious diseases to see if a bacteria is present or absent. They are also used so that I am able to see if a bacteria will respond to an antibiotic, by seeing if they carry antibiotic resistance genes, which can be crucial to getting patients on the right treatment at the right time.
Looking for specific variants of genes is also key to making sure that the treatments we give also don’t cause any unexpected consequences. A good example of this is when we use PCR and sequencing to look at genetic variants of a gene called MT-RNR1. A specific variant in this gene, m.1555A>G, is known to increase the risk of aminoglycoside-induced hearing loss. Aminoglycosides are a crucial antibiotic class that are used pretty widely, but especially in management of some conditions such as cystic fibrosis and certain types of cancers. A small number of people have a gene that makes them prone to something called ototoxicity as a result of taking these antibiotics, resulting in hearing loss. If we know a patient has this gene variant we can then choose to use different antibiotics, improving patient outcomes and avoiding a life long hearing impact.
Outside of screening linked to patients presenting with specific conditions, the use of DNA sequencing is being utilised more widely to look for genes or conditions before they even present with symptoms, in order to reduce time to diagnosis, and hopefully to be able to find patients and start management before they’re impacted or even present as unwell. A great example of this is the newborn screening programme that started last year. This screens newborns using the heel pricks of blood taken at birth so that rare diseases that could take months or years to diagnose by traditional means are picked up early in life, therefore allowing appropriate treatment to start earlier and hopefully saving lives.
DNA is fascinating and I love knowing about it. It’s not just me though. In recent years there has been an increasing trend for people to send off their DNA for other purposes than to hospitals for clinical testing. I’m not going to say too much about this in part one, but it was this that really inspired me to write these posts in the first place and is the main focus of part two of this blog series.
Just a quick google however provides a wide number of different companies offering a variety of DNA testing services outside of the NHS (NB I don’t advocate for any of them):
Crystal Health Group: Operates a network of DNA testing clinics, offering relationship testing and other services.
23andMe: Provides DNA testing for health, ancestry, and other personal insights.
Living DNA: Focuses on both ancestry and wellbeing-related DNA testing.
MyHeritage: Provides DNA testing, particularly for ancestry research.
AncestryDNA: Company specialising in DNA testing for ancestry discovery.
The complication with all of this type of provision of testing is that outside of the clinical world in the UK, where testing should be undertaken in accredited laboratories and reporting of the results must meet certain standards, sending off DNA to private companies is much less monitored.
I hope you can see by some of the technical descriptions just how complicated these DNA processes can be. How time consuming, and how expensive to get right. There is also a lot of nuance about the different types of PCR, sequencing, gene targets, and results analysis that can be offered under the umbrella of ‘DNA testing’. Without the right people involved to make sure that there is embedded quality assurance challenges could arise, depending on what kind of testing is undertaken.
As stated in a recent Independent article:
As they’re based on estimates, I suggest treating home DNA tests as a fun investigation to get to know your family history a little better rather than a to-the-letter representation of everything that’s ever happened in your gene pool – Ella Duggan Friday 28 March 2025
The devil for all of these things really is in the detail, and we’ll get into that detail much more in part two! For those of you interested in learning more about the history of DNA testing, I’ve included a talk below. Happy World DNA Day
There’s been a bit of a delay posting this one, as it was supposed to come out a couple of weeks ago, but I ended up needing to take a bit of a well-being break. Healthcare Science week was a brilliant blur but full on and, for once, when I went on leave I decided that all work, yes even this blog, needed to be put on hold so I could have a complete break. I hope absence has made the heart grow all the fonder……
Now, onto the science
At the start of Healthcare Science week, my family and I, because they love me, went for a night out to experience a different type of science…..forensic science. I wanted to go to see ‘Walking into a Murder Scene: an evening with Simon Fowler‘ by First Forensic Events for 3 reasons:
The first is that I think it is really helpful to engage with science beyond your discipline for inspiration and ideas. In this case, I’m not a big true crime fan or anything like that, but I was interested in how they deal with technical challenges we both share, such as low volume detection of targets by PCR amplification from human blood, as this could help with sepsis detection in clinical settings.
The second is that I have a long-term plan to write some pathology murder mysteries, by long term, I mean it’s my retirement plan, and so I also thought making some science notes could be helpful as success is mostly in the preparation.
Finally, I try to engage with science outreach wherever I can, no matter what the topic. I wrote a blog here last year about aviation outreach at a massive airshow known as RIAT and what learning that triggered for me. I really believe in seeking out and engaging with these opportunities, firstly because they do a lot to inspire me as to what more I can do. Secondly, because why reinvent the wheel? Learn from others about what works well and how I could switch up what I do. Last and by no means least, if we don’t support these people and these events, they may cease to happen. Finances are tight everywhere, and outreach is increasingly seen as a ‘nice to have’. Numbers talk, and so taking some time out of my day to be there to support others talking science is the least I can do.
The event was the first ones from a group known as First Forensic Events and was, in many ways, a trial run. The house was packed, though, and there was an obvious interest from those attending to just find out more about a world that most do not have access to. It got me thinking and as a result I thought I would focus this blog on what I took away in terms of how we, as scientists and Infection Prevention and Control professionals, could do more in terms of reaching out to a different audience and shedding some light on what we do to lift the veil in a similar way. I often think we don’t talk enough about the fascinating aspects of what it is we do for a living and this event made me realise that we are in position to share that with others and there are people out there who may want to learn more.
Location location location
The first thing I want to talk about is location. This event took place at the Royal Gunpowder Mills, which was objectively brilliant. One, it is not a place that is open that much to access, and so to be able to attend for an event already felt special. Two, it’s a place that’s interesting and quirky, and so even if people aren’t leaving and talking about how great your content is, they are likely to still be talking about what an interesting night they have had. I get pushed all the time to have events in cheaper and less interesting spaces because the costs need to be justified. The truth is, as much as we may dismiss them, locations can make or break events. Therefore, investing in them makes complete sense to me.
One of the reasons that location choice is so important is that it gives you the opportunity to really demonstrate that you have thought about the comfort and experience of your audience. Are there drinks available? What about food? How will people find their way to seats etc? Attendees will focus better on the content if they are not distracted by feeling hungry or thirsty or trying to understand where they need to be. They are also more likely to linger and talk to each other, which is key to both creating a buzz about the event and to permit natural network creation which will encourage future support.
A clear sense of identity
All things tend to be easier or work better if you have a clear sense of identity or what you want to achieve. This works for everything from advertising events and getting people into the room, to how people respond to the event itself. It is therefore worth investing a lot of time in both thought and planning in order to get this right, before diving deep into the practicalities and details.
When we spoke after the session it was clear that Simon’s focus was linked to training. His unique selling point (USP) for the session was to demonstrate not only some of the interesting cases he’d been involved in but also why and how he got into the work he did. He was also very clear that, in the same way we always want to focus on the patient, he wanted to make his sessions about the victims. Simon started off his session by talking about his core values and where he came from, in his case it was that he wanted a military career but that life turned out somewhat differently. He was diagnosed with Perthe’s disease which meant he was no longer eligible for military service, and so he then had to re-focus and choose a different life path. He built the start of his session up around his personal journey into science.
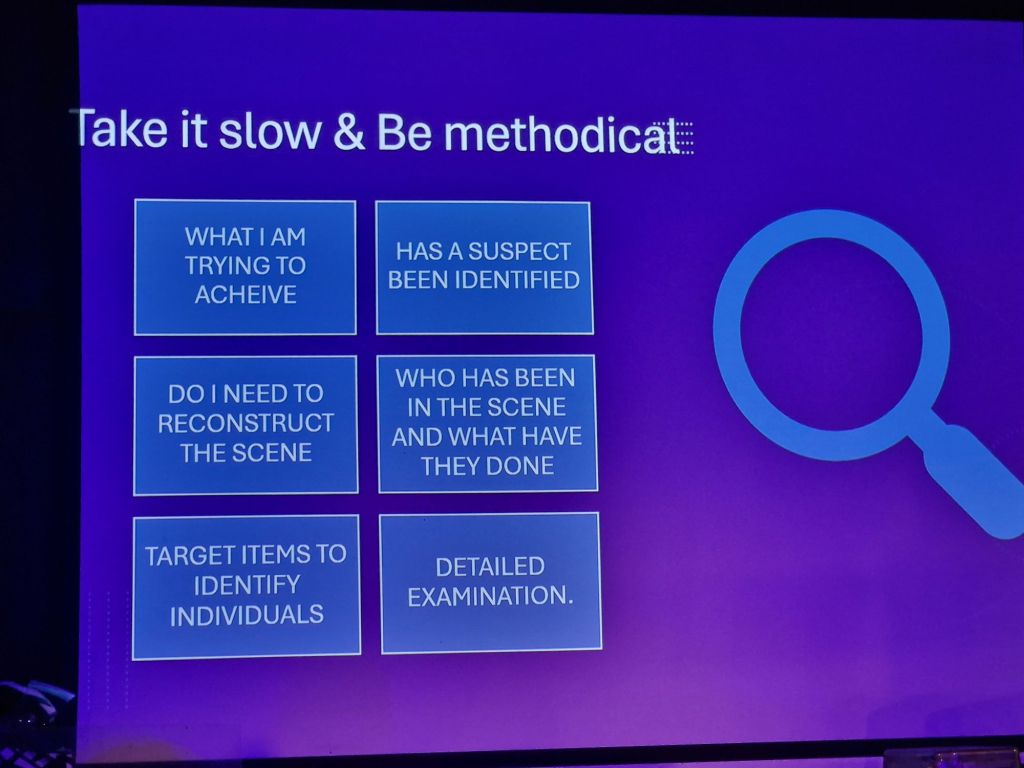
If we were to do something similar for health I think the need to be clear about our USP holds true, and for me, the things that seemed to engage the audience most were a focus on clear story telling with outcomes to show your role and it impacts i.e. what did you do and how did it change things? The other thing that seemed to really fascinate those present was discussion about prioritisation, outcomes and decision making. How do you decide what to do, in what order? How do you make decisions and how did those choices impact the end result? I suppose I’m talking about making thought processes an object of active discussion and raising awareness, rather than maintaining mystery or focusing purely on events. The stuff someone can’t find out by reading up about something on the internet and can only be got from a more intimate discussion based setting.
