Dr Claire Walker has been a paid up member of the Dream Team since 2013, token immunologist and occasional defector from the Immunology Mafia. Registered Clinical Scientist in Immunology with a background in genetics (PhD), microbiology and immunology (MSc), biological sciences (mBiolSci), education (PgCert) and indecisiveness (everything else). Now a Senior Lecturer in Immunology at University of Lincoln. She has previously written many great guest blogs for The Girlymicrobiologist, including one on turning criticism into a catalyst for change.
What may be less well known, even to regular readers of this blog, is that she did her PhD on finding genetic diseases, and as this ties in so well with the recent blog series I’ve been doing on DNA I thought having a guest blog from Claire might be the cherry on top of this particular ice cream sunday!
If you’ve missed any of the blog series of posts, especially if you want a refresher on how DNA works before reading about Claire’s work, I’ve included links to all the posts the below:
Having spent some time covering what is however, I thought I would follow up with a couple of book reviews that focus on how the world of DNA, DNA editing and DNA interpretation could change the lives of everyone involved.
When I was 26 I finished my Clinical Scientist training and was offered a full-time position at the hospital I trained in, with a good pay increase and a view to becoming a laboratory manager in the next few years. It was a great gig with a lovely team, good earning potential and support to further my clinical training. Unfortunately for them, I had just completed a secondment to a famous children’s hospital and had my mind absolutely blown. I had seen how immunology was being influenced by the study of human genetics, at the forefront of the field with cutting edge techniques which seemed, frankly, indistinguishable from magic. Suddenly, working in adult rheumatology and learning how to manage NHS laboratory budgets just didn’t seem so interesting anymore. So I turned down the job, went home, looked my husband in the eye, and said the words he’d been quietly dreading ever since I’d first jumped from environmental microbiology to human immunology: ‘I think I want to retrain… again.’
I applied for a PhD in genetics and immunology at University College London Institute of Child Health. Specifically, I focused on children with rare syndromes that didn’t have a clear diagnosis often called “syndromes without a name.” These kids and their families had often been on a long and frustrating diagnostic journey, seeing specialist after specialist, with no real answers. That’s where exome sequencing came in. By reading the protein-coding parts of the genome — the exome — we hoped to find clues hidden deep in their DNA that could point to the cause of their symptoms. Think of it like a high-stakes game of genetic detective work. Each patient’s exome was a puzzle, and sometimes, we’d find that one variant that explained it all. Other times, we discovered new candidate genes that had never been linked to disease before. Conversely, we found that some quite well-known genetic diseases could have highly unusual presentations – what we call expanding the clinical phenotype of a condition.
The disease I was assigned to work on was the oh-so-easy to pronounce and explain, Haemophagocytic Lymphohistiocytosis (HLH). HLH is a rare but serious condition where the immune system goes into overdrive and won’t switch off. Instead of protecting the body, it causes severe inflammation and can damage organs including the liver, brain, and bone marrow. It can look like a really bad infection, but it’s actually the immune system attacking the body from within. Some cases are triggered by infections or cancer, but others are caused by inherited defects in genes like UNC13D or PRF1. The children in my student were amongst the big chunk of patients where none of the usual suspects showed up on molecular testing.
But finding a genetic change through exome sequencing was only the beginning — I still had to figure out if it actually meant anything. Not all changes in our DNA cause disease, so we looked for the presence of the mutation in healthy controls and used predictive software like PolyPhen2 to solve the first clue: what would this mutation do to the protein the gene encoded? Then came the hard part — proving it. I had to design and run experiments to test how the genetic fault affected the protein’s job in the immune system, and whether that could explain the symptoms we were seeing in the child.
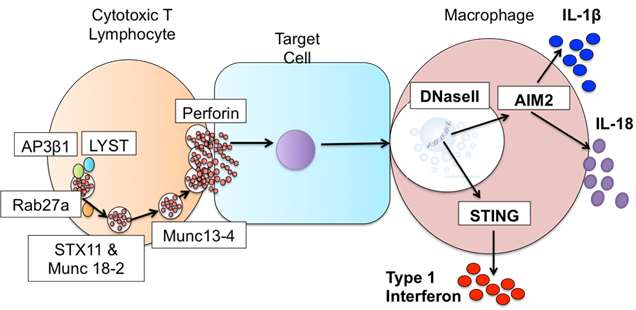
The hard work paid off, in my study we found: one case that was UNC13D protein defective HLH, but only affected the brain; one that turned out to be a totally different (and very rare) immune disorder; and one that revealed a brand-new genetic disease caused by defects in DNaseII resulting in something akin to HLH and another inflammatory condition. In all of these cases what this really gave us was the opportunity to get these kids an answer and onto treatment that could actually work for them.
Figure 3. Defects in DNaseII sit downstream of defects known to cause HLH. Image credit – Claire Walker, thesis.
For me what’s really fascinating about genetics is that what took me years of research is fast becoming a routine test – an incredible reminder of how quickly genetic technologies can evolve. What was once a complex puzzle of genetic mysteries is now providing families with the answers they’ve long needed, turning uncertainty into hope and paving the way for more personalized, effective care in the future. I think that alone was worth putting my husband through yet another ‘re-training’ episode, who knows what I’ll come up with next?
I hope this addition has given you an insight into why working to learn more about how our genes impact us is so important, but also how needed specialists like Claire are for us to do this safely and make the difference we want to make. Sometimes all patients need is an answer, a name to put to what they are going through, something that can provide a route forward even if it doesn’t provide a complete fix. Something so simple can be so difficult to achieve, but just because something is hard doesn’t mean that we shouldn’t try.
This month I’ve been honouring of World DNA day 2025 by publishing a number of posts linked to what DNA is, how we look for it, and what it means to send it away.
Today I’m talking about Upgrade by Blake Crouch. In the story explored in this world, DNA based technology, although very obviously rooted in present day science, has evolved and so has the impact and access to this technology for both individuals and society. In this post I thought it might be interesting to explore ow much of this book is science, and how much of it is fiction? Before I get onto that however, here’s a reminder of the other posts that have been available in the DNA blog series:
One of the reasons I picked Upgrade for the final book review is that I thought it would be interesting, after discussing the current usage of DNA for testing and therapies in previous posts, to explore a book that covers a slightly further future, based in 2060, and what impact the use of DNA technologies could have on humanity in the future.
