You may have noticed that I’ve been a little poor at keeping up with the Girlymicrobiologist site admin, and missing the odd weekly blog post. This isn’t because I’ve been slacking, honest, it’s more because I may have become a little distracted by a new project. I promise to get back on top of things soon, but in the meantime I thought I owed you an update.
Many of you have been kind enough to support last years project, which was a book aimed at supporting people to engage with research and research degrees, and I couldn’t be more grateful for your cheer leading. This new project, however, in the words of Monty Python could be described as ‘and now for something completely different’. It couldn’t be further from a book about academic study. This one is all about something else I love passionately, movies and TV.
I finished and launched the last book last October, and to be honest it hadn’t occurred to me, prior to letting it go into the wild, that I would write anything else till my retirement – when I’m planning to write some pathology based murder mysteries. It was never the plan to do something again, at least so soon. Frankly though, my brain tends to disrupt all my best laid plans, and ideas come meaning I just can’t help myself but get swept up. I’m blaming Ian McKellen inspiring me to ‘practice any art’.
Despite having no plans to do more, I have to say that I really enjoyed writing the first book, and I found the process of being able to write in a different way very fulfilling. I love writing this blog, and the first book is based on a lot of the pieces I have written for here, but it was nice to see them come together and take on a new and different life of their own. I also enjoyed mixing up the writing of something on a single theme with writing blogs on different topics for here, although I did rely a lot on Dr Claire Walker bringing together many guest blogs to allow me some writing time. It was lovely to see what those guest blogs brought to the site, and I really enjoyed seeing how including those voices really makes this feel even more like a community space. Without realising it, I think I caught ‘the bug’. Now, I’ve always enjoyed writing, this is my happy space, but I had never seen myself as an author, having held a book I’d written in my hands though, I can see how it could become a little addictive.
As I was sitting watching horror movies as part of my post release recovery, and researching for my 2025 Halloween post, I suddenly realised what I’d like to do next. I really wanted to write about some duel loves of mine, movies and TV plus infection.
Without any expectation of writing another book, all of a sudden I had a structure in my mind, and Don’t Open That Door had began…
You all know how much I am a movie and TV buff, everything from guilty pleasure reality TV, like The Secret Lives of Mormon Wives, to documentaries, and all genre of film (with the exception of torture porn horror movies, I’m a Blumhouse girlie). Whilst enjoying some down time with Mr Girlymicro, I realised how widely infection is featured in all kinds of different genera settings, some of it was actually pretty good, whilst some of it was really poor. So the first step was to do a whole bunch of research about what kind of examples were out there, by hitting up a bunch of different lists that have been collated by others, internet searches, and sourcing opinions from my movie loving friends. All of which led to the creation of a list of 138 options that needed a review to see if if they were actually linked to infection, and if they were infection based….was the infection content any good.
If you follow me (Girlymicro) on Instagram, you will have probably seen a number of stories that I’ve posted recently linked to movies I’ve been watching with some Infection Prevention and Control/micro commentary:
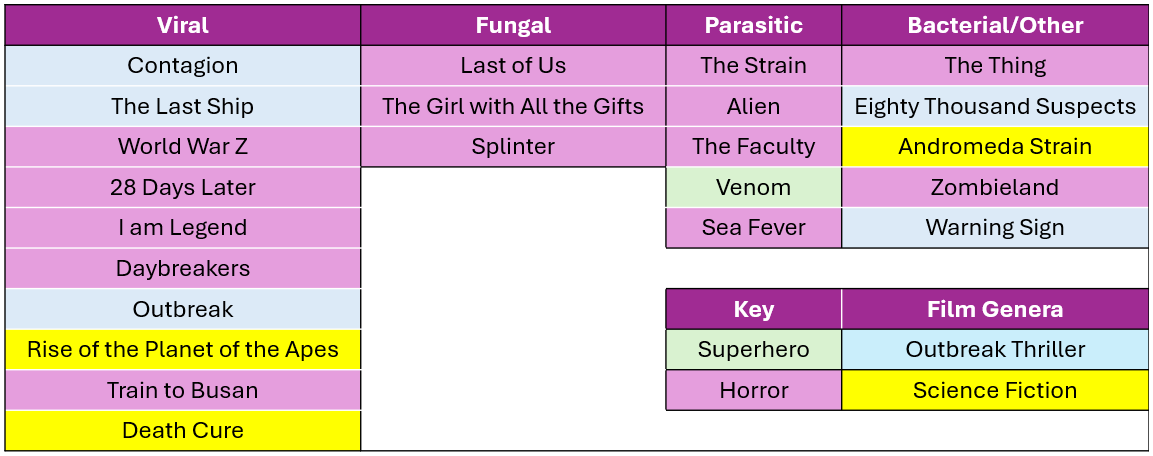
These have come about whilst I’ve been watching the 138 films/series with Mr Girlymicro to decide which ones make the cut to be included. I’ve watched some awesome films, some like Sinners, weren’t based on infection so couldn’t be included. I have also watched some truly bad movies, I even gave Resident Evil another go, and have spared you all by making sure that it is not included on the list. One of the considerations was that, even if the science wasn’t dreadful, I haven’t included anything that I or Rotten Tomatoes include as being truly horrible. I’m not just saving you on this, but also myself, as I’m having to watch included examples many times as part of the writing. I also felt it was really important to cover infections linked to viral, fungal, parasitic, and bacterial causes, just because they behave so differently and the interventions needed are so different. So the final list for inclusion involves movies and TV series that sit across infectious agents, although viruses are more represented than any other cause.
There are plenty of horror movies on the list, purely because they represent A LOT of the infection genera, but I was surprised at how many options there were outside of horror movies. I also tried to mix up certifications where I could, so that there are some options that everyone might enjoy.
Not everything could be included however, and there were also some exclusion criteria that impacted what I could include. Exclusion criteria included factors such as availability – no point including things that people can’t access, language options – I sadly only speak English so it needed at least English subtitles, and most importantly not based on real life events – this is about fiction.
For inclusion examples also needed to have infection as a central theme. This meant that health dramas could not be included as they only feature infection in some episodes, but at some point I do really want to write something that compares different medical dramas (House, New Amsterdam, Holby City etc) and maybe do a ranking scale….let me know if you think that would be a fun blog post.
Image credit The Red Dress
The reason it felt timely to talk about this today, is that the Biomedical Scientist magazine has been kind enough to do a whole feature on what the new book will look like, with a bit more detail, and some examples of what chapters will look like. It dropped on the 27th March and you can check it out the link here: https://thebiomedicalscientist.net/2026/03/24/infections-films. Also, how awesome is the art work they’ve done, can’t say enough how awesome The Red Dress are.
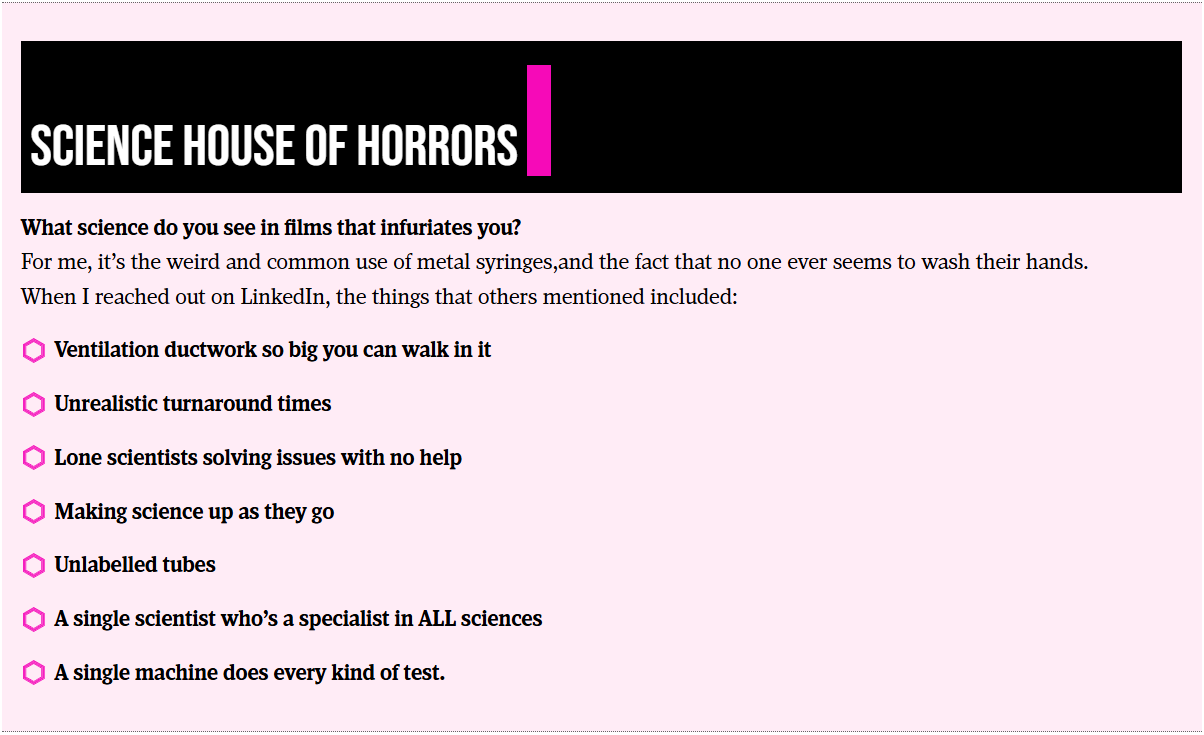
Whilst writing the article for the Biomedical Scientist and watching the example movies, I couldn’t happen but note how many weird and wonderful things are included as part of the science representation. Things that in my scientific career I rarely if ever encounter, but seem to crop up time and time again in Hollywood depictions of scientific life. I’m collating these for one of the final chapters in the book called ‘Science House of Horrors’ as I find them a bit fascinating. I’ve included some of the ones in the Biomedical Scientist article that I noticed, as well as those sent through as responses from social media, but I’d love to know if you have any others that I should include.
There are other opportunities to get involved though, I have 23 films and series examples, but there is room in the book to cover 25. I’m really keen to get other examples that include fungi, but if there is just something brilliant I haven’t included please let me know. There will also be a chapter called ‘Hall of Fame’ that covers both amazing movies that just don’t have enough infection in them to be included, or ones that were great but not quite as good an example of an infection characteristic as the ones already included. There is also the ‘Hall of Shame’ for examples, such as the TV series The Rain and Resident Evil, where the science is so bad that it is note worthy in itself.
Anyone who drops me an email to elaine@girlymicrobiologist.com and inputs into the House of Horrors, volunteers film examples I’ve missed, or suggests contenders for the ‘Hall of Fame’ or ‘Hall of Shame’, will get their name included in the list of contributors at the back of the book. Science takes a village, so does pulling together a book, and I’m really keen that this feels like it comes from our community. I hope you enjoy the article and I can’t wait to hear from you about your suggestions.
I am so excited by todays’ guest blog post. I’ve been so eagerly awaiting sharing it with you all. I don’t have any tattoos myself but it is something that is common amongst my friendship group, and I get asked about tattoo related infections A LOT. Partly as I was involved in some of the investigations when there was an issue some time back. So, a post that could help address some of the risk assessment and best practices linked to this art form felt very necessary, even though I didn’t feel I was best placed to write one. Then I saw this great article from Julie Russell on LinkedIn and I just had to reach out and see if she fancies writing a guest blog for me, and thankfully she said yes!
I first met Julie as Head of Culture Collection at Public Health England, that has since changed it’s name to the UK Health Security Agency. She was an inspiring microbiologist, who just had so much knowledge, and she became a great phone a friend. Since then she has moved on to work in a really different area where she still gets to put her microbiology and infection prevention and control knowledge to good use, as the director of a tattoo/art studio in Muswell Hill. No one is better placed therefore to answer the questions that I always get asked and have not felt best placed to answer.
Blog post from Julie Russell
After years in NHS microbiology laboratories, I joined the Public Health Laboratory Service, where I provided external quality assessment schemes and reference materials to laboratories worldwide. After that, I decided to do something completely different. I now co-own and manage Old Marine Arts Group, a tattoo studio in Muswell Hill, London.
It hadn’t occurred to me that tattooing, one of the oldest art forms in the world, essentially creates controlled wounds on people to decorate their bodies. I’ve had tattoos since my 20s – my first done in a legalised squat by a friend who’d never tattooed anyone in his life before. There was no personal protective equipment (PPE) involved; it healed beautifully, and I didn’t think about it anymore.
Many thousands of people across the UK have similar stories with no ill effects. Yet infections linked to tattooing have been recognised since the 19th century, and the government quite reasonably seeks to minimise such risks.
Tattooing, Skin, and Infection Risk
Bear in mind that the skin has a rich, diverse microbiome consisting of millions of microorganisms, some of which can cause infections if the skin is broken. Tattooing involves puncturing the skin with needles thousands of times, to a depth of approximately 1.5-2 mm, to place pigment into the dermis, creating a permanent design. Invariably, the tattoo process causes some bleeding, and after it’s finished, short-term redness, swelling and scabbing are normal. Resisting the urge to scratch is essential to minimise the risk of infection.
A July 2024 YouGov1 poll suggests 28% of UK adults – around 15 million people – now have tattoos. The UK Health Security Agency (UKHSA) notes that the true prevalence of tattoo-associated infections is unknown. There are no statutory notification procedures in place for infections specifically caused by tattooing, and no indication that such infections significantly burden the NHS. Various estimates suggest that approximately 1-3% of tattoos become infected in the UK. Most infections are mild local skin infections that can be treated with a single course of antibiotics; severe infections remain rare.
Interpreting the Evidence
Publications on tattoo-related infections must be read with caution. A December 2024 paper in The Lancet Microbe2, “Microbiology of tattoo-associated infections since 1820”, highlights rare severe cases such as necrotising fasciitis, leprosy and atypical mycobacteria outbreaks. The authors state that, “Despite advancements in public health policies and increased awareness of tattoo-related risks, a notable rise in both the number and diversity of microbial infections has been observed with an increase in the population opting for tattoos, particularly since 2000”. However, they provide no population-level denominators and conflate expected irritation, redness and swelling with true microbial infections. The authors fail to note that severe cases are overrepresented in the literature precisely because they are unusual. The paper may be a useful clinical catalogue, but it is not an incidence study.
A Brief History of Safety
Tattooists and clinicians have long recognised infection risks in tattooing. In the late 1800s, some artists infamously spat into powdered ink and sucked the needles during the tattooing process. Meanwhile, London-based artists in the early 1900s, such as Alfred South, promoted “the most perfect antiseptic treatment, painless and absolutely harmless”, whilst Tom Riley warned: “Caution to Ladies and Gentlemen thinking of being tattooed – First see the work of two or three tattooists then make choice {sic}. See that a complete set of new needles are {sic} used at each sitting as well as antiseptics”. Some early tattooists even wore white coats to convey a clinical level of cleanliness.
Legal regulation, however, arrived much later. It was still legal to tattoo children in the UK until the Tattooing of Minors Act 1969. Some aristocratic families reportedly tattooed babies for identification – in case, for example, their children were hospitalised or kidnapped.
Modern Regulation
Mandatory licensing changed the landscape. Under the Local Government (Miscellaneous Provisions) Act 1982, tattoo studios need to be registered. More recently, there is the British Standard BS EN 17169:2020, which covers safe and hygienic practice, although not many councils use it as a benchmark. This standard covers workplace preparation, equipment sterilisation, PPE, client consultation and aftercare. It requires studio owners to implement a comprehensive hygiene protocol to protect clients and staff, and tattoo artists to provide evidence of continued professional development.
Wales now requires tattooists to complete and pass a regulated Level 2 Infection Prevention and Control Award. Requirements in England and Scotland are less specific. Barnet Council licenses my studio; their Code of Practice 13 details the specific requirements for tattooing activities, in addition to those laid down in the Regulations applicable to all special treatment licensed premises. It notes that tattoo artists who are unable to demonstrate hygiene competence may be asked to complete a Level 2 hygiene certificate.
Reducing the Risk
Infection risk can be reduced through:
Good personal hygiene (artist and client)
Effective cleaning
Separating clean and dirty materials
Correct sterilisation or disposable equipment
Artists must assess clients for skin issues (including rashes, moles and scarring), alcohol or drug use, and relevant health risks (e.g. allergies, immunosuppression, pregnancy). Artists must be vaccinated against Hepatitis B.
Tattoo stations should be treated as clinical areas. Equipment must be protected from contamination; inks must be decanted into disposable cups; distilled water used for dilution of ink and ‘green soap’ (a vegetable-oil-based surgical soap used in the tattoo industry) or for washing the needles between colours.
Dressings applied afterwards are usually transparent, self-adhesive, polyurethane film (known as second skin in the industry), similar to those used for burns and post-operative incisions, or cling film attached to the skin with surgical tape. Clear aftercare guidance should be provided verbally and in writing about how to care for the tattoo whilst it heals (no swimming, spa pools, sunbathing, perfumed soaps or scratching).
Unlicensed Tattooing
Although it is illegal to tattoo in unlicensed premises, this is rarely enforced. Anyone can buy machines and inks online and tattoo friends at home, often with limited knowledge of hygiene.
Inspections across the UK vary, with some councils inspecting only once when the studio opens, while others do so more regularly. Licensing rules differ widely outside the UK. Excellent tattoo studios can be found abroad, but so too can be deplorable hygiene. Getting a tattoo may be a more permanent souvenir of a fun holiday than a fridge magnet, but it can be risky, and alcohol and sunshine don’t help healing.
Final Thoughts
Tattooing in the UK, when performed by licensed professionals, carries a low risk of infection. I believe the demand for tattoos will grow, and I support nationally enforceable, pragmatic safety standards.
Takeaway messages:
Tattooing by licensed professionals in the UK is low risk
Nationally recognised training and regulation are likely to emerge
A tattoo is a controlled wound—so please, as I once observed, don’t let your dog lick it
Kondakala, Sandeep et al. Microbiology of tattoo-associated infections since 1820 The Lancet Microbe, Volume 6, Issue 4, 101005
Training For Aspiring Tattoo Artists:
After two years in the tattoo industry, I now work with licensed tattoo artist, TomCatTatt, to provide introductory training for aspiring tattoo artists, covering the basics in safety and hygiene, legislation and licensing, and an introduction to tattooing techniques. Contact me for more information: julieru13@hotmail.com.
It’s the most wonderful time of the year! It’s time for the annual Environment Network meeting, where we get together to talk all things environmental microbiology; sharing new research and experience to improve practice. And your guide for the conference this year, live blogging the morning session, is the token immunologist in the group, Dr Claire Walker.
What is the environment network?
Before we get onto todays’ content, a little introduction to what the Environment Network is.
The Environment Network works to support people in clinical, engineering and scientific roles who are interested in environmental infection prevention and control (IPC) and/or the built environment
Do you want to know more about what to do with your water screening and air sampling results? Are you keen to understand the evidence behind equipment cleaning and the role of the environment in healthcare associated infection?
Then welcome to the Environment Network!
This is a network for people in clinical/scientific/engineering roles within the NHS and other associated organisations who are interested in the role of environmental infection prevention and control in preventing infection.
The aim of the network is to support infection prevention and control professionals involved in commissioning, environmental audit, water, air and surface testing within their Trusts. By working together we can share best practice between Trusts; as well as circulating the latest evidence and discussing personal experiences.
What are the aims of the network?
To support the development of member networks
To provide events where shared learning can be supported
To permit sharing of experiences and best practice to improve clinical interventions
To support and share research in order to achieve improvements in evidence based practice
What is our remit?
Environmental testing and monitoring within healthcare environments
On to today. First up we have Gavin Wood, an authorising engineer for water who acts as an independent advisor to Trusts. He is covering the fascinating topic of water associate outbreaks and what we can ask of our water safety groups during an outbreak. There should always be a policy which covers how to organise the estates teams and the water safety groups – covering who is responsible for each area during the outbreak. Regular outbreaks are caused by organisms like Legionella and Pseudomonas, but might include non-tuberculosis causing mycobacteria. Detection of these organisms during routine screening is reported to the water safety group to assess potential risk. Most pathogens that we look at will grow within a certain temperature range, so maintaining cold water as cold, and hot water as hot is essential. What we really don’t want is warm water stagnating in the system as the pathogens can thrive in it. On top of this, we need chemical control of organisms – mostly silver and copper ion systems. Stagnant areas of warm water are pockets where the pathogens might thrive so flushing the system and chemical controls are key in maintaining a healthy water supply in hospitals. Controls that are effective for indicator organisms that we routinely test for, like legionella, tend to be effective for any other outbreak organisms. In an outbreak situation the first port of call is the Legionella risk assessment which considers the efficacy of temperature and chemical control. After this, in line with guidance, all trusts should refer to their Water Safety Plan which is contains the detail on actions to take when results are outside the expected limits. Most of the time the authorised engineer already has the answers because the system is repeatedly routinely tested.
Like any system in a hospital, it is vital that the risk assessment and training is up to date. As Gavin says if we haven’t covered everything in the risk assessment, and if the water policy hasn’t been recently reviewed then the whole system is vulnerable. External audit by authorise engineers ensures the system remains optimal. Investigation of an outbreak focuses on the patient pathway – where has the visitor or patient been on their journey through the hospital. This process finds the clues to identify the source of the environmental outbreak. Surprisingly one of the main pieces of evidence comes from review of training and competence records, is everyone appropriately trained and acting in accordance with policy. If in doubt, going an witnessing monitoring and maintenance tasks can provide essential information in a high pressure outbreak situation. Gavin drives home how important practice is in this – we need this information as much on a random rainy Tuesday as much as we need it during a Legionella outbreak!
Our next talk comes from Karren Staniforth from UKHSA. She is a clinical scientist and UKHSA IPC specialist adviser, and is talking to us about the pros and cons of different outbreak investigation techniques. Karren invites us to imagine painting a busy ward in different colour 10cm squares, every single surface with a cotton tip swab. Imagine how long that could take and just how many squares you would end up with! Even if you took 200 samples, how many squares have you failed to test? Usually we can only take 20-40 samples…. So even if they all come back negative, it doesn’t necessarily mean there isn’t an organism there – its just that the sampling didn’t find it. The chances of going in and finding nothing is quite high, but if you put a patient in that room for a week, they will almost certainly find that organism (not that we recommend that as a testing method!).
Karren reminds us that reading environmental plates is quite an art and different from clinical samples, it’s a different skill and guidance from experts is essential. Clinical diagnostic laboratories aren’t accredited to process environmental samples and the staff aren’t trained to process and analyse this work. Commercial companies can come and do testing for you, and they are extremely good at routine work. Bespoke work is harder to commission, and that’s where knowing the network can really help! So if you have an outbreak of something unusual, it’s hard to find the information on what level of environmental organisms – like aspergillus – are ok, and what constitutes a danger to patients.
The questions becomes, what type of samples do we want to take and why? We need to understand basal levels of indicator organisms to work out when to act. Building on what Gavin has shared this morning, you need to look – really look- at what is happening in your environment. Karren reflects on how useful an audit can be but we don’t go into an outbreak with the information already in front of you, so your audit probably won’t ask exactly the right questions. Epidemiology provides the answers – which organisms and then which patients are affected, where and when? Identifying common exposures can be easy when infections match case distribution e.g. sequential patients with the same infection in the same room. However some are less obvious like laundry delivered to multiple sites causing infection clusters which are miles apart or commercial products that might only impact high risk patients in very low numbers, but at multiple sites across countries. This can be exceptionally difficult to trace. Though remember not every exposure results in colonisation and infection, and even if exposure is universal some patient groups are more likely to develop infections than others.
Knowing what kind of sample to take is essential, especially when sample numbers are limited. Negative results can be just as useful as positive results – and identifying the source of the outbreak is as much detective work as it is learning to read plates! Karren reminds us – ‘You don’t always need sampling, somethings are just WRONG!’.
To close the first session, we have Louise Clarke who knows everything there is to know about proper ventilation. Ventilation is essential the movement of air within a system. The law tells us we must provide ventilation under the Healthy and Safety at Work Act, and building regulations set a minimum standard for ventilation. The main reason for good ventilation is to have a safe and comfortable environment; to remove odours, to control temperature and importantly to protect from harmful organisms and toxic substances. We have natural ventilation (like opening a window!), mechanical ventilation which pushes air around the building and a mixed mode – a combination of the two. The preferred method for ventilating a hospital remains natural ventilation, something which really shocked the group. It might work well on a windy day but it certainly doesn’t cover all areas and some times of year, like winter, it’s really no good at all.
Like Lou says, simple is best. When we talk about ventilation, we need to ask what is the issue we are looking at? Human elements are usually a key element to understanding problems in ventilation – you need to think about when the issue arose and who was involved? Often there is a significant time lag between the problem starting and it’s detection in real time. You can be left scrabbling around for details long after the issue began. Lou walked us through the potential information sources to considering during an outbreak, including design records. Which tend to be a little less useful than you would imagine, considering they often tell you the purpose the room was designed for 30 years ago – perhaps not so relevant now! Echoing the sentiments of Karren earlier, one of the most important things you can do is go physically and take a look – not an audit, just turn up and use all your senses!
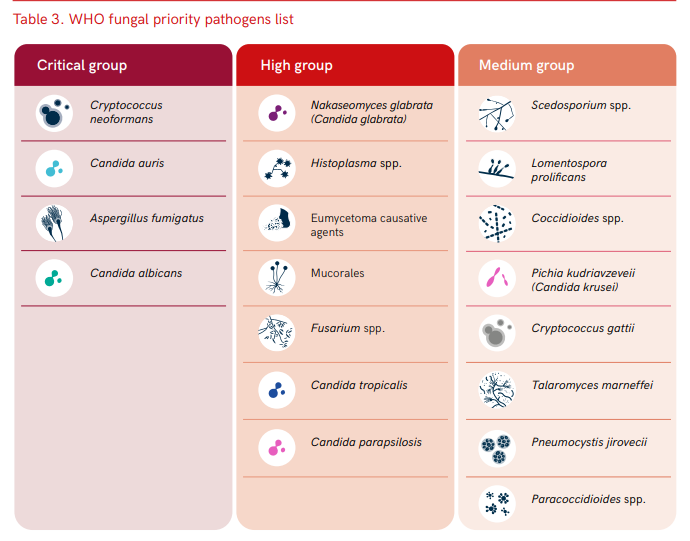
To kick off the session after a much needed cup of tea (Earl Grey, hot!) we have Dr Mariyam Mirfenderesky who is talking about the challenges of managing fungal outbreaks. Candidozyma auris (note the new name!) is probably one of the most difficult outbreak causing organism to manage. To help with this a Clinical Expert Reference Group was established in March 2025. Candida species are the dominating fungal pathogens of invasive fungal disease and account for >85% of fungaemia in Europe and the United States. Candidozyma auris was first identified in 2009 from a Japanese patient with ear discharge, and is a critical WHO priority fungal pathogen. It is fluconazole resistant and has a propensity to cause healthcare associated infection outbreaks. There are 6 independent clades, with clade 1 dominating in England. Mariyam walked us through the identification of the first neonatal case of C.auris from an eye swab – it was found in two infants, five weeks apart with no direct contact between the children. Fortunately both were colonisation with the fungus only. She then discussed the safety measures that should be in place to manage this difficult pathogen – particularly focusing on why the current cleaning protocols are insufficient to manage this threat. Her final points considered how to act when you detect C.auris – you must be decisive and act!
If you’d like to know more about C. auris, check out this blog post from earlier this year:
Next we have Dr John Hartley who is talking to us about investigating environmental surface mediated outbreaks – what you can’t see may still hurt you. Using the classic movie ‘the fiend without a face’ as a metaphor for IPC, John introduced the idea of modes of transmission between individuals. It feels like a simple problem, its just cleaning and handwashing after all! But we see there is a complex person-organism-environment dynamic system, and as John says, there is always a well known solution to every human problem – neat, plausible and wrong! John highlights the importance of continual surveillance and knowing ‘where the fiend is’. The controls are based on a four pronged approach – clean, replace, destroy or rebuild.
