This months posts all have a bit of a risk assessment theme, possibly because I’m back in the land of SARS CoV2 increased prevalence but also because I’ve been contemplating how moving away from a risk assessment led approach to a testing led approach has impacted on how willing people now are to undertake risk assessment. More on that maybe later in another post. What on earth has risk assessment got to do with environmental Infection Prevention and Control? Well frankly it’s the bit that’s often forgotten in terms of our clinical risk assessments. There are also lots of engineers out there making engineering risk assessments for environmental control, and they (for the most part) don’t contain anything clinical. Ventilation and surface transmission have featured linked to the control of SARS CoV2 but I wanted to write something to talk about the environment and environmental risk outside of this, partly because I can’t face writing another SARS CoV2 post for the sake of my mental health, it’s just hard right now.
So back to happier times and how my passion for environmental IPC got started. I joined the IPC team in 2007 after my first three years of Clinical Scientist training. I had a wonderful IPC doctor who was full of vision and aware of the need to increase the scientific technical skills within the team. The thing was that the rest of team wasn’t quite ready to embrace what was a very different approach, all very understandable, at that time IPC was very much focussed on hand hygiene and audits. So I spent some time with the various consultants and it became really obvious to me that there was an area where the introduction of some standardised methodology might immediately make a big difference. Environmental Infection Prevention and Control.
The team themselves were innovative in their approaches to IPC and had embraced environmental screening during outbreaks. The issue with it was there was a one size fits all approach, so organisms were not considered differently in terms of where and how the screening was undertaken. The sampling of rooms and wards involved taking a handful of swabs and just screening places that came to mind. There wasn’t work done on how many swabs needed to be taken within a certain size room in order to have sufficient sensitivity for detection or identification of high risk sentinel sites and how these might need to be changed based on organism. You’re negative predictive value of a screen without these considerations might not be as strong, leading you to incorrectly rule out a role for environmental transmission.
How did all of this work?
My role in the team became very much about how we solved some of these challenges. Undertaking work in patient rooms pre and post clean to define how many swabs needed to be taken. Take too many swabs and you’ll waste resources in both time and consumables, take too few and you’ll end up with false negatives leaving you to miss out on key risks as part of your risk assessment.