‘You are the next step in human evolution . . .’
What if you were capable of more?
Your concentration was better, you could multitask quicker, read faster, memorize more, sleep deeper.
For Logan Ramsay, it’s happening. He’s beginning to see the world around him, even those he loves the most, in whole new ways.
He knows that it’s not natural, that his genes have been hacked. He has been targeted for an upgrade.
Logan’s family legacy is one he has been trying to escape for decades and it has left him vulnerable to attack. But with a terrifying plan in place to replicate his upgrade throughout the world’s population, he may be the only person capable of stopping what has already been set in motion.
To win this war against humanity Logan will now have to become something other than himself . . .
In this world, DNA based technology, although very obviously rooted in present day science, has evolved and so has the impact and access to this technology for both individuals and society. It raises some interesting questions about what it means to be human. In this post I thought I would explore some of the science that is included, and what questions the use of this science brings into play.
Are visions of a world where DNA controls our lives unique?
Before I get into the science of the book however, I wanted to flag that visions of a world where the use of DNA testing, evaluation or modification, are not new. GATTACA (did you see what they did there……they are all DNA bases) have been around since the 90’s, when the technology we use clinically now was only in its infancy. Fear of how science could be used in the future is a pretty constant feature of this type of creative content, as it provides a safe way to explore these fears and ethical challenges. I suppose what I’m saying is that just because something is included in these kinds of visioning pieces does not make it bad, wrong or scary. It just means that we also need to think and reflect on what checks and balances are included as part of their introduction in order to make sure the world we create and influence based upon them is the one that we are aiming for, and we have taken steps that include the law of unexpected consequences rather than ignoring it. DNA editing is an amazing, technically complex and powerful tool that has the potential to be positively life changing, so please keep that in mind when you read the rest of this post.
The world of upgrade
In the world of Upgrade the impacts of climate change have really been felt. Entire cities have been flooded as the seas rise and access to food has become a real issue for vast portions of the worlds population. Logan, our protagonist is the son of a genius, a woman changing the face of science. Being the child of a world famous geneticist makes Logan feel the reality of being a normal person surrounding by an extraordinary vision.
I had extraordinary dreams but had been gifted only an ordinary mind
Sadly, as is often the case in these tales, his mothers (Miriam Ramsay) drive for change comes with a fair amount of hubris. In an attempt to address the food shortages Miriam, with Logan supporting as a junior scientist, develops a new gene editing tool called Scythe in an attempt to genetically enhance rice crops. The process goes wrong, and results in The Great Starvation that leads to the deaths of 200 million people.
As a result of the mass deaths, genetic manipulation using Scythe or related tools originating from CRISPR, are outlawed and their use results in a mandatory 30 year minimum jail term. Thus making the field of genetics either outlawed or suspect, and to the birth of the Gene Protection Agency, a police force which aims to track down those undertaking illegal manipulations or research.
Logan ends up going to prison for his work with his mother’s research, and his mother commits suicide. After serving his time Logan is released and joins the very agency that has been set up to prevent a repeat of the genetic manipulation that changed the world. At the start of the book Logan is investigating a scene where an explosion happens, his body is hit by shards of ice, and his life changes again…..forever.
My mother had tried to edit a few rice paddies and ended up killing two hundred million people. What havoc could she wreak—intentionally or through unintended consequences—by attempting to change something as fundamental as how Homo sapiens think?
So, what is gene editing?
I’ve already mentioned CRISPR but I’ve not described what it or gene editing actually are. Gene editing as defined by the World Health Organisation is:
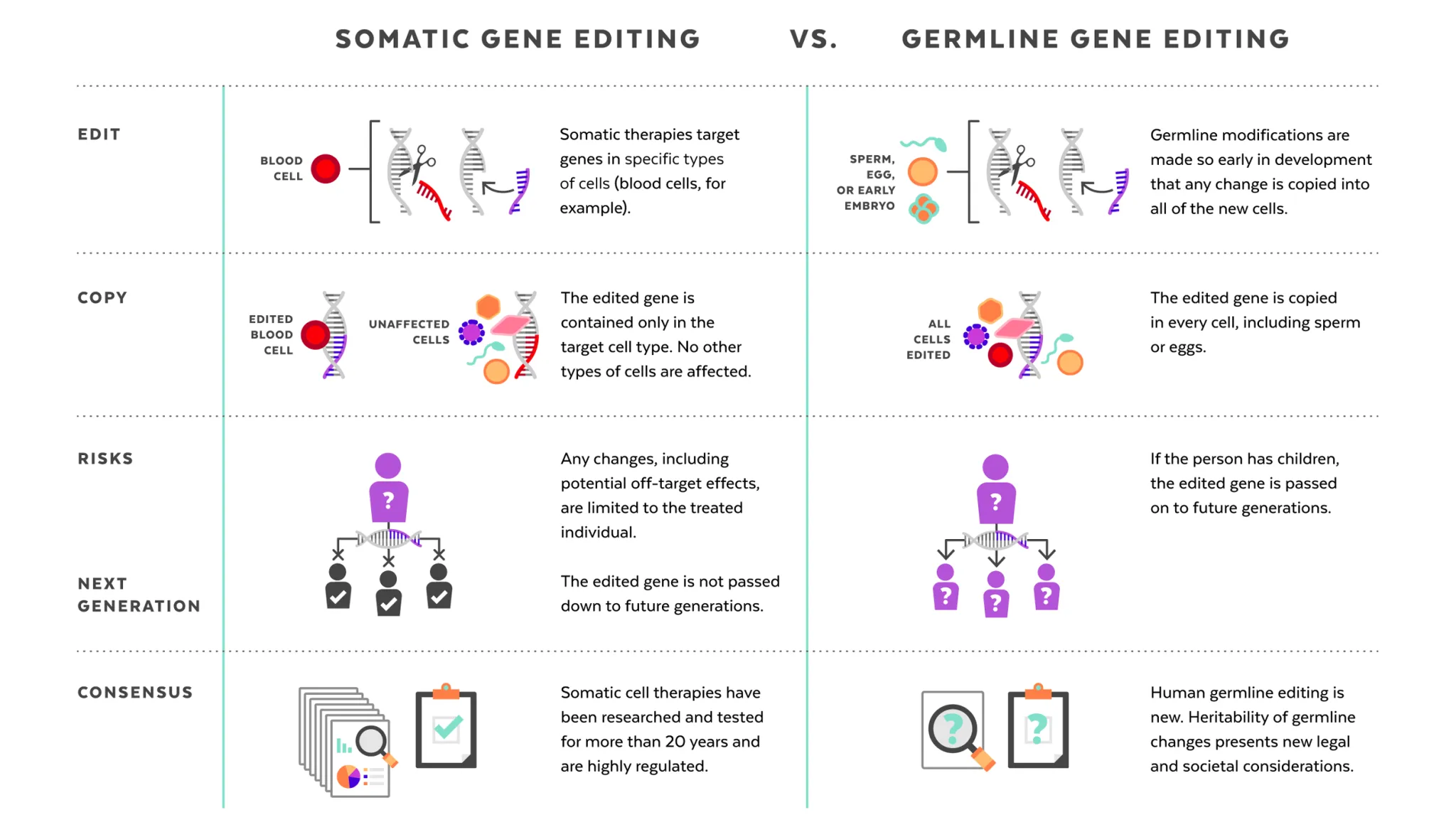
A method for making specific changes to the DNA of a cell or organism. It can be used to add, remove or alter DNA in the genome. Human genome editing technologies can be used on somatic cells (non-heritable), germline cells (not for reproduction) and germline cells (for reproduction).