Back to the fundamentals
Keeping to the basics and planning, lets talk set up. Location is important but so is the staging. Everything from what you are planning to wear, to props and the tech that you will use. Is your outfit comfortable and accessible? Are you going super smart/business, that could be seen as hierarchical? Will you go branded or display your geek like tendencies with, for instance, a CSI T-shirt? All options are fine but they need to fit with your USP. Who are you selling up on that stage? Choose an outfit that fits with deliberation rather than as an accident.
Making the staging visually interesting is useful, especially if people are sitting for a while before everything kicks off. Offering an intriguing set up means that people will engage before you even start, as well as allowing people to speculate what might happen later. Having props that you will use draws your audience in.
It is important at the planning stage to also be considering accessibility. Too many people believe they have a loud enough voice that they don’t need mics etc. That works for some people but there will be people in the audience who you don’t reach and who will find it a barrier to engagement. Mics also allow nuance in terms of being able to go both loud and quiet as needed, rather than focusing constantly on projection. The same with slides if you are using them. Will they be accessible to people who are colour blind? What level of text is appropriate? What fonts may permit engagement? Should you be image heavy? In the case of something linked to criminal cases or health, how much do you show? Gore, surgery, infection etc can be triggering, so consider what level may be needed/appropriate. If you are recording (pictures, video etc) think how this might impact your staging and movement and if it will change your lighting requirements.
During the show itself, when we attended, there were some technical issues as the laptop running the slides stopped working. I think this is everyones worst nightmare, but has also happened to us all at some point. It reinforced for me that if you are relying on tech as part of your staging, you always need to have a plan B about how you will handle things if something happens to that tech. How you will you pivot? Having a plan means that you will be less flustered and therefore impact the experience less for those attending.
Selling credibility
Credibility is everything, whether we realise it or not. Setting up and selling your credentials is an important thing to do both before the event and early on during the establishment phase. Why should we listen? What do you know? What’s your experience….really? There are multiple ways that you can both do this and embed it. Thinking about how you are going to both establish and sell your credibility is something we don’t often consider and may take for granted, but if you are trying to speak to new people, especially outside of your field, it is something to really think about.
One of the great ways that it was done at the First Forensic Event was that someone else whom people may be familiar with, in this case Donal Macintyre, introduced Simon linked to both the event and by covering his skills and expertise. We all use testimonials in every day life and this setting was no different. I’d heard of Macintyre Investigates but as someone who doesn’t engage with a lot of true crime work the name didn’t mean much. It did however mean something to most others there, and he also talked about the TV work and others things Simon had been involved with in order to try to establish wider credentials. This is no different really to someone reading out your bio at a conference, but re-pitched to make it useful to a different crowd, and still well worth doing.
The other thing that Simon did was to acknowledge the other members of his crew. This was important for two reasons. One, because we should acknowledge that we are not single person armies and the work and support provided by others. It makes you not only more approachable but also acknowledges the work undertaken by other people to get us to where we are. In this particular case however there was another important purpose in acknowledging the other people who were involved, and that was to enhance the credibility of the event itself. The other people involved in First Forensic Events are other forensic scientists and police detectives, which aid to further establish credibility by inclusion in networks and experience. If others are willing to add their names to your events then it also demonstrates their backing and investment in your undertaking.
A story in three acts
We’ve reached the nitty gritty. How will you actually structure your event to achieve your outcomes? What are you trying to achieve? Simon was clear that it wasn’t just about factual presentation, but about him and his journey as a scientist. I think that was a really good decision and something that many of us as scientists should consider when working up our presentations. We are not science in isolation from ourselves, and so bringing your full self to these events is bound to be more impactful, and also helps to engage your audience more. For this purpose the session was structured around stories, stories about self, stories about action, and stories about impact. This kind of story based structure enabled the audience to really engage as the human ability to engage with oral tradition goes back to us sitting around campfires and learning through listening to tales.
The first third was based around learning who Simon was, what drove him and how he got into his work as a scientist. Fundamentally this section is about building of rapport as well credential building. It also enables the audience to settle in and for an expectation setting phase to be undertaken. The second third was a practical session. This is where Simon demonstrated some practical aspects of what a bludgeoning event could cause in terms of blood splatter, and scene investigation. This enabled a change in pace and energy, which breaks things up for people as they will have been sitting for some time at this point and changes it from being a didactic slide presentation. It also means people go into the break with a level of introduction of what may be discussed in more detail post break and therefore your audience can choose how much information they are comfortable with, and gives an exit opportunity if needed. This gives detail without inclusion of people or actual harm, and therefore allows engagement without emotional risk. The final section, post interval, was based on actual cases, still rooted in technical discussion, which supports focus on facts rather than emotion. This type of structure supports engagement and gradual submersion rather than attempting to shock.
Speaking to the room
This brings us onto the audience. How do we speak in a way that allows the audience to truly engage. I’ve talked about structure but there are other things that can help. The first thing we can do is do some scene setting. Making sure at the start of the session that everyone know how the event is going to work and what the rules are. This includes some basic things like telling people that there will be an interval, what time it will be and how long it will run for, so everyone can make sure they know how long they’ll need to engage. In the case of this particular event it also included scene setting around what might be shown and discussed, making clear the level of imagery etc in order to reassure and expectation manage. It also included being very clear that it was completely OK for people to leave and return at any point, as people may be triggered by different things, different memories, in order to reduce distraction by discomfort or concern about whether removing yourself would be acceptable. It also included the fact that there would be a Q and A, and that Simon and his team would be available for questions both within the event and during the breaks.
As with any science event it is worth doing what you can to avoid exclusion of your audience by thinking about how you will use technical terms and being weary of abbreviations. Many of us use abbreviations without even thinking about it as part of our engagement (I used the term PCR earlier) as it is part of our language. Those in the audience are less likely to have the same shared language however, especially if you are reaching out to a new audience. Making sure you allow time to explain any technical terms you are going to utilise is a key thing to practice. When you think you have explained enough you are likely to need to explain even further. As someone who doesn’t work in law enforcement some of the terms and abbreviations used in this event didn’t mean anything to me. That didn’t really impact my understanding or get in the way of the outcomes however, but made me remember how healthcare is filled with exactly the same barriers to full understanding, and that I need to be more careful about how I talk about my job also.
One way to make sure that you get feedback on how to improve and make tweaks on things like language is by making sure that the first time you do anything you add plenty of cheer leaders/critical friends into your audience. These people can flag and help you improve for future events, as well as providing some reassurance and friendly faces in the room to help alleviate your anxiety.
Maintaining accessibility
I’ve talked about accessibility already in terms of supporting your audience to logistically engage, but now I’m talking about connection. How do we make sure that we allow participants to connect with us, feel engaged with us, and fully share in the event. There are some key ways that I think this can be done, although sometimes it can be scary. I think the key one for me is allowing yourself to show vulnerability. Sharing enough of yourself that others can start to see you as a person. This includes sharing things such as values and drivers, but also sharing failure and things that did not go so well. Allowing people to see you as a person and not just a role.
The other part of this is being open and able to laugh at yourself, and allowing others to join you in that moment. All of this can be really shown in less structured moments. Moments where you make yourself available to engage 1:1 in breaks etc. Also, in a more open way by including moments where audience members can fully participate in things like Q and A’s. I always find it helpful to set parameters for these. Being open about the fact that there is nothing off limits, especially with kids. So they can ask what my favourite colour, is or how much I earn, or what I find the hardest, without restricting them to the science. Setting boundaries and expectations in general means that everyone knows what the rules are. Can you use your phone? Can people take pictures? Can people leave? All of which enables people to focus on engagement rather than attempting to predict what’s in or out of scope.