By way of a case study, John told us about his experience of managing adenovirus outbreaks in a paediatric BMT ward. This is a very common virus causing 5-10% of febrile illness in early childhood. Almost everyone has had it, and it can establish latency which can reactivate during BMT. More often it causes severe morbidity and mortality in these patients who can develop hepatitis. What you can’t tell is if the child caught adenovirus from the environment or if it has reactivated post latency. However, whole genome sequencing (WGS) can resolve 1-3 SNPs across genomes – its not like looking for a needle in a haystack, its rather like looking for a needle in the whole of Texas. But WGS can be used to confirm or refute cross infection events.
Of course the next question is, what can be done? Visual assessment is not a reliable indicator of surface cleanliness, John described the varied methods which can be used to detect adenovirus. Then we need to develop the right tools to manage it – including development of environmental PCR as a measure of cleaning efficacy by GirlyMicro herself! Finishing on a Dr Who reference to delight a crowd of scientists is always a win – even if it is comparing adenovirus to the scariest episode, the weeping angels! Of course, when monitoring adenovirus, the most important advice is ‘Don’t Blink’.
To close the morning session we have Dr Sam Watkin discussing research tools to help predict the future of outbreaks. Sam began acknowledging the current challenges facing preventing transmission of environmental organisms. In his PhD he aimed to identify how microbes disseminate through the clinical space, if the starting contamination site determined how is was disseminated and if the usage of space influenced microbial transmission risk. IPC is often retrospective to the aim was to develop research tools to allow the development of prospective knowledge. Sam used cauliflower mosaic virus DNA markers as a surrogate for pathogens, and followed its movement around two different units. It was shocking to see how far this benign organism could spread in such a short time.
I think if we take away anything this morning it’s that nobody likes the new name for C.auris, and death, death to recirculating air conditioning units!
The morning was followed in the afternoon by a series of case discussions in order to help implement the learning from the morning, help everyone get to know each other, and support the sharing of peer to peer learning. The case discussions this year included:
Case discussion one (Facilitated by Dr John Hartley):
Seek and remove: approaches to source control for environmental surface mediated outbreaks
Case discussion two (Facilitated by Professor Elaine Cloutman-Green):
How to implement a multi-disciplinary approach to investigation of water borne outbreaks
Case discussion three (Facilitated by Louise Clarke):
Interpretation of ventilation data and applying it to ventilation risk assessments
Case discussion four (Facilitated by Dr Sam Watkin):
Determining the role of equipment in outbreaks: how do you investigate?
Case discussion five (Facilitated by Karren Staniforth):
Introducing new cleaning process: what should you consider?
Case discussion six (Facilitated by Dr Claire Walker):
Choosing new equipment and furnishings: what questions should you ask?
It was truly inspiring to hear the buzz in the room that all of the discussion created. Thank you to Mr Girlymicro (Jon Cloutman-Green) for being in charge of photography, and to all of our speakers and facilitators for making the day happen. Also, massive shout out to Ant De Souza for pulling the day together, Angela McGee for making sure we all turned up to the right place at the right time, Mummy Girlymicro for running the reception desk, and to Richard Axell for supporting all of the tech on the day.
Now it is all over, the only thing to do is to tap our feet until we all get to meet again in 2026, although the presentations and discussion sheets should go up some time during 2025. Until then however, if you want to know more either head to the Environment Network website to look at info from previous years, or read some of the other blog posts linked to environmental IPC down below.
For my birthday in 2014, I celebrated by submitted by PhD thesis for printing. I ripped off the band aid and committed.
For this birthday, 11 years later, I’m taking another leap of faith, and once more rolling the dice on myself. This time it’s still PhD related, but rather different. This time it’s to let you all know that I have written a book, which will hopefully go live on Amazon on Friday the 17th October.
It feels like birthday launches could become a tradition.
I’ve been talking about a super secret project for a while now, and the wonderful Dr Claire Walker has been taking on some heavy lifting in terms of arranging some guest blogs, so that I could write a book on my weekends rather than writing a blog. But what is the book, and why did it come about?
The Book
The book is entitled ‘It Shouldn’t Happen to a PhD Student: How to thrive, not just survive, during your PhD’. It has 40 chapters that take you all the way through from deciding you want to do to PhD, and thinking about where and what type, to submitting your thesis, and what kind of skills you may need to develop during your PhD to maximise your career success after it is done.
Professor Elaine Cloutman-Green, otherwise known as “The Girlymicrobiologist”, is a clinical academic with over 2 decades of experience leading research projects and supporting students at all levels, including PhDs. She also runs the popular Girlymicrobiologist blog, which aims to de-mystify science and support those wanting to engage with academic careers from A-level all the way through to career enrichment.
In this book, Girlymicro talks about the reality of what it is like to study for a PhD, what gateways you may need to pass through, and how to manage key relationships in order to achieve success.
This book starts at the very beginning, with why you might want to do a PhD, how you might decide what route to PhD is right for you, and what a successful application might look like.
It then takes you through your PhD journey, year by year, with tips about how to approach and succeed during significant moments, such as attending your first conference, or writing your first academic paper.
Finally, you will discover what other skills you need to develop during your PhD to give you the best route to success after your viva. All of this supported by links to activities on the Girlymicrobiologist blog, to help you with practical exercises in order to apply what you have learned.
Whether you’re planning your PhD, a healthcare professional looking to develop, or simply curious to know about how the world of academia works, The Girlymicrobiologist offers a refreshing blend of knowledge and relatable experiences. Get ready to laugh, learn, and be inspired to find a way into, what she describes as the best job on the planet.
This is the book I wish that someone had given me when I started on my PhD. I was pretty clueless and spent a lot of time finding my way, and making heaps of mistakes. It seemed only fair to write all of my learning down so that I can share it, not just with my own students but more widely, so that everyone is free to make their own new mistakes, not just repeat ones I’ve already made.
The Why
I’ve been talking about writing a book for ages, and I still have the original Girlymicro book I’d planned going on in the background. I was prompted to do this book now though, after spending an afternoon at an awards event and realising that I could tell you every person who was going to win in every category before the dinner even started. It made me think a lot about access and privilege. That night I came home and I was really glum, and I couldn’t quite process why I was feeling that way.
I slept on it and spent some time speaking to Mr Girlymicro the next day to process my thoughts. I talked about how much access to healthcare professions and even academic training schemes are now based on who you know, to describe the best way to get through gateways like applications and interviews. How, even once you are in them, to feel like you understand how things work and the undisclosed boxes that need ticking, you need to have someone who will let you in and tell you the unwritten rules, and frankly not all supervisors see that as their role. This means that I really feel like we are missing out on some amazing talent. People who would make wonderful PhD students, or academics, because they can’t get across the threshold or see themselves in the role.
Not everyone has strong connections with a university. Still fewer people know someone who has a PhD. The way the system currently feels is that if you can access information you really have such an advantage over those that don’t. I therefore see a lot of my medical colleagues getting access to PhD funding, and yet fewer and fewer of my nursing and scientific colleagues. I increasingly encounter more and more undergraduates who are reaching out because they need help to know why they aren’t being successful, because they don’t know what is expected of them. It has always been hard to get onto PhD programmes, and it should be. What it shouldn’t be is hard because you don’t have access to the right people to give you the knowledge you need to level the playing field.
I realised that was why I was feeling upset and unsettled. I don’t like unfairness. I don’t like inequity. I don’t like realising that I’m part of the problem. Mr Girlymicro commented, as I was off loading, that I had plenty of blog posts that talk about how to apply for and do a PhD, and so why didn’t I take the way I was feeling and turn it into something positive. A book. So, this book concept was born. A book where I set out to play my role in fixing the disparities as I see them.
The Vision
That conversation happened right at the end of May. I gave myself 3 months to take some content form this blog, as well as creating new content, to come up with a book of ~80,000 words that captures the advice I give to my PhD students, and those approaching me floating the concept of applying for a PhD.
Why 3 months? Well, if I allowed myself a year, I would take a year, and remember that other book? I still want that to happen at some point. The other thing was that I wanted it finished as close to the start of the academic year as possible, so that it could start benefiting people right away. We all also know that I have no patience, and so using my birthday as a cut off always felt right.
The book was finished at the end of August, and I’m in final edits before upload at the end of the month. I want it to be the kind of resource that people can dip in and out of, whether they are doing a PhD or not. Chapters, such as developing goals, or on public speaking, should stand alone to benefit even those who are not in academic study. The activities that can be accessed alongside the book, to help things like developing your elevator pitch, should only grow in number over time, and hopefully will be a good general resource for anyone that finds them, not just for those who are studying for a PhD.
My main hope however, is that people who are on a PhD will find it not only helpful, but something that will help them feel a little less alone in the process. There were times, as I was doing my PhD outside of a standard academic department, that I felt really lonely, and sometimes even very lost. Not everyone has a super supportive supervisor, not everyone finds those peers that keep you going. I was lucky that I had great colleagues who picked me, not everyone has that. I hope that this book can act a little like the friend you need, who you can turn to for advice, and to know that others have been there before and found a way to succeed.
What to Expect
I don’t know what to expect to be honest. I’ve never written a book entirely alone before, with thanks to Dr Helen Rickard and Dr Sam Watkin who have contributed text. I know why I needed to write this book, and as I say in the first chapter, knowing your why is the most important thing. I don’t expect it to be perfect, nothing is, but as I say to my students, the main thing is that it is done.
The book should go live on Amazon (depending on their turn around time) on Friday 17th October. It should be purchasable in 3 forms:
Ebook for £2.99 or included in your ebook subscription if you have one and free to download
Paperback for £9.99
Hardback for £15.99
None of this is about making money for me, but Amazon have minimum costs, especially if you want it to be available widely, so there we go.
To mark the occasion, although it is terrifying me at the moment, I’m holding a small book launch event at UCL on the same night. If you fancy, come and join me. After all, we should all do a little something that scares us, and I’m hoping if I feed you wine you will forgive any deficiencies knowing the reasons why this book came into being in the first place.
If you like, I’m kinda hoping you might also tell your friends…
Following on from the wonderful fungal post on fungal toxins (mycotoxins) last week from Dr Sam Watkin, I wanted to follow up with a post on the latest fungi of interest from a clinical perspective, Candidozyma auris. This fungi is getting more and more coverage, as well as becoming more important in healthcare, so I thought I would take a moment to talk about what it is, what it does, how to find it, and what to do when you do.
In a pre-pandemic world, which feels like a long time ago, Professor Lena Ciric was working at a media fellowship, and as part of that work wrote an article for the BBC on Candida auris, which has subsequently been renamed to Candidozyma auris.
This article came out in 2019, so maybe C. auris is not so new but in terms of the numbers of cases we are seeing within the NHS, and the changing prevalence out in healthcare systems more widely, it is definitely more of a feature and a concern than it was back then. Reflecting this change the UKHSA guidance Candidozyma auris (formerly Candida auris): guidance for acute healthcare settings which was originally published in 2016, has been updated recently (19th March 2025). It feels timely therefore to put something out in order to raise awareness of this organism and the unique challenges it presents.
NB I can neither spell nor pronounce Candidozyma auris and so we’re sticking to C. auris from this point out.
Yeast are a type of fungus, and Candida species are often associated with colonisation (present without causing infection or symptoms) on skin, in the mouth or within the vagina. If they grow up to high levels they can cause an infection called candidiasis, which often causes symptoms like itching or discharge. Common infections include Thrush and nappy rash. Candida albicans is one of the most common yeast infections seen within the healthcare setting, and in this kind of environment more serious infections can be seen, especially those linked to the blood stream, and occasionally serious organ infections.
C. auris was originally believed to be a relatively new species of genus Candida, as it often behaves in a similar way to the other Candida species. The reason for the name change to Candidozyma auris, was because, although in many ways it behaves similarly to its Candida cousins, it does have some differences in the way it behaves. These include features such as intrinsic antifungal resistance and growth conditions, that make it useful to characterise in a way that acknowledges it as a novel genus in its own right.
What is the difference between C. auris and the other Candida species that you know?
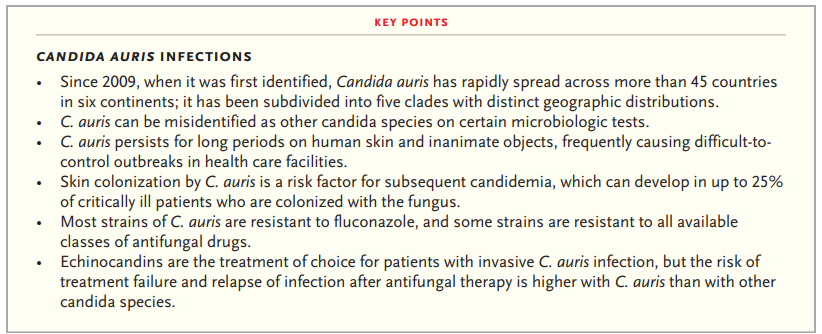
Many Candida species can cause severe infections within specific settings, however C. auris has been known to not only cause a wide variety of infections (bloodstream, intra-abdominal, bone and cerebrospinal fluid (CSF) infections), but ones which lead to significant mortality rates, with an estimated rate of 30 – 72% in severe infection reported in the literature.
Infections can occur in any patient group, although UK outbreaks have been most frequent associated with adult settings. Augmented care settings (such as intensive care and transplant settings) are at highest risk due to the vulnerable, long stay nature of many of their patients. Management of any infection occurring is complicated by the fact that C. auris has developed resistance to many available classes of antifungals, with emergence of pan-resistant strains, which add to the mortality risk.
C. auris also appears able to both easily transmit and colonise the skin of patients, with most patients being colonised before they go on to develop any subsequent infection. These colonised patients can then contaminate their healthcare environments, and unlike other yeast species, C. auris is able to survive and represent a continued risk within the environment for prolonged periods, all of which contributes to outbreak risk.
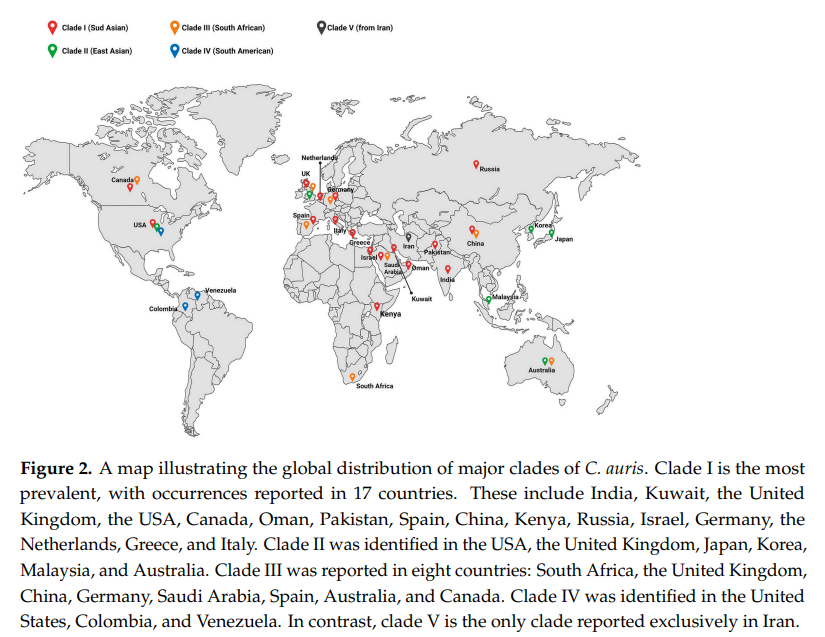
It was first identified in the ear canal of a patient in Japan in 2009, but has since been found globally, and is now separated into six genetically distinct clades:
Clade I = the South Asian clade, first detected in India and Pakistan
Clade II = the East Asian clade, first detected in Japan
Clade III = the South African clade, first detected in South Africa
Clade IV = the South American clade, first detected in Venezuela
Within the UK from January 2013 – December 2024, 637 C. auris isolates were reported through laboratory surveillance in England, with 59 (9.3%) isolated from blood culture specimens. It should be noted that not all labs report, and for some time many labs could not accurately identify C. auris, or actively screened for it, and so this may represent under reporting. A routine whole genome sequencing service is not currently available for typing, although it can be undertaken linked to specific outbreaks. Hopefully this will be up and running soon to better understand how the different clades discussed above are represented in the UK, and whether any of them are linked to more challenging outcomes than others.
Due to its global distribution, overseas patients may also be at increased risk of introducing C. auris into UK healthcare settings, with one centre reported 1.6% of their overseas admission detected as colonised, with patients coming from the Middle East, India and Pakistan, showing higher levels of recovery.
UKHSA guidance suggests we should screen any patient who has had an overnight stay in a healthcare facility outside of the UK in the previous year, as well as patients patients coming from affected units in the UK. This sounds relatively straight forward, but it can be challenging to identify patients who have had an overnight stay overseas on admission if they are not being admitted from overseas. It also relies on clear communication from other centres that they have an issue, if we are to screen patients from impacted units. Many centres have therefore decided to screen all patients on high-risk wards, such as intensive care, to address some of this unknown risk.
Risk factors for developing C. auris colonisation or infection should be considered when deciding on screening strategies and the list within the UKHSA guidance includes patients who have experience:
healthcare abroad, including repatriations or international patient transfers to UK hospitals for medical care, especially from countries with ongoing transmissions
recent surgery, including vascular surgery within 30 days
prolonged stay in critical care
severe underlying disease with immunosuppression, such as HIV and bone marrow transplantation
corticosteroid therapy
neutropenia
malignancy
chronic kidney disease or diabetes mellitus
mechanical ventilation
presence of a central-venous catheter or urinary catheter
extra-ventricular CSF drainage device
prolonged exposure to broad-spectrum antibiotic or antifungal use
Screening is undertaken by taking swabs from the axilla (armpit), groin and nose, although different patient groups may require additional screening. Patient surveillance is important for two reasons:
1) to understand which patients are colonised in order to introduce additional precautions to limit risk of transmission to other patients or the environment
2) to support improved patient management but allowing patients to be put on the most effective antifungal if they go on to develop any signs of yeast infection, in order to improve outcomes
If a patient is detected as positive, other screening sites can help manage individual patients and so UKHSA say additional site screening should be considered:
urine (especially if there is a urinary catheter in-situ, including intermittent self-catheterisation)
throat swab
perineal swab
rectal swab (in paediatrics we would consider a stool sample instead)
low vaginal swab
sputum or endotracheal secretions
drain fluid (abdominal, pelvic or mediastinal)
vascular access sites
wounds or broken skin
ear
umbilical area (neonates)
Swabs should ideally be processed on chromogenic media (colour changing agar plates) and fungal colonies confirmed using MALDI ToF or a validated PCR (my previous post on PCR may help with this). It can also be helpful to incubate plates at 40oC, as C. auris can grow as much higher temperatures than its Candida cousins, which can help with identification. If grown then the yeast should be stored in case you need them for future typing to help in understanding transmissions or outbreaks.
Why should we care about it?
Due to the high mortality rates for patients who develop infections, and the issues with choosing antifungals that work, it is really important that we know when we have patients who are colonised with C. auris. Controlling spread, even if patients don’t become infected, is incredibly important for the individual. This is because if a patient is detected as positive they won’t be de-alerted (have IPC precautions stopped) at any point and so it will impact them for months, if not years. These IPC precautions include isolation (keeping separate from other patients), and sometimes only being nursed by specific members of staff. These patient and staff impacts are so significant they’ve even been acknowledged in popular media, with a three episode arch covering C. auris in The Resident on Netflix (season three, episodes 18, 19 and 20).
Are there differences in how you might treat?
As I’ve already said, C. auris is pretty resistant to treatment compared to its Candida cousins. UK data indicates that isolates are resistant (don’t respond to) to the normal first line treatment of fluconazole, and often to other antifungals within the azole class. Some isolates have been resistant to other commonly used antifungals, such as amphotericin B (20%) and echinocandins (10%). Resistance to other antifungals can also occur whilst infections are being treated, and so it is important to monitor sensitivities (whether the drug works) and send to reference labs in order to understand the most appropriate therapy. Its resistance profile is one of the reasons the WHO have highlighted C. auris as a priority fungal pathogen for further research and to highlight clinical risk.
Its not just antifungals that are important however, antimicrobial stewardship is important in general, as prolonged exposure to broad-spectrum antibiotics and antifungal agents are risk factors for both C. auris colonisation and infection (again this links back to the high risk patient groups impacted). Therefore, doing a better job of monitoring and controlling antimicrobials in general is likely to have a beneficial impact on C. auris risk.
Challenges with environmental control
One of the many things I love about the new C. auris guidance is its focus on multidisciplinary input ‘Healthcare workers are encouraged to work in multi-disciplinary teams, including Clinical Infection Specialists and IPC teams, to risk assess and support the management of patients infected or colonised with C. auris‘. I think this is so important, especially with an organism that is so challenging and can present such a high risk.
Environmental control is a particular issue for C. auris as we know it’s ability to survive and can grow at higher temperatures than many other fungi, means that it is likely to survive well in the environment. It also has the ability to form environmental biofilms, which can mean it is difficult to impact effectively using standard cleaning techniques, and once within the environment has been been detected for 4 weeks.
Within the UKHSA documentation, environmental contamination for C. auris has been found on the following surfaces during outbreaks:
beds, bedside equipment, bedding materials including mattresses, bed sheets and pillows
ventilation grilles and air conditioning units
radiators
windowsills and other horizontal surfaces
hand wash basins, sink drains and taps
floors
bathrooms doors and walls
disposable and reusable equipment such as ventilators, skin-surface temperature probes, blood pressure cuffs, electrocardiogram leads, stethoscopes, pulse oximeters and cloth lanyards
Basically most of your healthcare environment, whether fixed or movable features. In order to help stop the transfer from patients to the environment, via staff, the use of personal protective equipment is really important. Therefore the use of gowns and gloves is suggested. Single use and disposable equipment should also be used whenever possible, and patients should be kept in single, ensuite rooms, to minimise the risk of C. auris escaping from within the bed space to adjacent clinical environments. Any items within the space should either be cleanable with a disinfectant, or disposed of after a patient leaves. One thousand ppm of available chlorine should be used for cleaning, but needs to be used in concert with an appropriate contact time if it is to be effective.
WHO fungal priority pathogens list to guide research, development and public health action 2022
Outbreaks
Most detections of C. auris cases detected are colonisation rather than infection (though colonisations can lead to subsequent infections). Within the UK there have been 5 significant outbreak of C. auris, each with over 50 cases, in addition to many sporadic introductions of single cases, frequently from overseas. Many of these have been in London or the South of England, and have resulted in considerable disruption to services over a prolonged period of time. This disruption can, in itself, be a risk to patients as it can result in delayed access to care. Outbreaks are also financially significant, with outbreaks reported as costing over £1 million for a service impacted for 7 months.
Although outbreak numbers are currently small, they are becoming more frequent, and even if infrequent have significant impacts. The need to control this risk before it becomes endemic within the UK health system is therefore significant. It is crucial therefore to collect more data and understand transmission routes of C. auris better.
Despite probable under reporting, it is clear that C. auris is becoming more common within UK healthcare settings, and has the ability to both cause significant issues for both individual patients and for services, due to outbreak impacts. Although fairly new on the scene there is increasing recognition of how C. auris could change fungal risks within healthcare, and even long stay residential settings. If we are going to adjust approaches in order to react to the new risks C. auris represents we need to both update our current practices, and invest in research, in order to learn how to do things even better. This is the reason that it feels important to share a post that is a little more technical than normal, both to help myself by learning more, but also to ensure that we are having conversations about an organism that has the ability to impact us all.
Friday just gone, 25th April, was World DNA Day. I’ve had a series of blogs that I’ve been playing around with linked to what DNA is, how we look for and investigate it and how we are exploring DNA in our everyday lives. Linked to this I’ve also got two book reviews coming where the world changes because of genetic testing and genetic manipulation. So this is the first of four part DNA bonanza.
I thought I would write these posts, because as much as artificial intelligence could change the way we live and is frequently discussed, we are all accessing DNA based testing more and more, with many of us not really thinking about how this too is changing the world in which we live.
I remember really clearly the first time I actively came across the concept of DNA, DNA testing and DNA manipulation. It was in Jurassic Park, when Mr DNA pops up at the start of the film to talk you through how they used DNA and cloning in order to make the dinosaurs. This film came out in 1993, I was 13 and I just remember how all of my class were queuing up to get tickets. It was the first film I really remember there being hype about, well that and Aladdin which was a different kind of seminal moment. It was the first film I remember watching and thinking just how cool science and scientists were.
In fact I talk about Mr DNA so much that the wonderful Mr Girlymicro brought me a Mr DNA Funko pop which lives on my desk at work and reminds me that the impression we make on people stays with them.
What does all this have to do with how we use DNA now? Well, in 1990 when Jurassic Park came out, the routine use of DNA, even in research, was still pretty much science fiction. The structure of DNA had only been described in 1953. Polymerase Chain Reaction (PCR), which is the main way we investigate DNA, had only been developed in 1983, and was only starting to become more widely available in the 1990’s. When I started working within healthcare in 2004, we were only really just starting to move from PCR being something that was used in research to something that was common place in clinical diagnostics. The leap from there, to a world where thousands of us can swab ourselves at home and post samples off to be diagnosed with SARS CoV2 during the pandemic, or to get information on our genetic heritage, would have sounded like something that would only occur in a science fiction novel if you’d mentioned to me back theb.
Just a flag, this part one post has a lot of the technical stuff linked to what DNA is and how we investigate it. You may want to skip this post and head directly for part two if you don’t want to be reminded of secondary school science, but if you can bear with me I think it will help some of the context.
What is DNA?
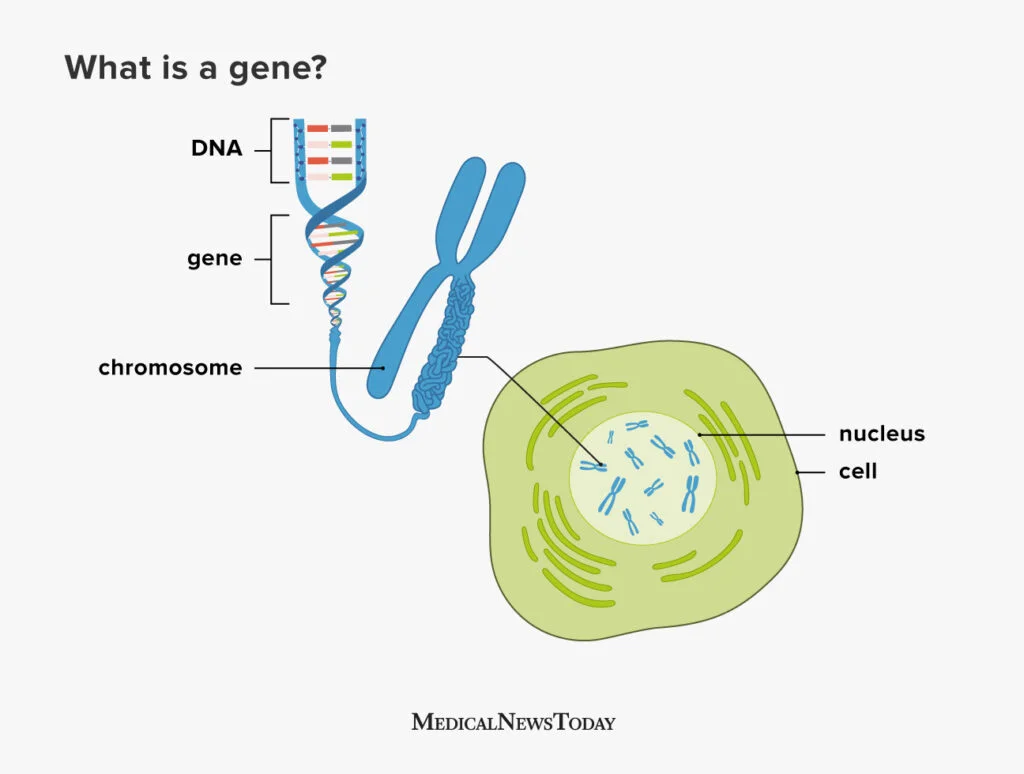
DNA, or to give it its full name Deoxyribonucleic acid, is commonly referred to as the building block of life. The structure of DNA consists of a double-stranded helix held together by complementary base pairs. The nucleotides that form the base pairs are adenine, thymine, guanine or cytosine. These nucleotides act to link the two strands together via hydrogen bonds, with thymine always pairing with adenine (T-A) and guanine always pairing with cytosine (G-C).