Before I go further I should probably talk about how CRISPR works and what it is used for. Tools like CRISPR/Cas9 are tools for gene editing, and are the present day origins behind the futuristic tools present in Upgrade. Emmanuelle Charpentier and Jennifer Doudna were awarded the Nobel Prize in Chemistry in 2020 for the development of CRISPR, commonly referred to as genetic scissors.
CRISPR allows you to design a targeted way of manipulating a gene section that you are interested in, and in some cases then replace it with an alternative gene section, which enables the gene to function in a different way. Being able to target and replace, or inactivate genes, in this way opens up a whole new world of possibilities, from health to industrial applications. There are three main approaches to gene manipulation:
Replacing a disease-causing gene with a healthy copy of the gene
Inactivating a disease-causing gene that is not functioning properly
Introducing a new or modified gene into the body to help treat a disease
Now, wearing my geek credentials on my sleeve, I wanted to share with you a music video that describes how CRISPR works. It’s set to the music of ‘Mr Sandman, bring me a dream’ and is retitled ‘CRISPR/Cas9 bring me a gene’. I love this as it I think it describes the history of the process really well. I will tell you now though, that when I made Mr Girlymicro watch this for the 5th time he could not get out the room fast enough, so this may just be a me thing.
Where is the science rooted in the present?
Having talked about the fact that gene editing isn’t the work of science fiction, I thought it would be useful to talk about how and where it is actually being used right now.
According to the Federal Drug Administration there are a variety of types of gene therapy products, i.e. products that manipulate genes, currently available:
Plasmid DNA: Circular DNA molecules can be genetically engineered to carry therapeutic genes into human cells.
Viral vectors: Viruses have a natural ability to deliver genetic material into cells, and therefore some gene therapy products are derived from viruses. Once viruses have been modified to remove their ability to cause infectious disease, these modified viruses can be used as vectors (vehicles) to carry therapeutic genes into human cells.
Bacterial vectors: Bacteria can be modified to prevent them from causing infectious disease and then used as vectors (vehicles) to carry therapeutic genes into human tissues.
Human gene editing technology: The goals of gene editing are to disrupt harmful genes or to repair mutated genes.
Patient-derived cellular gene therapy products: Cells are removed from the patient, genetically modified (often using a viral vector) and then returned to the patient.
There are a number of ways that gene therapy products are already being used for the clinical management of patients, including for patients with conditions such as HIV and sickle-cell disease. One big change that has occured during my clinical career is the use of CAR-T cell therapy for tackling some types of cancer. CAR-T cell therapy is a type of immunotherapy where a patients own T cells (type of white blood cell) are taken from a patient who has cancer, and the cells are then modified in order to better recognise and attack cancer cells within the patients body when they are then given back. So gene editing is already saving lives and in every day use, even if its roll out is currently limited.
Having established that gene editing is very much the next frontier for expansion in healthcare, it’s probably important to consider how stable these changes will be within the wider the gene pool. It’s worth noting that the human genome editing techniques that are being introduced in healthcare are linked to somatic cells, where changes would be non-heritable, rather than within germline cells, which are involved in reproduction, where any changes would be inherited by future generations. Most of the changes that are currently being targeted for gene therapy would not therefore cause the changes to be established within the gene pool. There is a question about whether the target genes, even for somatic changes, may become more established as some of those carrying them may not have previously survived to reproductive age, but to be honest this feels like the impact will be minimal and a price worth paying as a society for improving both quality and length of life in those impacted. Changing future generations of children is however a whole different ball game.