Pitching your future
How does it end? You’ve made it through, you’ve shown your full self. Hopefully you’ve felt that the audience engaged. You’ve made it through the Q and A. What do you do now? You need to make sure that you provide another opportunity to engage in the future whilst everyone is still paying attention. This is the moment to link to other opportunities, but this means you need to have those other opportunities set up and ready to share. What I’m saying is, as much as it’s crucial to focus on the right now, to make a real success out of events like these you need to be able to provide the next thing. So making sure you’ve planned ahead and have something else to sign post to is a key stepping stone to success.
Even if you don’t have another event planned you need to make sure you are thinking about marketing. What is your social media? Do you have a web page? Where can people go to find out more, either about you or about your future planning? Making sure that you have these things set up so that people can continue the engagement that they’ve started means that this is less likely to be a one off and more something that will be a stepping stone to future engagement. Having shown who you are and having brought people into your world, the logical thing is to make sure you have a plan for showing people what’s next.
So much that links us
So after all that, what did I think of forensic science. When I go to any of these things, what always strikes me is that we have so much that links us. Whether we are acting as detectives in finding an infection or a criminal linked to a crime scene, we are actually following very similar thinking and processes. We even use some similar techniques. I walked away thinking that I had been involved in a super cool event, but also struck by how brilliant it would be to do something similar for healthcare, and whether there would be anyone out there interested in setting something up. I left, as I almost always do, with my mind on fire with ideas and inspiration, and I wish to do so much more than I currently do. It reminded me how much we need to put ourselves out there and be brave. More than that even, it reminded me of how much the work we do is fascinating, and how interesting it would probably be to those that have never traveled in our footsteps. Perhaps even more so after the pandemic. So step up and step out, your audience awaits you!
It’s the 8th March, and we all know what that means…..It’s International Women’s Day!
This year, International Women’s Day is timed pretty wonderfully for me, as it happen to also be just as Healthcare Science Week is about to kick off. As both a woman and a Healthcare Scientist, I thought this was a great opportunity to combine the topics and talk about how these two things have impacted how my science career came about, and why I think a lack of recognition of both has incredibly important impacts on society as a whole. That said, this is also a post about how far we’ve come and the role that female scientific representation in the media has, and can have, on how we feel seen as women in science.
In what feels like a different life, where I was younger and had better hair, I was selected by the Royal Society of Biology to do some filming linked to raising the awareness of women in science. The session is short but was really interesting for me to do as it centered on who inspired me to become a scientist and how it happened. Now, many of you who read this blog will know all about that tale, but for context, I’ve linked to the video below:
The thing is, I suspect that there are still many people out there who might love to do science, and yet they’ve never had the chance to meet a scientist or really learn about the brilliant variability of a career in STEM (science, technology, engineering and maths). So what’s my point? Getting to actually meet and chat with a real scientist still feels like it’s a thing for the privileged few, not something that is available for mass consumption. You know what is available for mass consumption? TV and movies. This blog reaches 20 odd thousand people a year, a single episode of a TV programme, like Holby City, makes those numbers look so small they are not even worth considering. So it matters that the roles of female scientists within movies and on TV have not always been the most representative of either the careers available or the type of people that choose to engage with scientific careers. The reach and expectation setting that the media can have dwarfs any of the best efforts I can make across my entire career. Therefore, in order to celebrate International Women’s Day this year, I thought I would take the opportunity to talk through where we started with some of this representation in TV and the movies, and then celebrate quite how far we have come.
Why is it important to have women in science?
I kind of don’t believe I’m writing this section. This one should be a no brainer and yet I think it’s probably important to take a paragraph, especially with all the current commentary about equality, diversity and inclusion (EDI), to talk about why EDI matters.
The data supports the fact that we are far from a scenario where female representation in the workforce mirrors the distribution of women in the population. Worse than that even, is the fact that even if women make it into STEM careers they are doing less well than their male counterparts, including lack of representation in senior roles and general reduced access to research funding. There will be another post at some point about the source of some of these discrepancies but hint – it’s not because the women are worse at their jobs, that blog is still a little way away however.
One of the reasons for the lack of of women in STEM careers is that, according to work undertaken by Steinke et al in 2007, children are exposed to gender stereotypes and images of scientists through movies, TV shows and books where there is a lack of good representation of female scientists. They undertook work with primary school children where they asked them to draw a scientist, very few children drew female scientists and most listed media as the source of their inspiration. A similar study in Korea, in secondary school children, showed that only 16% of them drew female depictions of scientists. This kind of data backs up why media representation is so important, as you really can’t be what you can’t see. So many children do not realise that a scientific career is even a pathway that is open to them, if they are not fortunate enough to know one. If children can’t access what that career might look like through the information sources they access all the time then they don’t even consider it as an option for them when making their life choices.
But why should we care that we have less women working in science? What kind of difference do they make that we should try to move the dial on this?
Women make up just over 50% of many populations but much of the data produced by scientists, including clinical trial data, is biased towards male datasets. This leads to the outcome data for females often being less good. Some of this is likely due to a lack of female voice in the room when studies were being planned
There is often a research bias, where issues that purely impact women tend be under researched compared to issues that purely impact men
Inclusion of women in tech pipelines has been demonstrated to improved productivity and boost economic outputs
Science should be for everyone and therefore needs to include everyone. Science is best when it is seen through different lenses and priorities which different individuals bring to the table. Variable opinions drive improved change and innovation, so being inclusive is a win win
By increasing female representation in STEM we can switch up our focus from working to increase diversity and spending energy on being visible and role modelling, jobs that are overwhelmingly undertaken by women in STEM fields in addition to their day jobs, and allow women to compete better with their male colleagues by freeing up their time to focus on their science
What kind of representation did I see in the media when I younger?
Having talked about how important exposure to role models in the media are to encouraging women in STEM, I wanted to kick off by talking about the kind of representation I was aware of when younger and making decisions about my career choices. Now, a key disclaimer here, it appears that my teenage years were some horrific length of time ago, even though I’m blatantly still young, spry and filled with youth. Women, especially those in technical roles, often weren’t featured or were there to act as passive objects for men to respond to or act around. They were all too frequently there to be a foil for the men who were the focus of the storytelling. There wasn’t an abundance of female science representation in any of the media that I do remember, but what was present used to focus on 6 key stereotypes:
The Old Maid – the female scientist who is only interested in her work (and therefore not showing that you can be both a scientist and a person) who, as the film/show proceeds, has her female and emotional side brought out by the main male protagonist
The Male Woman – a female scientist who works in an all male environment. She is not as sexual a character as other women in the setting may be, but she is also not on the same level as the men she works with. She is often presented as having unhealthy habits, such as drinking issues, in order to show (it feels to me) that it’s unhealthy to try to be a woman in a mans world
The Naïve Expert – often a character in a film that is critical but does not contribute to any of the science solutions or really advance the story in any way. These often feel like box ticking roles or to aid the exposition of other characters
The Evil Plotter – usually a young and beautiful character who is there to trick the men within the film. They are set up to be hated by the both the other characters and the audience as they use their scientific knowledge and looks for evil. This one again strikes me as a way of demonising women who bring anything other than their knowledge of science and dare to be people with other needs as well
The Daughter/Assistant – this one is the typical smart and capable woman who is there as a subservient to a smarter, more well known, or more significant male character who will be the one to advance and resolve the plot whilst the female is there as a foil to show how smart and capable the male protagonist is
The Lonely Heroine – a woman who is depicted as intelligent and independent, and allowed to also be sexual, but somehow is not able to compete with her male colleagues. Usually, during the course of the story, she is gradually able to be seen and have an impact but only when she develops a relationship with a man who allows her to be acknowledged by others
Now, don’t get me wrong, all media and story telling is based on stereotypes and tropes, almost everything can be fit into a silo. That said, if the stereotype is only there to serve the male protagonists of the tale, that is a problem and it very much felt that way in films and programmes I watched growing up.
Scully effect
So what changed? I remember so clearly my first encounter with the The X-Files. It came out in 1993 (1994 in the UK) and I kind of missed it, but my sister and brother would not shut up about how great it was, so it took a while for this geeky 15 year old to discover Dana Scully and all of the science joy she would bring to me.
For those of you who don’t know anything about The X-Files (and you really should) according to Wikipedia ‘The series revolves around Federal Bureau of Investigation (FBI) Special AgentsFox Mulder (David Duchovny) and Dana Scully (Gillian Anderson), who investigate the eponymous “X-Files“: marginalized, unsolved cases involving paranormal phenomena. Mulder is a skilled criminal profiler, an ardent supernaturalist, and a conspiracy theorist who believes in the existence of the paranormal, whereas Scully is a medical doctor and skeptic who has been assigned to scientifically analyze Mulder’s case files.’ The reason that this series made such a difference for me, was because it was the first time that I saw a fully rounded female STEM character who was a person, with interests outside of her job, who was also an equal player in the story and able to challenge and lead within the series framework. She was more than just a foil, or a tool for exposition, and the number of times she was the one that did the saving became somewhat of a running joke.