Sections of DNA then combine together together to code for genes, which are sections of DNA that work together in order to code for proteins, that then permits the expression of our DNA in physical form.
Genes are organised into chromosomes or packages of DNA. Each chromosome is formed from a single, enormously long DNA molecule that contains a strand of many genes, with the human genome containing 3.2 × 109 DNA (3,200,000,000) nucleotide pairs, divided into 46 chromosomes formed from 23 pairs (22 pairs of different autosomes and a pair sex chromosomes).
So how do we get from DNA to proteins? The specific sequences of nucleotides that form our DNA are arranged in triplets (groups of three). To turn DNA into protein, it gets transcribed into RNA (ribonucleic acid) within cells, with each of these triplets coding (translating) into an amino acid, which then get combined together to form proteins. The amino acids combined dictate what form and function the resulting proteins takes. Proteins then serve as structural support, biochemical catalysts, hormones, enzymes, and building blocks for all the processes we need to survive as humans.
Long and short, everything comes from your DNA, it’s super important, and is unique to you, but it’s structure is complex and there’s a lot of it in each of us.
How do we investigate DNA?
Now that we know about what DNA is, and how important it is for life, not just for humans but for all living things, it makes sense why so much time and energy has been deployed into understanding more about what it means for us as a species, as well as for us as individuals.
I’ve mentioned that PCR was first developed in the 80’s but didn’t really come into routine clinical testing until the 2000’s. What is PCR though and how does it work?
I often describe PCR as a way to look for DNA that is similar to looking for a needle in a 25 story block of flats sized haystack. The human genome is 3.2 billion base pairs, and we are often looking for a fragment of DNA about 150 base pairs in length, 1/21 millionth of the genome. It’s quite the technical challenge and you can see why it took quite a while to be able to move from theoretically possible to every day use. What makes it even more complicated is that you need to know what that 150 nucleotide fragment is likely to contain or where it is likely to be positioned within those 3.2 billion base pairs to really do it well. The human genome was not fully sequenced, and therefore available to us to design against, until the year before I started my training at GOSH, 2003. The progress therefore in the last 20 years has been extraordinary, and I can only imagine what will happen in the next 20 years. Hence the book reviews that will be coming as parts 3 and 4 of this blog.
So, how does PCR work? Well the first thing to say is that there are actually a number of different types of PCR, although the basic principles are the same. For example, there are some types of PCR that target RNA. There are also types of PCR that are used more frequently within clinical settings for things like SARS CoV2 testing, that are called Real Time PCR, called that as results become available in real time rather than waiting for the end of the process. It is for Real Time PCR that the small ~150 nucleotide fragment length is an issue. So all of these processes have their own pros and cons. Like many things in science, you have to use the right process to answer the right question.
The basic principles shared between types of PCR are as follows:
Designing your primers:
Primers are the pieces of DNA that you design and make that will stick to your target piece of DNA you are interested in. The reason this works is because of the fact that the nucleotides that make up DNA are complimentary and so A binds to T, C binds to G. As DNA is double stranded you can design your primers (your equivalent to the magnets to find you needle in your haystack) so that they will bind to your specific target (the piece of DNA you are interest in). If you want to have your primer stick to a piece of DNA sequence that reads AAG CTC TTG, you would design a primer that ran TTC GAG AAC using the complementary bases, make sense?
You design one set of primers for one strand, this is called your forward primer (moving from 5′ to 3′), and then you design your reverse primer at the other end of your target for the opposite DNA strand (moving from 3′ to 5′). Doing it this way means that when you start your PCR process you end up with complete copies of your target. You will then successfully have pulled the needle from your haystack using you targeted magnets.
Undertaking the PCR:
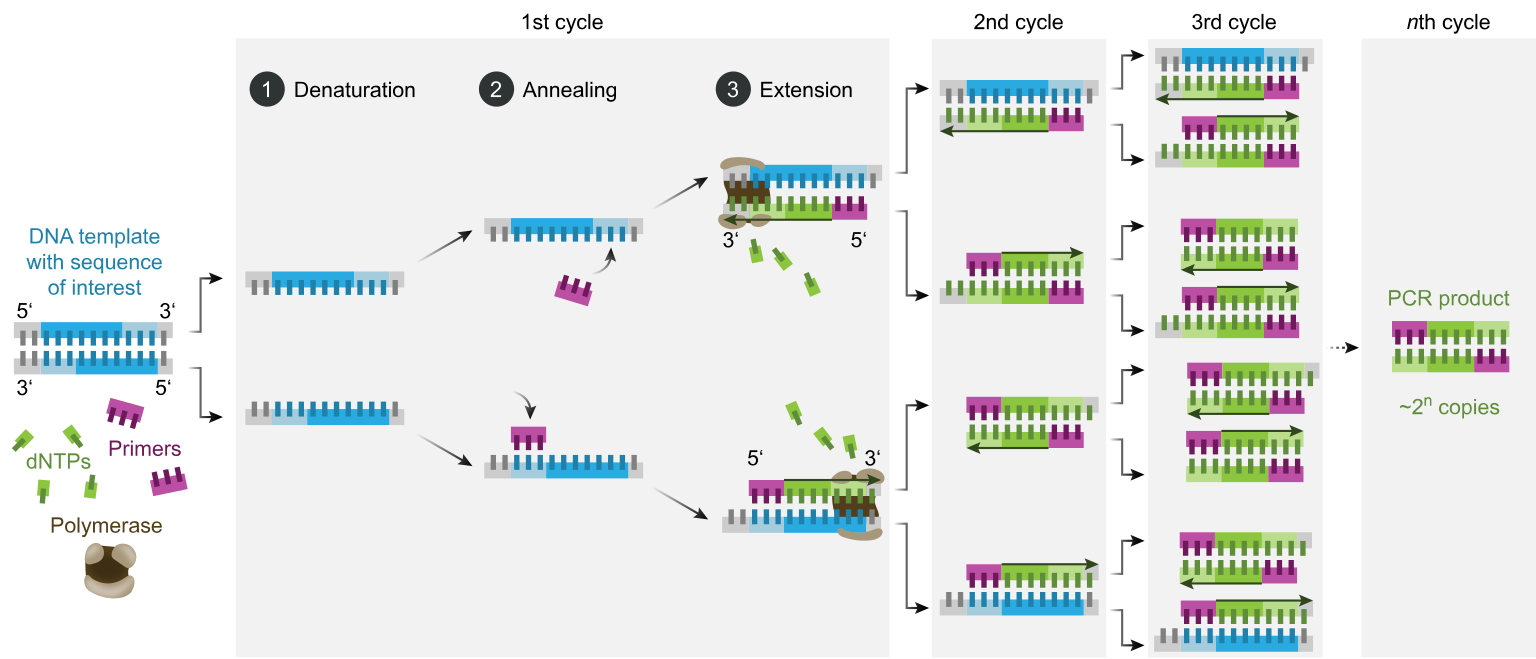
Once you’ve got your primers (which you can just order in once designed) you can then get onto the process of the PCR itself. You combine your sample that you think might contain the DNA target you are looking for (be that human, bacterial, environmental etc) with the reagents (chemicals) that you need to make the process work all in a single small tube. This tends to be a delicate process that needs to be undertaken at controlled temperatures as the protein that runs the process (Taq polymerase) is delicate and expensive. To do this we combine:
DNA Template: This is the sample that contains the DNA target you want to amplify
DNA Polymerase: Almost always this is Taq polymerase which is used due to its heat-stability as it originates from a bacteria that lives it deep sea vents. This allows it to function at the high temperatures required for PCR and is used to make the new DNA copies
Primers: These are the short, synthetic DNA sequences that you design to attach to either end of your target DNA region. These then allow the DNA polymerase to add nucleotides to create the new DNA strands
Nucleotides (dNTPs): These are single nucleotides (bases) that are then used to build the new DNA strands (adenine, thymine, guanine, and cytosine)
Buffer Solution: This solution provides the optimal conditions (pH, salt concentration) for the enzyme to function properly
Once you have your reagents you then put them on a platform that heats and cools for different steps to allow the enzymes to work and for the new DNA strands to be created:
Denaturation: The double-stranded DNA template is heated (typically to 95°C) to separate it into two single strands. This step ensures that the primers can access the DNA sequence of interest
Annealing: The temperature is lowered (typically to 50-60°C) to allow primers to bind to their complementary sequences on the single-stranded DNA. This is the step where your magnets find their needle
Extension: The temperature is raised again (usually to somewhere around 72°C, the optimal temperature for Taq polymerase activity). Taq polymerase extends the primers by adding complementary nucleotides based on the DNA sequence to create new copies of the original DNA target
These three stages are repeated in cycles, typically 20-40 times, which results in thousands and thousands of copies of the original target to be created, so that eventually your 25 storey haystack is made up of more needles than it is hay, and therefore it is easy to find what you are looking for.
Interpreting your results:
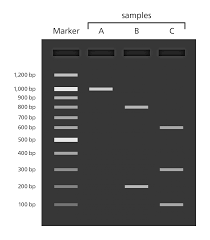
At the end of your PCR step, if you are using traditional PCR, you run what is now called your PCR product or amplicon (the things you’ve made) through something called a gel. This is just a flat jelly made of agarose (or seaweed) which also contains a dye that binds to DNA and allows to separate your DNA based on size. This allows you pick out where you have samples that have the massive amplification you are looking for, as you can see it as a band within the gel. If a band is there and the right size (as you know how big your target was supposed to be) this is a PCR positive.
If you need to know more detail than whether something is present or absent, for instance if you need to know not just that a gene is there but which variant of a gene is present, you need to be able to tell what the nucleotides that were added between your two primers actually were. To do this, you will follow up PCR with a process called sequencing.
You take your target PCR’d section and then put it through a process to work out what the nucleotides added were. This involves doing the PCR process again, to make even more copies, but the nucleotides added into the reagent mix have fluorescence attached so you can tell which ones have been added during the PCR process. G’s often produce a black colour when hit by light, A’s green, T’s red and C’s blue.
For our original sequence we talked about, AAG CTC TTG, the sequence would read Green, Green, Black then Blue, Red, Blue followed by Red Red Black. Colours are then back interpreted into a DNA sequence (a series of letters) and there you have it, you know what the DNA is between your primers and you can then interpret your sequencing result. If you have large fragments of DNA you are interested in, you may have to do this in overlapping segments and put it back together, something like a jigsaw, before you can get your answer, but the basic process is the same.
What can DNA tell us?
As I’ve said, the search for DNA and specific genes has become an increasingly normal part of providing diagnostics in healthcare. Most of us will have sent off a swab for a PCR at least once during the COVID-19 pandemic. PCRs are frequently used in my world of infectious diseases to see if a bacteria is present or absent. They are also used so that I am able to see if a bacteria will respond to an antibiotic, by seeing if they carry antibiotic resistance genes, which can be crucial to getting patients on the right treatment at the right time.
Looking for specific variants of genes is also key to making sure that the treatments we give also don’t cause any unexpected consequences. A good example of this is when we use PCR and sequencing to look at genetic variants of a gene called MT-RNR1. A specific variant in this gene, m.1555A>G, is known to increase the risk of aminoglycoside-induced hearing loss. Aminoglycosides are a crucial antibiotic class that are used pretty widely, but especially in management of some conditions such as cystic fibrosis and certain types of cancers. A small number of people have a gene that makes them prone to something called ototoxicity as a result of taking these antibiotics, resulting in hearing loss. If we know a patient has this gene variant we can then choose to use different antibiotics, improving patient outcomes and avoiding a life long hearing impact.
Outside of screening linked to patients presenting with specific conditions, the use of DNA sequencing is being utilised more widely to look for genes or conditions before they even present with symptoms, in order to reduce time to diagnosis, and hopefully to be able to find patients and start management before they’re impacted or even present as unwell. A great example of this is the newborn screening programme that started last year. This screens newborns using the heel pricks of blood taken at birth so that rare diseases that could take months or years to diagnose by traditional means are picked up early in life, therefore allowing appropriate treatment to start earlier and hopefully saving lives.
DNA is fascinating and I love knowing about it. It’s not just me though. In recent years there has been an increasing trend for people to send off their DNA for other purposes than to hospitals for clinical testing. I’m not going to say too much about this in part one, but it was this that really inspired me to write these posts in the first place and is the main focus of part two of this blog series.
Just a quick google however provides a wide number of different companies offering a variety of DNA testing services outside of the NHS (NB I don’t advocate for any of them):
Crystal Health Group: Operates a network of DNA testing clinics, offering relationship testing and other services.
23andMe: Provides DNA testing for health, ancestry, and other personal insights.
Living DNA: Focuses on both ancestry and wellbeing-related DNA testing.
MyHeritage: Provides DNA testing, particularly for ancestry research.
AncestryDNA: Company specialising in DNA testing for ancestry discovery.
The complication with all of this type of provision of testing is that outside of the clinical world in the UK, where testing should be undertaken in accredited laboratories and reporting of the results must meet certain standards, sending off DNA to private companies is much less monitored.
I hope you can see by some of the technical descriptions just how complicated these DNA processes can be. How time consuming, and how expensive to get right. There is also a lot of nuance about the different types of PCR, sequencing, gene targets, and results analysis that can be offered under the umbrella of ‘DNA testing’. Without the right people involved to make sure that there is embedded quality assurance challenges could arise, depending on what kind of testing is undertaken.
As stated in a recent Independent article:
As they’re based on estimates, I suggest treating home DNA tests as a fun investigation to get to know your family history a little better rather than a to-the-letter representation of everything that’s ever happened in your gene pool – Ella Duggan Friday 28 March 2025
The devil for all of these things really is in the detail, and we’ll get into that detail much more in part two! For those of you interested in learning more about the history of DNA testing, I’ve included a talk below. Happy World DNA Day
I got an alert of my phone last week that I set up this blog on WordPress 10 years ago! That was a bit of a shock I can tell you. That said, as I posted about in 2020, although I set up the blog and made my first post as I finished my PhD in 2015, I didn’t start posting regularly of another 5 years. I started it as I was looking for my next passion project but I didn’t really know what I wanted to say for quite a while. Despite the gap between starting and regular posting however, 10 years still feels like a gateway and something worth marking. I thought therefore that I would write something that reflects how I, my practice, and in someways the world, feels like it has changed in the last 10 years to mark the event. On the back of that, it also seemed fun to embed a few of the blog posts that have been put together since Girlymicrobiologist began in order to show how this blog too has changed and grown.
Apologies, this turned into a bit of a long one.
Microbes have changed
In 2015 I had finished my PhD in January, as well as a PGCert in Teaching and Learning in Higher and Professional Education. I had just taken my final clinical exams (Fellowship of the Royal College of Pathologists) in September and found out I’d passed them in November. After a decade of focus linked to completing what felt like an unachievable list of academic steps I was done. The question therefore was………what’s next? So, in December 2015 I started my first ever blog post, although I had been sitting on the web page for 6 months not knowing how to begin. This is how that Girlymicro blog began:
So, this is my first ever blog post. Bear with me as I don’t really know what I’m doing.
I’m what is know as a Clinical Scientist and I work in Infection Control.
Most people don’t know what a Clinical Scientist is so I thought I should briefly explain.
Most scientists that work within hospitals are involved with imaging (X-rays, CTs etc) or processing patient samples. We all work to support diagnosing patients. Did you know that scientists are involved with >80% of all diagnoses within the NHS? Their work is crucial to improving patient care, but the scientists are often unsung heroes as they often never meet the patients they help.
I do not work in the lab all the time like many scientists. I’m a clinical scientist, so half my time is spent working in a patient facing role within infection control and the other half involves bringing science to infection control to make it more efficient/evidence based. I work within a hospital with a team comprised of nurses, doctors and scientists. I have a PhD in infection control. I am also working towards my final clinical qualification (Fellowship of the Royal College of Pathologists) which is the same as my medical colleagues. My job is to help the translation of the science into a form that healthcare professionals can work with. Sometimes this means working with language so we are all on the same page. Other times this means working with the latest science and technology and developing new tests that will help.
I’m passionate about my job, but I’m also aware that many people don’t know that it exists and I’m hoping that this blog will help to change that. I plan to share a bit about what my day to day life is like as well as the science which I hope will inspire others to become healthcare scientists. After all, I have the greatest job in the world. And that is worth shouting about.
During the 10 years between setting up the website, with a world of good intentions, and writing today, many things have changed. Not least of all are the organisms people care about and the way transmission is understood. My PhD thesis was on the role of the environment in transmission of healthcare acquired infection. In many ways, getting papers published out of it was a struggle as very few journals were interested in the built environment and Infection Prevention and Control (IPC). Now organisations such as the Healthcare Infection Society run entire events linked to it, and I run something called the Environmental IPC Network, as the topics impacts so many of us. On a national level I’m now involved in writing guidelines to help support environmental IPC, all of which was a pipe dream when my thesis was being written. It felt like a very lonely area to be working in, but over the last 10 years it feels like the built environment is finally being recognised as an important component to how we keep patients safe in the world of IPC. I’ve now even had my own PhD students continue the work.
The other thing that has changed are the organisms that are perceived as being important. Even more though, there are organisms that were not even thought about in 2015, or didn’t exist, that can or are impacting so many lives, for instance Candida auris is a new kid on the block, and Mpox was called something completely different. Few people cared about Gram negative bacteria when I started my PhD, let alone Adeno. This was true even to a certain extent when I finished. I’ve worked on Adenovirus for over 2 decades, so it feels especially vindicating to see it make it onto the UKHSA priority pathogen list for research. All of this is to say, you don’t need to follow the crowd, if you find a problem that you believe is important enough, stick at it. Gather the evidence and put it out there. Eventually you’ll find others that join you in seeing the significance of your direction of travel.
Speaking of organisms, in 2015 we testing for the odd Coronavirus, and of course the severe acute respiratory syndrome (SARS) outbreak had happened, and the Middle Eastern Coronavirus (MERS) outbreak was ongoing. Many of us had been concerned with the potential of Coronaviruses to cause a pandemic, but most of the planning was still linked to Influenza based risks, as that was what had been seen historically. Awareness sadly does not necessarily link to preparedness, and as lived experience shows, the SARS CoV2 pandemic was both fast and devastating. We were unprepared, but I don’t know that we ever could have been.
Outbreaks with a worldwide distribution are not unusual and the table below shows just how many have happened or have been ongoing from 2015 onward. It also shows that not all outbreaks with world wide spread are considered to be pandemics, and not all pandemics have death tolls in the millions. In fact a pandemic is defined as “an epidemic occurring worldwide, or over a very wide area, crossing international boundaries and usually affecting a large number of people”. With this classical definition including nothing about population immunity, virology or disease severity. So, preparing for a pandemic is not as simple as it can initial appear.
NB for ease I grabbed this list from Wikipedia, please don’t judge me for it
The table also shows quite how hard life can be in the world of IPC as the organisms don’t stop because we are tired and need a break. In fact the world re-opening post pandemic, combined with some of the scientific distrust that the political handling of the pandemic created, and the fear people experienced, means that managing outbreaks since has been an ongoing struggle. Vaccine hesitancy is having a real impact on transmission and making a key line of defense less effective. Many experienced experts in this field and others related to infection and public health have now retired or moved away due to the ongoing personal impacts. This means it’s more important than ever to turn up, be seen and to have engaged conversations across boundaries and silo’s in order to develop trust and support patient safety. No matter how hard it feels, it is still worth it.
My clinical world has changed a lot, partly because of the changing organisms and the pandemic, but also because the patients and healthcare are changing. It can take quite a lot to keep up with all of these changes, and you have to be fully engaged with an approach that aligns with continuous learning to stay up to date. On top of this, when you start out as a trainee with over a decade of training ahead of you, you have also got a list of key education targets to prioritise. It can therefore feel very much like you are just working your way through a list of items that need to be ticked off so you can eventually get to the finish line. There is a lot of ‘onto the next thing’ as soon as you manage each key milestone because otherwise it can feel overwhelming. One of the key things I’ve realised since 2015 is the importance of cherishing the moment and recognising the importance of progress, rather than rushing from one thing to the next with my entire focus about keeping an eye on the prize.
Passing FRCPath first time is still one of the most challenging things I’ve done in over 2 decades in healthcare. To be honest, I’d rather do another PhD than take FRCPath again, any day of the week. I wish that I could have found a way forward where I didn’t let my ability to pass, or risk of failure of an exam define me, but for many years it did. I’m pretty sure that telling my younger self this would have achieved nothing, as it takes time and distance to be able to understand that the tick list isn’t everything, but just in case it helps anyone reading this……you are more than the sum of the exams you sit, the letters after your name or the achievements on your CV. You have value no matter where you are on the pathway, no matter how many diversions you have taken, and to be honest, it’s OK to also decide the end destination is no longer for you. Who you are matters more than any tick list.
Part of the way I’ve gained perspective on my own training is by supporting others now through theirs. Seeing PhD students go through their own trials and tribulations, and sharing in their eventual successes., has given me insight I couldn’t have gained any other way. Supporting Healthcare Science training, everywhere from writing curricula to mentoring individuals at all stages of their careers, has allowed me to see things from all kinds of different perspectives. It’s given me so much insight, as well as time to reflect on how I felt and what might have helped me along the way, in order to try to help others better.
I feel more seen as a Healthcare Scientist than I ever have. I feel that Healthcare Science as a discipline and a profession is more seen than it ever has been. There are so many more routes into Healthcare Science these days, with so many more options. This is a truly brilliant step forward from when I joined, when there really was only one route as a Clinical Scientist and having to really fight to show that you could do things differently if you wanted to go another way. As the same time however, all that choice can feel a bit overwhelming, and in some cases paralysing, as people just don’t know where to start. In order to reach more people and support them in navigating this changing landscape though does require a willingness to be visible, to bring ourselves and our stories, in order to show others what an amazing profession this is. To show the openness and diversity of the workforce, in order to make sure everyone knows this can be a profession that is welcoming and open to everyone. You can’t be what you can’t see, so let’s make sure we are seen!
I have been fortunate enough to have experienced opportunities that I never believed would be open to someone as normal as me. I don’t come from a privileged background. I didn’t go to private school or attend Oxbridge. I don’t have connections, or a rich family to bail me out and pay for my exams/conference fees/fancy memberships. So when I get invited or asked to do amazing things, I of course say yes, but I’d think to think I’m saying yes for more than just me. I’m going into spaces and having conversations with people so that I can represent. Represent my workforce. Represent my gender. Represent my background and represent my family. To do so is an immense honour and a privilege that I don’t ever lose sight of.
No one I knew, outside of work, had ever had a New Years Honour, so it never even occurred to me I would get one. Being able to undertake work in Africa which aims to reduce infant mortality by 20% in high mortality settings, is not work that I thought I would ever get involved with, it felt too big for someone like me. That’s just it though, ‘someone like me’. We put so many labels and restrictions on ourselves. We limit our own vision. If the last 10 years have taught me anything it’s that you probably can’t see where you will end up, there’s too much joyful chaos in life for that, but you can control saying yes. Saying yes to things that scare you. Saying yes to rooms that may intimidate. Saying yes to being open to opportunities and changes in direction, even when you have no idea where they might lead you. Half the joy is in the discovery, so put on that adventure outfit and head out the door.
I’ve talked about the tick list and why visibility matters, and not just for you as an individual. Now I want to talk a bit about glass ceilings and choosing to do things differently. I have, over the years, lost count of how many times I have been told that something wasn’t for me. Not for me because of my background, profession or gender, or maybe just because I didn’t fit in. I used to hear a lot of ‘no’ and I used to feel like others could define me. The thing I’ve learnt is, that the only person who can define you is you. You can give away your power to others and let them made those choices for you, or you can own your path, your career and your choices, in order to define yourself. I’m not saying any of this is easy. I’m not saying it is fast or straight forward. I am saying it is a choice.
I became the first non-medical Infection Control Doctor (that I know of), because I worked to create the path to get there, which hopefully others will now follow. I didn’t know that was possible when I started, and it came with a goodly number of fights along the way. There were days when I definitely believed the ‘no’s’ and didn’t think it would happen, but I kept trying, I kept showing up. It became clear that I would never make Professor at my original home within UCL, due to long standing bias for medical over scientific backgrounds. So I pivoted and found a new academic UCL home that welcomed me and supported me in my journey instead. Things that are worth fighting for take time and commitment, and nothing is guaranteed. Paths are often not well trodden, and so finding the right people to support you along the way is key. Don’t drift. Make your choices consciously. Know what you are willing to fight for. Know also what you are prepared to let go of. When things come together share the knowledge, share the path, and make it easier for others to follow. Drop that ladder down or prop the doorway open.
I had thought it was post pandemic blues but I think it’s just transitioning to another phase of life and career that got me thinking about this one. I’ve been working at GOSH for 21 years this year, pretty much my entire working life. During this time there have been two mentors that have pretty much introduced me to and gotten me through everything. In my clinical life it has been Dr John Hartley, and in my academic world it has been Professor Nigel Klein. Now, John retired part way through the pandemic, and he really is the reason I have my Consultant post, as I took his Infection Control Doctor role. Nigel sadly passed away last year, before he had the chance to retire. In my head, I’m still the new girl on the block, the new person in the department, the young upstart. It is a shock to look around and realise I am now one of the people who have been there longest and I have very large shoes to fill, knowing how unprepared I feel to fill them. The giants that have gone before have left, but I wasn’tt prepared for them to leave. I think the biggest shocker has been that there are some who now look at me in the same way that I looked at John and Nigel, when I don’t feel like I am even in the same league. I think they will always loom large in my mind, and I honour what they taught me by embedding it in my practice.
Your career can feel like such an open pathway ahead of you. Then you wake up one day and realise you, probably, have less than a decade left. It’s at moments like that you really need to think about what it is that you want to achieve, what you want to prioritise, in order to maximise the impact of the time you have left. Ten years feels like a long time, but its really just 2 cycles of PhD students, 2 large project grants and only 3 trainee Clinical Scientists. It’s no where near as long as it feels and so planning ahead takes on an all new perspective. If your a planner like me, now is the time to plan for this new phase of your career.
Learning that you can’t fix everyone or everything
Part of that planning for the future is also knowing what not take on. I am a simple soul, I like being liked. It’s taken me a long time to grow in my leadership to the point where I acknowledge that I not a god, and I don’t have a magic wand, therefore I can’t fix everything or everyone. Nor can I be liked by everyone. Part of being a leader is making tough decisions, part of being a leader is also about honesty and not saying the easy things, just to be liked. Sometimes, I have learned, putting off the difficult conversations and the difficult decisions does no one any favours and so it’s best to have them early. As a mentor, you are there to advise, but the decision are owned by the person making them. You are not people’s parents and they are not children, we should therefore be aiming for adult adult conversations. Acting like a White Knight can actually do more harm than good, as you are removing learning opportunities for those you swoop in and save. It is a difficult balance to know when to step in and when to maintain a pure supporting role. It is one that I will continue to get wrong. All I can do is learn, do my best, own the consequences, and aspire to be better.
The flip side of learning you can’t fix everything is being aware of your duty to try to make things that are in your remit of control or influence as good as they can be. As I’ve said, I have a decade left in all likelihood, and therefore my job is to ensure that I maximise the opportunities for others until the day I don’t have the ability to influence any more. My career is very much no longer about me, it’s about those who I will be leaving behind to carry on once I’m writing murder mysteries and drinking martinis at three in the afternoon. My job is to support as many people as possible to be in the best position possible when I walk out the door for the last time. I realise it’s now my job to keep the doors open and assist people through them. Whether it’s mentorship, nominations, or speaking peoples names in rooms they haven’t been invited into, I plan to do all I can to make sure that I pay it forward every opportunity I get.
