
Well my friends, it’s been an age. I think I have a reasonable excuse but I am sorry to have left everyone in the lurch by not being well enough to post. I’ve been laid up with Shingles. It was the first time I’ve had it, although as many as 1/3 of us (who have previously had Chickenpox) might have it at some point in our lives. My father pointed out that this whole event might be karma (I believe he was *mostly* joking) as he had Shingles for the first time earlier this year and I responded as a typical medical child in terms of management, without really acknowledging the pain and discomfort. I’m now 4 weeks in and functioning OK most of the time on pain killers but it has certainly been much more of an experience than I had accounted for when I saw the rash appear. Working in what I do I knew a lot about the Shingles experience on paper. Having now been through it however; I thought I would share not only some Shingles facts but also about the difference between ‘knowing’ and ‘Knowing’, as there are probably lessons to be reminded of for all of us when we see all our patients (or in my case supporting my father).
What is shingles and how is it related to chickenpox?
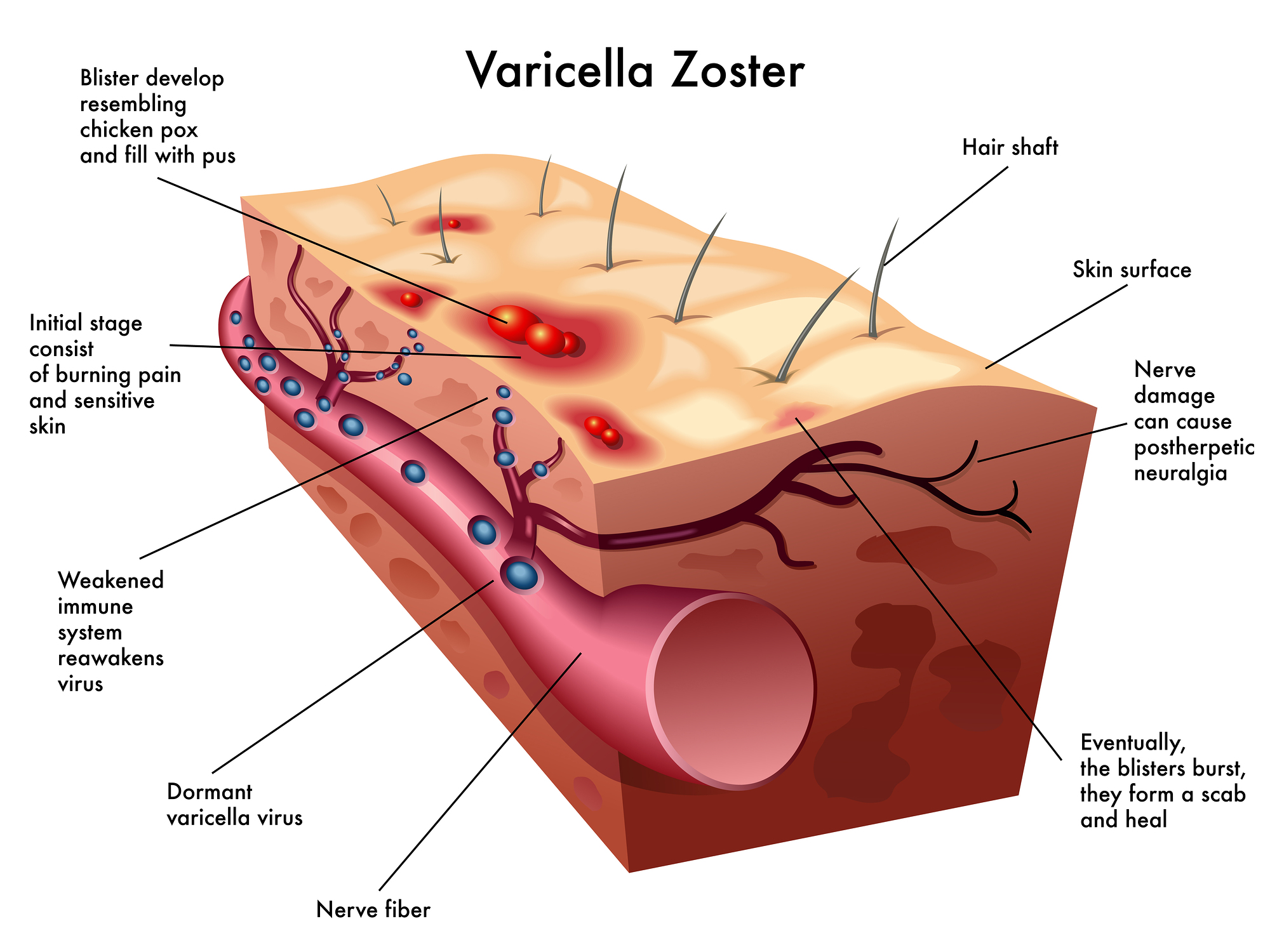
Shingles, otherwise known as Zoster, is caused by the Varicella Zoster virus or VZV. VZV is also the causative agent of Chickenpox, which is also known as Varicella. VZV looks like a fried egg under electron microscopy (a high powered way of viewing virus) and is part of the human herpes virus family, related to the same viruses that cause cold sores. Chickenpox and Shingles are intrinsically linked, with Varicella being the primary infection and Zoster being the reactivation of the virus.