It wasn’t just me that the character of Dana Scully had an impact on, her character led to what has been described as the Scully Effect. The Scully Effect refers to the phenomenon where women were inspired to pursue careers in STEM after watching The X-Files. This was the first time I think I really became aware of the power of the media to impact in more than a superficial way. The impression of this effect has been upheld by a recent study to try and capture some of the way that the Scully Effect impacted on those who watched the show, so you don’t just have to take my word for it.
There is no doubt that the role of Scully in The X-Files felt like a watershed moment for featuring women in STEM careers. Having just talked about the difference that Special Agent (Dr) Dana Scully made in terms of female representation in science I’m now going to excluding medics from the rest of this discussion as a) they are featured much more frequently in all forms of media and b) the lack of female scientific representation is one of the reasons that students see medicine as the only route open to them, rather than seeing the world of opportunities available within the world of science careers. (I still love you Dana, you’re still my girl)
So where did the change in TV go from there? Now, there are a few honorable mentions I’d like to give a shout out to, these are obviously based on my person taste, but I do think they are examples where things have continued to change for the better:
Bones is a police procedural linked to investigations of human remains undertaken by Professor Temperance “Bones” Brennan (Emily Deschanel), who is a forensic anthropologist, supported by FBI Special Agent Seeley Booth (David Boreanaz). Now, in many ways Bones fulfills many of the Old Maid stereotypes, but there are many key differences. For one, her intelligence is always held up as a positive and with high regard, and she is considered to be so valuable that her challenges with more emotional interactions are considered to be over whelmed by the value her intellect brings, which is quite a different take. Secondly, her emotional journey is mostly chaperoned by another female character in the show, Angela Montenegro, rather than relying on a male character for their character development (yes, yes, I know her and Booth get together but I’ll die on the hill that it’s secondary to Angela). Finally, and maybe most importantly, the character of Bones is very clearly signposted as being based on a real person, Kathy Reichs, who was also involved in making the show. As I said, representation is important and the fact that this clearly shows that you can be a successful scientist, and perhaps even close the circle and be inspiring enough to have a TV series based on you to inspire more young people, is a massive step forward.
Kathy Reichs
Two other TV science representations I love come from other police procedural or fantasy series, both are lab guys, all of which probably tells you a lot about who I am. These guys both speak to my heart as they are fully formed characters, not just single dimension caricatures of female scientists. They have flaws, they have passions, they are authentic, and most of all they love the science that is their calling. (this isn’t to say that science has to be your calling for it to be your job, I just love that there are representations of scientists on TV who love science the way I love science)
First, I’m kicking off with Abby Sciuto from NCIS. She’s a forensic scientist, who in that TV way has a world of completely different science skills rolled into one, but I still love that about her as she exhibits so much scientific curiosity. As an ex goth myself, one of the other things I love about her is her sense of self expression and not being limited or making herself smaller on the basis of what others think about her. She the opposite of those female scientific characters who rely on others to enable them to be people rather than lab coats. I fully respect and am so happy to see this kind of female science representation.
Second, is Ella Lopez from the TV series Lucifer, a TV series based on a comic where Lucifer, as the devil, abandons Hell to run a nightclub in Los Angeles. He then (for plot reasons) becomes a consultant to the LAPD and hi-jinks ensue. She’s also a forensic scientist who works for the LAPD, are you sensing a theme? I don’t know whether this is because of the kind of series I like, or whether the writers of these kind of series just feel like they have more time and scope to devout to full character representation. The reason I love Ella is that she is the complete opposite of the Old Maid/Male Woman stereotype. She is the emotional heart of most scenes, and is accepted for bring her full emotional quirky self to the table. As someone who often feels judged for wearing her heart on her sleeve, I love this is represented as a strength in this characterisation of a female scientist.
Let’s talk movies?
So what about the movies? In some ways female scientific representation is always slightly more challenging in films. Slightly due to the nature of the medium, there is often less opportunity for character development (as you have a few hours vs multiple episodes) and so they still tend to fall very much into some of the stereotypes already discussed. There is still a strong tendency for strong female characters, when present, to still fulfill the Evil Plotter stereotype, and the film industry in general struggles to have female roles that are not reliant on male roles for context. That doesn’t mean there are not plenty of films despite this that have female characters I enjoy (Jurassic Park and Contact being just 2 on the left of the image below).
In terms of movies I want to discuss though, let’s start with the one on the right, Dr Elizabeth Shaw from Prometheus (2012). Those of you who read my Halloween blog on how the Alien movies reflect the world of Infection Prevention and Control, will already know how much I like this film series. One of the reasons the series appeals to me in general is that it doesn’t shy away from strong female lead characters, it started with Ripley after all. The female lone survivor trope is strong with this series, but I also like it when characters like Elizabeth are the ones that survive because they don’t shy away from their intellect and aren’t scared to be the smartest person in the room. Too often we hide away from owning our space as women, and I love a film where the characters are given license to own their space.
Talking about films where women are given permission to own their space, this next one is based on historical figures. My favourite female scientist movie of all time is hands down Hidden Figures, which came out in 2016. This film is loosely based on the non-fiction book by Margot Lee Shetterly and is about three female African-American mathematicians: Katherine Goble Johnson (Taraji P. Henson), Dorothy Vaughan (Octavia Spencer), and Mary Jackson (Janelle Monáe), who worked at NASA during the Space Race. If you haven’t seen this film I cannot recommend it enough. When I have bad weeks this film reminds me of the fights that others have fought just so I can occupy the space that I’m in, and the continued need to be that fight for the generation that will follow me. It’s about so much more than female representation, some of the challenges that these women faced due to the colour of their skin is mind blowing to someone growing up in the UK, not to say that there are not ongoing diversity and inclusion issues here. This film to me is everything that science representation on the big screen should be, and it’s just a pity that there aren’t as many examples as can be found on the small screen.
All hail Marvel
All this brings me to the one place that I feel consistently hits it out the park for me in terms of both female character representation and in showing scientists as real three dimensional people, Marvel (both Marvel Cinematic Universe and Marvel Studios). Personal opinion, but I feel like Marvel have done more for showing women who are scientists and characters in their own right than most other genre series, an irony I am aware of for a series based on comic book characters. This is probably made possible because they can draw on character development from so many decades of story lines in order to make it work.
My all time favourite is Dr Jemma Simmons from the Agents of SHIELD series, but that could be because you are able to get to know the character over 7 seasons. Film wise, I really love Dr Jane Foster from the Thor series. Previously my all time favourite film science character was Shuri from the first Black Panther series, I’m pretty conflicted about this now however due to some of the anti science opinions held by the actress.
There are frequently great scientific characters embedded across all parts of the Marvel universe ,however, and so I encourage you to find your own favourites. To help I’ve listed some of the big hitters, in terms of main characters, below.
Thor film series with Dr Jane Foster
Agents of S.H.I.E.L.D. TV series with Dr Jane Simmons
Ant-Man (and the Wasp) film series Dr Hope van Dyne (and Janet van Dyne)
Doctor Strange film series Ms Christine Palmer
Spider-Man film series (not actual scientists as too young to have careers but….) Mary Jane Watson
Black Panther film series Shuri
Captain Marvel film Dr Wendy Lawson
Eternals film, possibly all of the film characters as they are after all eternal
Another thing that I appreciate about the Marvel films is that even when a character is not present, due to them being part of another story stream, they often reference the absent character, and not just in a way that talks about their positioning linked just to a romantic other. One of my favourite examples of this is below, from Age of Ultron, and is part of a conversation about why Pepper Potts and Jane Foster are not at a party. The dialogue goes like this:
Avengers: Age of Ultron (2015)
If you are looking for something you can watch with your family, that will hopefully inspire the next generation of scientists, and help ensure that the next time a child is asked to draw a picture of one they may choose to draw a woman instead, this is a great place to start.
I feel we’ve come such a long way in terms of female scientific representation in the media, but there is so much more that needs to happen. We can all work to drive this by being aware of the films we choose to watch and where we decide to spend our money. Those of us working in science can also do a lot to make sure that we take opportunities presented to us that mean we will be seen, and hopefully inspire those who will follow us. Let’s embrace the moment, step out from the shadows, and truly show why having women in the scientific space is crucial for the best science to occur.
Thank you for taking some time out of your day to share International Women’s Day with me!
Norovirus is estimated to cause more than 21 million cases every year worldwide and to cost the NHS over £100 million every year. Because of its impacts, there’s been a fair amount in the news related to Norovirus recently as the numbers have been up this year. I thought the timing might be good, therefore, to talk about this clever and tricky virus, and why we should care about it even if it is not likely to result in significant harm to most people.
In their recent blog post the UK Health Security Agency (UKHSA) have listed a number of reasons why levels might be higher at the end of 2024 than in recent years:
Post-pandemic changes in population immunity
Changes in diagnostic testing capabilities
Changes in reporting to national surveillance
A true rise in norovirus transmission due to the emergence of GII.17
I’ve written a post before about food poisoning and food borne outbreaks, but as Noro (Norovirus) is the queen of this particular court, I thought it was high time I gave her the recognition she deserves and explain some of the reasons they’ve listed in more detail so that the reasons might become clearer.
What is Norovirus?