I have the job I planned for and dreamt about for 2 decades. It is my dream job and I love it I wouldn’t change it or my decision to go for it for the world. There is no doubt however that post pandemic it has been hard. I don’t know if it’s because I’m getting older, because the job and the world right now feels pretty intense and hard core, or because my body still kind of hates me for what I put it through during the pandemic, but I definitely feel burnt out and recognise that even a dream job can be a lonely place to be.
The thing is, not every day is going to be a great day. Even in a dream job there will be bits that are harder or speak to you less. It’s also OK to not be OK. The world, and especially those of us in infection control, have been through a prolonged period of pretty significant stress and trauma. We are not going to be the same people we were going in. You don’t have to change the world every moment of every day, sometimes showing up and doing your best is enough, and what your best looks like will be different at different times. I have learnt the importance of asking myself, what would I say to a friend in this situation, and to show myself the kindness that I would show to others rather than acting as my own harshest critic. Try to take a step back and give yourself the prospective you need to find a route forward.
Just the act of writing this post has made me realise how far I’ve come. If you’d asked me in 2015, I would have said being a leader is about setting an example, about getting things right, about showing competence and keeping a cool head. I’m sure leadership is about some of those things, but what I have learnt, for me, is that leadership is about authenticity.
It’s about prioritising bringing my whole self to every encounter. It’s about saying sorry when I make mistakes, rather than pretending to always be right. It’s about sharing that I too am finding it hard, rather than pretending to be OK, but that success is about showing up anyway. It’s about the fact that some people will find this bringing of self about sharing of weakness and use it as a route to criticise, not everyone will like or even ‘get’ what you bring to the table. It is also about knowing that you don’t have to like or be liked to work with others, but that it is instead about developing shared goals, and that diversity of thought makes us stronger and not weaker. Finally, it’s about knowing that it can be scary to share who you truly are as the comments and the insults hit harder without having an armoured shell in the way. However, if you don’t show that you can bring your whole self to a space others will feel less able to do so. Creating safe spaces where people can truly be themselves is one of the greatest things we can do, and so we need to model the way forward so that others don’t have to take that risk instead of us.
Of all the posts I was most scared to share when I wrote it in April 2021 was the one where I talked about losing my sister and how it felt to know that I wouldn’t be able to have children on top of losing her. It was one of the first really personal and vulnerable posts that I put out and I was really scared of what the response might be, both from family and from strangers. Instead, it was shared more times than any other post, and people still come up and talk to me about it, my sister, and Morgan my niece, who we also lost. Something that terrified me, led me to being able to talk about something that impacts so many and is talked about so little. Sharing, was a bravery I don’t think I would have managed in any other way than on this blog, and having conversations with people who read it are so meaningful to me, even now.
More recently I shared a post about what it feels like now, over 10 years since losing my sister. I really wanted to post how something that feels so insurmountable, in terms of not having children when you wanted them, can actually turn into something where your life still has so much meaning and joy. A position I could not have even imagined in 2010 when I lost them. I truly, honestly, love my life. My life has meaning and I have achieved things that I’ve been forced to admit would not have been possible if my life had taken a different course. I hope that sharing this can help others who are not there yet to know that there is a future where they will smile, laugh and feel valued again, no matter how dark the moment feels.
I’ve always been a family girl, but I’ve not always prioritised them in the way that I should. I’ve missed funerals and weddings for work. I’ve cancelled dinners and missed trains home. The pandemic, and life in general, has made me decide that I need to put my family first, and thus myself. There needs to be balance to make it through the marathon of a healthcare career, and some of that balance requires that the job cannot always be the thing that defines who we are. Mummy and Mr Girlymicro are my world, and every moment spent with them makes me a better person and thus better at my job. Bringing my whole self to my job and my leadership requires me to nurture precisely that, my whole self. So credit where credit is due. My family support me in being able to do what I do. They make me martinis when I’ve had a bad day, give me water when I’ve forgotten to drink, and feed me when I’ve inevitably forgotten to eat. They love me for my flaws as well as my strengths, and put me back together when I break. They are my everything, and so they need to feel like my priority in life. I guess my learning is this, don’t become so focused that you forget to acknowledge the people that got you there, and don’t be so ‘eyes on the prize’ that you forget to enjoy the journey with those who care.
Last, but by no means least. I have learnt to embrace the unexpected. I’m a planner but when I started posting on this blog I didn’t really have a plan. I had no idea where I was going or what I was doing. I just knew that it felt like it was something that was needed and had been asked for as part of a challenging time when people were looking for information. It was something that was supposed to be a little hobby that unexpectedly became a central rhythm of my life. Something that is a focus of a little time every day. Something that feels mine when less and less of my working life feels that way. It’s a space where I really feel I can connect, in a way that is probably a little insane for something I throw onto a page and don’t see people read. None of this was planned, and yet it has changed my world. It has changed my plans for the future. It has given me a creative outlet, and some hope in pretty dark times. So, if I have a thought at all for you to take from this overly long blog post, it is this. Embrace the random moments that come your way. Embrace the actions that you roll a dice on and don’t think will lead you anywhere, because every once in a while, without you even being aware of the whys or the how, they may change your life for the better.
This weekend I’m off to Torquay for the Agatha Christie Spring Literary Festival. It will involve talks, a statue unveiling and even a ball! Some of you will know that I’m a massive Agatha Christie fan and love a good murder mystery. It’s part of the reason my ambition for when I retire is to finally have time to write some of the pathology murder mysteries that I have drafted out. I’m planning a three book series called The Murder Manuals. Anyway, that’s some way off but I still love to indulge in a bit of Agatha joy.
Whilst thinking about it this weekend, when I should have really been packing instead, it occurred to me that maybe one of the reasons that I love my job so much is because, in many ways, working in Infection Prevention and Control (IPC) is like working to solve real life mysteries and challenges on a daily basis. You come into work every day not really knowing what the future will hold and spend your days trying to uncover who the criminals (microorganisms) are and how to prevent future ‘crimes’, in the form of infections. This feels even more true having recently posted about how a forensic science lecture I went to looked at solving crimes. So, whilst my head is all linked to the detective process (I suspect I’m more Miss Marple than Hercule Poirot, although really I’d love Mr Girlymicro and I to be Tommy and Tuppence) I thought I would write about why I believe IPC professionals make the best healthcare detectives.
Beginning at the end
Like most good crime dramas, we in IPC, often make our entrance towards the end of a story when we things have already happened. We then have to work backwards to understand what’s happened as well as working forward to prevent any future risk (‘crimes’). Now, the point we get involved can range a bit. Just like in detective dramas, if the crime is obvious the police get involved early. Sometimes however, Miss Marple suspects a crime has occurred (think Sleeping Murder) but everyone else can be slow to get onboard.
In the world of IPC sometimes there are very clear events that need to be looked into. An outbreak for instance is traditionally described as 2 cases linked in person, place and time, or a single case of a significant infection, such as Ebola. This works pretty well most of the time but there are circumstances where using this definition can mean it takes you longer to identify an outbreak, or ‘crime’, has occurred. An example of this is when outbreaks are linked to an intermediate environmental source. This means that you may have low level numbers of cases which don’t appear to be linked in time, or even person, but are just linked to location. I’ve written about the importance of environmental IPC before, but this is one of the reasons it can be particularly tricky.
Need to understand the rules
In every detective story there are rules. If you’re in a Christie novel there will be a denouement, if you’re watching Columbo you will always see the murder at the start, and if the murderer is a female she will always be the person Morse tries to flirt with badly at least once. Infection Prevention and Control is no different. There are unwritten rules that you need to learn and which will help guide you on your way. Vancomycin Resistant Enterococci outbreaks will often have an environmental component. Norovirus outbreaks within staff often have a secret staff member who vomited in the toilet and told nobody. Pseudomonas aeruginosa outbreaks make people ask ‘have you checked your water?’ All of these things give you a way to start investigating and a set of questions to begin with.
Now, here comes the word of warning. Just like The Murder of Roger Ackroyd broke the rules, so do bacteria and other outbreak causes not always behave the way they are supposed to. Just like any good police drama with a rebellious detective, you need to know the rules but also know when to ignore them. Know when to switch tack and think that your MRSA outbreak may actually be linked to your ventilation system, not direct hand to patient transmission. Be neutral enough when looking at your data to not ignore the clues that are there. Red herrings will be present and distract you, so know when to call a fish a fish.
Start broad and narrow down
One of the best ways, with any investigation, is to start broad and narrow down. This enables you to avoid diving down rabbit holes and missing other pathways that should be investigated. Very rarely can you turn up to a country house murder and exclude most of those present, and as Hercule Poirot famously states “it is always wise to suspect everybody”, and the same is true with IPC investigations.
Ask yourself, why do I think that there’s something happening? How do I know that cases occurring at the same time are actually linked? How are my surveillance systems set up to support identification of low levels of cases over prolonged periods? How sure am I then that a ‘crime’ has actually been committed? Once the body as been found, in terms of looking for sources, where do I get my information from? Do I consider just other patients, or patients and families, or patients, families and the environment, or even patients, families, environment and staff. This, all before you even start to consider how different organisms behave in different types of patients. In a country house murder you need to consider those above stairs as well as those below, and in stories like the A.B.C. Murders, you even need to consider those who came and rang your doorbell.
There are so many moving parts within healthcare and we need to ensure that we are capturing as much of that landscape as possible when we start our investigations. Starting broad supports this, but you also then need to know the key moments to start excluding options so that you can eventually get to the depth needed to support interventions and change. Eventually you have to have the scene where you commit and name the murderer. Within IPC, events such as outbreak meetings can really help with this, as unlike our favourite detectives, we can’t keep all the information to ourselves right to the very end. These meetings bring people together to both help gathering information but also to decide on how to focus next steps.
A plethora of unreliable witnesses
In A Murder is AnnouncedMiss Marple states, ‘Please don’t be too prejudiced against the poor thing because she’s a liar. I do really believe that, like so many liars, there is a real substratum of truth behind her lies’. One of the things that is often quite difficult to pin down during IPC investigations is….what is the truth? Truth is often seen as definitive but in reality truth relates back to the lens through which the individual sees the world. For instance, if you asked me what I was doing at 7am last Wednesday I wouldn’t lie, but I would have to offer some form supposition as I can’t actually remember precisely. The other complication is that those directly involved may be even less able to recall their own roles. If I’m sick in hospital days can merge into one and I’m focussed on my physical reality rather than taking in my environment. This is all before we take into consideration the fact that we may be providing sedatives and other medications that could impact recall. Would I remember that one of my visitors mentioned my niece had diarrhoea……..probably not.
Within IPC investigations no one is likely to remember every physical action, which is why audit can be a helpful addition, in order to have an external person capture trends. In other scenarios the actual witnesses to the event can’t speak, for instance ventilation gauges that may have fluctuated or alarmed (is that a voice?) to an event that no one wrote down or reported. This is especially challenging when you are trying to get to the bottom of grumbling outbreaks that have been going for some time, but also is a particular challenge linked to infections with organisms that may not become apparent for months, such as some surgical site infections or infections with pathogens like Aspergillus. Memory can make individuals particularly poor witnesses in these scenarios and good record keeping and notes are essential to support look back investigations (investigations where you are looking back to capture risks and event detail).
Need to know which tools to use
If you only interview half of the witnesses in your case, you’ll be lucky to get even half of the story, as it will all depend on which people hold the information. On some occasions you will luck onto all the answers with the first witness, but is this a risk you want to take? The same can be true in IPC investigations if you don’t think about the tools or sampling methods you want to access from your toolkit. Is your main focus on using bacterial culture? Do you have a method that will work even if the patient is on antibiotics? If you are looking for a viral cause, what method is best? PCR is not PCR is not PCR. You can look for RNA, or DNA, you can extract from different volumes and different types of samples. The pros and cons of all of which need to be considered. Putting together a sampling strategy in response to an investigation is like choosing the pieces of a jigsaw puzzle whilst knowing that you are not going to have all of the bits. You want to choose pieces that give you the best chance of accurately guessing what the picture is.
In IPC there are various pieces of documentation that will help with thinking in this area. Documents like the UK Standards for Microbiology Investigations (UK SMIs) can help guide thinking linked to which samples might be useful to take. UKHSA also has various documentation linked to outbreak investigation with specific organisms and interpretation criteria, such as measles, C auris, and TB. At the end of the day however, just like your detective walking into a murder scene, you will need to work out how to apply that guidance to what you see in front of you.
It’s all about the clues
Once you have investigated and questioned your witnesses then you need to be able to work out from your clues which pieces are useful and which are your red herrings and may lead you astray. Like all investigations the most important thing is to be methodical but you then need to make time to be able to think and reflect. Poirot famously once solved a case without leaving his front room, just by being able to sit and question those involved. I’m not saying that this is something we should try in terms of IPC, but I do think it holds some lessons for us about the power of thinking time. Especially when you are in the midst of an outbreak there is often a real drive to be seen to be doing something, responding to everything, and constantly doing more. After 20 odd years in micro/IPC I think I’m beginning to think that Poirot may have been onto something.
If you are constantly changing or adding in responses it can be really difficult, even if you reach resolution, to know which thing you did made the difference. Early on in an outbreak it can be easy to rush into making recommendations prior to having gathered all the information you need. It sometimes feels good to call an exposure meeting the minute you get the information that an event has happened. For instance, you may have days to respond in the case of something like a chickenpox (incubation period 8 – 21 days), before those patients become a risk to anyone else. Therefore waiting to call a meeting until you have gathered all the clues, until you know everyone’s immune status, levels of exposure etc, can mean that your meeting is so much more effective in managing any risk. Waiting until you have a decent action plan for where you might search for clues, i.e. sample, may mean you find the answer so much more quickly then having to go in for multiple attempts. Taking a breath and putting thought before action may mean you get to the final result so much faster. So utilise those Little Grey Cells!
Not everyone takes kindly to be investigated
IPC should not be about blame, but just like the house guests in a country house murder may not take kindly to a visit from Inspector Japp, some occupants of your ward may be less than happy to see IPC walking up to the nurses station. Although I talk about the similarities between IPC and detectives, we should not be feared and act like police, or worse than that judiciary. Often the reason why Jessica Fletcher gets further faster in finding the murder than the police at the scene is because she is seen as just another friendly visitor rather than someone looking to find fault. Her focus is on building and utilising relationships in order to gather information. She is often seen by the other witnesses involved as being part of their team, and the outputs of her investigations are often linked to co-production of outcomes by sharing information, rather than going it alone.
In general, as in many areas of working life, relationship building is key. You see Jessica all the time in Cabot Cove, not just when there’s been a murder. That means that by the time she finds the body she already knows most of the players and has built up relationship capital with those involved. This enables her to sometimes ask the challenging questions. I believe the same needs to be true for IPC. If clinical teams only see us when things go wrong, they are automatically going to be somewhat defensive. If they see and work with us when times are going well, as well as less well, they are more likely to feel we’re in it together with shared ownership. All of which means we may also get to the source that much faster when we need to.
Sometimes there’s a twist in the tail
There are a number of famous Agatha Christie stories where the murder victim turns out to not actually be dead, I won’t spoil them here. The same can be true for IPC cases. There are certain organisms, of which Adenovirus is my personal favourite, that can both cause primary infection and then go latent and reactivate later. Often this reactivation is linked to immune status, and of course many patients in hospital have immune systems that are doing less well. These present challenges as you can look like you have a cluster of cases but, due to the type of patient, they can all be independent findings that happen to cluster together. So, without the right investigations you can call ‘murder’ when actually there is no corpse. Being happy to hold your hands up and step down when you have new information is an important trait, but knowing to get the testing done to enable you to do so is even more so.
The other scenario that can happen is, as Sherlock Holmes famously said, “When you have eliminated the impossible, whatever remains, however improbable, must be the truth“. There will be things that have been done, behaviour that has occured, that you would never imagine or predict. Over the years I’ve found a lizard in a bathtub, olive oil used as skin care by parents, and all kinds of things in fridges and freezers, just as the tip of this iceberg. Things that out in the real world would probably not be a risk, but in the healthcare world can lead to all kinds of issues, none of which would be on my primary list of questions when trying to identify a source. The world continues to surprise me, and therefore in the world of IPC keeping enough of an open mind to to respond to the unexpected is essential.
It’s a team sport
Poirot has Hastings. Morse has Lewis. Sherlock has Watson. Tuppence has Tommy, and Jessica has most of the population of Cabot Cove. Solving crimes benefits from teamwork and IPC is no different. I’ve spoken about the importance of relationship building but doing IPC investigations well benefits from more than even that. One of the key ways these partnerships work is by creating the space where the discussion and reflection we’ve already talked about can happen. In healthcare, which is far from a contained setting with only a handful of key players, being part of a team can also provide vastly more eyes and insight into what happens in reality.
The Hawthorne effect is a type of human behaviour reactivity in which individuals modify an aspect of their behaviour in response to their awareness of being observed
One of the reasons that it’s important to undertake a team response within IPC is that if I turn up, a stranger or less frequent visitor on the ward, then those on the unit may behave differently because I’m there. If you see IPC hanging around a sink, for instance, then you may suddenly focus way more on your hand hygiene efficacy then you would otherwise. If I go to speak to a family, they may say different things to me than they would to the bed space nurse they see everyday. In order to get the full picture I may not always be the right person to ask the questions. Being fully integrated, being seen as part of the team, or having relationships with people that are, can make all the difference in terms of the success of your activity. Everyone benefits from having a Hastings to send in to ask questions from time to time.
No greater satisfaction than being part of the denouement
I don’t know about you but I just love the moment that everyone gathers at the end of a Christie novel and detective starts the process of walking everyone through all of the different clues, red herrings, and witness statements. The moment when you discover if you’ve picked up on everything that was on offer to you, and even more than that, the anticipating of waiting to hear if you’ve put it all together in a way that a) works and was b) actually correct.
I feel the same way when I finally have that moment when I crack the case, when I find the source, or even just get to the point where I understand a tricky result. The hallelujah moment when you look down at the jigsaw pieces you have and you can finally see the full picture. It’s the reason that some of our favourite investigative successes live on for years in teaching and case studies. I will talk about the case of the Norovirus and Biscuit Tin to anyone who will listen even now. The settings may be different but every detective, whether in a novel or in healthcare, loves to regale others with their exploits. We just can’t help ourselves. My excuse is that sharing the learning helps is all. That said I’m off to attend a talk called ‘How to kill people for profit’. I’m assuming it will give me all the tips I need to be the next cozy murder success and maybe even weave in the odd IPC detective drama moment into the mix.
This post was supposed to be something quite different. It was supposed to be about One Heath and a great podcast created by Beckman Coulter I was involved with in 2024, alongside some really inspiring people. In some ways it still is that, but because of the cruel reality of life it is actually also something quite different.
”Going Macro on Micro” is a podcast that Dr Simon Doherty and I were involved with that explores emerging themes and pressing issues in the world of microbiology. As the host, Dr Lough, says the podcast covers everything from investigating the global challenges of infection control to unveiling the future of diagnostic technologies.
The week the final episode of the podcast dropped, before Christmas, I got some pretty devastating news. Sadly Simon has passed away. Now, I didn’t know Simon well. We’d emailed since doing the podcase together and I kept an eye on the awards he received and his really interesting posts. In this limited contact though, he still managed to inspire. Recording the series with him was such a privilege. He was kind, open and funny. More than that he was so knowledgeable and I came away feeling like I’d learnt so much. I am so sad that I won’t be able to build on the foundation we laid to continue to learn from him and talk about the challenges/opportunities that face us in the fascinating world we both inhabited. I thought about not sharing these episodes when I heard the news, but then decided that I don’t want you to lose out on the honour I had of learning from him direct. I hope that you will hear both his wisdom and his challenge, and also aspire to do better, as I do, as a result. Thank you Simon.
I’ve decided to keep the focus on Simon and just put some graphics and links here that might supporting learning more about antimicrobial resistance and One Health. At some point when the loss of Simon has had a little more time to be processed I will think about writing something in a little more depth reflecting on his comments and the overlap between human health and veterinary medicine. Until then, the links to the episodes are below:
Ahmad Nayeem , Joji Ronni Mol , Shahid Mohammad. (2023). Evolution and implementation of One Health to control the dissemination of antibiotic-resistant bacteria and resistance genes: A review. Frontiers in Cellular and Infection Microbiology
Episode One
Rhouma, M., Soufi, L., Cenatus, S., Archambault, M., & Butaye, P. (2022). Current Insights Regarding the Role of Farm Animals in the Spread of Antimicrobial Resistance from a One Health Perspective. Veterinary Sciences, 9(9), 480. https://doi.org/10.3390/vetsci9090480
Episode Two
Sanseverino, Isabella & Navarro, Anna & Loos, Robert & Marinov, Dimitar & Lettieri, Teresa. (2018). State of the Art on the Contribution of Water to Antimicrobial Resistance. 10.2760/771124
Episode Three
Sanseverino, Isabella & Navarro, Anna & Loos, Robert & Marinov, Dimitar & Lettieri, Teresa. (2018). State of the Art on the Contribution of Water to Antimicrobial Resistance. 10.2760/771124
Episode Four
Sanseverino, Isabella & Navarro, Anna & Loos, Robert & Marinov, Dimitar & Lettieri, Teresa. (2018). State of the Art on the Contribution of Water to Antimicrobial Resistance. 10.2760/771124
Episode Five
Sanseverino, Isabella & Navarro, Anna & Loos, Robert & Marinov, Dimitar & Lettieri, Teresa. (2018). State of the Art on the Contribution of Water to Antimicrobial Resistance. 10.2760/771124
Episode Six
Sanseverino, Isabella & Navarro, Anna & Loos, Robert & Marinov, Dimitar & Lettieri, Teresa. (2018). State of the Art on the Contribution of Water to Antimicrobial Resistance. 10.2760/771124
The World Health Organisation (WHO) talks about it like this:
Antimicrobial Resistance (AMR) occurs when bacteria, viruses, fungi and parasites no longer respond to antimicrobial medicines. As a result of drug resistance, antibiotics and other antimicrobial medicines become ineffective and infections become difficult or impossible to treat, increasing the risk of disease spread, severe illness, disability and death.
I think it’s easy to forget that although AMR is a big part of the professional life of most Infection Control and microbiology professionals, even for other healthcare professionals it features less often, let alone for members of the public. It can be surprising therefore when you do go out and about, or even just talk to friends and family, to hear some of the ways that non infection professionals think about how AMR works and who it impacts.
Common misconceptions I hear when talking to people about AMR:
It’s the body that becomes resistant to antibiotics
I have never taken antibiotics so I cannot get a resistant infection
Antibiotics treat all types of infection
Antibiotics can be stopped when the symptoms stop
Only infected patients can transmit antimicrobial resistance
If you reflect on some of these myths, it’s actually pretty easy to understand how they come about. Most people are focused on themselves and act from a human centric point of view. Many people give little, if any, thought to the multitudes of living bacteria that co-exist in their bodies. Once you accept this as the starting point, most of these myths are actually based on pretty small mental leaps. If, however, you don’t switch your point of view before you start having conversations about AMR, you can unwittingly end up reinforcing the very misconceptions you were aiming to address.
One of the reasons that I think this post is timely right now, is that I am already seeing more posts linked to how we should not be putting artificial medications into our bodies, alongside the back lash against vaccines, and so it seems to me a good time to remember what a difference these, now common, medical interventions have made to the lives of individuals and public health in general.
Let’s start with a little bit of context
Hardly any of us will have living memory of life without access to antibiotics and what life was like in a world without vaccination. One way to really get a feel for the impact these common interventions have made is to look at the impact in the last 30 years on reducing child mortality (death). Even in this recent time period, massive progress has been made due to advances such as the rota virus vaccine, but also in getting more global access to antimicrobial therapy where it is most needed.
Public health is multi factorial, with impacts being cumulative and made by more than just one thing, so not all of these impacts are made by antibiotic and vaccine availability. Other steps to reduce death linked to infectious disease include everything from clean water and sewer systems to pasteurisation and other means of food safety controls. The impact of these combined approaches is massive, but as the UN sustainable development goals show us, those of us who are access to clean water are not actually in the majority and more is yet to be done to ensure equality of access.
To aim to undo some if not all of this century plus of progress is something I find pretty hard to process. If you’ll forgive the momentary indulgence, I have to state that I think the current anti-vaccine and general anti medical stance that is being seen within some groups and communities is ultimately an act of extreme privilege It’s a privilege to be able to choose not to access something that is readily available to you and not available to others. It is a privilege not to have to live first hand the consequences of what the alternative might hold. It’s also a privilege to be able to change your mind and choose to access something later. Thinking of things in this light doesn’t necessarily help with having conversations in a supportive and open way when some of the underlying thinking may be so different, but it may mean we can flip the dialogue from one of imposition to one about the power of choice, and supporting evidenced based decision making for all.
Where does AMR come into this?
There’s a big stat that everyone quotes about more people dying from AMR than cancer by 2050, with an estimated 10 million deaths. As a scientist, I get the need to quantify and use numbers, as a human being however, I find that numbers that are so big can just be off-putting. They are so large it can make us, as individuals, feel powerless to impact them.
For me, the reason this conversation is so important to have in the right way, and pitched to the right communities, is because if we are going through a period of global push back against the common interventions, such as vaccination, that have successfully reduced mortality and provided first line protection, then our final line of defence in terms of treatment is now even more vital. 2050 isn’t that far away, and we are already seeing consequences linked to more resistant organisms being identified in severe infections. Therefore, the time to be having conversations and really raising awareness to impact decision-making is now. Sadly, this is coinciding with a period of time when trust in healthcare professionals and science in general feels very low. Instead of being defeated by this, however, we need to use it a driver to really focus on how we can do it better.
One of the other reasons that AMR is both important and challenging to communicate is that it is always in constant flux. You can’t just learn about it and move on. The mechanisms change, the diagnostics change, and the interplay of all of these factors within the bacterial host interactions can make it even more complex and hard to engage with. To exemplify this, the figure below was something I saw posted on Bluesky and fell in love with, as I adore the fact that it lists all kinds of routes to AMR in a single image, thus capturing the complexity of what we’re dealing with.
That said, you don’t have to understand all or any of this image to understand the core of why AMR is going to be a problem moving forward. The main thing to take away from it is that AMR is complicated, and as a result you will hear many different messages linked to it, and those messages will continue to change as we learn more and the impacts are felt differently. As a result, it can then sound like we don’t know what we’re doing, or just end up really off putting, as there isn’t one clear message we are getting out there for people to cling onto. We, therefore, need to build this flexibility into messages and link around core themes rather than trying to talk in absolutes. Otherwise, we risk losing more of the public confidence than has already occurred.
What is being done nationally?
This year, a new version of the UKs National Action Plan for confronting AMR has been released and within it there is a strong focus on the acknowledged need to educate both members of the public and healthcare professionals on AMR.
There is also plenty in there about increasing equitable access to antimicrobials, the need to improve diagnostics to help support both diagnostic and antimicrobial stewardship, and something that pleased me greatly, a special mention of the role of the built environment in managing AMR.
The thing is, top-down approaches will only ever get us so far. At some point, those of us involved in all things infection also need to be consciously including some of these drivers in our own every day practice.
No one can do everything, but whether you are collaborating with industry, undertaking research, or working in clinical practice, we have to embed AMR based action into our encounters. Do you include an AMR slide into all of your teaching? No matter the audience? Do you take the moment when it comes up with friends and family to just talk about the fact that this issue exists? Can you free up some capacity and undertake some public engagement?
Recognising there is a need is not the same thing as addressing that need, and we also have to be there to hold strategic partners and organisations to account in order to make sure action happens. So, let’s consciously match that top-down approach with a bottom-up drive for change.