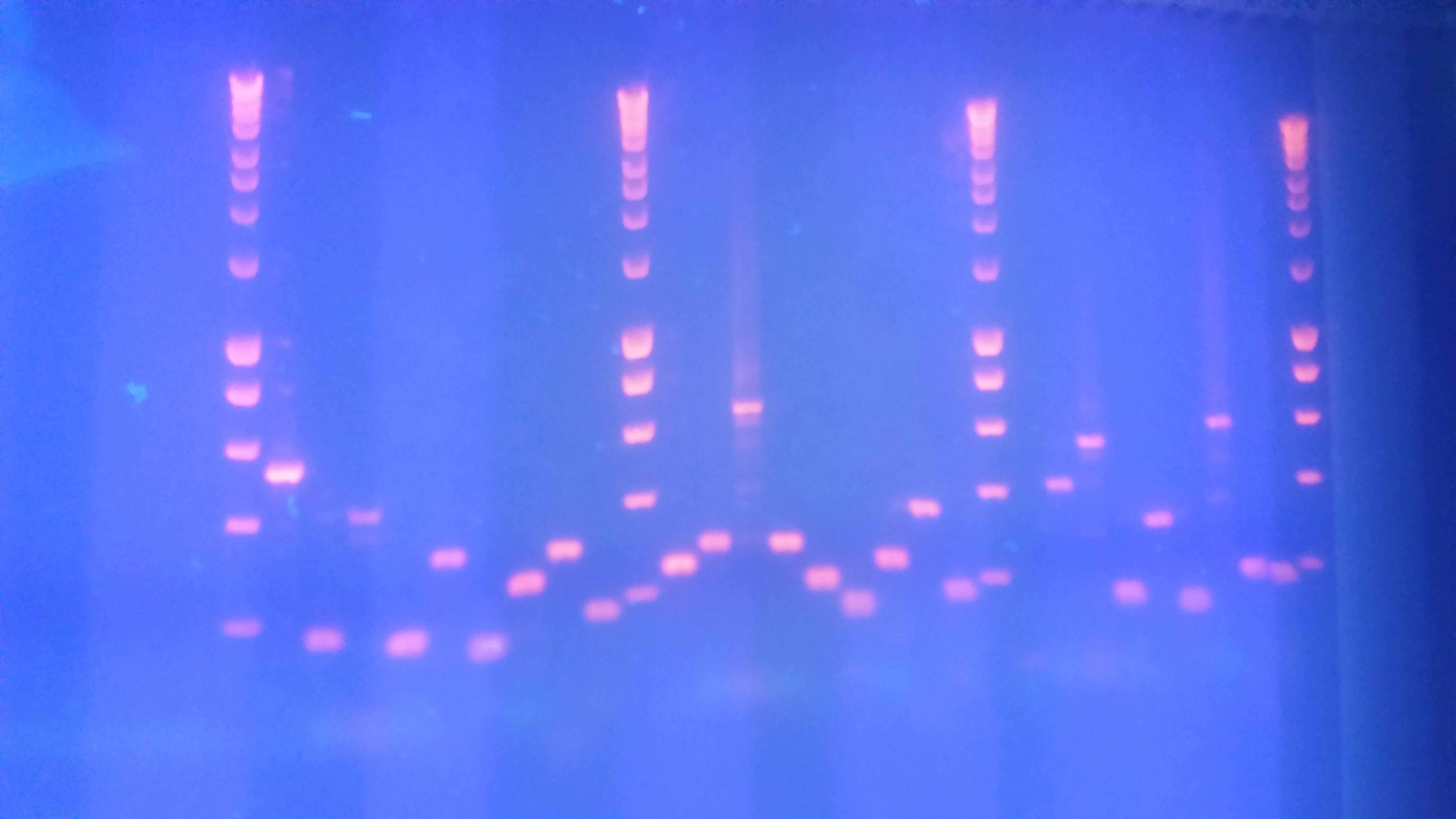
One example of this was looking for adenovirus in rooms post clean. Adenovirus can have serious consequences if acquired during bone marrow transplant, and unlike in adults children won’t all have had some form of prior infection. Mortality rates can be as high as 50 – 80%, depending on underlying condition, for a new acquisition. Combine this with the fact that adenovirus can survive in the environment for >3 months and patients can shed loads in the millions via both stool and respiratory secretions you can see that this might be an issue for infection control. I initially started out screening 24 – 30 sites in rooms and then gradually used data from both pre and post cleans to establish sentinel screening sites that are now screened in every room after cleaning to ensure that the next patient is not exposed to environmental transmission risk. We now screen 12 sites, 10 sites was just on the edge of sensitivity, in that if the room failed only 1 site would fail when screening 10 sites. By screening 12 sites if a room fails it tends to fail in 2 – 3 sites which means that the screening isn’t sitting right on the edge of sensitivity.
Even choosing the methods to screen with proved to be tricky, I had to specially develop methods in terms of what kinds of swabs to use, and how to introduce controls that would enable me to understand if the very cleaning agents used to screen were inhibiting my PCRs. Environmental screening is both very similar and very different to clinical processing and so to undertake it properly requires a certain level of work in order to modify the processes to make sure that results reflect actual contamination levels rather than providing false reassurance.
I felt like I’d finally found both my place and my passion. A place where I felt that my scientific background really contributed to the team and could be used to make things safer for patients.

Eventually way back in the mists of time, otherwise know as 2010, I started to develop further some of the work I’d been doing with the team and embarked upon an NIHR funded fellowship looking into the role of the environment in transmission of healthcare acquired infection. The more I learnt about how the role of the environment was considered to be coincidental, the more my own data demonstrated that that just wasn’t true, at least within the paediatric environment. I’ve written just recently about why paediatric IPC is different and the environment and the way that patients interact with it are definitely a big component of that.
So what do I mean by the environment?