So, let’s start by talking some virology. Feel free to skip this section if the technical stuff doesn’t really appeal to you, I’ll try to include plenty of context in the other sections so they still make sense.
Norovirus is a single-stranded positive sense non-enveloped RNA virus, but what is that, and what does it mean?
RNA (ribonucleic acid) – We talk about DNA being the building blocks of life but viruses act a little different as they are able to take over the mechanics of the cell/host they invade. This means they dont have to have DNA to function. Their genomes (the code for what they are) can be made from RNA alone.
RNA molecules range widely in length and are often less stable than DNA. RNA carries information that can then be used to help cells build proteins using the machinery in the host, which are essential for replication and other steps
Single stranded – RNA is frequently single stranded, versus DNA, which is normally double stranded (there are however examples of single stranded DNA viruses, such as Parvovirus)
Positive sense – Noroviruses use their own genome as messenger RNA (mRNA). This means the virus can be directly translated (tell the cell what to do) into viral proteins by the host cell’s ribosomes (cell machinery) without an intermediate step
Non-enveloped – This refers to a virus that lacks the lipid bilayer that surrounds enveloped viruses, meaning that they are sometimes called ‘naked’. These viruses are more resistant to heat, dryness, extreme pH, harsh treatment conditions, detergents, and simple disinfectants than enveloped viruses.
Noro is part of the family Caliciviridae, and human Norovirus used to be commonly referred to as Norwalk virus. As genetic information has become more available, it is now known that there are 7 common genogroups or G types of norovirus (GI – GVII), only some of which can infect humans (GI, GII and GIV).
Representative virus strains and their known carbohydrate ligands are shown in orange. Data are adapted from PLoS ONE 2009, 4, e5058.
Within these main genogroups, GI and GII contain a number of different genotypes, which will circulate at different amounts across different years and cause most of the infection we see in the population. You can also probably see that, although we use numbers to talk circulating strains, they also commonly have names, often based on the city or area where they were found. This can make everything a bit confusing, so I’ll mainly just use numbers here. This year, as talked about by UKHSA, the primary culprit is a rise in GII.17.
Symptoms/presentation
Noro is interesting as it frequently presents as something known as ‘Gastric flu’. This means that initial symptoms are often linked to a headache and feeling generally unwell, potentially with a fever. So, not just the diarrhoea and vomiting that people often think of associated with this virus.
That said, you also get the perfectly well to sudden projectile vomiting type of presentation, which is what people think of. Norovirus is the reason I once sat at a train station and vomited on my own shoes, as it just came out of nowhere. There is often a very short, intense spike in temperature, and then it is upon you. This form of intense and sudden presentation is just one of the reasons for the transmissibility of this particular virus. The lack of warning means that it is almost impossible to get away from others, and you won’t have ‘taken to your bed’ before the acute symptoms start.
It is worth noting that as well as these differences in adult presentations, presentations in young children are often also different, with more diarrhoea rather than vomiting. This means that Noro in young children can slide under the radar until adults caring for them then start to feel unwell.
The incubation period is pretty short (a couple of days), and so transmission windows in close quarters can be pretty intense. The duration of illness in most people is also pretty short, although symptoms tend to come in waves, and so it can be difficult for individuals to predict in some cases when it will finally be over. All of this is true for your standard healthy immunocompetent adult, but it is worth remembering that in both children and immunosuppressed adults, presentations, severity of illness, and length of infectivity can be very different.
Diagnosis
Most diagnoses of Norovirus within the community are going to be based on symptoms and presentation, as in most cases, any management is going to be symptom relief by maintaining fluid balance, etc. More specific diagnostics therefore only tend to be undertaken within healthcare environments, where it is important to know viral details to help inform risk assessment linked to transmission, as well as to monitor recover and inform epidemiology (what strains are spreading and if any of them are cause more severe disease).
There are many possible ways to diagnose Norovirus in the lab, from routine diagnostics using molecular methods and immunoassays, to how people are looking to diagnose using Norovirus in areas like care homes in the future using smart phones and other novel methods.
Maja A. Zaczek-Moczydlowska, Azadeh Beizaei, Michael Dillon, Katrina Campbell. Current state-of-the-art diagnostics for Norovirus detection: Model approaches for point-of-care analysis. Trends in Food Science & Technology, Volume 114, 2021, Pages 684-695
In terms of immunoassays, there are a couple of commonly used tests. The first are lateral flow assays (LFA), which most of us will be familiar with in terms of the lateral flow assays used for SARS CoV2, and the principles are similar. Enzyme immunoassays (EIAs) follow similar principles but are usually undertaken in the lab with many samples being processed at the same time, allowing much more widespread testing to be undertaken.
Which diagnostic test is most appropriate depends on how frequent cases are. In outbreak or high prevalence settings, then EIA has sufficient sensitivity to detect most cases. If circulating levels are not very high, i.e. outside of the standard season or outbreaks, or in high risk settings where missing cases could have severe patient impacts, such as some healthcare settings, then most publications suggest molecular methods are the most appropriate way to test.
The molecular methods listed include isothermal amplification, with Loop-mediated isothermal amplification (LAMP) being a common method that was recognised during the pandemic for detecting SARS CoV2, and can be used outside of the traditional lab environment. I, in fact, validated a LAMP test for Noro when I was a trainee, so it’s been around for a while. The other listed is high throughput sequencing (HTS), which is a much more demanding technique requiring specialist skills and equipment, but also gains you all kinds of info, including that linked to strain and transmission data.
The most common molecular diagnostic test for Norovirus in high-risk settings is actually via polymerase chain reaction (PCR). This will usually target roughly a 130 base pair section of the Norovirus RNA genome out of the (on average) total 7500 base pairs of the virus, roughly 1.7% of the genome. This target area will usually enable differentiation between the common GI and GII species, which helps with monitoring and is chosen based on being present in all of those types in order to maximise sensitivity. Further differentiation into genogroups requires HTS but is often not needed outside of outbreaks and public health level epidemiology.
Norovirus is traditionally thought to be spread via what is known as the ‘faecal-oral’ route. That means that bits of poo and diarrhoea end up being swallowed by the person who then gets infected. This is because if someone has diarrhoea and goes to the bathroom, they will have up to 100,000,000 copies of the virus. This can then land in the area of the toilet, especially if the toilet seat isn’t closed on flushing, contaminating the surrounding area for anyone who goes into the bathroom and uses it afterwards. If someone then enters that bathroom and is susceptible to the virus, it is thought you then only need to swallow 10 – 100 copies of those 100,000,000 to become infected, and so only a very little is needed to spread the virus onward.
This isn’t the only route however. One of the issues with the acute vomiting phase of Noro is that someone vomiting can also vomit 30,000,000 copies of Noro. As the vomiting can be projectile, and come with a lot of force, this is ejected at high speed and can form what is known as an aerosol. This means the invisible vomit ‘cloud’ can hang around in the air for some time after the original vomit, meaning that anyone walking into the room where the vomit occurred for some time afterwards, or is present when it happens, can breath in the virus, and thus get infected that way.
As people can be infectious for some time after they’ve had acute infection (at least 48 hours) or when they have initial gastric virus symptoms before becoming acutely unwell, spread can commonly occur due to contamination of food products prepared by those infected. The common example is self catered events, such as weddings and birthday parties, where someone made a load of food on the morning and didn’t start to feel unwell until later in the day. 24 – 48 hours later a lot of the guests then suddenly start to feel unwell. This is a route via which lots of people can get sick from a single event and is known as a point source. Hand hygiene is always key, especially so when dealing with food, but the viral loading of people who are unwell with Norovirus means that avoiding being involved with food may be the only option, as there may just be too much virus present on hands etc to remove all of it easily.
The final route to consider is indirect spread. All of the circulating virus that’s in the air or in water droplets from the toilet flush, then will eventually come down and land on surfaces. Therefore those surfaces end up having a lot of virus upon them, and the virus, as non-enveloped, can survive on surfaces for some days. This means that then interacting with those surfaces can be a transmission risk, and so cleaning, and again hand hygiene, is really key to stopping ongoin spread.
Outbreaks
As those infected can be become unwell suddenly and spread lots of virus in a short period of time, Norovirus can be difficult to contain. Once an event occurs, all of the various transmission routes mean that Norovirus outbreaks can be difficult to control, and management is based upon rapid identification of cases and, if in hospital or even on a cruise ship, restricting contact to other people in order to reduce risk of spread.
The biggest issues occur in the kind of areas where lots of people get together, high densities of people in physically confined areas. Everywhere from military training camps to schools and nurseries can be affected. As mentioned before, centres where people may present in atypical ways due to age or underlying condition can also make it more complex to contain infections and prevent spread. Hospitals have high population densities with restricted space for movement, combined with patients that are high risk as they already have conditions that impact immune function or make them more vulnerable.
Outside of traditional health and residential areas, such as care homes, cruise ships are at high risk as passengers can feel fine when they get on board and then experience symptoms in a confined space, with little room to spread out.
Even once recovered from symptoms, some of the passengers are also likely to continue to shed the virus (one adult study suggested for 182 days) and therefore some of those who get sick early on and recover may continue to be a silent source and risk for other passengers if they don’t have good general hygiene practices.