What resources are there to help talk about AMR to other professionals
Having talked a lot about the need to talk to other healthcare professionals and seeing so much about #WAAW this year, it does really feel progress is being made to support us all to do this better.
Those of you who are UK based have probably heard of and support the Antibiotic Guardian programme (https://antibioticguardian.com/). This programme has lots of resources and supports personal action by asking you make a specific pledge about what you will undertake linked to addressing AMR.
Every year, new infographics come out that talk about different aspects of AMR. Some of these, like the one above, link AMR into commonly known components of healthcare practice, such as hand hygiene, in order to support individuals to feel empowered to act. Others focus more on messaging about antibiotic courses, or as we heard a lot about at the FIS/HIS conference last week, things like IV to oral switches, and sending the right samples to enable a switch from broad to narrow spectrum antibiotics. There’s plenty of ones out there now that can be really useful to embed in talks or laminate and put up on walls. The UKHSA especially have recently released a lot for WAAW, and because there are so many, you can keep them on rotation so that they don’t just become invisible as people see them too frequently.
I’ve also been involved in creating various content this year, as have many others, including webinars and podcasts to explore some of the issues linked to AMR and provide different routes via which healthcare professionals can engage with information and CPD on this topic. I’ve included a link to just one of these below in case it’s of interest, but a quick internet search will provide you with all kinds of others.
The main thing to remember is that we all like to receive our learning in different ways, and so ensuring that we remember that when we’re designing our education strategies is one of the best ways to be impactful.
What resources are there to help talk about AMR to members of the public
The resources you might want to use linked to AMR will vary greatly based on your target audience. It’s important to remember that even if someone is a healthcare worker they are also a member of the public, and depending on their personal background or setting they work in, utilising content created for the general public may serve both purposes.
There is some really great video, podcast, infographic, blog, and other content aimed at public outreach on AMR. There’s even a musical called The Mold that Changed the World, about Fleming and Penicillin, as the first antibiotic.
There are lots of different entry points when you are thinking about content that might be appropriate, and you’re likely to go to different depths depending on whether you are doing a one off encounter or a more prolonged piece of relationship building.
The post that is linked to at the start of this article on AMR as a Super Wicked Problem may help with choosing your content. You may also want to consciously address some of the myths mentioned at the start or even start your conversation with the fact that many antibiotics actually started as products identified in nature, and so are not as far from natural compounds as may be frequently thought.
Some of you who have been reading this blog for a while will know how proud and passionate I am about The Nosocomial Project, which aims to use a science, technology, engineering, arts and mathematics (STEAM) approach to talk about infection and infection risks.
As part of this work, we organised a two part festival linked to AMR entitled Rise of the Resistance Festival. All of the content is split across YouTube and the website. I’ve included linked here in case any of it is useful in your own settings when you are looking for inspiration or planning content. The content covered in the festival included everything from a play aimed at pre-school aged children entitled Sock the Puppet, who is a hand puppet who is scared of germs, expert panels, comedy sets, and Klebsiella as a drag queen. I still have so much fun rediscovering this content, and I hope you’ll feel the same way.
I would make a plea that we all work together on this one to do some myth busting and get messages about AMR out there, but also find a way to get messages across that are entertaining/joyous and filled with hope for what we can achieve, rather than focusing on the horrors of what happens if we don’t get our act sorted. I think all of us, including healthcare professionals, have had our fill of trauma in the last few years. So, let’s focus on empowerment and positivity to make this change happen, rather than following in the footsteps of those who want a world of decisions driven by fear.
I’m off to the Federation of Infection Societies (FIS) conference this week. I’m involved in 3 sessions over 2 days, and in many ways, these types of events are a complete highlight for me. I get to be inspired by hearing new science, I get to catch up with wonderful colleagues who I don’t get time to see very often, and I get to immerse myself in all things microbiology without the distraction.
There is another side to this coin, however, and that is both the anxiety that builds before I go, and that can last throughout the whole event. The ever-present spirals of ‘do I know anything?’, ‘will I say something stupid?’, ‘will I know anyone?’, and the classic ‘do any of these people actually like me?’.
The combination of this social anxiety with the, sometimes long, very peopley days, can mean that I hit spirals pretty easily and the lack of solo recovery time means that I can find it pretty exhausting by the end.
Now, I’m obviously not talking about extreme cases of social anxiety that may require informed medical or long-term support. I’m talking about situational anxiety that most of us may find ourselves in from time to time.
Just in case there is anyone out there in a similar boat, I thought I might put together some things I’ve learnt along the way that help manage some of my anxiety traits and enable me to actually enjoy the experience rather than dreading it.
Do your prep work ahead of time
The first thing I’ve had to learn is that I can’t just pretend that doesn’t happen. I can’t wish it away. What I can do is be prepared and make sure that I have made the process as trigger free as possible.
For me, this is about simple things, like getting a hotel as close to the venue as possible. It means that if I just need a 30-minute alone break, I can take one. It removes anxiety about getting lost or forgetting something crucial and not having time to go back for it, which, although minor, can be the final straw. It’s also about making sure that I have pre-found all the rooms I need to locate ahead of time, so I know where I’m going, and that ahead of multi-day meetings I have a plan for which sessions I’m going to before I even travel to the event.
Know your triggers
I know that I have a few things that really lead to anxiety, but perhaps more unique to me, is the fear that I was have an auto immune attack and won’t be with people who understand what is needed. I learnt early that the best way to cover this one off is that I very rarely travel alone, especially over seas. I often travel with my mum or one of a very small list of truly trusted people, who I know would understand how to get me help if required.
Something that is more likely to strike a cord with others, is that I am also the girl who has walked into conference rooms, spent 15 minutes and walked out, as I knew no one and was just overwhelmed. I’m not proud of these moments, but I think it’s important to acknowledge that they have occurred. Although, to be honest, when they’ve happened, I mostly felt invisible, so I doubt anyone noticed.
I have discovered that I need to know that the space is one where I feel welcome for me to perform at my best. This sense of welcome can be either intellectual, because of the topics covered, or because of feeling a sense of community, as the room contains people within my field or in strong alignment with my values. I’ve found the overwhelming feeling hits most strongly when I’ve been in very large political or strategic sessions, where I felt out of my comfort zone on both intellectual and community counts.
That said, I’m not too bad in the sessions themselves, I’m there to learn something new, and learning excites me even now. It’s the breaks that are my nemesis, especially when large groups all surge into a space at the same time, and the weight of expectation that you must now network lands. The seconds that feel like hours of desperately searching for faces you recognise and being forced to face the fact that yes, you really should go up and speak to that absolute stranger, as it’s the right thing to do. It’s these moments that can cause me to bolt for the nearest bathroom.
Carve out time for yourself
One of the key mechanisms I’ve identified to help with my triggers is that I make sure I have enough time to myself, be that eating food away from the venue so I feel more certain what it contains and less at risk, to making sure I have evenings to myself to process and unwind.
I usually come over as really social, and really into spending time with people, and I am both of those things. I also only have a limited amount of social battery, and so in order to maintain that extrovert part of myself I have to have recharge time. I love talking to people about this blog, I love hearing about and responding to other peoples work, but at a certain point I need to sit down with an audio book and a cup of tea in order to do it well. This means that when I go through the brochure ahead of time, and plan my sessions, I make sure that I have enough blocks of time to enable me to be my best self when I’m in the space with others. Sometimes all you need is a walk to a local coffee shop and back to give you the perspective you need.
The wonderful thing about having hit my 20th year as a Healthcare Scientist, is that I now also know quite a few people, some of whom I’ve known for well over a decade. This means that at most events, there are also people who I count not only as colleagues but as friends. People that I can just go and spend time with that doesn’t include social commitment. Those friends you have that you can just be in the same space without any demands being made. If I’m at an event where these people are also attending, then I know that I have someone I can just excuse myself to catch up with if I’m having a moment. It’s also the great thing about ensuring that you have a hotel room nearby. Your safe bolt hole is only minutes away.
Make an agreement with yourself about how much is enough
The fact that you have social anxiety does not provide a free pass to escape one of the fundamental purposes of attending conferences, networking. It’s key to your career, it’s key to your development, it needs to happen. The thing is that there are varying degrees of what networking can be, and before you’re in the space, you need to decide what level you are aiming for and will therefore achieve. For me, my deal is that I will, on each day, speak to one person I don’t know. I am not allowed to finish my day without this happening, but once I have had that one daily interaction, then any further moments are a bonus. Once that one challenging moment is over with the pressure is off, and then I almost always over achieve on my goal.
Be realistic about how much you can expect of yourself
The key thing I’ve learnt is that I have to realistic when I’m making that deal with myself and deciding on achievable targets. For me, there is not point is saying I will speak to five people I haven’t met before, as I’ll just be setting myself up for failure. You will also find that I rarely sign up for conference dinners, as I have over the years found that if I’m in a space with other people from 08:00 – 18:00 I will really struggle to then spend yet more time with other people, no matter how lovely or interesting those people are. All I will want at that point is room service, tea, and a movie in my room.
Everyone will have their own tolerances and lines. The important thing is to have enough self reflection to know what yours are. Otherwise, you just add guilt into the anxiety mix, which is not much fun for anyone.
Learn how to work a room using tools you are comfortable with
One of the other things that I’ve learnt about myself, is that although I get super anxious standing in a room trying to approach someone at the coffee table, I am much much more comfortable moving around the exhibitor stands. The guys at the exhibitor stands are motivated to speak to those who approach, and there are usually science based discussions that I am eager to have. This, for me, is a match made in heaven, as it breaks me into the speaking to people I don’t know in a very gentle way. If I’m lucky, I will also meet others when I’m wandering around, which will allow me to tick my ‘speak to one stranger box’ as exhibitors do not count on that front. The added bonus is that I also often manage to find cool new stuff I’m interested in or develop collaborations whilst this is happening, so it’s a no lose scenario for me.
The other thing that having worked for 20 years has given me is the opportunity to be asked to be involved with sessions. For this girl with social anxiety, this is actually a great thing, despite the fact that it sounds like it should be stressful. I’ve never minded public speaking in the same way as I worry about 1:1 interactions. When I speak, all I can do is put my best foot forward and hope that others will be interested in what I have to say. For the most part, if people don’t engage they will just leave and not give it another thought. On the positive side though, if people find what you say interesting enough to want to speak to you afterwards, this a great way to tick the ‘speak to one person you don’t know box’ and as they are approaching you all you have to do is respond. I find this so rewarding, but I also appreciate how fortunate I am to have this type of opportunity and how much it helps me manage to get the most out of events.
Prepare your exit strategy
One of the important things to bear in mind, and which I often forget, is that others do not necessarily feel the same way about social requirements. I struggle when people arrange evening meals at meetings when you’re already booked to spend a full day together. I understand the purpose, it’s lovely to build bonds and memories, and logistically it’s easier. I rarely, if ever, hit the end of the meeting day and wish to spend the few hours downtime I have with others, over reading in the bath however. There are frequently times I can’t opt out of these moments, but where I can, I will often have a pre planned reason to excuse myself. Often, this is work related, as I will always genuinely need to do some email catch up, and doing this after dinner means working till midnight. I don’t lie but I may pre-plan my rationale for not being available to support both my work load and my mental well being. I will never not pre-inform, as that is rude. People will have budgeted and made arrangements, so I will never last minute drop, but if the option arises I may flag unavailability at the planning stage.
Don’t succumb to expectations and pressure
People are amazing and much more welcoming than you expect. I’m always counting myself as so fortunate is be asked to unexpected drinks, meals and catch ups at conferences. I have learnt that I need to not get caught up in the moment and end up crossing the carefully curated boundaries I have put together, in order to ensure that I can last the social distance of the conference. I’m a planner for a reason and I don’t riff off the plan well. I also struggle with saying no. This means that there have been multiple times when I’ve said yes to that dinner, or those drinks, and have then suffered the consequences afterwards. Now, I work hard to keep to my boundaries so that I don’t make life harder for myself. This can be surprisingly difficult as all these invites are inclusive and well intended, I just have to remind myself to make the sensible choice to enjoy the entire event, rather than burning out after a single evening.
Know that this is an essential part of the job, so invest in coping strategies early in your career
The truth is that networking and attending these kinds of events is essential. They are a fundamental way of hearing the latest science and expanding your knowledge. They are also key for collaboration and building your networks, as well as dissemination of your work. No matter what anyone says, I have found that science fields tend not to be meritocracies, there’s plenty of ‘who you know’ involved, and the only way to address that is to get yourself out there. So you will need to learn how to navigate these settings, and the earlier in your career you manage that, the more rewards you will reap.
I’ve talked about some of my own pitfalls and things that I’ve implemented to help me, but you will have your own triggers, and each response will need to be customised to yoi and your needs. What is true for all of us is that you are not alone, and if you are in need of someone to speak to during the horror of a break, then I am always happy to be your person. This is what I look like and I will never turn you away.
Know that it gets easier
The longer you hang on in there, the easier it gets, honestly. I haven’t walked out on an event in a decade, although the toilet hiding is still a little more frequent 🤣
Pre manage your expectations of yourself and make sure they are reasonable
Book with a group or a friend if you can to take the edge of socialising with strangers
Join a social network, as you can use it to find like-minded people, and it can give you a virtual introduction rather than the cold approach
Similarly, join a society. Societies often have small meet-ups either before events or at meetings, and so you can make connections in a smaller, less intimidating space
Submit work. It’s much less intimidating if people come and speak to you rather than the other way around
Know it’s absolutely OK to need to tap out and have your own space, but make sure this is pre-planned so you don’t miss the reason you came to the event
Right, well, having talked about the need to be prepared. I haven’t even packed yet, so I’d better get on that. If any of you are Liverpool bound, make sure you come and say hi. I’m there Wednesday and Thursday.
All opinions in this blog are my own
If you would like more tips and advice linked to your PhD journey then the first every Girlymicrobiologist book is here to help!
This book goes beyond the typical academic handbook, acknowledging the unique challenges and triumphs faced by PhD students and offering relatable, real-world advice to help you:
Master the art of effective research and time management to stay organized and on track.
Build a supportive network of peers, mentors, and supervisors to overcome challenges and foster collaboration.
Maintain a healthy work-life balance by prioritizing self-care and avoiding burnout.
Embrace the unexpected and view setbacks as opportunities for growth and innovation.
Navigate the complexities of academia with confidence and build a strong professional network
This book starts at the very beginning, with why you might want to do a PhD, how you might decide what route to PhD is right for you, and what a successful application might look like.
It then takes you through your PhD journey, year by year, with tips about how to approach and succeed during significant moments, such as attending your first conference, or writing your first academic paper.
Finally, you will discover what other skills you need to develop during your PhD to give you the best route to success after your viva. All of this supported by links to activities on The Girlymicrobiologist blog, to help you with practical exercises in order to apply what you have learned.
It has not been a great week for science, with many of us being concerned about how the presence of a vaccine denier on the successful ticket to the white house will impact public health initiatives and the quality of science communication in general. I’ve been thinking a lot about how we got here and how, even more than previously, embedding good science into mediums that are routinely accessed by the majority, will be crucial in ensuring the reach of accurate science communication when some of the more standard public health routes are bound to suffer in the coming years.
I think it will be a surprise to none of you that I am a bit of a lover of TV and movies, we’ve also covered a number of book reviews linked to this blog, and I like nothing better than snuggling down with a good book and a cup of Darjeeling. What does any of this have to do with anything? Infection, infection control, and science in general is a huge chunk of my every day, but this isn’t the case for everyone, or even most people. Many people are passive absorbers, meaning that they may not search out information but take on board when they encounter it when going about their lives. This means that the quality of what they encounter may be hugely variable, depending on how and where this happens. I’ve previously talked about the quality of the science in some of the books I enjoy, including the News Flesh series, as well as posting last week about how infection control is represented the Alien movies for Halloween. These are fun posts to do, but it made me think of the most popular movies that are linked to infection out there. How good is the science they represent? and by doing this better, could we support science literacy in general?
IMDB list of Top 25 Virus/Pandemic/Epidemic/Infection Movies
In order to think about this more detail I hit the Internet Movie Database (IMDB) which contains all kinds of lists, including a top 25 of Virus/Pandemic/Epidemic/Infection Movies (https://www.imdb.com/list/ls094715071/)
A Quiet Place (2018) (Girlymicro comment – I don’t know that this should count as it’s an alien invasion film)
Bird Box (2018) (Girlymicro comment – I don’t know that this should count as it’s an unknown enemy film that does not appear to be linked to infection)
Now, I have only seen 16/25 of these, Mr Girlymicro has seen 22/25, so between us we have most of these, so hopefully I’ll be to comment from a position of knowledge on a fair few of these. Before we even start however, as you can see from my commentary on this list, the poor science starts early during the classification of some of these as infection movies, even before we start to talk about the science content of the movie/show itself. Firstly, let’s look at the name of the list = Top 25 Virus/Pandemic/Epidemic/Infection Movies and how it related to the actual definition.
An increase, often sudden, in the number of cases of a disease above what is normally expected in a specific population and area.
An outbreak, which carries the same definition as an epidemic, but is often used for a more limited geographic area.
The CDC suggests epidemics occur when an agent and susceptible hosts are present in adequate numbers, and the agent can be effectively conveyed from a source to the susceptible hosts. Whereas a pandemic refers to an epidemic that has spread over several countries or continents, usually affecting a large number of people. The starting epidemic is usually due to a combination of factors including:
A recent increase in amount or virulence of the agent,
The recent introduction of the agent into a setting where it has not been before,
An enhanced mode of transmission so that more susceptible persons are exposed,
A change in the susceptibility of the host response to the agent, and/or
Factors that increase host exposure or involve introduction through new portals of entry
So you can see from the above that a number of movies on this list don’t actually count under the terms linked with to the title. Some of them are alien invasion, some of them are climate change related, and one is even on the topic of bioremediation. Yet there they are on the list.
For some of the others, I’ve already covered their concept during my Zombie post, so I’m not going to go through these in this blog, but focus instead on the ones that fulfill the epidemic based criteria. That said, give me a shout if you’d like a more in-depth zombie comparison post as Train to Busan is an awesome movie, and I’ll accept any excuse to re-watch it.
Let’s start at the very beginning
The first film on the list is Outbreak, a film that came out in 1995, with a description of ‘A team of Army doctors struggle to find a cure for the deadly Motaba virus that was transported from Africa to North America by a white-headed Capuchin monkey and is now spreading quickly throughout a small California town.’
This movie has an amazing cast, but I have to say I don’t want any of them in my team if it came to trying to lock down a high risk infection from an unknown source (vector). In terms of the escape monkey component. You’d think that it is far fetched, and if you’d asked me yesterday I would have said just that, but just today on BBC News there was a story on 43 escaped monkeys from a research lab in the US. So far fetched it may be, but not unheard of, in the case of vector escape.
Even if the vector component may not be quite as unlikely as I’d previously thought, I’d like to say that the rest of the practice in this is highly suspect at times. That said, I do have to admit, that I once went to a talk by a scientist who was looking for viral transmission sources of haemorrhagic fevers in Africa. They showed pictures of the table where they performed autopsies on found deceased animals in the jungle, under the same canopy as the table where they then sat down for dinner. So, as much as the way that high consequence infectious diseases (Ebola etc) are not portrayed as accurately as I’d like, maybe this is a movie of its time, as was that lecture. I really want to enjoy this movie, as it so defined how many of us had our first introduction to outbreaks and what they could mean, but almost 30 years on I don’t think I could recommend the scientific accuracy it portrays. The fact that this is still the top rated movie does not bode well for our scientific literacy hopes.
What a difference a decade makes
Almost 15 years after Outbreak, Contagion was released in 2011. This was the first of the infection movies on this list that I saw after I’d started working within Infection Prevention and Control. Contagion is described as ‘Healthcare professionals, government officials and everyday people find themselves in the midst of a pandemic as the CDC works to find a cure.’ I remember going to see this with a scientist friend and whooping out loud at the explanation of an R0, it gave me so much joy I was shushed by someone else in the cinema, to my ongoing shame.
The CDC defines an R0 as ‘The basic reproduction number (R 0), also called the basic reproduction ratio or rate or the basic reproductive rate, is an epidemiological metric used to describe the contagiousness or transmissibility of infectious agents.’ So, see if you share my joy at how the movie explains what this is, in a way that is so much more approachable than the CDC definition:
This film is not perfect, I clearly remember losing my mind about the glove use at one point, and SPOILER ALERT, it was that poor glove use that meant I was OK with one of the characters dying, but the underlying science is well explained and some of the approaches to containment and vaccination are definitely well routed in evidence. The differences in the quality of embedded science between Outbreak and Contagion are highly noticeable. Part of me wonders if some of the drivers for this heightened quality is linked to awareness of the topic due to the 2009 Swine Flu pandemic, or whether this was part of a wider shift towards improved factual grounding in these kinds of movies.
When talking to Mr Girlymicro about this movie, whilst writing this post, he has pointed out that despite my enjoyment he found it an act of ultimate depression which he will not be watching again, and that was when he watched it before the pandemic. It may therefore be, something that triggered my science joy may, in fact, be too depressing or triggering for other reasons to equate to true enjoyment for the general public. This may be an example of something that could risk being dis-engaging by being too close to the truth, despite being second on the IMDB list. Especially in a post pandemic world, this is a line that may prove difficult to walk and prove to be a barrier to movies and TV on this topic being commissioned in the short to medium term.
A completely different movie about primates
Still on viruses and re-visiting our primate theme from Outbreak comes Rise of the Planet of the Apes , which was also a 2011 release. It came out the same year as Contagion, and in the same discussion as Mr Girlymicro stated he would not re-watch that movie, for all the accuracy of it’s science, he would watch Rise repeatedly, and I can testify that in fact he has. Rise has the following description ‘A substance designed to help the brain repair itself gives advanced intelligence to a chimpanzee who leads an ape uprising.’ This is a really interesting addition to the category, as the pandemic aspects of it are mainly actually addressed in the closing credits which demonstrate how a pandemic can spread across the globe, with the film very much focused on the human (and primate) story behind the build up.
This film utilises a viral vector to try to address and revert brain abnormalities linked to Alzheimer’s, with a scientist desperately trying to find a cure for his father, whilst undertaking clinical trials on primates. Now, the clinical trial aspects of this film could not be further from the reality, and any scientist caught undertaking clinical trials and then sneaking the medication to treat their father would at best be fired and at worst been imprisoned. Somehow, because of the focus on the relationships rather than the science, the bad science in this movie bothers me significantly less than that represented in Outbreak, possibly because it feels deliberately portrayed as more like science fiction than science fact. There are some aspects of science to this one that I find interesting and like. The idea of a vaccine or medication behaving differently across species barriers is something that is interesting and could be deeply seated in evidence based plot-lines. I am aware, in this age of post truth and vaccine denial, having a film that focuses on how a vaccine or treatment could end life as we know it may not play into the goals I’m wishing to achieve using popular culture.
Let’s not forget about fungi
In recent years there’s been a rise in the quality of TV and the amount of choice has exploded, especially on streaming and other services. The switch to being able to film big budget TV over shorter film equivalents has provided storytellers with the capacity to really explore bigger and more complex tales that may not have been possible in under 3 hours.
This is last and most recent entry onto the IMDB list and is also the only TV entrant. It is our first step away from the world of viruses, into the world of mycology and all things fungal. The Last of Us came out in 2023, although it’s based on a computer game that was released in 2013. The series is set ‘after a global pandemic destroys civilization, a hardened survivor takes charge of a 14-year-old girl who may be humanity’s last hope.’ This is therefore a great combination of the way different mediums impact popular culture. The plot asks big questions about how far you would go to get a cure for the world, how much is one persons life versus the possible saving of mankind. It’s a real homage to the power that vaccination could hold to impact the world, and how when one isn’t available how desperately people might act in the search for a cure. This is the only entry on the list that came about post pandemic, and I think it is because of that (despite being a parallel to the game) that really resonates on where that desperation comes from, and despite the current vaccine back lash, shows how different outcomes could be.
The very first scenes of the series are a flashback interview from before the pandemic where a scientist talks about what they think the next bit pandemic will be, and I have to say the whole scene brings me unacceptable levels of science joy.
Anyway, this one played so much into my particular ball park that I worked with Liv Gaskill at ID Transmission on a series of articles that talked about the science behind both the Last of Us computer game and the resulting TV series, which pretty closely followed the same plot. This four part series was a real joy to be involved with and so I’m hoping that you might enjoy them too:
I wonder if fungi will be increasingly represented in this genre a) due to the success of The Last of Us and b) as viruses feel a little too close to home these days and so the fungal world might feel like a safer sand box to play around in. This could provide a safe way to have accurate science portrayal, alongside entertainment, as the real prospect of a fungal pandemic is thankfully pretty small.
A shocking oversight
We’ve reached the end of the list, but not the end of the blog post as I want to address an appalling over sight on the IMDB list, and that is the omission of The Strain on the list. This is also a TV series, where season 1 was released in 2014, covered a series of 3 books, and ran for 4 seasons. The series is described as ‘A mysterious viral outbreak with hallmarks of an ancient and evil strain of vampirism ravages the city of New York.’
The strain – episode one, season one
There are many reasons why I love this series (and at some point I should do a vampirism and infection blog to include things like Ultraviolet) is that some of the main characters are epidemiologists linked to the CDC and so some of the science exposition as part of the job based discussions is very pleasing. The other reason I like this series is there is a definite bait and switch, in terms of the causative agent, with all the initial dialogue being linked to your standard viral outbreak, with a gradual reveal that the culprit is actually a parasite. This adds a layer of interest as the approaches to dealing with transmission really start to reflect this, and provide an interesting change as the characters are also forced to pivot and discuss the differences. So, the use of a non-viral infection is not as unique as some of the coverage of The Last of Us may imply. That said, the general science outside of the epidemiology in this definitely becomes more to serve the horror plot than feasibility as time progresses.
Where are the bacteria?
You’ve survived ~3000 words of outbreak talk, covering viruses, fungi and even parasites. You may however be struck by the lack of bacterial cause in any of these listings. I’ve been thinking about this whilst I’ve been writing this blog and I’ve come up with a few thoughts as to why this might be the case:
Too close to home – many people have experienced bacterial infections themselves in their loved ones, sometimes with tragic consequences. It may be hard to therefore suspend belief enough to enjoy the offering. I wonder if this will be true to an extent for viruses now, or whether popular culture will be a safe way to explore collective trauma linked to the pandemic
Too slow – one of the features of many of the scenarios in these movies and shows is that the impact to fast and significant. This an important aspect of making events have real risk and in raising tensions. If accurately portrayed bacterial infections may be too slow in their impact OR the deterioration is so quick there is insufficient time for viewer engagement
Not dramatic enough – bacterial transmission (as described by R0) are not going to be as dramatic as their viral counterparts, so if you subscribe to ‘go big or go home’ this transmission route is probably not the one to drive a sprawling plot-line forward
Too commonly encountered – there are 101 medical shows which have bacterial infections and their consequences featured and so they may be too close to a different genre
The science is pretty hard to get right – as people are more familiar with the topic the less story flexibility there is and the greater the need to not be too jarring for those you are trying to engage. At least in the UK, many people will have been taught about Typhoid Mary and the John Snow Cholera outbreak, and so may have some familiarity. It may also be that these also make people think of the past, and this is not the feel many of these properties are trying to evoke.
So maybe bacteria are a harder sell, although I’d be intrigued to throw a little antibiotic resistance into the mix, or some bacterial toxin related drama and then see what cool things could be done as a result. Maybe that might be my future project 🙂 Let me know if you think that there is a bacterial based film/series that I’ve missed.
It’s Halloween weekend, and in previous years I’ve talked about all things Zombie and infection transmission. This year, though, I thought we talked about something a little different, infection control precautions through the lens of the Alien movie series. Most importantly, I’m going to talk about those initial interactions with the unknown that we frequently see in both these movies and in infection prevention and control (IPC), and whether we too would open the door when someone presents at the air lock?