I set out to talk to more people from different backgrounds about the questions that I had about environmental IPC, this eventually led to me and others establishing the Environmental Infection Prevention and Control network so that we would have a place to continue to have these conversations.
The first thing we talked about is what is the environment? Is it just surfaces? Does it include the surfaces of medical devices? How do things like water and air fit into all of this. Some of the things I include when I talk about the different categories are below. In terms of medical devices I think of these linked to decontamination, which I will post about at some point. This field obviously has a lot in common with environmental IPC but has been longer established and came about because those items have an acknowledged patient risk, whereas the rest of the environment has been slightly ignored in risk assessments.

Most of the standards linked to environmental IPC are either set by engineers, and therefore are based on infrastructure rather than a clinical risk assessment. The other standards include things such as visibly clean with no dust, dirt or debrie. Admittedly if your surface is visibly dirty it is unlikely to be microbiologically clean but it is also possible to have a surface that appears visibly clean and still has pathogens present, they are afterall…………microscopic and not visible to the naked eye. This means there is a real challenge for IPC teams where they need to work between standards with little guidance to really tackle the role of the environment in transmission……..at least back then in 2010. I’m glad to say that this is definitely changing but it still presents plenty of challenges.
Why is managing the environment so hard?
First and foremost it is the thing that everyone interacts with, patients, visitors and staff and that often no one thinks is s risk. Visitors won’t think twice about putting a handbag on the floor and then putting it on a bed so their friend can get something out. How many times have you seen a WOW or portable equipment rolled between rooms, including highly resistant organisms, and rarely have I seen anyone clean the wheels before it goes into the next bedspace. You can easily see how bits get moved about.
We obviously advise everyone to wash their hands in order to control risk. This means that most people associate sink with being the ‘clean’ items in bed spaces. Whereas in a paediatric hospital up to 60% of the sink backs may have faecal flora as the parents are all in nappies. This means if you do what I have had to do, which is balance a clipboard on the back of a sink to permit hand hygiene, you may have just covered your clipboard in bugs that you will happily move to your next location, your pen, your face. This stuff is hard and the solutions are far from straight forward, especially when you can train staff but many of the interactions are linked to people you can’t easily educate like visitors and patients.
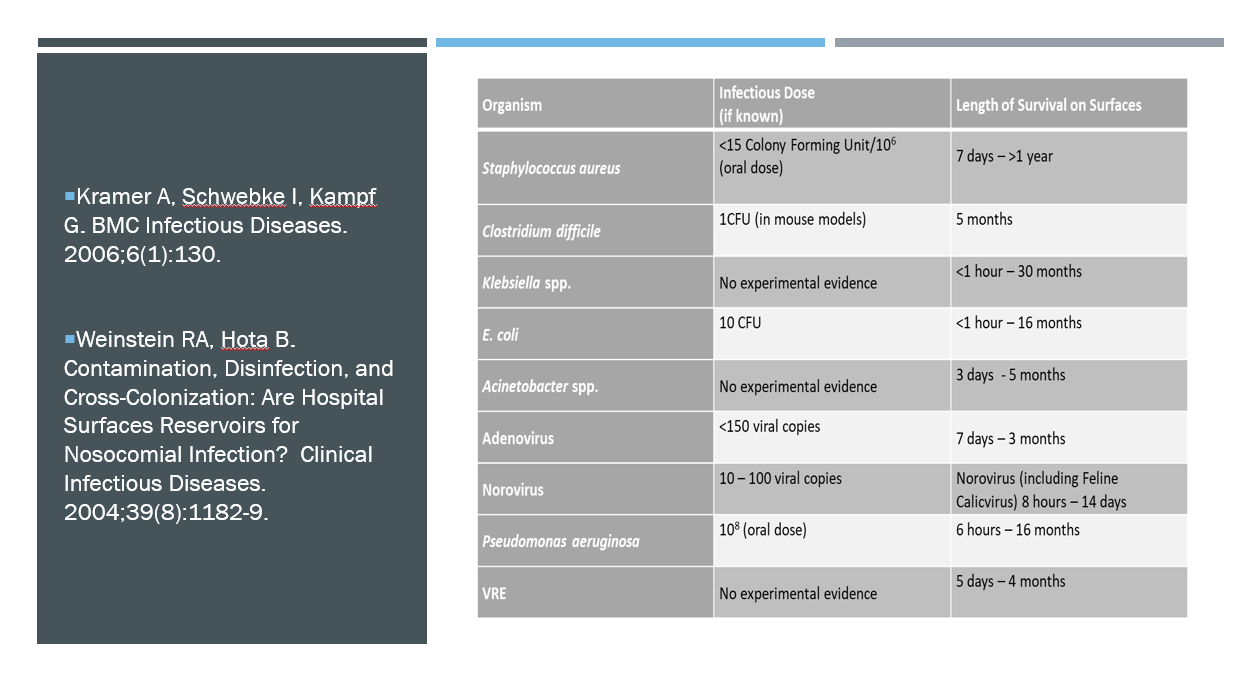
Another reason environmental IPC is hard is that it sometimes breaches the basic rules of outbreak investigation ‘linked in person, place and time’. As you can see from the table below organisms once in your environment can survive for a very long time. That means you may just see single cases split over prolongued periods and so it can be very difficult to recognise you have linked cases, especially if you don’t have access to molecular typing.