It can also be a challenge to decontaminate some of the surfaces, as they are often predominated by soft furnishing where it can be difficult to use cleaning agents with sufficient activity as Noro can be resistant to disinfection and present in such high loads it can be hard to remove. This has led to the surfaces in cruise ships being a continued risk even when all of the original passengers have departed and a completed fresh set has boarded.
Seasonality
Norovirus outbreaks are seasonal, with the peak occurring in the winter months. This is partly because, as humans, we tend to spend more time indoors in close quarters with each other during the colder months. We get together for the festive season, and because the nights draw in earlier. This means that we tend to spend more time in higher density interactions than in the summer, where we might be out eating alfresco or going for evening walks, or in my case, cocktails. We also tend to travel to other households and cook for each other as part of the seasonal festivities, which means the food borne route definitely comes into play. Finally, as temperature and humidity impact on the indirect surface route, environmental conditions mean that the viruses survival on surfaces at this time of year is probably more prolonged. Norovirus never really goes away, but the number of cases definitely spikes during the winter.
Strain variance/immunity
The UKHSA mentioned that one of the reasons that there may be more Norovirus cases around now is because one of the current predominant strains is GII.17. The chart below is linked to circulating Norovirus in China, so not the UK, but you can see, even over a few years, how the levels of different circulating strains changes, and that within years there are normally a few strains that co-circulate with a predominate strain type.
Cao, R., Ma, X. & Pan, M. Molecular characteristics of norovirus in sporadic and outbreak cases of acute gastroenteritis and in sewage in Sichuan, China. Virol J 19, 180 (2022)
GII.17 is a less common strain and so many people will not have experienced it recently, if at all. If you haven’t had GII.17 before you won’t have immunity and therefore are susceptible to infection. Even if you have had GII.17 before, one of the reasons control of Norovirus is hard is that immunity is short lived. Even if you have experiences GII.17 before, therefore, the data shows that immunity lasts for anywhere from 6 months to 4 years, and therefore only relatively recent infection is protective. Finally, there is no cross strain immunity, so if there are three circulating strains of Norovirus in a season, unless you have experienced each of them in the relatively recent timeframe, it is possible to get multiple episodes, 1 from each strain, in a short period of time.
Prevention/Actions
Norovirus particles retain infectivity on surfaces and are resistant to a variety of disinfectants. This means that not only direct transmission routes (such as person to person) but indirect transmission via surfaces can be important. Interventions therefore need to take into account all of these different routes. Some common recommendations include:
Hand hygiene with soap and water (alcohol gel is less effective as Noro is a non-enveloped virus)
Staying away from other people until 48 hours after symptoms have ceased (as you often get a second wave of symptoms which increases risk of spread)
Avoid cooking or preparing meals for other people until at least 48 hours after symptoms have ceased, and ensure good hand hygiene when you re-commence
Cleaning with disinfectants (bleach etc at home) may be required, and multiple cleans may be needed due to the amount of virus present
Time cleaning so there is enough time for any virus in the air to settle on the surface, so a re-cleaning after 2 hours will probably be needed
Avoid going into a space where someone has vomited for 2 hours if possible to reduce the risk of inhaling virus
Ensure you are aware that Noro can present with gastric flu type symptoms, headache and temperature, before gastric symptoms start, and so be weary of seeing high risk individuals if you have any symptoms present (especially those in hospitals or immunocompromised)
Due to the challenges with short lived immunity and high viral loading, you won’t be able to avoid getting Norovirus into confined areas and high risk settings, so rapidly identifying when you have cases and making sure that your interventions enable you to stop secondary spread is key. If you get sick, stay home, ensure you keep hydrated, and don’t let the virus fool you into thinking it’s done when you are feeling that little bit better on day 2, it’s Noro’s way of tricking you into going back out into the world an spreading it further. The queen of the gastric viruses is super clever and so we need to be even smarter to prevent her spread.
I’m back from a lovely week away at Disneyland Paris, celebrating Christmas and escaping reality (a post on Disney and denial as a coping mechanism is on its way). Whilst I am still struggling with the return to reality this weeks blog post is supplied by the wonderful Callum Barnes. Callum is a disciple of the biomedical sciences, current master’s student creating a more authentic lab experience for those after me, aspiring consultant microbiologist (the best discipline, sorry Claire – you see he understands, like me, that micro will always trump immunology).
Callum is supervised by Dr Claire Walker who is a paid up member of the Dream Team since 2013, token immunologist and occasional defector from the Immunology Mafia. Registered Clinical Scientist in Immunology with a background in genetics (PhD), microbiology and immunology (MSc), biological sciences (mBiolSci), education (PgCert) and indecisiveness (everything else). Now a Senior Lecturer in Immunology at University of Lincoln. She has previously written many great guest blogs for The Girlymicrobiologist, including one on turning criticism into a catalyst for change.
Two years ago, I began a placement year in the microbiology department of a pathology lab, unsure of what was to come, and unsure of myself and my skillset as a scientist. As I think every scientist feels at some point, I was mostly concerned that I would be a hinderance to all the wonderful staff that were just trying to get on with their jobs. Everyone was amazing though and helped me develop the skills and confidence I needed to successfully complete my IBMS portfolio verification. Returning back to university for my final year, I found the lab-based work so much easier than in my second year with my experience, but… something was different. This wasn’t the same stuff I just spent the last year working on, where was the LIMS? The booking in of the samples, the investigative process and the, frankly, the occasional chaos were missing. That’s not to say the labs weren’t good – they were great – and the staff that developed and ran them miles better, but something felt like it was missing. And that’s when my now supervisor Dr Claire Walker came to me with a project for my Mbio year.
Claire and I both have experience in the NHS, herself a lot more than me, but we have both felt and experienced the environment that a pathology lab has. It has a very unique feel to it, slightly alive in my opinion. This is not a very common experience to have in academia though as most academics have a research background, which means that the practical pathology side of things can sometimes get lost when students do their practical work. As such, Claire and I have been working on creating a lab experience that is as authentic to an NHS pathology lab as possible.
But why even bother? The students are learning the same things, just in a different way, so does it really matter? Well in fact, yes, it does! As Claire has said previously, the pilot study she did had very good results, so the data is there to back up our work. But imagine for just a second that you are looking at applying for medicine, and you have two offers. One university offers a fully simulated experience using manikins and actors – the whole shebang. And the other university teaches mostly through theory and shadowing – no practical experience is offered. I know which course I would enjoy and learn the most from. Medical schools know this too and is why most of them offer simulated teaching – it makes for better doctors too.
So, we should really ask, why isn’t this offered for biomedical scientists? Maybe it’s cost, maybe there isn’t the associated prestige. Whatever it is, I am sure that our work will guarantee a truly authentic clinical laboratory experience here on the iBMS accredited course at the University of Lincoln – something I know will provide the right skills for the pathologists of tomorrow.
It’s the Easter weekend and I haven’t posted a book review in forever, so I thought I would post a review of something that not only I think all scientists should read, as a tale of when science goes wrong, but also because it’s been dramatised and so you could also spend some of your weekend enjoying it in multiple media forms.
I didn’t really know much about the Theranos company before I read this book. I had seen a couple of news articles and video clips of Elizabeth Holmes, but I don’t think it made quite the same coverage in the UK as in the states. I do remember a video of her talking about being able to do several hundred tests from a drop of blood and rolling my eyes and being dismissive as it struck me as scientific nonsense. I didn’t realise this was a system that had been rolled out for actual patient testing and as the basis for clinical decision-making, which to me is incomprehensible. I’m getting ahead of myself however, here is what the book is about.
Bad blood is written by the journalist John Carreyrou, who broke the story at the Wall Street Journal. It is a chronological re-telling of the rise and eventual fall of the Theranos company and its founder, Elizabeth Holmes. It is based on interviews and fact finding that were collected for the articles and runs up until the start of criminal prosecutions.
Elizabeth Holmes is a self-proclaimed Stanford dropout who left university to pursue a bio tech start-up. She claimed to be terrified of needles, so established a company that would enable the avoidance of venopuncture blood draws by using point of care testing using a finger prick to provide the same level of diagnostic information. The end vision sold to investors was that this could all be done by a small microwave sized machine that could, eventually, be sold for home use as a form of self monitoring. The platform was rolled out into patient use at Walgreens chemists, as the first step in a national roll out. Testing patient samples and providing clinical results in Phoenix, Arizona. Interestingly, to me, as this was a private biotech company, there appears to have been little to no oversight of this diagnostic roll out, despite producing a medical device.
The book covers how investment was attracted and rapid growth attained because of the strength of this vision and the charisma of the woman selling it. It also covers how, despite scientists not being able to deliver this vision, it continued to be sold and how the very negative company culture allowed this to happen. All company employees were made to sign non-disclosure agreements, they were prevented from talking outside their teams, their emails were monitored, and threats of legal action appear to have been common. This meant that many of those working on development were unaware of the significant flaws with what was being sold, and those that were and considered or tried to whistle blow were taken down legal routes, where Theranos had considerable more financial capability to attain a positive outcome.