Spoiler warning! This post is going to mention things that happen in various Alien movies. If you haven’t seen them it may, therefore, contain spoilers – the best way to deal with this oversight in your viewing (if you are concerned) is to just get out there and watch them as Alien is the same age as me 😁
This post was inspired by watching Alien Romulus again this weekend, which, if you haven’t seen it is the best Alien movie in forever.
In preparation for the cinema release I also did a re-watch of a number of the movies in the franchise. Just in case you are less familiar, and inspired to do the same, the list includes a variety of films in different sub-genres as listed below:
Whilst watching these I was struck by a number of moments that made me think about behaviours during the pandemic, but also tales of heard of some activities that occurred during the response to the Ebola pandemic and other high risk clinical settings. Not all of these moments would have been massively out of place, in terms of parallels with these films, and demonstrate that both risk assessment and clarity of thinking can be impacted and lead to responses outside of what would be normally expected.
The thing to remember is that there are usually protocols for just about everything, so most of the decision-making should occur and have been thought out long before the situation ever arises. The problems are almost always linked to human factors in the way we respond to stress and unexpected situations, and when the protocols appear to go out the window. So, just like every character and every space ship in the Alien franchise has a protocol for how to behave when they encounter new life, strange situations or sick crew members, every healthcare facility also has protocols to help deal with illnesses we see less often or that get issued when new diseases are encountered. Healthcare facilities may not have air locks, but they do have labs and isolation facilities, so the parallels may be more present than you’d imagine.
Infection is not always obvious
One of the first themes that recurs throughout all the movies is that infection is not always obvious, either to those on the other side of the air lock, or to the individuals outside waiting to come in. Infection with the parasite sometimes occurs when the stars of our show are unconscious, be that due to trauma or medical interventions, and so they are unaware of the Facehugger on character action that has occurred.
In terms of IPC the same if frequently true, both for viruses and bacteria. Some viruses have what is known as a pre-symptomatic phase, where you are infectious to others before you even know you are sick. This was a big problem in the early stages of the SARS CoV2 pandemic. Even for bacteria, when we talk about antibiotic resistant bacteria, most people are colonised and have the potential to act as silent sources without even knowing it, with only small numbers going on to develop infections.
The truth is not always apparent
Even when an individual knows that something has happened, and are aware of their close encounter with Alien kind, the truth of their scenario may still not be apparent to either them or to others. If you look at the Facehugger situation, surely once the terrifying creature has dropped off without apparent poor consequences, then everyone breaths a sign of relief and is grateful for the near miss, not knowing that this is only the beginning. When you combine this with the fact that some people will determine this to be a low risk event and therefore not want to disclose, as they are aware of the inconvenience that will result, you end up in situations where not all the information is available.
This can also be true in real life clinical situations. Patients may not know they have been exposed. Patients may also present with symptoms that they haven’t recognised as significant, or that they have risk assessed themselves and decided they aren’t concerned about and so don’t disclose. This can happen more easily they you think, especially at the start of something, where patients don’t feel particularly unwell, or they just have a couple of vesicles/small rash. In the latter stages, when patients are presenting because they feel unwell, they may be confused or not always able to accurately disclose what’s happened. Occasionally, this may be a deliberate attempt to withhold personal details, but most often it’s because they are rightly focussed on how they are feeling in the moment. Plus, if you asked me to accurately recall everyone I met and everything I ate a week ago, I’m not sure I could, even when well.
By the time you realise the condition is a threat it may already be a risk/out of control
One of the consistent themes across all of the movies is that situations get out of control before anyone truly understands the situation and the risks. It’s only when the person that you breached protocol for suddenly starts to writhe and the horror stands before you in all its glory do you truly understand the implications of the decisions you’ve made. At that point you are trapped in your glass med bay with a growing Alien and your self recriminations are not going to save your life.
This one is a rather more dramatic version of some of the conversations that happen amongst healthcare workers when you phone to give results and have conversations about whether patients had been in the right precautions and the staff member was wearing the right personal protective equipment (PPE). There have definitely been times when staff have made a risk assessment and not followed the protocols about what PPE to wear and have then responded to these phone calls with ‘what can you do?’ in relation to the exposure. Sadly, in some cases there is nothing that can be done once the guidance has been bypassed but to wait and see, which is the reason for the guidance in the first place. Fortunately, for most scenario’s in the real world, the consequence isn’t bloody horror, death and an alien threat to mankind.
Risk assessment is linked to risk management
One of the reasons that protocols are in place in the Alien movies is that someone, somewhere, has obviously recognised the risk of infection in a small contained community where everyone interacts and lives on top of each other. Even in Aliens, when you’re talking about somewhere the size of a colony, this principle stands. This is because you are unlikely to be able to access a clinical trial on a mining ship, or develop a novel antiviral on terraforming mission, even if what you’re importing is a more traditional style of infection, versus an Alien parasite. The extent of the risk mitigations needed will always align to the risk itself. If you are concerned about an introducing something that is untreatable, then your measures are going to be much more extreme than if your infection is likely to just mean someone goes to bed and takes paracetamol for a weekend. If you can’t treat, then prevention is your only option. After 9 movies there doesn’t appear to be a Xenomorph (Alien) cure and so measures taken to prevent allowing one into your space need to match the risk they present.
This approach is definitely seen in response to infection in IPC. If you have a condition that spreads easily, rapidly and can be incapacitating for a period (i.e. norovirus) then you will use a different set of precautions to those that you use to manage something which may not be as transmittable but is untreatable or has life threatening consequences such as a haemorrhagic fever. Having conversations and being open with people about the risks of getting things wrong and ensuring that individuals understand why responses are different in different circumstances are a key requirement for people working in IPC, and something I think we should all endeavour to do better at. I think the days of asking people to blindly follow protocols should probably be behind us, as I think the Alien movies demonstrate that if people don’t get the why, they often ignore some of the core components based on external drivers
So, what lessons can we learn?
Beware of acting on incomplete information
Decisions are consistently made in these movies based on incomplete information, which leads them to underestimate both risk and consequences. A great example of this is the way people use information related to the black goo, especially in Alien Romulus, maybe don’t inject yourself with a substance that doesn’t have a proper name let alone a full data set for you to understand what it does. The other thing is that information is often treated as static, and so there is very little rapid inclusion of new info, rather than being mindful of an iterative response to new data, so help constantly inform and improve your risk assessment. It’s always worth being conscious of when is enough is enough when it comes to information and decision making.
Emotions get in the way of logic
During the movie Covenant, the entire crew is made up of couples. I get this in terms of colonisation, but in terms of good decision making, and in relation to risk this is just a one way route to bad outcomes. There’s a reason that in a certain Zombie series husbands have kept their zombie wives locked in basements rather than removing the risk to them and others. There’s a reason medical professionals should not manage their loved ones. Emotions interfere with logic, and there is no way under this setting you are managing to make decisions without your emotions getting in the way. It’s a reminder that if we become aware that we are in an emotive place, it may be the time to step away and take a deep breath, before making that judgement call or even tap out entirely and allow someone more removed to take our place.
The contrast between human emotional decision making and evidence based decision making, usually undertaken by the android cast, is beautifully explored during Romulus via Andys story arch and is one of the highlights for me in terms of enjoyment.
Science doesn’t change based on how much you wish the outcome to be different
One of the reasons that emotional involvement in decision making can be so challenging is that it can interfere with perspective and accurate interpretation of risk, thus impacting risk perception. Sadly the truth that wishing does not impact outcomes is hard to argue with, but it is human to try to persuade ourselves we have more control and ability to influence the outcome than we do. Under stress, our natural tendencies towards pessimism or optimism are definitely amplified. All of this means that when there is someone at the door banging and begging to be admitted, it is easy to persuade ourselves there is a) enough time to manage to open the door safely and b) the consequences of opening said door will not be as bad as we fear. Emotions don’t change outcomes but we are almost programmed to hope that they can.
An individual will always want to be the 1 in a million
The reason someone opens the door is the same reason that when one character looks at another and utters the fateful and true words ‘it’s too late’, and it almost definitely is, neither one acts before everything gets out of control. Humans are not good at dealing with numbers and risk when they are actively involved in the situation. One of the reasons we aren’t in that we throw sentences around saying it is a 1/million chance. We, as humans, have a tendency to focus the fact that, although it is a long shot, there is a chance that things can go your way. Sadly, as someone who has experienced the opposite, where my sister died in a 1/10,000 pregnancy, someone always need to be the one. The stats work both ways, whereas most of us survive in the world by only focussing on one side of the equation. This therefore impacts our capacity to evaluate any risk in situations we are involved with. Somebody always bears the cost and few of us can bear the vulnerability of acknowledging that that somebody could be us.
The people with the most experience are not always the ones making the decisions
One of the other main themes in these movies is that decisions, when not being made by friend and loved ones, are often being made by people in positions of power, not necessarily based on knowledge or even accepting of prior experience. This works well or not so well based on how well they listen to those who do have the information to help improve their decision making. Chains of command, especially in high stakes scenarios, are not necessarily bad, as we’ve already talked about the risks linked to emotional decision making, but so much depends on how well they work and how they place value on evidence based choices rather than hierarchy.
The other theme here is the trusting of unknown sources, especially ones with no evidence of expertise, over those who have either lived experience or expertise. I think this one resonates a lot right now, when there are so many sources of misinformation out there, and so many conspiracy theories that rely on speculation and rumour. Fact checking is key, be that on a space ship or deciding on your vaccination options.
Not everyone has the same thought processes
One of the other reasons decision making goes astray in these movies is because those involved in that decision making often have undisclosed values, beliefs or drivers that are impacting their choices, and this process is not always obvious to those others involved. This is true from androids that may or may not be obviously androids and who will have programmed ‘primary directive’, as well those working for the corporation. This is interesting as they often have more complete information than the others involved, as well as seeing the situation through a different lens because of how they view the world. This means that they can see others as disposable or views risks different, as they have a set of criteria that they wish to achieve which is more than just survival. Although in clinical life the juxtaposition is rarely so extreme, the challenge of reaching alignment when people come with different world views can definitely impact shared decision making.
Smart people can do stupid things
Having said all of that, smart people can in general do stupid things, even without all of these complications. Even when the experts are the ones making the decisions they can still make the wrong ones, especially when tired, stressed, or lacking all the information. This is the reason why protocols are key, drawn up and decided upon when all of the confounders to good decision making are not present.
You need to follow the standard operation procedures
In the end this entire post has been a very very long way of saying ‘JUST FOLLOW THE SOP!’
Many of these movies but have been much shorter with a much reduced body count, if those involved had just followed the pre-established procedures laid down for their safety. Obviously, we don’t have so many Xenomorphs as a daily risk factor in healthcare, but the same is true for us. SOPs are rarely there for the sake of it, they are there to support decision making so that in times of stress or information overload, you are not having to seek extra information to support good decision making, you have it freely pre-digested and available to you. So the next time you think twice about donning that PPE or the closing that isolation room door, ask yourself ‘would you open the airlock door?’, think twice and do the right thing.
And now for something completely different
Finally, because this is something that has amused me whilst watching these films and is probably not something that I can talk about in general down the pub. The computer in the Alien movies is usually referred to as Muthur, pronounced Mother. I just want to share my joy that the analysis software that is used to help analyse 16S rDNA runs, to give you microbiome analysis i.e. tell you what bacteria are present in your sample, is called Mothur, and also pronounced Mother. I’m sure the two things have nothing to do with each other, but allow me my scientific joy that something which was so ‘other world’ when it came out to me as a scientist has the same name as something imagined from ‘another world’.
Also, if anyone needs a science advisor on their next project, give me a shout as this post has brought me much joy and I think I may have missed my calling 🙂
Firstly, lets start with an apology. I’ve haven’t posted for a month as I’ve been struggling health wise and not really been able to get to a laptop to be able to write. Although annoying, it has given me plenty of time to think about what I might want to write next, so hopefully you’ll forgive me.
Now, onto the present. I’ve been in post for 20 years this month, and have also just spent some time recording a couple of webinars that covered bits about the journey to consultant. It felt timely, therefore, to put something out there talking about my experience of the consultant journey. Word of warning, though, this is only my experience, and everyone’s journey is different. I hope my sharing this it will help others, both in validating the aspiration but also in supporting expectation setting by talking about what it was really like to go through. Frankly, I want to be clear that it is never as linear as it appears from the outside and that that is perfectly OK.
So, let’s start at the very beginning. On my first day in post (all the way back in 2004) I was told that I was on an 11 year programme from trainee to consultant, and boy did I drink that cool aid and believe that would be the truth, after all these people were my bosses, supervisors and mentors. Sadly, it transpired that although they were being inspiring they were also far from being completely honest in terms of disclosing how straight forward, or not, the programme and progression actually were. I am now a Consultant Healthcare Scientist, although it took me 16 years rather than 11. Now I’ve reached the promise land I want to be clear that it was no where near the linear journey that I was sold on recruitment and there was a lot of struggle at every single stage. That being said however, now I’ve crossed the line, I wouldn’t have had it any other way. It was dealing with those barriers and obstacles that made me really decide who I was and what I wanted. It was also where most of the learning was truly at. So I wanted to write a blog post that doesn’t sell the ideal but discusses the realities of what some of those barriers looked like and to make those facing them a) feel less isolated and b) know they can be overcome.
You have to be doing the job to get the job
This one took me a long time to fully comprehend, as it can feel counter intuitive, but you have to already be doing most of the role in order to be able to get the role permanently. It is easy, in moments of frustration, to turn around and say ‘that’s not what I’m paid to do’ or ‘if they want me to do that job they need to pay me for it’. There are definitely times when you need to dig your heels in about workload and boundaries, but this generally needs to be the nuclear option. For the most part, you need to be prepared to roll your sleeves up and jump in to get the experience so that you are well placed to advocate for a post to be created, if that’s your aspiration, or to enable you to apply elsewhere with confidence. For me, I learnt huge amounts when I provided maternity cover for a year as a trainee. It built trust and showed willing to my clinical lead as well as providing me with experiences I would not have had in any other circumstance, enabled me to springboard into my next post, and meant my clinical lead wanted me stay enough they found money at the end of my training. Maintaining an openness to opportunities and an awareness of the fact that stepping up, although not always recognised financially or otherwise, does come with benefits on all sides and is an important part of playing the long game.
There is no single way to get from A to B
When I started, I thought the journey would be straight forward. I’d finish training, I’d get my 4th year funded, I’d get a Clinical Scientist post. Then I would work towards FRCPath and a PhD, hopefully moving into a Principle Clinical Scientist post. Once I’d achieved my tick boxes, my loyalty and hard work would be rewarded and a Consultant post would be forth coming. That’s just not the way work places and budgets work however. On this one patience is THE virtue, and the sooner you can acknowledge that A doesn’t immediately lead to B, the better for your mental well being. That said, the training pathway now available for Healthcare Scientists does make, at least the early stages, more straight forward.
Counter intuitively I’m going to say that, looking back, not having access to the straight forward route has been the most beneficial thing that could have happened to me. I would never have ended up with a clinical academic career if I hadn’t needed to acquire further salary funding and a PhD. I would never have ended up in Infection Prevention and Control if my training programme had been funded for the full four years. So many of the things I value the most only came about because I had to find ways around barriers and due to glorious happenstance. Despite being challenging in the moment, I’m grateful for every detour taken.
When it comes down to it, the person responsible for your progression is you
This one may feel harsh to hear, but no one is as invested in your career as you are. I’ve had a fair few people over years who’ve come to me and said that they deserve to be given X or Y. No matter how true this may be, this isn’t how it works in reality. If you want something to happen, you have to be the driving force to make it so. You are the star of your own movie.
I think a good example, for me, of this was my training programme. I was really fortunate that no one would block anything I wanted to do. The flip side of that coin was that no one sorted anything out on my behalf. It was my responsibility. I could go to any clinic, shadow anyone I wanted to shadow, but I had to reach out to find the contacts and arrange it. I had to have a vision of where I wanted to be and put together the pieces to enable me to get there. This is, in turn, enormously freeing and terrifying. It taught me early to be the master of my own destiny, and this is an important lesson for anyone on this pathway, irrespective of how supportive your surroundings at some point you will have to make it on your own.
You will hear a lot of no
One of the reasons to learn early to be your own driving force is that you will hear a lot of no as you under take this journey, whether that be linked to funding, exams, or posts. If you haven’t set your own direction then it can be hard to keep driving, as you may not be sure what you keep pushing for. As the old adage says, if you don’t have faith in yourself, no one else is likely to.
A lot of the no you hear will not be personal, a lot of it will be nothing to do with you or your skills. That doesn’t stop it from being hard to hear or from it feeling personal when it is not. A key skill that isn’t much talked about is learning how to respond to these challenges. You need to move to a place where you are able to process and move on without carrying that rejection with you. To learn from the moment and then let it go, so you always emerge a stronger, better person for the experience.
You have to know what matters
Something that can really help when facing the barriers and challenges along the way is being really clear what matters and why you are pursuing the choices you’ve made. Why does this route align with your own personal values and beliefs? If you understand your ‘why’ then you can weather the delays. It makes it so much easier to get back up when you’ve taken a knock.
The other side of this, which we don’t talk about anywhere near as much, is the importance of knowing what doesn’t matter. You can’t fight a battle on all fronts, and there will be positions you get into when you discover that you are fighting for something out of habit or without thinking about it. This is a waste of energy that you could be focusing on something that actually matters to you. Developing the self reflection to know when this is the case and using it to remove yourself from the arena is one of the most freeing and valuable skills you can invest in. I learnt this late, and I really wish I’d realised it earlier.
It is not an even playing field
I started this journey as pretty naive. I think I genuinely thought everyone would have a similar set of challenges and barriers to overcome. This just isn’t true. I know people who’ve become Consultants over a weekend with no external advert or interview. I know of trainees who’ve gone from point A directly to point B because their faces fit and everything aligned for them, not many but some. The challenging reality is that sometimes the playing field just isn’t even. Some disciplines are more set up for straight forward progression than others. Some disciplines have a bigger medical leadership who may not understand the role of Healthcare Scientists. In all honesty, being a woman in science is also not always straightforward. The gender issues are not always as obvious, but they are definitely still there, and that’s before we even start talking about other diversity issues.
When confronted with moments where this imbalance becomes apparent, we always have 2 choices, you can quit, or you can continue to fight. One of my core values has always been about parity of access, and one of the reasons I became a Lead Healthcare Scientist was to be in a position where I had the capacity to influence in this area. So when you come across inequality on your journey, whether it’s something you face or become aware of as an ally, I would always encourage you to be the change you want to see and to remember these moments when you are in a position to make life different for those that follow you.
Know that it’s OK to change your mind
So far, I’ve talked a lot about making Consultant, but I think it’s important to talk about the fact that it’s OK to also not want to end up as one. Life is about far more than work, and even in work we all find different sources of joy. The job role as a Consultant is not the same as a qualified Clinical Scientist. You won’t get lab time. There’s an expectation that it’s not a 9 – 5 role, and you will sacrifice a lot to get there, both financially and in your home life. It’s not the right choice for everyone, irrespective of your capability to do the role if you chose. I just wanted to take a moment out to write something that is supportive of starting along this route and then deciding it isn’t for you, for all kinds of different reasons.
Sometimes, I think people feel pressured to continue as ‘I’ve started so I must finish’. I love where I’ve ended up, and it was always my passion. If that wasn’t the case, then I would always support ending up where your passion does lie. That could be in the lab, in education, in quality or leadership. We are so lucky to have so many different options. I’m also aware that I talk about ending up working where your passion lies, and that is also not right for everyone. For many people, that passion doesn’t lie at work at all but with other aspects of their lives, and work is just what enables those things to happen. In my clunky way, I suppose what I’m trying to say is you do you boo and don’t let the pressure of expectation or external influences lead you down a pathway that isn’t right for you.
Bring yourself to every interaction
This all brings me onto something that also took me a long time to embrace. You can’t spend a career spanning decades pretending to be somebody else. For about my first 5 years in post, I didn’t really talk about the things that interested me. I didn’t talk about being a gamer and a geek because I was just really concerned about any judgement and how that might impact my career progression. It took me a while to accept that putting on a front is both really tiring and limits the amount of genuine relationship building you can do.
That said, I acknowledge that it can also be really hard to turn up as your whole self. I know there are some leaders out there who say we don’t owe our full selves to work, but I don’t think I know how to do it any other way. If I want those I lead to share something of themselves so we can build true connections, then I don’t think I can do differently. I’m not saying that everyone has to share every aspect of their lives, but I think I have to lead by example. For me, this means embracing the fact that I am not perfect and that I will have bad days as well as good, and make it OK to talk about those things. For me, that opens up dialogue on coping strategies and deeper dialogue versus pretending that everything is perfect. Everyone brings something different and we should honour that difference by embracing it rather than hiding who we are.
Sometimes, it’s just a case of continuing to show up
I’ve talked a bunch about some of the reasons that making Consultant may involve surmounting or finding a way around barriers. I think one of the things we talk less about is the fact that the thing that often makes the most different is continuous effort. At its heart it’s about continuing to show up, on good days and on bad. It’s about demonstrating commitment and being in it for the long haul.
Now, when I say continuous, no one expects every day to be the same, but there is a consistency linked to intention. If you are clear where your ambition lies and stick to it, it is easier for those around you to also factor that into their thinking. If you are changing the goal and ambition regularly, then can be harder for those trying to support you. It’s not that you can’t change your mind, but you should try not to scatter gun your approach. Making Consultant, to me, like getting a PhD, mostly seems to be about a tenacity of purpose that means you keep showing up, combined with the patience to know it will happen eventually.
Always remember why you started the journey
I think many of you will know that patience is not my greatest asset and so I found the journey so frustrating at times, as I had such a clear vision that was not always shared by others. For this reason, you really need to know that the pursuit of this is right for you, right for you when start, but also stays right for you along the way. It’s that clarity of purpose that can re-centre you when things are tough or when you are facing those no’s. Without it you could easily falter and it may be that it really isn’t the right option for you.
The other reason to have that clarity of purpose is that it is not like reaching the destination transports you to a land of rainbows and bunnies. Consultant roles have their own challenges, and in many ways just having the title doesn’t really change anything. The job is still the job. Therefore, if you aren’t sure along the way, you may just be signing up for more of something that may not be what you want it to be. The flip side of that coin is that if you are sure, and know what you are working for, you are likely to end up in the job you’ve dreamed of and aspired towards for over a decade, and that feels pretty damned good.
The people make the journey worthwhile
I just wanted to finish with something that has struck me more and more as I moved along the stages to becoming a Consultant. Although all the professional stages feel significant, it’s the people I’ve met along the way that I am most grateful for. It’s these people who will stick with you long after the nerves and stresses of an exam are just a distant memory. They will be the ones that guide and pick you up when you hear the no and face the obstacles. They are the ones that, when they celebrate with you, make the celebrations really worthy of the name. So don’t be so focused on putting one foot in front of the other that you forget to look up and find time to develop the relationships that will last a life time.
As Girlymicro has a) got tonsillitis and b) attempting to run the day, todays blog is a guest blog brought to you by frequent Girlymicrobiologist contributors and Environment Network stakeholder members: Sam Watkin and Dr Claire Walker.
It’s the most wonderful time of the year! Today is the Environment Network meeting where we gather together to talk all things environmental risk assessment. This is a network for people in clinical, scientific and engineering roles within the NHS and other associated organisations who are interested in the role of environmental infection prevention and control in preventing infection. Despite being an immunologist (Claire Walker) for most of my career, this is one of my favourite meetings of the year. Everyone is deeply passionate about what they do and how we can work together to exchange ideas and improve practice.
Too kick us off, we have the wonderful Professor Elaine Cloutman-Green and Lena Ciric welcoming us to a day of interactive sessions on key issues in the field. Prof C-G sets the scene for our day introducing the concept of our different perceptions of risk assessment and the challenge of unexpected consequences. Of course we understand the triumvirate of identify, understand and mitigate problems but how an engineer approaches risk is quite different to how a clinician might. As Prof C-G says clinical risk assessment is not a zero harm game, it is about controlling real rather than theoretical harm. A balance needs to be stuck between what is most appropriate for the patient – we could keep patients in bubbles and not even have healthcare professionals approach them, but I doubt that patient would fare very well! There is a need to balance the approach of the clinical and the engineer to find an optimal position to minimise harm. To make these decisions we need to consider the interaction between organism, patient and the built environment in order to work out what the control measure should look like. Problems aren’t simple, we need to accept and embrace that risk assessment is a complex process. And perhaps most importantly we need to take the time to see the perspectives of others, or we might never see the elephant in the room.
Risk assessment has the potential to make use all uncomfortable, as scientists we do not enjoy the unknown. In good risk assessment A plus B does not always equal C, it might do 50% of the time so we have to rely on our best judgement. Moreover, risk is not static. All patient and clinical environments are quite different as we need to pick the point that works for that situation – National guidance can never cover all of these unique situations. A multi-disciplinary team approach is essential to ensure we are asking the right questions.
Next up we have Dr Susanne Surman-Lee giving a talk on combining clinical and engineering risk and why working in silos hinders risk assessments. Silo working at all levels, even within a team, can cause a raft of problems, with poor communication, different priorities, resource conflicts and inefficiencies. This can mean those in each silo work to their desired outcomes, not taking into account what other requirements may be. The danger of this is that it ultimately increases the risk to patients.
A poll found that the event was well attended by people from a range of disciplines, covering many relevant professions to environmental infection control. We often all want different things from a building, be that aesthetic, cost or usability. What is critical, and reflected in new guidance, is that the purpose of a building must be to put the patient first.
To escape working in silos, the audience recognised that communication is absolutely key. Working as a single team, sharing respect, data sharing and fostering a collaborative culture is all needed to break down individual working silos. This enables the project team to work as a single unit, supporting faster, safer decisions across strategic levels.
A set of examples on real-world decision-making processes highlighted not only the importance of accurate record keeping when it comes to decision-making, but also what can happen when an IPC challenge is only viewed through teams working in silos.
When considering waterborne infection risks, a multitude of challenges, both from an engineering and non-engineering standpoint must be considered. This can range from inadequate usage leading to stagnation, poor hygiene during installation and poor labelling, outlet misuse, poor cleaning techniques and inappropriate assessment if transmission risks as examples.
Ultimately, we must consider the problem as a whole. Different hazards and sources of pathogens overlap, meaning we must work across disciplines to mitigate risk. We also must gather information from multiple sources to identify risks to make sure a risk isn’t overlooked.
Updated guidance has recently been produced following an outbreak of non-tuberculous Mycobacteria for the safe design and management of new buildings calls for collaborative working throughout the project, with continual risk assessments and project ownership by the trust. Having a multidisciplinary approach can help effectively design and manage risk, improving IPC risk assessment and decision-making procedures.
In this final session before some essential caffeine, we have Andrew Poplett taking us on a whistle stop tour of derogation management. Derogations, like puppies, are for life – if you agree to one you must be sure as they are extremely difficult to reverse. We know that unless specifically stated much of the guidance in not mandatory. However departure or derogation from HTM should provide a degrees of safety NOT LESS THAN that achieved by following the guidance laid out in the HTM.
A derogation is an exemption from or relation of a standard or rule but it must be carefully managed, documented and justified. It must be risk assessed and cannot be to reduce costs. Of course, the bugs haven’t read the HTMs and they really don’t care about the budget! Minimum standards and patient safety guidelines cannot be derogated, but for those for those ‘nice to haves’ there is some wriggle room. So why do we want to derogate? Situations like conflicting guidance and refurbishment of existing buildings. Once again we are lead to the conclusion that these decisions must be the result of a multi-disciplinary team approach and risk assessments – these decisions can’t be made solely by a financial manager, an engineer, a microbiologist or infection prevention and control, but requires a meeting of minds to reach the right conclusion. The cornerstone of derogations is communication, ideally reaching a sensible and agreed consensus that balances risk, compliance and other important factors (like cost!). Ego needs to be left at the door or we might need to start hiring some referees!