Finally, even when you get to the point where you think you have a problem it can be difficult to have an environmental monitoring scheme that can rule in or rule out the environment as a source. These can’t generally be developed well on the fly as part of an outbreak surveillance. They really need to be developed and tested, ideally as part of surveillance systems, outside of outbreak scenarios. The problem with this being is that ut is resource intensive and you don’t even know what organisms might be there to judge the success of your monitoring method. You don’t know the dose and initially inoculum location to judge spread and how well your system is working.
How do we understand this better?
Myself and others have been working to create different types of markers in order to help us gain some direct rather than the indirect evidence that learning from outbreaks gives us.
You can do this is a number if different ways. We are working with an artifical marker developed from cauliflower mosaic virus that then allows us to inoculate different markers across units in single locations. We can inoculate items only touched by staff, or families and then monitor the spread out from this single locations across the units. Because we have control of the dose we are putting down we know how much cleaning/hand hygiene will be required for removal. We also know how long it will last. This means that we can investigate transmission routes and intervention failures in a controlled way to better inform our response to outbreaks, as well as making the whole thing safer by better understanding what we are doing well and where we could improve.

Other people are doing great work with visualisation techniques, both to help people understand risk better but also to work to improve design in order to make things safer before they even get into the healthcare setting.
How has it changed my practice?
Without this work I wouldn’t have the amazing job I have today, but more importantly than that I think our environment would be more risky for patients. When we first started screening rooms post adenovirus positive patient discharge more than 50% of them were visibly clean and met the national standard, but had adenovirus still present (we clean with chlorine that degrades free DNA). We now are also doing weekly screening of the communal areas of those wards as it has shown that we pick up intervention failures by a screening failure, hopefully before it is seen by a patient acquisition.
We have an entire policy that includes how we respond to patient cases linked to environmental IPC. If we get Klebsiella acquisitions we screen sinks responsively as sentinel sites, as we’ve found that if the sinks are negative we don’t find it elsewhere in the environment and its probably a different route. If we find it on sinks then we undertake a wider screen.
We’ve also learnt the hard way that you also need typing to support picking up those grumbling transmission chains and so have done a bunch of work to develop in house typing pathways, still as ever in progress.
Finally we’ve launched ward manuals so that our clinical teams get teaching and have information on how the water and air work on their wards, as well waste etc. Environmental IPC is a team sport and if you don’t work closely with the people that are effectively living in the space you will never succeed at making things safer in the long term.
Anyway, if any of you need a sleeping aid here is my PhD thesis on this topic (health warning it’s long and may not be all that good). Also some of my papers linked to this are uploaded here. Finally, if this has really sparked your interest have a look at the Environment Network website which has more info. I hope you will learn to love the world of environmental IPC just a little and even if not appreciate how important it can be to consider when you are thinking risk assessment.
All opinions on this blog are my own