This was all compounded by a lack of oversight and, as there were no regulatory affairs staff employed, allowed governance processes to be manipulated. The company had two laboratories, one to develop their new technology known as Normandy, and one which was disclosed and Clinical Laboratory Improvement Amendments (CLIA) accredited which containing more standard technology platforms known as Jurassic Park.
Eventually, after the death by suicide of one of the employees and increasing press coverage seen by external scientists who questioned how this was possible, as well as clinical alarm bells, enough momentum was gained to put together a story that shone the light on why this approach was disastrous for the patients who were relying on it.
The story is already available in many different forms, including a TV series that is currently available BBC iPlayer and Disney+
Listening to the audio book of this book whilst I write this blog post it makes me think that are a lot of points that shock me as a English scientist working in such a highly regulated environment, both for NHS services but also for me as a state registered individual. It has also made me reflect on how crucial support for escalation and whistle blowing is to ensure that scenarios also get flagged when those services are not providing the quality of service required. I’ve briefly outlined some of my reflections below:
Governance
I spend a lot of time in governance meetings, both local and national. I even sit on a number of grant, research and ethics panels. I don’t think I’ve ever encountered the kind of lack of governance and accountability described in this book. That said, I’ve never worked in private industry or a start up. Just going through this book has made me have a new recognition for how important it is that boards and other oversight structures, ask the difficult questions and undertake constructive challenge in order to identify problems early and reduce risk.
Responding to No
At every stage in this re-telling smart people tried to raise concerns. When concerns were raised those people raising them were either isolated or asked to leave. Those who played the game and did not rock the boat were promoted, ending up in a scenario where the entire of the senior leadership were either the ones who didn’t want to hear or were people that didn’t want to challenge. In other words Elizabeth deliberately surrounded herself with yes men and thus created her own echo chamber. You can see, to an extent, how this can happen in other settings and where unacknowledged risk could therefore be introduced, and so ensuring that challenge is encouraged and not victimised is key to success.
Female leadership
Being a female leader is challenging, being a female leader in the technology and science sectors is both challenging and unusual. I can’t help thinking when reading this book how much of a back lash will occur and impact other female innovators. Elizabeth was heralded as unique and special for being a female in this area, I feel it’s likely that her actions have significantly set back other women in this space trying to make room for themselves. In addition to the patient harm caused, this is one of the things that upsets me the most.
Authentic leadership
To succeed, Elizabeth crafted a new image of herself. She changed the way she dressed to look more like Steve Jobs, whom she admired. She even changed her voice to use a lower octave, as she felt it made her more unique, memorable and aided success. I’m rather struck by the fact that she changed the way she dressed to look and even sound more like her male compatriots. If she changed these external factors, I can’t help but think what else she changed, and how much she went against all the principles of authentic leadership. She shared little of the real her, and I wonder how much that facade enabled her to distance herself from the reality of what she was doing. For me, it’s a reminder of why authentic leadership is so important, to put yourself out there and also to be held to account, rather than introducing a facade which distances you from your actions.
Quality assurance
Quality assurance, ensuring you get the right result on the right patient in the right time frame, seems to have features little if at all in the Theranos story. They utilised out of date reagents, the way they undertook validation testing is like nothing I’ve ever encountered, and they topped it off by actually lying about how and where results were produced. It’s easy to think that we would never act in the same way, and I doubt any of us would to the same extent, but there are aspects of laboratory life which I think would be open to monitoring challenges. The expansion and use of home testing, and even point of care testing (POCT) presents a lot of quality control and assurance challenges. These tests are conducted outside of standard laboratory settings, often by individuals with less knowledge about the processes. How do we increase access whilst maintaining quality in these circumstances? I think it’s something many of us are wrestling with.
Research and innovation
Innovation has risk associated with it, research wouldn’t be research if there were not unknowns. The patient impacts of this work however have given me a chance to reflect on how import ethics and governance reviews are to controlling these risks. As the testing was not rolled out during a trial, there was no consenting of patients to those risks. The people who ran the institutions in which they were rolled out were also not informed that they were effectively partaking in a research experiment. This means that all those involved are less likely to engage in research based processes in the future, as trust has been broken, even if it were to happen with different more established individuals. Thus the behaviour of a few impacts us all, and therefore as scientists we have a responsibility to flag this bad behaviour as and when we see it.
Listening to the scientist in the room
The scientists in the room were not heard. The company was led by people who lacked technical skill. Rather than understanding their limitations, they actively denied any lack of knowledge. They therefore didn’t listen when those best placed tried to flag issues. There was also no route for whistle blowing, either to the board, or to external organisations, partly due to the NDAs and threats of litigation. As a leader, this has made me reflect on both how important it is to listen to those skilled individuals you have working for you, but also how much there needs to be processes in place that bypass me in the case of a need for escalation. No one is perfect, and it is so important that concerns are heard and acted upon.
Silos limit productivity and communication
One reason that Theranos not only manage to hide its failings, but also probably failed in the first place, was that everyone was kept in silos and isolated from each other. There were no multi-disciplinary collaborations, sharing was actively forbidden, and there were no cross department routes of communication. Everything was linear, up and down. This can easily be seen as a failing in other large institutions, not because of an active plan, but because we don’t encourage enough cross organisational working. Collaboration is key to innovation, trouble shooting, but also to fault finding and improvement. It takes effort to do well, but is worth investing the time and energy into for improved results.
Vision alone is not enough
Vision without follow through is always going to fail. Vision without working pragmatically on turning it into reality will not succeed. Once you move from vision into implementation or delivery, it cannot be enough that you alone own the vision. It has to be shared, it can no longer be owned by an individual. By sharing it, you also have to take onboard the input of those others, and if you cling to the original too tightly then you are setting it up to be a disappointment.
People are the ones who suffer
People were actively hurt by this poor use of science and innovation. The scientists themselves suffered when they tried to raise the alarm, emotionally and through litigation. Most of all though, the patients who placed their faith in a diagnostic that could never deliver suffered, either through over or under treatment. Because this tale occurred in the states, those failings also came with a financial burden, as well as a physical one. This book makes me so grateful for the NHS and our regulatory structure for the governance and protection it provides. Nothing is perfect, but an imperfect something is so so much better than the alternatives. I hope you find the book as eye opening as I did.
I adore Christmas, it’s one of my favourite times of the year. I meant to get this one out before Christmas, but to be honest, I was too busy having family time. For those of us working or looking for some fun reading between Christmas and New Year I thought this one might still be of interest.
Every year the British Medical Journal have a wonderful tradition. They post some free to access journal article. Now, these aren’t just any journal articles. They apply serious scientific processes to brilliant topics, such as the disappearance rates hard vs soft centred chocolates in ward environments presented as an observational study.
These articles always bring a smile to my face, and if you’re looking at an entertaining way to learn more about scientific processes or scientific writing these are a great place to start. I hope you’ll feel the same when you have a read of some of the ones linked to below, and know that there are more out there if you want to journey down this particular rabbit hole.
Merry Christmas, and thank you so much for spending another year in the company of the Girlymicro blog!
Objectives To determine the overall rate of loss of workplace teaspoons and whether attrition and displacement are correlated with the relative value of the teaspoons or type of tearoom. Design Longitudinal cohort study. Setting Research institute employing about 140 people. Subjects 70 discreetly numbered teaspoons placed in tearooms around the institute and observed weekly over five months. Main outcome measures Incidence of teaspoon loss per 100 teaspoon years and teaspoon half life.
Results 56 (80%) of the 70 teaspoons disappeared during the study. The half life of the teaspoons was 81 days. The half life of teaspoons in communal tearooms (42 days) was significantly shorter than for those in rooms associated with particular research groups (77 days). The rate of loss was not influenced by the teaspoons’ value. The incidence of teaspoon loss over the period of observation was 360.62 per 100 teaspoon years. At this rate, an estimated 250 teaspoons would need to be purchased annually to maintain a practical institute-wide population of 70 teaspoons.
Conclusions The loss of workplace teaspoons was rapid, showing that their availability, and hence office culture in general, is constantly threatened.
Objective To investigate whether sleep deprived people are perceived as less healthy, less attractive, and more tired than after a normal night’s sleep. Design Experimental study. Setting Sleep laboratory in Stockholm, Sweden. Participants 23 healthy, sleep deprived adults (age 18-31) who were photographed and 65 untrained observers (age 18-61) who rated the photographs. Intervention Participants were photographed after a normal night’s sleep (eight hours) and after sleep deprivation (31 hours of wakefulness after a night of reduced sleep). The photographs were presented in a randomised order and rated by untrained observers. Main outcome measure Difference in observer ratings of perceived health, attractiveness, and tiredness between sleep deprived and well rested participants using a visual analogue scale (100 mm).
Results Sleep deprived people were rated as less healthy (visual analogue scale scores, mean 63 (SE 2) v 68 (SE 2), P<0.001), more tired (53 (SE 3) v 44 (SE 3), P<0.001), and less attractive (38 (SE 2) v 40 (SE 2), P<0.001) than after a normal night’s sleep. The decrease in rated health was associated with ratings of increased tiredness and decreased attractiveness.