If you break the rules, you really need to document why, what, who and when. It’s not to say that we shouldn’t, as we know every circumstance is difference. But transparency is essential to the process, and they do need to be reviewed regularly. As a final thought, Andrew invites us to consider that it is important to remember that it is always cheaper to invest the time upfront because short cuts tend to end in expensive disaster.
After a quick coffee break, we have Louise Clarke from GPT Consult discussing capturing water and ventilation risks as part of governance strategies. First off, we must understand what risks we actually need to assess and manage. We often have aging infrastructures, changes in usage, hidden infrastructure, access challenges and maintenance works. Not only that, how people use and view spaces factors into the risks we must assess.
When assessing risk, it must be suitable and sufficient. But what does that actually mean? It depends on what you are trying to deliver, what you are looking for and what is being managed. Five-by-five risk matrices do not necessarily capture the complexities of these risks. Not only this, a huge amount od information is required for effective assessment. Factors like patient factors, unique building features, data from building management systems must all be considered. Not only that, but there are a large amount of unknown factors which need to be considered. The current state of a building and the equipment in place is important to consider, with the impact these may have in the future on risk taken into account. Overall risk profiles are needed but challenging to achieve as many people view the risk of a setting from different perspectives.
All risk assessments must be performed within the appropriate legislation. This covers government legislation, approved codes of practice and best practice guidance (such as the HTMs). To ensure that all standards and met and the process of derogation is appropriately followed, governance structures have to be followed. But these structures themselves can be difficult to navigate. The reporting of information gathered from the building (such as information from the building management system) can be challenging through these structures. How do we ensure the data is appropriately recorded, interpreted and presented? Do governance structures effectively allow for this process and make sure that the data collected useful and enables risk assessment? So, how should the data we collect from the building be presented? As with many things, it depends. What the intended use of the information is, how is needs to be interpreted and disseminated all matter.
Typical governance structures include water and ventilation safety groups. These groups serve to bring together estates, infection control, representatives from the relevant clinical units, contractors in order to assess risk and make informed decisions. Are such meetings suitable to address risk? The volume of data that must be presented, understood and used to inform decisions is massive, and these meetings are time-constrained. A lot of the processes will be informed by the risk appetite of the organisation. Information may not be available and work may not be possible. As such, appropriate record keeping and reporting is crucial. Taking this all in, governance strategies which to be implemented must be practical, realistic, effective, suitable and sufficient.
Sadly Dr Derren Ready from UKHSA is enjoying a marvellous holiday so we have a recording from him today. We are venturing into the field of community risk assessments and the considerations that are notably different from in the hospital. There are significant challenges, as highlighted by the consideration of the prison system where an outbreak might further restrain the liberty of the prisoners impacting significantly on their mental and physical wellness, thus careful balances need to be struck. In essence, the challenges of the community require a different set of questions to be answered in risk assessment.
In community risk assessment the first stages fall to information gathering and fact checking. Information gathering might focus on the clinical, epidemiological, microbiological or environmental factors. Context of the information should be considered. In public health we often act on suspicion as time is of the essence. In the initial stages there is often simply anecdotal information and there is a need to all the facts to be checked through this dynamic process.
UKHSA bases its risk assessment of five key areas. The first of which is severity which is the seriousness of the incident in terms of the potential to cause harm to individuals or to the population. This is graded from 0-4 where 0 has a very low severity like head lice in a school whilst class 4 are extremely severe illnesses which are almost invariably fatal, like rabies or Ebola virus outbreaks. The second area is uncertainty, how sure are we that the diagnosis is correct based on epidemiological, clinical, statistical and laboratory evidence. The third area is the likelihood of the organism spreading covered by an assessment of the infective dose, virulence of the organism, mode and routes of transmission, observed spread and susceptibility of the population. Again the areas are graded from 0 to 4 allow qualification of the potential risk. The fourth area is intervention, what could be done to alter the course of the outbreak? This ranges from minimal, non invasive procedures like handwashing to an urgent mass immunisation campaign or withdrawal of all contaminated food products. Clearly some outbreaks don’t lend themselves well to specific interventions an example would include responding to a cluster of vCJD disease where remedial intervention is particularly challenging. The last key area is context. The easiest way to consider this is to think about the broader environment in which the event is occurring. Factors like public concern, attitudes, expectations, strength of professional knowledge and politics have the potential to influence decisions about the appropriate response to an outbreak.
The best way to approach this complex process is through the use of a dynamic risk assessment where the risk assessment is continually reviewed throughout the outbreak. This allows UKHSA to make the best possible decisions based on the best information available. These dynamic risk assessments can be classified an routine, standard or enhanced based on the response required to an event. The take home message is very much that risk is not static and we need robust frameworks to ensure we make the right decision at the right time.
In our final talk of this morning, we have our own soon to be Dr Sam Watkins from UCL/UKHSA. Sam’s research interest in detection of surface based pathogens in the hospital. Surfaces can be come contaminated and play an important role in the spread of infection around the hospital. Once considered tenuous, the role of surfaces in the persistence of healthcare associated infection is now well established for several pathogenic organisms. The current standard is for surfaces to be visibly clean but there is no guidance on assessment of microbiological hygiene of surfaces. It’s extremely important to remember that just because something looks clean, doesn’t mean it isn’t crawling with bugs! Again, we must consider that a one size fits all approach cannot be enforced across the NHS as we have so many different situations and patient requirements.
Sam’s research focuses on development of new tools for assessing surface-based transmission risk. Surface sampling can be many different things from contact agar plates, to specific swabbing or sponges, to PCR identification of specific viruses in a outbreak scenario all of which have different purposes. All of this information can help support clinical risk assessment and the actions of infection prevention and control. Currently surface sampling is most commonly used as a retrospective measure after a clinical incident during outbreaks. Sadly there is little guidance or framework in place to guide process in this area. Furthermore, the identification of a pathogen on the surface doesn’t provide sufficient information on if this is the cause of the outbreak. Sam’s work has been to gather prospective evidence gathering through surrogate markers which mimic a microorganism in the environment without posing any infectious risk. In Sam’s work, he has been using cauliflower mosaic virus across an outpatient and inpatient haematology oncology unit. Three markers derived from the genome of the cauliflower mosaic virus were used and inoculated on various risk level surfaces. After 8 hours the swab samples were collected from pre defined sites. The movement of the surrogate markers across the unit were investigated over the course of five days. Within 8 hours there was widespread movement of the markers across the outpatient unit. A slightly less dramatic spread was noted in the inpatient site. From this we see that there is huge variability in the dissemination of markers, markers deposited on high risk sites where identified in a greater number of places. Paediatrics certainly adds an additional dimension to this work, with children spreading viruses through an exciting game of hide and seek in the department! An important take home message here is that a one size fits all approach is unlikely to be successful, given the highly varied nature of clinical settings. A unique approach to surface-based transmission risk assessment and mitigation may therefore be needed.
With the morning session drawing to a close. We look forward to a delicious lunch, more coffee and interactive case based discussions this afternoon!
If you want to find out more about environmental infection prevention and control and future events you can check out the Environment Network here. Girlymicro has also previously posted about risk assessment and the role of the environment in healthcare settings, links to more posts can be found here. The main theme of the day was that we all need to get out of our silo’s and talk more, so let’s start that change by being bold, starting conversations and getting out of our boxes!
I’ve been thinking a lot about pathways in healthcare lately, from having conversations about T-levels and apprenticeships this week, to equivalence and Higher Specialist Scientific Training (HSST) posts. It’s made me reflect a lot on my own training pathways and the fact that the majority of the advice I received was that the only option, in terms of approach, was to work harder and do more. Now, don’t get me wrong, there is some merit to that, and there is also some truth, but I had it drilled into me that you can’t be successful if you do a 9 – 5. You must always do more. You must always over deliver. You must always be adding to and diversifying your CV.
This advice and approach has been key to me developing into the person I am now. I am objectively successful and so grateful for the support I’ve received along the way. I have the long dreamed of Consultant post, and my dream job. I was made a professor within 10 years of finishing my PhD. I’ve held multi-million pound grants and have over 50 publications. The other side of the coin is that, despite being exhausted, I can never sleep for the number of things I haven’t finished, and I constantly feel like I’m not doing or achieving enough. I’ve also written before about the impact of my anxiety levels when I’m tired or try to step away. So, as new starter season comes upon us, I wanted to take a moment to really talk about the messages we are giving our trainees, and ourselves, to think about how true they are for current training opportunities and what we can do better for those that follow us.
Let’s start with a bit of history and the messaging that we used to focus on as part of training
Goal orientated view of the world
During my first week as a trainee Clinical Scientist, I was sat down and told that it was an 11 year training scheme to Consultant, but it was up to me to put in the work and make it happen. Well, I worked pretty damn hard, including not having a weekend off at one point for 3 years, and it still took me 16 years. Does that make me a failure? I don’t think so. Does that mean that I should have worked hard to make it happen in 11? I’m not sure of how I could. In fact, I don’t know of anyone who made it happen in 11 years. Of the 4 of us who started, only 3 are now Consultants, and we were a pretty committed bunch. So were we all set up to fail?
The whole scheme was designed with that 11 year target in mind. I understand it from a strategic point of view. There are a lot of boxes to be ticked. Our situation was made even harder as there were only 3 years’ worth of funding for a scheme that required 4 years of professional practice to gain registration. That meant you also had to prove yourself worthy and useful enough that someone would decide to fund you for that extra year. Otherwise, everything had been a waste, and you would walk away unregistered and unlikely therefore to get a job.
My main problem with this approach is that it doesn’t really allow scope for exploration, and it really doesn’t allow time for creativity. It trains you into the ‘onto the next thing’ approach. I certainly had no time for celebration or reflection between stages. I was always trying to make sure that I was useful enough to remain employed, and in later stages, as it took me 13 years to be made permanent, I had to also ensure I was bringing in sufficient money to cover my salary so I would be kept in a job. It also means that when you finally do get all those boxes ticked and get your dream job, you are so trained into the tick box way of life that you are left searching for what the next box should be, rather than embedding and celebrating what you have achieved.
There is nothing that cannot be fixed if you work hard enough
When I started work, I used to read a book at my desk during my lunchtime, like I had when I worked at Birmingham City Council. It would always be some variety of fiction novel. I came into work one day during my first few months, and a pile of textbooks had been left on my desk with a post-it note suggesting that maybe I should read these instead. The implication, to me, was that it was not acceptable to have downtime, that any moment I had should be used to continuously work and improve myself. In short,’I must try harder’ ‘I must work more’ in order to justify the privileged position I was in. If I wasn’t going to lunchtime talks, the time should be used for other improving activities.
I also remember clearly listening to amazing female Healthcare Scientists talking at events about how, to achieve as a woman, you always had to work harder and do more than anyone around you. It was made very clear that it was required to constantly go above and beyond if you wanted to reach their position, if you wanted to succeed, if you wanted to make a difference.
The messaging has always been pretty clear. No matter how hard you are working, it probably isn’t enough, and you must work harder. Otherwise, you will fail and let everyone who had faith in you down, as well as yourself. If experiments fail, you don’t go home, rest and reflect, and come back tomorrow. You stay and set it up again. There were just too many midnight finishes to count during my journey to Consultant. If you want it, you will just work harder until it happens. I submitted my PhD a year early in order to achieve FRCPath whilst on my fellowship. At the same time, I took a PGCert in education because I recognised that it was important for my career path and my interests. Looking back, doing those three things simultaneously was foolish beyond measure. At the time, I thought I was just demonstrating that I had what it took.
Effort must be continuous
At the very start of training, I remember sitting over a bunsen burner crying. I was so ill, but no one around me ever took any time off sick, and it was just not considered to be OK. Eventually, I was sent home as I just couldn’t breathe, but it was very much ‘see you tomorrow’. Having an ‘off day’ was not something that happened. The hard earned truth I’ve learned to accept is that my best looks different from day to day. Some days, I could take on the world. Other days, I struggle to crawl across the line at the end of the day. Especially with a health condition made worse by stress, the idea that I can just ignore it, carry on, and always achieve amazing things every day is sheer madness. This was how I tried to work, however, and it took seniority and growing older to come to terms with the fact that this was just not achievable.
The thing about seniority is interesting. There is something about seniority and being able to give yourself permission to do things differently, which is worth mentioning. That’s not the real difference, though. I think the real difference is in the expectation setting. I try to be the person who gives others permission to acknowledge that some days are harder than others. Who checks why people are still there when they should have gone home. Doing this for others has the side benefit of reminding me that sometimes it’s OK to also do this for myself. It is not possible, nor is it necessary, to work at 100% all of the time. There will be days when you absolutely need to bring it, but there will be recovery days when what you should do is catch your breath, and if possible, do some reflection in order to make things better long term. A career is a marathon and not a sprint, after all.
There is no room for failure
This one isn’t just a work thing. It’s definitely a family thing too. My father is infamous for saying that no child of his has ever failed anything, and we weren’t about to start now when I was worried about FRCPath.
The Clinical Scientist training programme has always been competitive. Getting into the programme was competitive, but even when you were in it, my experience was that the programme itself was pretty competitive. The people on it were used to being at the top of their class, and I experienced a fair amount of posturing throughout my first 4 years. Far from being tackled and a focus placed in peer support and collaboration, I feel like the rhetoric around the programme added to this. The focus on there not being enough places for us all to get posts when we finished, and the constant commentary on only the best of the best being able to get Consultant posts, placed us in direct competition with each other from day one. Therefore, you couldn’t talk about challenges for fear of disclosing weakness that would impact your future. That atmosphere is one of the reasons I’m so passionate about talking about the reality of the job on this blog, both the highs and the lows, as I didn’t have any way to normalise my experiences when I was training and in the midst of them. I hope posting will help others in finding a benchmark for ‘normal’ that I didn’t have.
Even on a day to day basis failure was not an acceptable part of training. To this day, I remember that one of my fellow trainees reported a NEQAS result (part of a quality control scheme), and she got it wrong. The result got reported, and the department lost a point on the national scheme. In reality, it should have been checked by someone else before it went out, but it happened. The virology consultant at the time never spoke to them again. We would sit in joint tutorials, and he would ask a question, he would then wait for my response even if I was just repeating what my colleague just said. He would respond to my answer but not theirs. There was never a review of what had happened and how the mistake had occurred. There was no acceptance of the fact that being part of a quality scheme is there to support learning and to identify where improvements can be made. There was just a long-term change in the way that trainee was seen and how they were then supported. It was a clear demonstration of what would happen if a mistake was made and that it would impact how your working life would be from that point on.
Quitting is not an option
The same trainee went through a hard time during her final year. She basically spent a lot of her time crying, and the response was that she was allowed to come in 30 minutes late. She started to see a therapist, and even though we never met, I owe that therapist a lot. Her therapist pointed out that in the three years she had been in post she had never been out for a cup of tea with a colleague, so she was given homework to ask someone out for tea, and she asked me. This was a real turning point for me. We went for tea, and we had a real conversation about the things that were both hard and good. It was the first time that I felt less alone. It was also the start of a conscious decision I made to take people off site for tea, to support better conversations, that I’ve continued to this day.
Later that year, she walked away. She made a decision to go a different way. It took enormous strength to do it, and even now, I have enormous admiration for her. Until that point, I hadn’t known anyone make a decision that prioritised their wellbeing rather than the CV tick boxing. The general attitude was that Healthcare Science is a small world, and you were incredibly fortunate to be a part of it. It was so hard to get into, and you had put in so much that you would be crazy to walk away. There was judgement linked to failed experiments, let alone walking away from the programme. Seeing someone break that mould was incredibly powerful.
The truth is none of these messages are entirely true, so how do we do a better job of messaging for current training programmes?
Training is just that, a learning programme, a time to explore, fail, and reflect on those failures in order to learn to do things better. If the messaging I experienced as a trainee now feel less than ideal, what messages should we be encouraging? I’ve been having a think and these are some that I would like us to have better conversations about:
We are more than the sum of our qualifications
Not everyone is going to become a Consultant. Not everyone is going to get FRCPath and a PhD. You know what, that’s perfectly OK. It doesn’t stop you aspiring for those things if that’s what you want. However, our trainees are not in a Hunger Games style competition to be the last one standing. More than that, how good you are at your job is not dictated by how many qualifications you pick up along the way. Some of the most amazing Biomedical Scientists I know and have the privilege to work with don’t have a masters degree. It’s OK to be a brilliant band 7, and be satisfied and fulfilled by the role you have. Your qualifications don’t define your worth, and it’s OK to make choices that aren’t about playing CV bingo. It is also OK to decide that those things matter to you, you still aren’t defined by them. They have the value you choose to give them.
It’s OK to pause and reflect
No career is a straight path, no matter how it looks from the outside. There will be bumps along the way and the odd hill/mountain to climb. You will reach the destination better for it. You will be able to handle the journey a whole lot better if you allow yourself time to pause and reflect along the way. A big part of development is about making time to reflect on where you are and where you are going to, but also asking the big questions about whether those decisions and reflections you’ve made previously are valid for where you are now. You will be working for decades, and the decisions you make in your 20s are unlikely to reflect the decisions you might make in your 40s, so making time for active reflection isn’t a luxury, it’s an essential part of a professional career.
Knowing when to change direction requires courage
In many ways, I’ve been pretty fortunate, the things that I’ve wanted have aligned with my values and have stayed pretty consistent. This could easily have changed, however. I suspect that if I’d been able to have a family, my focus may have altered somewhat. Knowing when to change your focus or direction is important. This a balancing act between knowing when you just need to double down because things are getting difficult, or when you have truly shifted as a person and that you have to change direction to reflect this. Mentorship and coaching can really help with both this and the reflection that may get you to that moment. Acknowledging that continuing down a path ‘just because’ may not be the right thing and that it requires courage to sometimes jump off a cliff and make a big switch is a step that may require additional support.
Your value is not defined by your productivity
This is the one that I struggle with most and therefore know I probably fail to provide the best leadership around. I often feel that ‘I’m do what I say’ not ‘do what I do’ in this area. I often feel defined by my to-do list, and when that gets out of control, as it often does, I place a LOT of judgement on myself. The thing is, if I get hit by a car tomorrow, no one is talking about my to-do list failures at my funeral. I hope that they will talk about how I made them feel, and maybe even this blog. It is hard, but we can choose what defines us. You have that power. One of the reasons this blog is ‘Tales of a recovering workaholic’ is because I recognise I need to change, and I’m hoping to do a better job of playing this on forward and encouraging our trainees to be defined as well rounded individuals with interests outside of work. We need to encourage a holistic view of value in ourselves and others.
There is no prize for working the hardest
The biggest lie I felt that was embedded in my original training programme was that if you just worked hard enough and ticked the required boxes, the prize was there at the end of the race. The hard truth is working hardest does not get you the job. Ticking all the boxes makes the outcome more likely, but it doesn’t guarantee you anything. There is no prize for the most midnight finishes. Trust me, I’ve done enough of them to know. To a certain extent, the prize for working hard is more work. If you set the bar at working most weekends, then your work just expands, so you have to work most weekends in order to keep on top of everything. If you require external validation, like me, this can be a really dangerous game to get into. If we see this in our trainees or ourselves, I think it’s important to recognise and actively find other ways to find that validation before it becomes built in or results in negative consequences.
The next generation of trainees deserve to benefit from the experiences of those that came before, both in terms of knowledge and in learning how we could do it differently. The working environment has changed, as have our trainees and training pathways. By thinking more about our messaging we can make the work place right now more suited to where we want it to be, rather than relying on chance to make it better. Everyone has a role to play, but we, as leaders and educators, should be prepared to lead by example and own the change we wish to see.
I woke up at 5 this morning, the alarm wasn’t set to go off until 6:15. I am desperately tired and in need of more sleep. Instead of allowing me this simple luxury my brain decided to a) run through an experimental protocol, b) draft a paper I need to write, and c) plan a conference presentation. Sadly, my body wasn’t in alignment with this and so none of it has been written down or recorded anywhere. I am therefore exhausted still and have no concrete outputs to balance it out. I’d like to state this was a one off, but it is in fact my life and daily existence.
People often ask me how I manage to ‘do’ so much. The sad fact is that I really don’t think I manage to ‘do’ very much at all. I’m always a chapter behind on my ‘to do’ list. That combined with the fact that I only manage to get as much done as I do because Mr Girlymicro keeps our lives together by making everything happen at home, means that I thought I’d write something that talks openly about what the reality of having a mind that just doesn’t stop looks like.
I only have 2 speeds
I think those people who think I achieve a lot only see me in ‘doing’ phase. Running around spinning multiple plates at the same time and being totally ‘eyes on the prize’ focused. The other side to this is that when this Duracell bunny phase is over, I become the sloth girl who inhabits the sofa and doesn’t contribute to house work or the want to leave the house. The challenge is that work generally gets the Duracell bunny which means there is very little left over for real life. Hence Mr Girlymicro deserving the husband of the year award 15 years running, and the fact that I need to find a way to split my energy better.
My mind can’t switch off
One of the reasons for the enormous to do list, is that although my body switches off, my mind really doesn’t. I would really love it if it did. Today is Easter Monday, it’s before 9am, and I would really love to be able to sit and chill out. Instead I’m writing this blog as my mind is so full of stuff that this is my equivalent of relaxing as it enables me to focus, and thus relax a little. I don’t know if this is how everyone lives? I really don’t. I have so many thoughts, I remember so many things I should have done, things I should be doing. My mind can make my life a less than relaxing existence. Lovely Mr Girlymicro has brought me some Lego for later though so that I can use it to help, as the process of doing something whilst watching a movie or listening to an audio book, is basically my relaxed happy place. It’s important to have a strategy when my head is spinning out of control.
I find it very uncomfortable to only do 1 thing at a time
This leads me onto another thing. I need to be doing at least 2 things at once to feel comfortable. I’m writing this blog whilst watching CSI on Netflix, later I’ll be putting together Lego whilst enjoying a movie, I even need an audio book to sleep. One of the reasons I’m so happy to have my little bathroom office is that I find it really challenging to work in silence and so it means I can have music or a book running as background audio. I really find it helps me focus. The advantage to this way of living life is that does it enable me to plan talks in my head whilst doing other things, or to plan a text book or blog outline whilst writing a policy. This adds to my ‘to do’ list but also helps keep my head above water when I’ve made too many commitments.
I’m physically lazy and don’t pull my weight
For all that my mind is active I am physically lazy. I always joke that I was born to lounge on a chaise lounge with a book in my hand surrounded by my library with someone to bring me Darjeeling on request. I know that I must be challenging to live with. I get so focused on things, that without adult supervision, I have a tendency to forget to eat or drink, one reason that I am much healthier when I work from home. When I work on-site I tend to come home in a ball of flames, exhausted by my working life and physically broken, and therefore contribute negligibly to doing any form of physical chores. I’m working on it, but saying that, whilst Mr Girlymicro is working upstairs here I am writing this blog instead of tidying the kitchen. I did say he deserves awards, and I am a work in progress.
My mind doesn’t let me rest
One of the other factors that contributes to my physical laziness is that I am so tired all the time. I rarely get a decent nights sleep. If I wake up between one and three to go to the bathroom, my brain kicks in as I’ve had just enough sleep. It’s then fully engaged, whilst my body remains sleepy, with things I should be doing or random thoughts. The same is true even if I get back to sleep, I rarely if ever manage to sleep to the alarm. I do all the tips that everyone talks about, I keep a notebook by the side of my bed, I make notes into this blog so get things out of my mind, but I find switching off really hard. Some of this is because I should probably just take some painkillers/antihistamines, to manage other things, but some of it is definitely the fact that my brain just doesn’t want to play normal.
I am a starter not a finisher
Another side effect of having a mind that is constantly full of ideas, is that it can be challenging to bring any of them to completion. I am very much a starter not a finisher. Finishing anything requires a lot of active effort, otherwise I have a tendency to get distracted by the next good idea that comes along. I think it’s one of the reasons that over the years I’ve become slightly obsessed about keeping my promises and deadlines if I’m given them, even if it means I work weekends and evenings, as I’m hyper aware of my natural tendency to drift. If I make a commitment I can be pretty over the top and harsh with myself about delivering on time. As a people pleaser, this has gotten me into trouble in the past due to over committing to too many things. There have been a lot of very late nights and lost weekends. These days I’m trying to not over commit, whilst using this particular fear of failure to ensure that I still finish things on occasion.
I find focusing on being in the moment incredibly challenging
I am aware that some people are able to really ‘be’ in the moment. When they achieve something, when they have successes, they are able to really be fully present in the moment and enjoy the depth of emotions that that presence achieves. Don’t get me wrong, I enjoy the moment, but my brain is always onto the next thing. I’m always planning and looking forward. In many ways this is a really useful trait, but it means that I’m pretty rubbish at stopping and smelling the roses. I think this is another contributor to why I find it so hard to relax, as even when I’m having a lovely time I’m planning for the next thing. When I’m on holiday, I find it hard not to be planning for how I need to address work when I get back. When I’m at work, it’s always about how to keep us moving forward, and what needs to happen next. I need to make more run for tea 🙂
I spend my day being reactive when I would love to be visionary
My tendency to plan is one of the reasons that I find the current state of the NHS and my role within it so stressful. I want to be planning how to make us better, but because we are still recovering from the pandemic, even if the outside world has moved on, I spend a lot of my time still in reaction mode. It’s one of the reasons that research is so very important to me. In that aspect of my role, as well as in education, I feel like I can be focused on how to make things better and move things forward, whereas that can be more challenging clinically. It is why I love and value the different aspects of my role, education, research and clinical, as they balance each other off for the different needs that I have personality wise. It’s why my role is perfect for me and I’m so grateful that I have been able to develop it the way I have.
I feel I should be doing so so much more
All of this leaves me with a continuous general underlying feeling that I should be doing so much more, that there is so much more to do, and that I need to be better. There’s a lot about this which is good, especially when I was training and it could be channeled into ticking off the necessary boxes. Frankly, it was also easier to work full force and recover when I was in my 20’s and 30’s. I don’t think I had the self awareness, or self reflection skills I have now to understand my drivers in the same way back then. I also don’t think I had the self forgiveness to handle my lack of perfection and therefore be open to change. Now, although looking in the mirror and seeing my flaws can be challenging, it also inspires me to be better and I try to treat myself with the kindness I would offer to others. All traits have a light side and a dark side. My brain means that I am more physically broken and can make the lives of those around me harder by not contributing as much as I should. It also enables me to create change and make the lives of others better. It has been the enabler and the driver to allow me to reach where I am today, and to do things like start this blog. Although peculiar, it is of more benefit than it is harm, and after 44 years in each others company, we have finally reached an en tant cordial, where we still strive for improvement but also live in acceptance of the reality of what the day to day looks like. So my advice, learn to love yourself for who you, whilst striving to be better.
Last week, I was lucky enough to be the Lord Mayor’s Colloquies (an academic conference or seminar) on water and sanitation, where the wonderful Dr Susanne Surman-Lee was speaking. It was an event sponsored by the Lord Mayor and supported by the Worshipful Company of Plumbers.
What has this got to do with bathrooms I hear you ask? Is it because it was on water and sanitation? Is it because these things impact healthcare design? Or are linked with infectious diseases? Is it because of the LAKANA Mali study? You’d like to think, but actually the trigger for this post was none of these things. It was triggered because I have a habit of hiding in bathrooms.
Hiding in bathrooms
I have posted before about networking, and that I’m not a natural in this regard. I have over time developed tools and approaches to aid me, but I still don’t love it. Now for a confession, and to be honest I genuinely don’t know if this is just a me thing as I haven’t really talked about it. Sometimes when I just can’t face networking, I hide in the bathroom of wherever the event is taking place so I don’t have to be in the room until just before the event start so I don’t even have to try. I’ve hidden in some pretty Class A bathrooms in my time, at the Houses of Parliament, at fancy hotels and most recently at Mansion House.