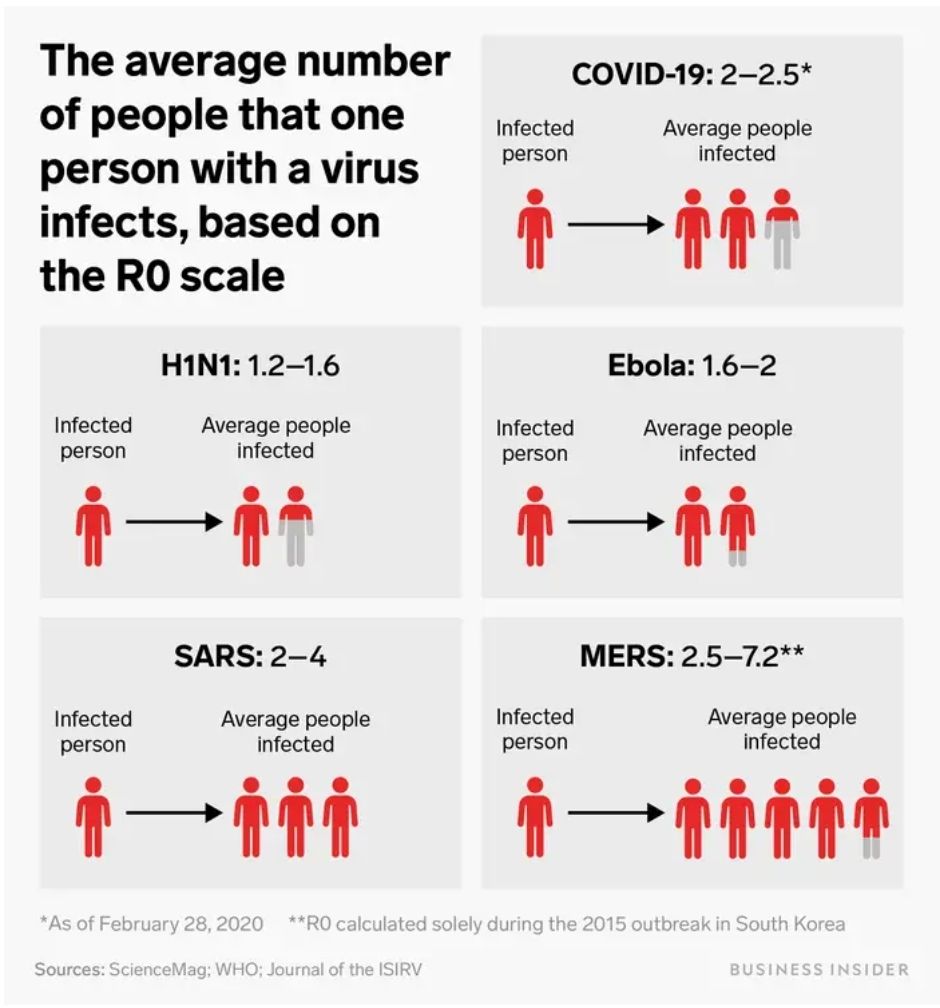
The technology discussed within Upgrade has moved on somewhat from CRISPR. It retains some features of current technology however, as the delivery of Scythe is via viral vector. The interesting thing about this form of delivery is that, in the world of Upgrade, the viruses have been modified and use their standard invasion routes to deliver the genetic material into cells, but, unlike the way that this is being undertaken as part of gene therapy in current healthcare, the viruses do not appear to have been fully modified to remove their ability to cause infectious disease. Some of the plot, therefore, is driven by the fact that it is possible to undertake wide spread indiscriminate gene editing within the human population. The modified viral cells retain their transmissibility alongside their gene editing functionality, and so a gene manipulation can spread in a similar way to any respiratory viral infection. The R0 within Upgrade is 8, which means that every person infected will infect, on average, 8 other people, which means the potential for spread within the population is massive. (If you want to know more about what an R0 is, I’ve covered it in a previous post here). It is not clear to me whether the gene targets within Upgrade are targeting just somatic changes, or a combination of somatic and germ line, but when you can spread so widely so quickly that is probably not the main consideration.
What questions does Upgrade raise?
Within the world of Upgrade, the gene editing doesn’t just target a single gene, but a whole suite of different genes for large scale changed. The problem with using gene manipulation that changes multiple gene targets, that are non-personalised to the condition/individual, and are highly transmissible, is that it is highly likely that the changes won’t work for everyone’s genome. There are going to be side effects or potentially significant impacts. Within Upgrade these are seen through errors that then occur in the brain due to protein mis-folding, very similar to how prion diseases work. The change in some people is catastrophic and there is no intervention available to reverse it. Using indiscriminate gene manipulation has the power to create mass disruption and change societies. It is this power for change that is the jeopardy that drives the novel. Is the cost worth the outcome, and who gets to decide? How much collateral damage would we be prepared to accept, even if the wider benefit to society is a positive one?
Prion diseases: A rare group of neurodegenerative disorders October 2022 In book: Viral, Parasitic, Bacterial, and Fungal Infections Antimicrobial, Host Defense, and Therapeutic Strategies (pp.651-662) Edition:1 Chapter: 53 Publisher: Elsevier: Academic Press
What does it mean to be human?
As part of this risk/benefit consideration, Upgrade asks a lot of questions of the reader, the main one of which, for me, is what does it actually mean to be human?
There is a genetic definition of what it means to be human, but the gene modifications within humans causes our protagonist Logan to ask some very valid questions about what it actually means to be human. Is it just about genetics? How much can we change not only our genes, but our outlook/perceptions, as people and still remain human?
The ‘upgrades’ received cause different characters in the book to judge humanity in general, and other human beings, in very different ways. Do genetic changes make you superior? Does being intellectually smarter permit you to make decisions for others for their benefit, as determined by the smarter individual? In many ways this brought to mind, for me, the old approach to clinical decision making, which was very paternalistic and the role of the person/people impacted was highly passive. I’d like to think we are now moving towards a much more patient focus decision making process, but this book made me think about what would happen if this model was used, not just for one to one interactions, but for the future of humanity.
The question about decision making is an interesting one however. There is plenty of data that demonstrates improved decision making in small groups, and if time is of the essence how would you engage with enough people for a decision to be valid? Especially a global decision? How many people would you need to interact with for a choice about changing the DNA of your species to be valid? How would you manage a lack of consensus? Would you let the world burn whilst the choice was being made, or would you accept that at some point someone would need to step in and lead the way forward? It’s the uncomfortable space between ethics and pragmatism, and definitely not something that is easy to answer, even conceptually.
Is intelligence the problem?
As discussed above, a lot of the plot driven by the counter to our protagonist in Upgrade, is based on the concept that if humans were smarter they would make better decisions. Therefore, by improving how people think and removing some of the emotional component the human race would be improved and therefore ‘saved’. This is especially important in the world of Upgrade, as because of the damage that is being done linked to climate change and other damage caused by humanity, the clock is ticking and Logan is very aware in his upgraded state that there is only 100 years left to save mankind.
The problem, as it plays out to me, is that it is very much not about intellect however, it’s about the ability of individual humans to care enough for others. For one person to make decisions that costs them rather than benefits them for the sake of someone that they do not know well if at all. This is especially true for problems that are going to impact future generations, like climate change, where the people most impacted have yet to be born. By the time we ‘meet’ those who will be most affected it will be too late to save them. Even for a present day context it raises questions, we all think of ourselves as having empathy and caring for others, so why does that not play out and allow us to care for the migrants that are dying trying to join us and share in our safety? Why is our compassion so limited?