Conclusion Our findings show that sleep deprived people appear less healthy, less attractive, and more tired compared with when they are well rested. This suggests that humans are sensitive to sleep related facial cues, with potential implications for social and clinical judgments and behaviour. Studies are warranted for understanding how these effects may affect clinical decision making and can add knowledge with direct implications in a medical context.
Objective To quantify the consumption of chocolates in a hospital ward environment. Design Multicentre, prospective, covert observational study. Setting Four wards at three hospitals (where the authors worked) within the United Kingdom. Participants Boxes of Quality Street (Nestlé) and Roses (Cadbury) on the ward and anyone eating these chocolates. Intervention Observers covertly placed two 350 g boxes of Quality Street and Roses chocolates on each ward (eight boxes were used in the study containing a total of 258 individual chocolates). These boxes were kept under continuous covert surveillance, with the time recorded when each chocolate was eaten. Main outcome measure Median survival time of a chocolate.
Results 191 out of 258 (74%) chocolates were observed being eaten. The mean total observation period was 254 minutes (95% confidence interval 179 to 329). The median survival time of a chocolate was 51 minutes (39 to 63). The model of chocolate consumption was non-linear, with an initial rapid rate of consumption that slowed with time. An exponential decay model best fitted these findings (model R2=0.844, P<0.001), with a survival half life (time taken for 50% of the chocolates to be eaten) of 99 minutes. The mean time taken to open a box of chocolates from first appearance on the ward was 12 minutes (95% confidence interval 0 to 24). Quality Street chocolates survived longer than Roses chocolates (hazard ratio for survival of Roses v Quality Street 0.70, 95% confidence interval 0.53 to 0.93, P=0.014). The highest percentages of chocolates were consumed by healthcare assistants (28%) and nurses (28%), followed by doctors (15%).
Conclusions From our observational study, chocolate survival in a hospital ward was relatively short, and was modelled well by an exponential decay model. Roses chocolates were preferentially consumed to Quality Street chocolates in a ward setting. Chocolates were consumed primarily by healthcare assistants and nurses, followed by doctors. Further practical studies are needed.
Objective To detect and localise the Christmas spirit in the human brain. Design Single blinded, cross cultural group study with functional magnetic resonance imaging (fMRI). Setting Functional imaging unit and department of clinical physiology, nuclear medicine and PET in Denmark. Participants 10 healthy people from the Copenhagen area who routinely celebrate Christmas and 10 healthy people living in the same area who have no Christmas traditions. Main outcome measures Brain activation unique to the group with Christmas traditions during visual stimulation with images with a Christmas theme.
Methods Functional brain scans optimised for detection of the blood oxygen level dependent (BOLD) response were performed while participants viewed a series of images with Christmas themes interleaved with neutral images having similar characteristics but containing nothing that symbolises Christmas. After scanning, participants answered a questionnaire about their Christmas traditions and the associations they have with Christmas. Brain activation maps from scanning were analysed for Christmas related activation in the “Christmas” and “non-Christmas” groups individually. Subsequently, differences between the two groups were calculated to determine Christmas specific brain activation.
Results Significant clusters of increased BOLD activation in the sensory motor cortex, the premotor and primary motor cortex, and the parietal lobule (inferior and superior) were found in scans of people who celebrate Christmas with positive associations compared with scans in a group having no Christmas traditions and neutral associations. These cerebral areas have been associated with spirituality, somatic senses, and recognition of facial emotion among many other functions.
Conclusions There is a “Christmas spirit network” in the human brain comprising several cortical areas. This network had a significantly higher activation in a people who celebrate Christmas with positive associations as opposed to a people who have no Christmas traditions and neutral associations. Further research is necessary to understand this and other potential holiday circuits in the brain. Although merry and intriguing, these findings should be interpreted with caution.
Objective To determine whether artificial intelligence (AI) can generate plausible and engaging titles for potential Christmas research articles in The BMJ. Design Observational study. Setting Europe, Australia, and Africa. Participants 1 AI technology (Generative Pre-trained Transformer 3, GPT-3) and 25 humans. Main outcome measures Plausibility, attractiveness, enjoyability, and educational value of titles for potential Christmas research articles in The BMJ generated by GPT-3 compared with historical controls.
Results AI generated titles were rated at least as enjoyable (159/250 responses (64%) v 346/500 responses (69%); odds ratio 0.9, 95% confidence interval 0.7 to 1.2) and attractive (176/250 (70%) v 342/500 (68%); 1.1, 0.8 to 1.4) as real control titles, although the real titles were rated as more plausible (182/250 (73%) v 238/500 (48%); 3.1, 2.3 to 4.1). The AI generated titles overall were rated as having less scientific or educational merit than the real controls (146/250 (58%) v 193/500 (39%); 2.0, 1.5 to 2.6); this difference, however, became non-significant when humans curated the AI output (146/250 (58%) v 123/250 (49%); 1.3, 1.0 to 1.8). Of the AI generated titles, the most plausible was “The association between belief in conspiracy theories and the willingness to receive vaccinations,” and the highest rated was “The effects of free gourmet coffee on emergency department waiting times: an observational study.”
Conclusions AI can generate plausible, entertaining, and scientifically interesting titles for potential Christmas research articles in The BMJ; as in other areas of medicine, performance was enhanced by human intervention.
Objective To examine the effect of a (fictional) doctor working during the festive period on population health. Design Natural experiment. Setting England, Wales, and the UK.
Main outcome measures Age standardised annual mortality rates in England, Wales, and the UK from 1963, when the BBC first broadcast Doctor Who, a fictional programme with a character called the Doctor who fights villains and intervenes to save others while travelling through space and time. Mortality rates were modelled in a time series analysis accounting for non-linear trends over time, and associations were estimated in relation to a new Doctor Who episode broadcast during the previous festive period, 24 December to 1 January. An interrupted time series analysis modelled the shift in mortality rates from 2005, when festive episodes of Doctor Who could be classed as a yearly Christmas intervention.
Results 31 festive periods from 1963 have featured a new Doctor Who episode, including 14 broadcast on Christmas Day. In time series analyses, an association was found between broadcasts during the festive period and subsequent lower annual mortality rates. In particular, episodes shown on Christmas Day were associated with 0.60 fewer deaths per 1000 person years (95% confidence interval 0.21 to 0.99; P=0.003) in England and Wales and 0.40 fewer deaths per 1000 person years (0.08 to 0.73; P=0.02) in the UK. The interrupted time series analysis showed a strong shift (reduction) in mortality rates from 2005 onwards in association with the Doctor Who Christmas intervention, with a mean 0.73 fewer deaths per 1000 person years (0.21 to 1.26; P=0.01) in England and Wales and a mean 0.62 fewer deaths per 1000 person years (0.16 to 1.09; P=0.01) in the UK.
Conclusions A new Doctor Who episode shown every festive period, especially on Christmas Day, was associated with reduced mortality rates in England, Wales, and the UK, suggesting that a doctor working over the festive period could lower mortality rates. This finding reinforces why healthcare provision should not be taken for granted and may prompt the BBC and Disney+ to televise new episodes of Doctor Who every festive period, ideally on Christmas Day.
Objectives To identify Barbie brand dolls that had medicine and science themed professions in comparison with other career dolls and to determine their accuracy in meeting clinical and laboratory safety standards. Design Descriptive quantitative study. Setting Visual and data analysis of web searches.
Main outcome measures To identify the kinds of medical and scientific subspecialties that the Barbie dolls (and a comparison doll group) worked in; and to determine whether these medical professional and scientist dolls met laboratory and clinical safety standards. Additional data about doll demographics (ie, age, ethnic group, and sex) were also collected.
Participants 92 Barbie brand dolls were analyzed: doctor (n=53), scientist (n=10), science educator (n=2), nurse (n=15), dentist (n=11), and paramedic (n=1). 65 non-Barbie brand dolls were also analyzed for comparison purposes: doctor (n=26), scientist (n=27), nurse (n=7), dentist (n=2), engineer (n=2), and magnetic resonance imaging (MRI) technician (n=1) dolls.
Results Barbie brand medical professional dolls (n=80) largely treated children (66%, n=53/80), with only three (4%) medical professional dolls being directly depicted working with adults. Of the 12 scientist Barbie brand dolls, none met all proper personal protective equipment requirements related to hair and clothing. Barbie brand dolls often came with items, such as laboratory coats, microscopes, stethoscopes, and glasses, that children stereotypically associate with doctors and scientists. While comparison dolls offered a wider range of age and ethnic groups than the Barbie doll group did, the dolls similarly struggled to portray a wide range of medical and scientific subfields and most comparison dolls did not wear proper personal protective equipment.
Conclusions Medicine and science themed dolls help to inspire tomorrow’s medical professionals and scientists. All toy companies should ensure that future medical professional and scientist dolls meet clinical and laboratory safety standards and diversify the types of medical and scientific professions represented (especially among male dominated fields). For young girls’ sakes as much as her own, Barbie must keep shattering glass ceilings.