What do these terms actually mean? Well, to ever get Shingles you need to have had Chickenpox at some point in your life, you can’t get Shingles without ever having the other. Once you have been infected with the virus for the first time (primary infection) and develop Chickenpox the virus then goes dormant when you recover in the nervous system (trigeminal and dorsal root ganglia). The virus is held in check (held dormant) and stopped from replicating by the immune system. It is when this immune system fails to hold the virus in check that it begins replicating again (reactivation), leading to the development of Shingles.
Most people is temperate climates i.e. non tropical, tend to get Chickenpox in childhood, but the infection is much more severe if acquired in adulthood. When you get your first infection you are infectious by the respiratory route for 48 hours before the vesicular (pus filled) lesions appear. After this the main infectious route is via contact with the rash itself, although some groups are still an airborne risk. Those exposed to the virus have an incubation period of 8 days (10 till rash appearance) – 21 days, with up to 28 days if prophylactically treated as a contact. Groups such as the immunosuppressed and pregnant woman are at increased risk of complications, such as pneumonia if infected.
Shingles presents in a similar way to Chickenpox, but is more localised. In my case I had sore and painful area on my back, which over the course of ~ 5 days spread around to my front, all on my right side. On Friday I went shopping with my mum and when I arrived home at 5pm I was so exhausted all I could do was sleep. I wasn’t feeling great the next day and by the evening the painful area of skin began to be itchy and I noticed a small red patch. I’m super allergic to just about everything under the sun so I assumed it was a local reaction. When i woke the next morning the rash had spread and I had a characteristic set of lesions, which meant I called 111 and got a referral for treatment. The pain then increased alongside the itching and 4 weeks later I am still suffering from radiating pain down my right arm, sensitive and painful skin where the rash has just about healed and tiredness.
How is it diagnosed?
The Shingles rash is fairly characteristic. It appears in a band along something called a dermatome (see image). The dermatome where the lesions are present are linked to the nerve where the virus has reactivated and is replicating, which leads to the virus travelling to the skin and forming lesions. The pictures of the rash below are some of my lesions on day 1 when I presented to the GP. Over the course of several days more lesions appeared and the rash continued to spread, in what we call cropping. It always stays on one side of the body and is highly localised.



Often, as the presentation is fairly clear, diagnosis can be made just by taking a history and examining the rash. Vesicular fluid can also be taken from the lesions themselves by removing the top of the lesion and using a swab to get at the fluid; which is then placed into viral transport medium (VTM) for further processing. Historically this was via tissue culture and visualisation of the virus, but more commonly now is by polymerase chain reaction (or PCR), so looking for the DNA of the virus itself. This is much more sensitive and rapid. These additional tests are usually only undertaken in cases where the presentation is less clear cut i.e. the immunosuppressed or to allow follow up in case of vaccine failure/response.
What is the treatment/management?
I hate going to any form of healthcare, I think I’ve mentioned this before. The fact that I called 111 was therefore a huge thing for me, so why did I? One of the biggest risks linked to Shingles is the risk of post herpetic neuralgia i.e. nerve pain. There has been data collected to show that treatment, in the form of aciclovir, can help reduce the risk of this, but only if commenced within the first 72 hours. A Cochrane Review in 2014 stated that oral aciclovir did not significantly reduce the risk of long term pain but helped in reducing it during the 1st 4 weeks. My rash was so classic that I knew either way that I needed to ensure I started treatment as soon as possible for either outcome to be impacted.
Interestingly when I said to my father that the pain could easily last 6 weeks + I didn’t know why he sounded so horrified, now I do. Although the pain hadn’t properly kicked in at the point where I got treatment, if it hadn’t started to reduce by the point I’m now writing this I wouldn’t have known what to do. One of the main delays in getting any blog out has been the significant pain when using my right arm, and I’ve only just been getting through work. This blog for instance even now has had to be written in small chunks across a day, whereas I would normally have just knocked it out. I am therefore super glad that I started treatment as soon as possible, even though the tablets were ENORMOUS!

How do I stop myself having a recurrence?
There are vaccines available to help prevent Shingles which are aimed at those aged 70 to 79. The vaccines should aid in prevention of shingles for ~5 years and there are 2 shingles vaccines used in the UK:
- Zostavax, a live vaccine given as 1 dose (similar, but not identical to the Chickenpox vaccine)
- Shingrix, a non-live vaccine given as 2 doses, 2 months apart (used for those people who can’t have the live vaccine)
I have spoken previously about having poor viral immunity and so it’s been recommended that I should consider having the Shingrix vaccine by my local immunologist; which may be a way forward. The main way to reduce the risk of this happening again however is to learn to take better care of myself so that I don’t get so run down. This is easier said than done, being an Infection Control Doctor during a global pandemic, but I need to make room to sleep and at least eat better when I’m not on service. I always worry that if I stop I may never get going again, but this recent experience has shown me that if I don’t make time for some rest and relaxation by body will take that choice away from me.
Top tips:
- Beware of whom you come into contact with whilst you have Shingles, non Chickenpox immune people may be at transmission risk
- Make sure you loosely cover the rash if you can to prevent risk of contact transmission to others
- If you have a rash develop on your face ensure that you see medical support
- If you suspect you have Shingles make sure you get it reviewed within 72 hours to support management
- If eligible for the vaccine make sure you get it to reduce your risk of developing Shingles in the first place
- The pain is substantial and if you are a daughter, probably don’t minimise it’s impact to your father 🙂
Anyway, I’m back, even if not 100% and I’m so glad to be posting again. I may just need to take it a little slower for a while. If you are on the edge of exhaustion, learn the lesson I did not and take some time for you, you owe it to yourself!
All opinions in this blog are my own.

Hope the pain recedes xx
LikeLike
Thank you 🙂 It’s just time I guess, every week it get s better
LikeLike