One of the reasons for this has nothing to do with intellect, and would in no way be altered no matter how smart we become. It’s based on a theory known as the Dunbar number, which predicts that we can only empathise with a maximum number of 150 people, the number of people that would likely to have been the maximum size of our primate tribe. More than this, we can only truly care, to the point we may want to sacrifice, about a much smaller number of people. The book therefore postulates that we aren’t held back due to a lack of intelligence or innovation, we’re held back by a lack of compassion and the ability to truly care about people we don’t know and will never meet. If we are to change anything about ourselves in order to save mankind therefore, it’s not intellect we need more of, we need to find a way to increase our capacity for compassion and therefore change our Dunbar number, to adapt for the world we now find ourselves in. So maybe the answer to the problem is to become more ‘human’ rather than less.
Where do all of these questions leave today’s gene editing technology?
Gene editing technologies are making massive strides, saving lives, and positively helping people who have serious health conditions.
Somatic gene editing is well established, and has been developed over the last 20 years so that regulation is in place, and it being more and more routine rolled out in countries that have access to advanced scientific technologies. The problem is just that however, these interventions are technologically challenging and incredibly expensive, and therefore not universally available. This means that they also do not necessarily take into account the diversity of the human genetic population or the lived experience within different cultural communities. Regulation is also not present universally, with some people forced to access these therapies through the use of rogue clinics, or by undertaking medical tourism, which brings with it increased risk. There is also the potential for illegal, unregistered, unethical or unsafe research and other activities, including the offer of unproven so-called therapeutic interventions, as with any emergent technologies. Ensuring equity of access and appropriate regulation will be essential to ensure a safe global adoption of these therapies.
Germline gene editing is however in a very different place, as this would lead to the editing of DNA in a way that may be heritable across generations. There is an intense debate linked to its use as the the future generations that would be impacted would have no capacity to consent to the changes, and or risks, that are being made. There could be possible risks and consequences for offspring and for society in general, and once that genie is released it will not be possible to put it back in the bottle. Discussing what circumstances it would ever be appropriate to undertake these changes requires us all to be actively engaged in these discussions.
I hope you’ve enjoyed these series of blogs linked World DNA Day and taken some to celebrate the miraculous nature of just being you. I’ve really enjoying sharing some of the technical information, but also diving into some fictional worlds and discussing the thoughts that they provoke. With summer coming up I hope you may even pick up a copy of these great novels and dive into their worlds yourself. If you find any others in your reading adventures, return the favour and let me know. I may even include them in a future review. Happy reading.
Friday just gone, 25th April, was World DNA Day. I’ve had a series of blogs that I’ve been playing around with linked to what DNA is, how we look for and investigate it and how we are exploring DNA in our everyday lives. Linked to this I’ve also got two book reviews coming where the world changes because of genetic testing and genetic manipulation. So this is the first of four part DNA bonanza.
I thought I would write these posts, because as much as artificial intelligence could change the way we live and is frequently discussed, we are all accessing DNA based testing more and more, with many of us not really thinking about how this too is changing the world in which we live.
I remember really clearly the first time I actively came across the concept of DNA, DNA testing and DNA manipulation. It was in Jurassic Park, when Mr DNA pops up at the start of the film to talk you through how they used DNA and cloning in order to make the dinosaurs. This film came out in 1993, I was 13 and I just remember how all of my class were queuing up to get tickets. It was the first film I really remember there being hype about, well that and Aladdin which was a different kind of seminal moment. It was the first film I remember watching and thinking just how cool science and scientists were.
In fact I talk about Mr DNA so much that the wonderful Mr Girlymicro brought me a Mr DNA Funko pop which lives on my desk at work and reminds me that the impression we make on people stays with them.
What does all this have to do with how we use DNA now? Well, in 1990 when Jurassic Park came out, the routine use of DNA, even in research, was still pretty much science fiction. The structure of DNA had only been described in 1953. Polymerase Chain Reaction (PCR), which is the main way we investigate DNA, had only been developed in 1983, and was only starting to become more widely available in the 1990’s. When I started working within healthcare in 2004, we were only really just starting to move from PCR being something that was used in research to something that was common place in clinical diagnostics. The leap from there, to a world where thousands of us can swab ourselves at home and post samples off to be diagnosed with SARS CoV2 during the pandemic, or to get information on our genetic heritage, would have sounded like something that would only occur in a science fiction novel if you’d mentioned to me back theb.
Just a flag, this part one post has a lot of the technical stuff linked to what DNA is and how we investigate it. You may want to skip this post and head directly for part two if you don’t want to be reminded of secondary school science, but if you can bear with me I think it will help some of the context.
What is DNA?
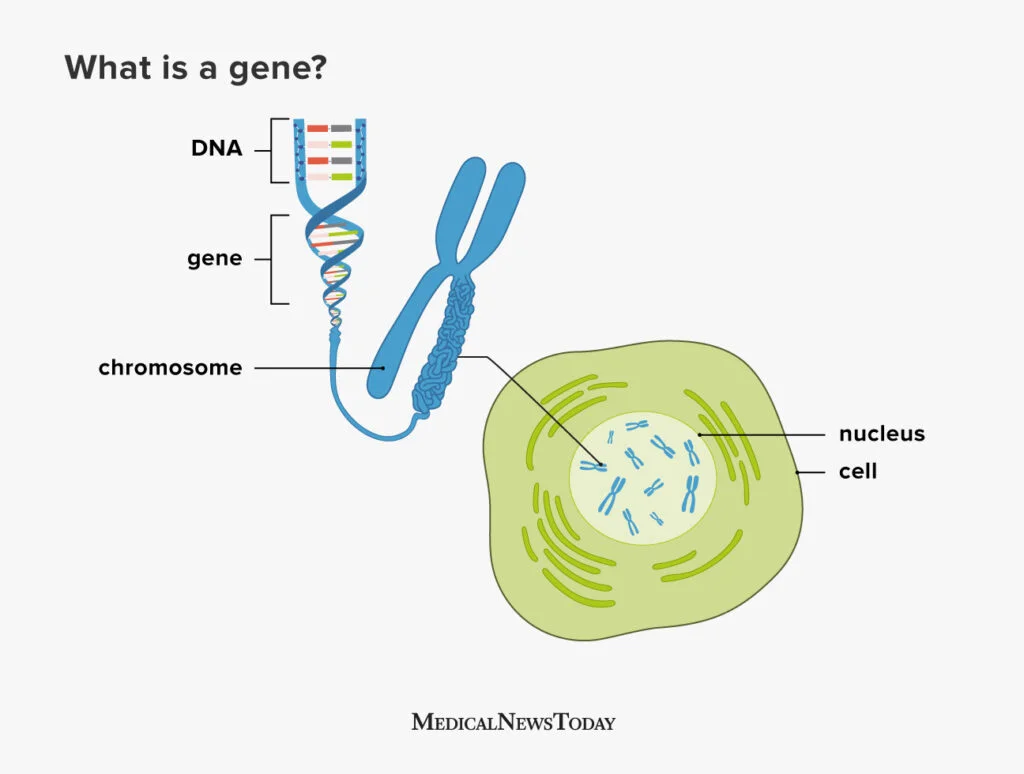
DNA, or to give it its full name Deoxyribonucleic acid, is commonly referred to as the building block of life. The structure of DNA consists of a double-stranded helix held together by complementary base pairs. The nucleotides that form the base pairs are adenine, thymine, guanine or cytosine. These nucleotides act to link the two strands together via hydrogen bonds, with thymine always pairing with adenine (T-A) and guanine always pairing with cytosine (G-C).