Some days, I just can’t face the sea of people and trying to come up with something interesting that I can bring to the conversation. It is especially bad when entering rooms when I just don’t know anyone or at least anyone well. Occasionally, my game face just fails me and so I find myself locked in a toilet cubicle negotiating with myself about what point I will leave in order to still look like I’m arriving in a timely fashion and with a window to grab some tea.
The negotiation is also about convincing myself to not a) hide at the back of the room, b) just call it quits and go home, and c) look confident and like I haven’t been hiding in a bathroom when I enter the room.
The negotiating doesn’t end here. Many years ago I made a deal with myself. I am allowed to hide in the bathroom, but only pre-event. Once I make it to the room I am not allowed to leave without speaking to at least one person I don’t know. It doesn’t have to be extensive, but it has to be a deliberate act of networking. One of the reasons I find this bit easier is because post event, at least, the one thing I have in common with the other attendees is that we’ve just engaged in the same activity. So that’s the rule, one person, one conversation before I’m allowed to leave. I don’t know if I’m the only one that has these types of rules, but now you all know if you see me hiding out in a bathroom, there is a reason why.
Developing a more than normal interest in bathrooms and water
You won’t just find me in bathrooms at events, however. Working in IPC has waaaaay more to do with bathrooms than I could ever have imagined before I came into post. From overflowing toilets to drain flies, we deal with it all. We often joke that we don’t know which members of the team are Mario and which are Luigi, as even when it isn’t an IPC issue, we still get all the plumbing calls.
As time has progressed, I’ve developed strong opinions on a wealth of topics that I never thought would hold meaning for me, from sink design to tap choice. I’ve also learnt a lot more about IPS panels (the panels at the back of your sink) and TMVs (thermostatic mixer valves) and how both can impact on other areas, such as my need to revalidate my specialist mechanically ventilated rooms.
One of the key things I’ve learnt, as well as being open to continuously learning, is that relationships in this area are key. This is an area where you need to be able to ‘phone a friend’. Friends aren’t just other people in IPC. You need to build relationships with engineers and designers, as well as those people in the lab who can talk you through your water-based results. You simply can’t do this one alone. There are too many factors. Collaboration is key, and the sooner we recognise we can’t do it alone, the more impactful we will be.
Promoted to a bathroom
I don’t know if there’s any meaning behind it, or whether it is just an amusing coincidence, but when I finally got to a point in my career where I was allowed my own office it turned out it was a converted toilet cubicle. My office still says on-call bathroom on the door, alongside one of my favourite things the team have ever given me, my Dame Elaine sign (they always joke it will happen one day). It is a rather compact space, but I love it, and at least they remembered to take the actual toilet out.
The irony of a blog post that starts with how much I hide in bathroom cubicles then discussing how my office is now one is not lost on me. Quite a lot of people don’t like it as a space, as it has no natural light or any ventilation. I don’t know if it’s because I’ve been hiding in bathrooms for way longer than I had a bathroom office, but I find it a really comforting space. I like the lack of distractions. I like being able to spin my chair and reach for anything I need. I like being able to listen to peppy music whilst I work, as I hate working in silence, and not having to worry about bothering others. To me, it’s sanctuary.
Being considered a bathroom expert
One of the things I didn’t realise when I started out as a Healthcare Scientist is how organically interests grow and end up turning into something more. I started involving myself in all things built environment and IPC, because I wanted to understand it better. I wanted to learn more. As time went on that wanting to learn led me to develop more and more questions, as I found gaps in the literature and questions I couldn’t find the answers to. Maybe because I am a scientist, those questions led me to create studies and collaborate with others to gain knowledge that not only solved some things but also created more questions. I’ve also had the painful experience of making bad decisions based on a lack of evidence to enable me to make better ones. Therefore, I think this area (water and water safety) is one that is often overlooked and yet is critical to all healthcare and healthcare environments.
One of the reasons it’s so easy to make less than ideal judgements and decisions in this area is that IPC teams get so little training on this. Most will know something about Legionella pneumophila and Pseudomonas aeruginosa, but very few will know much about other key organisms, such as atypical mycobacteria or Elizabethkingae. What can feel like fairly low consequence decisions based on aesthetic appeal, such as which tap you prefer, can have significant consequences down the line which might not be seen for years. This can make it hard to tie up cause and effect in order to lead to improved learning without external support.
I never aspired to, or meant to be considered an expert in this area, but somehow I have accrued some level of knowledge by being in a Trust that is always building, and having stayed in one place for 20 years to see the cause and effect in real time. For the same reasons, I’ve also published a few papers linked to ways to improve water hygiene, although only a handful.
The main thing I’ve done is establish the Environment Network as a way to share learning and talk through challenges, and more recently, a course that sits alongside it to help support those who are interested and don’t want to make the same trial and error mistakes that I did. I am far from an expert in reality. There’s too much to learn, and the landscape alters too quickly. What I am is intellectually curious and determined to try to learn enough that every decision I make it better than the last one.
Bathroom based recognition
I started this post talking about a Worshipful Company of Plumbers sponsored event at Mansion House and my bathroom based adventures. I thought I should finish it by telling you why I was there and how this transpired in case any of you would be interested in joining me at future versions.
As I said, there don’t seem to be that many people who work clinically who are interested in water safety, although I’m pleased to say the number is increasing. There are, however, amazing women working in this area from the microbiology perspective, women like Dr Susanne Surman-Lee and Elise Maynard. The brilliant thing about these women is that they are truly interested in engaging with others and also raising up other women. I first met Susanne 17 years ago as a trainee when she was working at UKHSA, she won’t remember the event but she made a definite impression on me, and I’ve known Elise for over a decade. They are my ‘phone a friends’ when I need expert advice. They also lead on a bunch of different guideline writing groups in relation to water, and over the years have been kind enough to include me so that these groups, which are usually fairly heavily engineering led, include a clinical perspective.
Over the years, we have written a few BSI guidelines together, and the one that I think is most useful to those of you out there in IPC is this one, BS 8580-2:2022 Water quality. Risk assessments for Pseudomonas aeruginosa and other waterborne pathogens. It has a wonderful table at the back from Elise that contains all of the kinds of organisms you are aiming to control and if there are any specific areas to be considered, such as Klebsiella pneumoniae and sinks. We’re currently writing a new one to help people make sampling based decisions, and one on atypical mycobacteria should hopefully start later in the year. Susanne also organises the Royal Society of Public Health water webinar series, and I’ve been fortunate enough to deliver a couple.
All of which ended up with me being here:
Worshipful Company of Plumbers Livery Ceremony May 2023
In 2022, I was asked if I’d consider becoming a Liveryman for the Worshipful Company of Plumbers, linked to my work on water and women in leadership. It’s been a fascinating process, and at some point I might do a blog post on it. Needless to say, I agreed and in May 2023 I was clothed in the Livery. One of the great things about joining has been to meet so many people who are also really interested in how we manage water better and differently. There are also so many different perspectives. At the Mansion House event, my one conversion ended up being the leader of a sustainability nonprofit who was interested in using STEAM (science, technology, engineering, arts and mathematics) approaches to change how people think about water. This strikes a bell with me, as some of the challenges in the healthcare setting are around people thinking of sink areas being ‘clean’, whereas they are frequently highly loaded with bacteria and therefore potential risk.
Members of my team now jokingly refer to me as Her Plumbship, and all plumbing queries are light heartedly directed my way. The thing is, in this area, none of us can do it alone. I’m not a plumber (despite what my CV says). Nor am I an engineer, an environmental microbiologist or sustainability expert. If we are to make things better, make thing safer and deliver on key goals like those listed by the UN, we have to come together. We have to embrace the fact that there is no such thing as a stupid question, be prepared to stick our heads above the parapet and be uncomfortable in our lack of knowledge in order to work towards a better shared understanding.
This month is the start of a painful re-entry into normal life. Normal life in terms of work demands, normal life in terms of commuting and normal life in terms of getting back to not eating party food and leftovers for at least 50% of our meals. Now, mummy Girlymicro, Mr Girlymicro, and I have done our fair share of celebrating over the last few weeks, including eating out at large catered events and throwing our own parties for friends. Clinically, norovirus is now giving us its cyclical peak, and there was also a lot of food related outbreak news over the holidays. I thought, therefore, that I would start this years IPC related posts with one on foodborne outbreaks and the kinds of organisms involved.
Food related sickness and outbreaks can be caused by a number of different microorganisms and through a few different routes. The two main routes are infection and intoxication, and these are related to the organisms that tend to be the causative agents. The foods that are linked to these routes are also different, and if investigating can give you an idea of what you might be looking for, especially when combined with presentation, both in terms of clinical symptoms and speed.
Infection vs intoxication
Intoxication based food poisoning is usually linked to rapid onset symptoms following the ingestion of the food i.e. a matter of hours. This is because the symptoms aren’t related to an infection based process, where symptoms are linked to the invasion and replication process of the organism. There are two main types of toxins, heat stable and heat labile toxins. Heat stable toxins can be problematic, as once present in food these cannot be removed purely by re-heating to an appropriate temperature. Heat stable toxins, such as those produced by Bacillus cereus, are produced when the bacteria are present, hitting the right temperatures then kills the bacteria but the toxins remain. This process can be exacerbated when foods are not rapidly chilled or are left at a temperature where the bacteria could grown, there is therefore a prolonged period when toxins could be produced. Toxin related food poisoning (intoxication) can be caused by both bacteria and fungi.
Infection based food poisoning is linked to the ingestion of the organism itself, and presentations are therefore usually delayed as the organism needs to infect the gut mucosa. Many organisms that produce toxins can also cause infection related symptoms if present in high enough loads, and if suitable temperatures for bacterial kill are not met. Infection based food poisoning can be due to viruses, such as norovirus, parasites, such as E. histolytica, as well as bacteria, and the risks are often related to food hygiene efficiency as well as production factors.
Patient management
Most food related illness self resolves and management is mainly focussed on maintaining hydration and electrolyte balance. There is usually a requirement to undertake a minimum isolation period of 48 hours post symptoms in order to prevent any ongoing risk of person to person transmission, even if the original acquisition is thought to be via a food related source. Isolation may need to be prolonged in relation to certain groups because of the risk of ongoing to spread to others, either through personal hygiene awareness or through work based activity.
Recommendations for the Public Health Management of Gastrointestinal Infections 2019: Principles and Practice has a lot more detail on the main organisms associated with foodborne illnesses and some of these requirements for isolation. I’ve attached a copy below, but the link is also here in case it’s useful.
If symptoms continue for period of a week or are especially severe it may be necessary to take samples in order to identify a causative organism in order to support patient management. When taking a patient history it’s important to capture any patient specific risk factors (see below section on risk groups), travel history, recent event attendance history and details of hobbies (such as preserving) that may impact of food ingestion patterns. Additional individual management options can include antimicrobials (antiparasitic or antibacterial) and for non-bloody diarrhoea without fever antidiarrheal agents.
How do these organisms get into food?
Organisms can get into food from numerous sources. They can be present in the environment in which the food comes from, such as manure that is used to fertilise salad plants can contain organisms, like E. coli, even more so if human waste is used. Food, such as oysters, can be contaminated as part of their life cycle as filter feeders if they are growing in an environment where they are exposed to animal or human waste, and so can harbour organisms like norovirus and become highly loaded. Food can also become contaminated as part of the production or manufacturing process, contaminated from other items that are produced in the same facility, contaminated from the processes, such as the water or preservatives utilised, or from failures in the preservation process that would normally have removed organisms that are naturally present linked to food.
Organisms can also come from the humans involved in the process. Those manufacturing or handling the food may be carrying or infected with organisms, whether symptomatic or not. A Staphylococcus aureus colonised person making sandwiches may contaminated the food they are making. An asymptomatic norovirus infected canteen worker could expose those being served food by unwittingly contaminating food and/or serving implements. In the case of bacteria, low level contamination from those producing the food may then be able to grow up to levels where ingestion results in symptoms if the processes are not well enough controlled.
Food processing and manufacturing
Most food preserving techniques aim to ensure that if contamination occurs during production or manufacturing it is not able to replicate to the point where the organism would cause symptoms in those who ingest them. Many preserving techniques aim to control organism survival or replication/loading via either temperature, cell lysis/resource availability or both. There are two main groups of techniques, either physical or chemical.
Some of these processes are more prone to risk of failure than others, both depending on the process and where is it being undertaken. When undertaken in food manufacturing, these techniques are usually undertaken under highly controlled conditions using the HACCP process in order to manage some of this risk variance:
Food preparation in the home
Obviously, none of us are following HACCP processes when we are preparing food at home, that doesn’t mean that there isn’t any risk to home cooking. One of the hazards linked to cooking at home can be the home environment itself. I’m still aware of people who wash out chicken or turkey cavities in their kitchen sink, unaware of the droplets that are produced and how they can then deposit on other surfaces, which are now contaminated whilst appearing visibly clean. Other hazards can link to the fact that most of us don’t have access to rapid (blast) cooling, and therefore when cooking big batches of food and putting in the fridge, the cooling process may not be fast enough to prevent bacterial growth. Also, in terms of equipment, I work in IPC and I’m a bit of a control freak so I possess things like meat thermometers, in order to ensure that meat has reached appropriate safe temperatures. I am aware that not everyone lives in this particular world, and so may not have some of these pieces of kit lying around.
Most of the time if you end up preparing food less well at home the consequences are non-ideal but not massively serious, however, if you have an ‘at risk’ member of your household or visiting then it becomes more important to focus on controlling these risk, both through the food that is brought and how it is prepared.
Food preparation (catering)
We’ve already talked a little about the HACCP processes that are put in place to control risk in formal settings. Catering can be a tricky area of risk, even if undertaken by professionals. It is one thing to undertake catering in your restaurant or a space you work in all the time. Catering however, is often undertaken in sites that are not the ‘home’ of either the professional or the average person. Catering equipment can be hired to serve food in church halls, for weddings or other special events. It can also be undertaken on beaches, in forests and other remote locations with variable levels of power to support refrigeration. This can mean that control processes, such temperature control, are undertaken in atypical ways, such as temperature control using ice packs, which will have variable efficiency depending on external factors, such as ambient temperature.
Home catering for parties also brings risks. I love to throw an afternoon tea party for charity, but that means that I am suddenly trying to put waaaaaay more in the fridge than I normally would. Food may be out on a table for a number of hours. Some of the food may also be high risk, such as cheese or smoked fish, and it will be next to less high risk foods. Also, if you are not used to prepping food for large groups, you may inadvertently increase risks by the order in which food it prepped. That is without the risk of people bringing food to contribute to yours which you don’t know the origins of, or people picking up food with fingers and therefore increasing risk of spread if they have anything onboard.
Food storage
Once all of that catering is done, you are then left with a decision, what do you do with all the food that is left? Do you then try and shove it all in your fridge or freezer? Do you give it people to take home in Tupperware pots? How much have you taken into account the length of time that food has been non-temperature controlled? What does that do to the use by? Is everyone aware of any re-heating requirements or the dangers irrespective of re-heating of intoxication?
Issues with food storage are true not just for party catering, but also for batch cooking, something a lot of us are doing more and more of now the weather is colder and because food it more expensive. Foods like stews and rice dishes, which are high risk for intoxication, are also the kinds of foods that fulfil a lot of batch cooking requirements. It is really important to bear these risks in mind, ensuring rapid cooling and that temperature is monitored appropriately.
This also extends to ensuring that even dry goods are stored appropriately. We’ve all been there when we’ve found the pack of spice that 15 years old. Spices, canned goods and other preserved food have been identified as the source of outbreaks, and even when originally in good condition can become a risk if not well maintained, such as dented cans or if moisture has gotten into packets.
What kind of incidences are we talking about?
Over the Christmas period there have been two well publicised food related outbreaks, one linked to E.coli in cheese and one linked Cronobacter sakazakii (previously Enterobacter sakazakii) in infant formula.
BBC News – One dead after E. coli outbreak linked to cheese
This outbreak was linked to the presence of STEC toxin producing strain of E. coli. This leads to an intoxication that can impact of kidney function. Although not stated, elsewhere it was reported that the cheese may have been made from unpasteurised milk, removing one of the stages used to control organism risk in food production.
Advice for individuals from UKHSA included:
“Washing your hands with soap and warm water and using bleach-based products to clean surfaces will help stop infections from spreading. Don’t prepare food for others if you have symptoms or for 48 hours after symptoms stop.
“Do not return to work or school once term restarts until 48 hours after your symptoms have stopped.”
The other recent recall was linked to possible contamination of infant formula detected at manufacturing. Formula feed outbreaks linked to Cronobacter sakazakii have been noted in the past, with a large outbreak in France being the last large scale event. Infection does not just lead to GI symptoms but is associated in some patients with presentations such as blood stream infection and/or meningitis.
The formula included in this recall is mostly used in healthcare or is prescribed to individuals. This makes it critical as it is likely to have been given to an ‘at risk’ population. Milk related contamination is particularly challenging as heating impacts the nutritional content of the milk and so use of thermal risk reduction is not straight forward. Some hospitals, such as the one where I work, undertake an additional step, pasteurisation, for any formula feeds due to be given to high risk infants because of this well acknowledged risk in order to support infection risk reduction.
BBC News – Baby formula recalled over bacteria contamination fears
Current and Future Perspectives on the Role of Probiotics, Prebiotics, and Synbiotics in Controlling Pathogenic Cronobacter Spp. in Infants October 2021 Frontiers in Microbiology 12
There are obviously multiple examples every year of foodborne risks linked to contamination at source or HACCP failure, but these are the ones that have been most recently featured in the national press.
Are any groups at higher risk?
Although food related infection or intoxication can impact anyone, certain groups are more at risk of significant symptoms requiring treatment or are more at risk linked to certain organisms in terms of presentation. These groups are your very young, very old, the immunosuppressed and pregnant women. The very young and very old are more likely to need support linked to dehydration, and all 4 groups are likely to be less able to mount immune responses to invasive infection. The immunosuppressed and pregnant women have specific guidance linked to avoiding high-risk food groups because of severity of impact if infection occurs.
One particular organism linked with significant infection risk for pregnant women and the immunosuppressed is Listeria monocytogenes.
Microorganisms 2022, 10(8), 1522
Listeria crosses the gut wall at locations known as Peyer’s patches, and from there invades lymph nodes and blood. Once in the bloodstream, it can progress to cause meningitis/encephalitis by infecting the brain. In pregnant women it can also cross over into the placenta, where it can cause infection in the foetus/unborn child. Foodborne listeria outbreaks have been associated with a wide variety of foods, but are often linked to preserved foods and cheese.
There are a number of stages to investigating foodborne outbreaks. Initially, there will need to be some sort of flag to suggest an outbreak event. This is usually a number of people attending GPs or A&E linked to a single event, an uptick in samples positive for a specific organisms that is noted through lab reporting, or any cases of specific reportable organisms which will then get followed up.
Depending on the circumstances, a combination of the following steps will be undertaken:
Patient questionnaire (case)
Questionnaire of those who attended the same event but did not get sick (control)
Sampling and microbiological testing of possible implicated food, if still available
Sampling of the production environment, such as factories or restaurant kitchens
Investigation needs to be undertaken to identify the target food or batch as most production facilities will make more than one kind of food and will have multiple batches. If the outbreak is linked to a specific event, multiple types of party or other food is likely to have been available. Getting more information about what those who got sick ate vs the others enables you to narrow down what the culprit might be.
Once you have your questionnaires, it’s time for a little bit of stats. This enables you to calculate something called the relative risk for the cohort. The cohort being all those people who were at the same event, ate at the same restaurant, brought food from the same factory etc. This will include those who became unwell and those who did not. For each type of food or batch you can calculate a ratio of the risk of disease (infection/intoxication) in people who have been exposed (ate that food) compared to those unexposed (decided that food was not for them).
You then get a list of risks for different food types eaten. So if the following food was available at our event you can then undertake the calculation:
pigs in blankets
mini fish and chips
turkey and stuffing roulade
mini pavlova (with cream)
cheese pinwheels
If the number if >1 then it indicates and increased risk, if RR = 1 then it doesn’t impact on risk, and if RR <1 then there is a risk reduction. So in the case of our party food:
pigs in blankets RR = 1
mini fish and chips = 0.98
turkey and stuffing roulade = 1.73
mini pavlova (with cream) = 1.1
cheese pinwheels = 0.99
In conclusion………the turkey probably did it!
I hope that’s helpful, I know there’s loads more that could be covered, and if you are interested in anything in particular drop me a comment and I’ll see if I can post a follow up. The main take away is that there are multiple organisms that can cause foodborne infection/intoxication, and whether it’s home or out and about we can all be impacted. For most of us, it’s an unpleasant but low consequence event, but there are are people and populations where the outcomes can be much more severe. So, if you’re ever asked to complete a questionnaire please do so, and don’t ignore those news articles that tell you to throw an item away as it’s not a risk worth taking.
As I continue the slow road to feeling more like myself again I thought it might be nice to have a guest blog from the wonderful Sam Walker on some of the things that have been happening in the research Girlymicro world, so you know I haven’t been entirely resting on my laurels and eating copious amounts of chocolate. One of my favourite papers ever is based on the release of cauliflower mosaic virus DNA into a ward space, to support prospective tracking of where organisms go, instead of trying to guess based solely on where we find them without origin data. Due to a number of technical factors this approach to improving environmental transmission pathways hasn’t widely been repeated………..until now!
Sam is a Doctoral Research Student whose research focusses on the development for environmental surface monitoring protocols to inform clinical risk assessments and infection control procedures. His project aims to develop an evidence base for the presence of nosocomial pathogens in the hospital environment, as well as model the transmission of pathogens in clinical spaces. He obtained an MBiol degree from Aston University in 2020, with projects focusing on C. difficile spore germination.
Infection Control Research
“I imagine the swabbing part will be easy, it’s the data processing I’m worried about”. I think I said this about a month before the largest, and final, sample collection campaign in my PhD project. Famous last words.
A little bit about me – my name’s Sam and I’m one of Elaine’s PhD students. I’m finishing off my third year now (crunch time!). My project focusses on developing evidence-based surface sampling guidance to inform infection prevention and control practice. Practically, this involves collecting a range of samples from different clinical spaces and seeing that they can tell us in terms of microbial communities and microorganism dissemination, then using this information to target guidance for designing the most effective surface sampling protocols. In order to best inform this, we designed a study which looks at the movement of microbial surrogate markers through several different wards at Great Ormond Street Hospital. This involved a lot of preparation and many evenings swabbing sites across four wards. As of last week, all this sampling work has finished and I thought I’d share a few reflections on what the experience of conducting research in an active clinical space was like.
Working across settings is amazing!
For many projects focusing on clinical practice, particularly ones relating to IPC, working in collaboration with a clinical institution is absolutely essential. As my project involves collecting evidence from clinical settings to then process and develop into guidance, in my case this work wouldn’t be possible without this collaborative approach. As the end goal of my project is guidance that will inform clinical practice, not only is it important that the evidence is gathered from clinical settings, but it’s essential we understand the routine challenges faced by IPC teams. We can design the best set of guidance with all the technical detail in the world, but if we don’t take into account every day IPC challenges and what implementing this guidance will actually look like, then in a way it would fall flat. Being in the clinical space also opens up the possibility for conversations with the people who live and breathe IPC all day – the hospital staff! Informal discussions we have had over the course of this most recent sampling project have given me completely new insights and ways to view the work we’re undertaking which I never would have thought of otherwise! Getting this insight from working in clinical settings will ultimately improve both the quality and utility of the work we produce.
Stepping out of my comfort zone
As a lot of project is lab-based, the trips outside of this setting into clinical environments can be a bit of a shock to the system. I’m used to, and probably most at home in, a quiet laboratory space with a few other people at the most, maybe the odd visitor and the trusty PCR machines. The majority of the time I make the journey from UCL to GOSH, it’s to meet either with Elaine or other members of the IPC team, or maybe to pick something up from the microbiology labs there. When it’s time to collect samples however, this is a completely different experience.
The units we looked at in this most recent piece of work we did were two outpatient and two inpatient wards, serving different patient populations. One of the first things I really noticed was just how different these wards all were. I knew that there would be some big differences, for example I knew that the cardiac intensive care unit would be a very different experience to the oncology day care unit. What I didn’t necessarily expect however, was just how different the two outpatient wards would be from each other, and how different the same ward could be on different days.
With these differences came a different way to approach the research at hand. For the outpatient units, that often meant waiting until all the bed spaces were free so we could go in and collect the samples from the environment. This wasn’t always possible though, and sometimes we just had to accept that we weren’t going to get all of the samples we set out to gather. This took quite a while to get used to – my inner laboratory scientist was wincing at the thought of lost data points. Being able to put this to one side and carry on was a skill that took a while to master, particularly when sampling with a team. No-one will thank you when you’ve been on the ward for an hour and a half and you propose “just waiting a few more minutes” to see if a bed space will become free. Having that skill to just move on however turned out to be very useful when collecting the data, as it meant we could focus more effort in the areas we could collect samples from.
All this boils down to how the space is used completely differently. The hospital is first and foremost for providing care to patients, and as a researcher I have to acknowledge that I am a guest in the space. Understanding and accepting that we won’t always be able to collect all of the 65 or so samples we planned to on a given day is just part of the process when conducting sampling in the real-world hospital setting. At first, I remember feeling like this may be frustrating when it came to analyzing the data, and that it would make interpreting my results harder due to data gaps. However, looking back on it now, I actually feel it makes understanding the story the data tells easier, and much more insightful. Being able to relate the information we gathered to how the space was used at the time of collection, even where samples could not be obtained, just makes the story all the more applicable to real clinical practice and, in this case, how microbes could move through the clinical space under all sorts of conditions.
Anticipate the challenges
While embracing the dynamic environment of the clinical space is really important for putting data gathered in these settings into context, it doesn’t mean that there isn’t a fair share of challenges with it. Before I began the sampling campaigns, both my supervisors absolutely insisted that I pre-planned every tiny detail. Down to the exact number of extra swabs I would take for each day. And I cannot think of better advice when it comes to performing this sort of work. Planning is absolutely everything. One of the reasons missing some data points during collection didn’t impact the overall quality of the data was because we anticipated that we may miss some points each day, so planned to take extra to account for this. We planned a detailed sampling sheet, so we could not only check off samples as we took them, but could make notes as we went around the ward on the environment to help with the downstream analysis. I cannot stress it enough; thorough planning made the whole experience so much better.
One challenge of conducting this piece of work was the intensity of the settings. I have a very much academic background, having done my MBiol degree and gone straight into my PhD. In other words, I have no clinical training whatsoever. This wasn’t so much of a problem in wards which were not high dependency, however I really noticed this lack of clinical exposure when we did the sampling in the cardiac intensive care unit. I knew it may be a difficult experience, given the nature of the ward we were going in to, but it still was a shock the first day of sampling there. I’m incredibly grateful for the team I did this part of the work with, who had the experience to navigate the space as well as make sure I was alright being in the setting. I think that this support, alongside taking some time to reflect on the overall experience, was invaluable for this particular component of the work.
This leads me on to the other absolutely key point for doing this sort of research – having the right people with you. As academics, we often won’t have been trained in clinical practice. This can not only make some clinical spaces quite intimidating, but also can make them hard to read. For example, without a clinical understanding of what is going on in a bed space, it can be hard to know whether to ask if it’s alright to take a swab of the bed rail quickly, or if you should leave the space and move on. Having people with you who can help read these situations is so important, both for help with collecting the data but also for supporting the researcher. Another massive benefit I noticed was the links formed between me, the researcher, and the ward staff. Having someone involved who has experience in both worlds can really help break down any barriers on entering the space and help everyone understand the work that is being done, and how it relates to the ward.
Top tips for laboratory researchers gathering samples from clinical spaces
So, having said all that, my top tips on performing research in clinical spaces as an academic are:
Planning is everything!
Anticipate and embrace the unique challenges of this sort of research
Have a good team who can support you in the clinical space
And finally, get involved! Undertaking research in clinical settings is very rewarding and I would highly recommend it wherever possible!