Sections of DNA then combine together together to code for genes, which are sections of DNA that work together in order to code for proteins, that then permits the expression of our DNA in physical form.
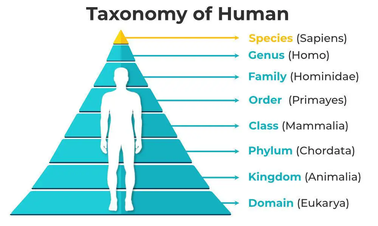
Genes are organised into chromosomes or packages of DNA. Each chromosome is formed from a single, enormously long DNA molecule that contains a strand of many genes, with the human genome containing 3.2 × 109 DNA (3,200,000,000) nucleotide pairs, divided into 46 chromosomes formed from 23 pairs (22 pairs of different autosomes and a pair sex chromosomes).
So how do we get from DNA to proteins? The specific sequences of nucleotides that form our DNA are arranged in triplets (groups of three). To turn DNA into protein, it gets transcribed into RNA (ribonucleic acid) within cells, with each of these triplets coding (translating) into an amino acid, which then get combined together to form proteins. The amino acids combined dictate what form and function the resulting proteins takes. Proteins then serve as structural support, biochemical catalysts, hormones, enzymes, and building blocks for all the processes we need to survive as humans.
Long and short, everything comes from your DNA, it’s super important, and is unique to you, but it’s structure is complex and there’s a lot of it in each of us.
How do we investigate DNA?
Now that we know about what DNA is, and how important it is for life, not just for humans but for all living things, it makes sense why so much time and energy has been deployed into understanding more about what it means for us as a species, as well as for us as individuals.
I’ve mentioned that PCR was first developed in the 80’s but didn’t really come into routine clinical testing until the 2000’s. What is PCR though and how does it work?
I often describe PCR as a way to look for DNA that is similar to looking for a needle in a 25 story block of flats sized haystack. The human genome is 3.2 billion base pairs, and we are often looking for a fragment of DNA about 150 base pairs in length, 1/21 millionth of the genome. It’s quite the technical challenge and you can see why it took quite a while to be able to move from theoretically possible to every day use. What makes it even more complicated is that you need to know what that 150 nucleotide fragment is likely to contain or where it is likely to be positioned within those 3.2 billion base pairs to really do it well. The human genome was not fully sequenced, and therefore available to us to design against, until the year before I started my training at GOSH, 2003. The progress therefore in the last 20 years has been extraordinary, and I can only imagine what will happen in the next 20 years. Hence the book reviews that will be coming as parts 3 and 4 of this blog.
So, how does PCR work? Well the first thing to say is that there are actually a number of different types of PCR, although the basic principles are the same. For example, there are some types of PCR that target RNA. There are also types of PCR that are used more frequently within clinical settings for things like SARS CoV2 testing, that are called Real Time PCR, called that as results become available in real time rather than waiting for the end of the process. It is for Real Time PCR that the small ~150 nucleotide fragment length is an issue. So all of these processes have their own pros and cons. Like many things in science, you have to use the right process to answer the right question.
The basic principles shared between types of PCR are as follows:
Designing your primers:
Primers are the pieces of DNA that you design and make that will stick to your target piece of DNA you are interested in. The reason this works is because of the fact that the nucleotides that make up DNA are complimentary and so A binds to T, C binds to G. As DNA is double stranded you can design your primers (your equivalent to the magnets to find you needle in your haystack) so that they will bind to your specific target (the piece of DNA you are interest in). If you want to have your primer stick to a piece of DNA sequence that reads AAG CTC TTG, you would design a primer that ran TTC GAG AAC using the complementary bases, make sense?
You design one set of primers for one strand, this is called your forward primer (moving from 5′ to 3′), and then you design your reverse primer at the other end of your target for the opposite DNA strand (moving from 3′ to 5′). Doing it this way means that when you start your PCR process you end up with complete copies of your target. You will then successfully have pulled the needle from your haystack using you targeted magnets.
Undertaking the PCR:
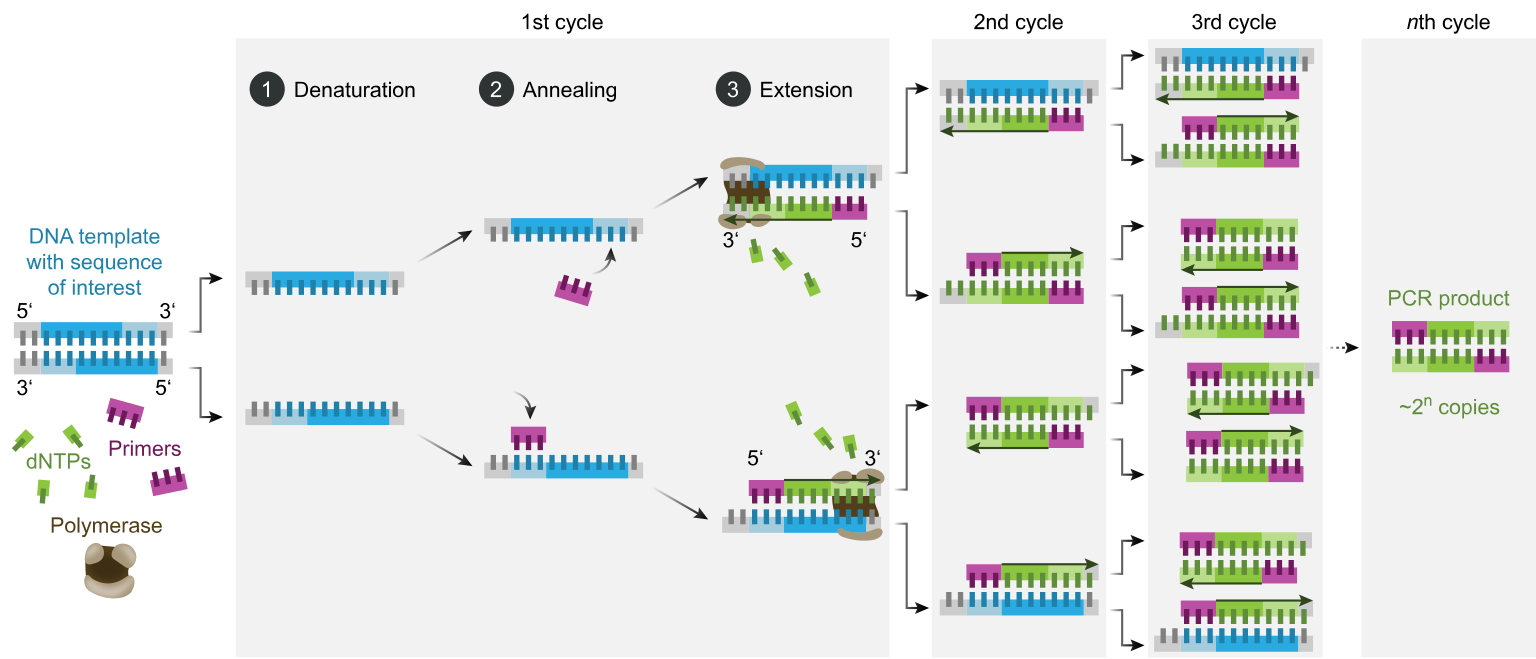
Once you’ve got your primers (which you can just order in once designed) you can then get onto the process of the PCR itself. You combine your sample that you think might contain the DNA target you are looking for (be that human, bacterial, environmental etc) with the reagents (chemicals) that you need to make the process work all in a single small tube. This tends to be a delicate process that needs to be undertaken at controlled temperatures as the protein that runs the process (Taq polymerase) is delicate and expensive. To do this we combine:
DNA Template: This is the sample that contains the DNA target you want to amplify
DNA Polymerase: Almost always this is Taq polymerase which is used due to its heat-stability as it originates from a bacteria that lives it deep sea vents. This allows it to function at the high temperatures required for PCR and is used to make the new DNA copies
Primers: These are the short, synthetic DNA sequences that you design to attach to either end of your target DNA region. These then allow the DNA polymerase to add nucleotides to create the new DNA strands
Nucleotides (dNTPs): These are single nucleotides (bases) that are then used to build the new DNA strands (adenine, thymine, guanine, and cytosine)
Buffer Solution: This solution provides the optimal conditions (pH, salt concentration) for the enzyme to function properly
Once you have your reagents you then put them on a platform that heats and cools for different steps to allow the enzymes to work and for the new DNA strands to be created:
Denaturation: The double-stranded DNA template is heated (typically to 95°C) to separate it into two single strands. This step ensures that the primers can access the DNA sequence of interest
Annealing: The temperature is lowered (typically to 50-60°C) to allow primers to bind to their complementary sequences on the single-stranded DNA. This is the step where your magnets find their needle
Extension: The temperature is raised again (usually to somewhere around 72°C, the optimal temperature for Taq polymerase activity). Taq polymerase extends the primers by adding complementary nucleotides based on the DNA sequence to create new copies of the original DNA target
These three stages are repeated in cycles, typically 20-40 times, which results in thousands and thousands of copies of the original target to be created, so that eventually your 25 storey haystack is made up of more needles than it is hay, and therefore it is easy to find what you are looking for.
Interpreting your results:
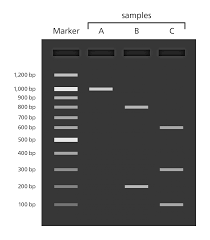
At the end of your PCR step, if you are using traditional PCR, you run what is now called your PCR product or amplicon (the things you’ve made) through something called a gel. This is just a flat jelly made of agarose (or seaweed) which also contains a dye that binds to DNA and allows to separate your DNA based on size. This allows you pick out where you have samples that have the massive amplification you are looking for, as you can see it as a band within the gel. If a band is there and the right size (as you know how big your target was supposed to be) this is a PCR positive.
If you need to know more detail than whether something is present or absent, for instance if you need to know not just that a gene is there but which variant of a gene is present, you need to be able to tell what the nucleotides that were added between your two primers actually were. To do this, you will follow up PCR with a process called sequencing.
You take your target PCR’d section and then put it through a process to work out what the nucleotides added were. This involves doing the PCR process again, to make even more copies, but the nucleotides added into the reagent mix have fluorescence attached so you can tell which ones have been added during the PCR process. G’s often produce a black colour when hit by light, A’s green, T’s red and C’s blue.
For our original sequence we talked about, AAG CTC TTG, the sequence would read Green, Green, Black then Blue, Red, Blue followed by Red Red Black. Colours are then back interpreted into a DNA sequence (a series of letters) and there you have it, you know what the DNA is between your primers and you can then interpret your sequencing result. If you have large fragments of DNA you are interested in, you may have to do this in overlapping segments and put it back together, something like a jigsaw, before you can get your answer, but the basic process is the same.
What can DNA tell us?
As I’ve said, the search for DNA and specific genes has become an increasingly normal part of providing diagnostics in healthcare. Most of us will have sent off a swab for a PCR at least once during the COVID-19 pandemic. PCRs are frequently used in my world of infectious diseases to see if a bacteria is present or absent. They are also used so that I am able to see if a bacteria will respond to an antibiotic, by seeing if they carry antibiotic resistance genes, which can be crucial to getting patients on the right treatment at the right time.
Looking for specific variants of genes is also key to making sure that the treatments we give also don’t cause any unexpected consequences. A good example of this is when we use PCR and sequencing to look at genetic variants of a gene called MT-RNR1. A specific variant in this gene, m.1555A>G, is known to increase the risk of aminoglycoside-induced hearing loss. Aminoglycosides are a crucial antibiotic class that are used pretty widely, but especially in management of some conditions such as cystic fibrosis and certain types of cancers. A small number of people have a gene that makes them prone to something called ototoxicity as a result of taking these antibiotics, resulting in hearing loss. If we know a patient has this gene variant we can then choose to use different antibiotics, improving patient outcomes and avoiding a life long hearing impact.
Outside of screening linked to patients presenting with specific conditions, the use of DNA sequencing is being utilised more widely to look for genes or conditions before they even present with symptoms, in order to reduce time to diagnosis, and hopefully to be able to find patients and start management before they’re impacted or even present as unwell. A great example of this is the newborn screening programme that started last year. This screens newborns using the heel pricks of blood taken at birth so that rare diseases that could take months or years to diagnose by traditional means are picked up early in life, therefore allowing appropriate treatment to start earlier and hopefully saving lives.
DNA is fascinating and I love knowing about it. It’s not just me though. In recent years there has been an increasing trend for people to send off their DNA for other purposes than to hospitals for clinical testing. I’m not going to say too much about this in part one, but it was this that really inspired me to write these posts in the first place and is the main focus of part two of this blog series.
Just a quick google however provides a wide number of different companies offering a variety of DNA testing services outside of the NHS (NB I don’t advocate for any of them):
Crystal Health Group: Operates a network of DNA testing clinics, offering relationship testing and other services.
23andMe: Provides DNA testing for health, ancestry, and other personal insights.
Living DNA: Focuses on both ancestry and wellbeing-related DNA testing.
MyHeritage: Provides DNA testing, particularly for ancestry research.
AncestryDNA: Company specialising in DNA testing for ancestry discovery.
The complication with all of this type of provision of testing is that outside of the clinical world in the UK, where testing should be undertaken in accredited laboratories and reporting of the results must meet certain standards, sending off DNA to private companies is much less monitored.
I hope you can see by some of the technical descriptions just how complicated these DNA processes can be. How time consuming, and how expensive to get right. There is also a lot of nuance about the different types of PCR, sequencing, gene targets, and results analysis that can be offered under the umbrella of ‘DNA testing’. Without the right people involved to make sure that there is embedded quality assurance challenges could arise, depending on what kind of testing is undertaken.
As stated in a recent Independent article:
As they’re based on estimates, I suggest treating home DNA tests as a fun investigation to get to know your family history a little better rather than a to-the-letter representation of everything that’s ever happened in your gene pool – Ella Duggan Friday 28 March 2025
The devil for all of these things really is in the detail, and we’ll get into that detail much more in part two! For those of you interested in learning more about the history of DNA testing, I’ve included a talk below. Happy World DNA Day
I’m back from a lovely week away at Disneyland Paris, celebrating Christmas and escaping reality (a post on Disney and denial as a coping mechanism is on its way). Whilst I am still struggling with the return to reality this weeks blog post is supplied by the wonderful Callum Barnes. Callum is a disciple of the biomedical sciences, current master’s student creating a more authentic lab experience for those after me, aspiring consultant microbiologist (the best discipline, sorry Claire – you see he understands, like me, that micro will always trump immunology).
Callum is supervised by Dr Claire Walker who is a paid up member of the Dream Team since 2013, token immunologist and occasional defector from the Immunology Mafia. Registered Clinical Scientist in Immunology with a background in genetics (PhD), microbiology and immunology (MSc), biological sciences (mBiolSci), education (PgCert) and indecisiveness (everything else). Now a Senior Lecturer in Immunology at University of Lincoln. She has previously written many great guest blogs for The Girlymicrobiologist, including one on turning criticism into a catalyst for change.
Two years ago, I began a placement year in the microbiology department of a pathology lab, unsure of what was to come, and unsure of myself and my skillset as a scientist. As I think every scientist feels at some point, I was mostly concerned that I would be a hinderance to all the wonderful staff that were just trying to get on with their jobs. Everyone was amazing though and helped me develop the skills and confidence I needed to successfully complete my IBMS portfolio verification. Returning back to university for my final year, I found the lab-based work so much easier than in my second year with my experience, but… something was different. This wasn’t the same stuff I just spent the last year working on, where was the LIMS? The booking in of the samples, the investigative process and the, frankly, the occasional chaos were missing. That’s not to say the labs weren’t good – they were great – and the staff that developed and ran them miles better, but something felt like it was missing. And that’s when my now supervisor Dr Claire Walker came to me with a project for my Mbio year.
Claire and I both have experience in the NHS, herself a lot more than me, but we have both felt and experienced the environment that a pathology lab has. It has a very unique feel to it, slightly alive in my opinion. This is not a very common experience to have in academia though as most academics have a research background, which means that the practical pathology side of things can sometimes get lost when students do their practical work. As such, Claire and I have been working on creating a lab experience that is as authentic to an NHS pathology lab as possible.
But why even bother? The students are learning the same things, just in a different way, so does it really matter? Well in fact, yes, it does! As Claire has said previously, the pilot study she did had very good results, so the data is there to back up our work. But imagine for just a second that you are looking at applying for medicine, and you have two offers. One university offers a fully simulated experience using manikins and actors – the whole shebang. And the other university teaches mostly through theory and shadowing – no practical experience is offered. I know which course I would enjoy and learn the most from. Medical schools know this too and is why most of them offer simulated teaching – it makes for better doctors too.
So, we should really ask, why isn’t this offered for biomedical scientists? Maybe it’s cost, maybe there isn’t the associated prestige. Whatever it is, I am sure that our work will guarantee a truly authentic clinical laboratory experience here on the iBMS accredited course at the University of Lincoln – something I know will provide the right skills for the pathologists of tomorrow.