This post was supposed to be something quite different. It was supposed to be about One Heath and a great podcast created by Beckman Coulter I was involved with in 2024, alongside some really inspiring people. In some ways it still is that, but because of the cruel reality of life it is actually also something quite different.
”Going Macro on Micro” is a podcast that Dr Simon Doherty and I were involved with that explores emerging themes and pressing issues in the world of microbiology. As the host, Dr Lough, says the podcast covers everything from investigating the global challenges of infection control to unveiling the future of diagnostic technologies.
The week the final episode of the podcast dropped, before Christmas, I got some pretty devastating news. Sadly Simon has passed away. Now, I didn’t know Simon well. We’d emailed since doing the podcase together and I kept an eye on the awards he received and his really interesting posts. In this limited contact though, he still managed to inspire. Recording the series with him was such a privilege. He was kind, open and funny. More than that he was so knowledgeable and I came away feeling like I’d learnt so much. I am so sad that I won’t be able to build on the foundation we laid to continue to learn from him and talk about the challenges/opportunities that face us in the fascinating world we both inhabited. I thought about not sharing these episodes when I heard the news, but then decided that I don’t want you to lose out on the honour I had of learning from him direct. I hope that you will hear both his wisdom and his challenge, and also aspire to do better, as I do, as a result. Thank you Simon.
I’ve decided to keep the focus on Simon and just put some graphics and links here that might supporting learning more about antimicrobial resistance and One Health. At some point when the loss of Simon has had a little more time to be processed I will think about writing something in a little more depth reflecting on his comments and the overlap between human health and veterinary medicine. Until then, the links to the episodes are below:
Ahmad Nayeem , Joji Ronni Mol , Shahid Mohammad. (2023). Evolution and implementation of One Health to control the dissemination of antibiotic-resistant bacteria and resistance genes: A review. Frontiers in Cellular and Infection Microbiology
Episode One
Rhouma, M., Soufi, L., Cenatus, S., Archambault, M., & Butaye, P. (2022). Current Insights Regarding the Role of Farm Animals in the Spread of Antimicrobial Resistance from a One Health Perspective. Veterinary Sciences, 9(9), 480. https://doi.org/10.3390/vetsci9090480
Episode Two
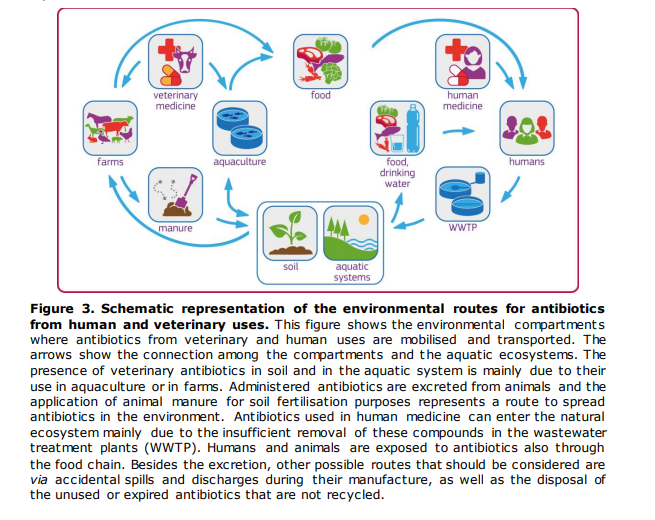
Sanseverino, Isabella & Navarro, Anna & Loos, Robert & Marinov, Dimitar & Lettieri, Teresa. (2018). State of the Art on the Contribution of Water to Antimicrobial Resistance. 10.2760/771124
Episode Three
Sanseverino, Isabella & Navarro, Anna & Loos, Robert & Marinov, Dimitar & Lettieri, Teresa. (2018). State of the Art on the Contribution of Water to Antimicrobial Resistance. 10.2760/771124
Episode Four
Sanseverino, Isabella & Navarro, Anna & Loos, Robert & Marinov, Dimitar & Lettieri, Teresa. (2018). State of the Art on the Contribution of Water to Antimicrobial Resistance. 10.2760/771124
Episode Five
Sanseverino, Isabella & Navarro, Anna & Loos, Robert & Marinov, Dimitar & Lettieri, Teresa. (2018). State of the Art on the Contribution of Water to Antimicrobial Resistance. 10.2760/771124
Episode Six
Sanseverino, Isabella & Navarro, Anna & Loos, Robert & Marinov, Dimitar & Lettieri, Teresa. (2018). State of the Art on the Contribution of Water to Antimicrobial Resistance. 10.2760/771124
I’ve been talking to quite a lot of people about antimicrobial resistance lately. Partly because I’m involved in a big clinical trial called LAKANA, but also because I’ve been recording some content for the Department of Education and school teachers linked to Infection Prevention and Control. What has struck me is that something that has such a massive day to day impact on my working life hasn’t really made its way into the public consciousness just yet.
As last week was antimicrobial awareness week, I thought I should take the opportunity to talk about antimicrobial resistance and why I think we should be working hard to talk about it more: in the pub with our friends, with our families over Christmas, and with our patients and students.
Photo courtesy of Anthony De Souza
What Is Antimicrobial Resistance?
When I go into classrooms and speak to members of the public they sometimes think that antimicrobial resistance is when our bodies become ‘immune’ to antibiotics. This isn’t the case. When we talk about antimicrobial resistance or, for the rest of this blog post, antibiotic resistance (as I’m talking about bacteria) is when the individual bacteria are not affected by the antibiotic or it works less well (see my introduction to antibiotics post for a bit of background).
Antibiotics work in two main ways. They are either:
Bacteriostatic = inhibits the growth of bacteria.
Bactericidal = kills bacteria.
The way the antibiotic works against the bacteria can be linked to the way that the bacteria become resistant to the antibiotic. I’m going to do another blog post with some of the technical details of how this works and how we detect it, so bear with me for a couple of weeks. For this post, the main thing is to know that it is the bacteria that become resistant, not us, and that there are a number of different ways that this can happen:
Intrinsic resistance = the antibiotic will never work against that particular bacterial species because of the characteristics that species has. This includes things like Vancomycin not working against Gram negative bacteria as the molecule is so large.
Selective resistance = where a mixed population of resistant and sensitive bacteria are impacted by antibiotic use and the resistant ones survive and therefore become dominant.
Acquired resistance = where previously sensitive bacteria acquire the ability to resist the effect of an antibiotic, often through acquiring genes, which allow them to change the way they function or replicate.
Levels of antibiotic resistant bacteria are being detected in increasing numbers in food (linked to farming), in the environment, and within humans: both in hospitals and in the community. It’s for these reasons (and others) that it has been modelled that more people will die linked to antimicrobial resistance than cancer by 2050. If, as a population, we have more resistant bacteria onboard as part of our normal flora, it is increasingly more difficult to treat us when we need it. It will also become increasingly more difficult to do ‘standard’ surgeries such as hip replacements, tonsillectomies etc. as these require us to give prophylactic antibiotics when you’re in surgery in order to reduce infection risk. This means we may have to live with long-term conditions that currently we would surgically correct.
Most of us think about antibiotics as being something that we either give to really sick people in hospitals or a fairly harmless way to get back to our every day lives when we’re feeling unwell at home. In many ways that is true. Most of us will have had multiple courses of antibiotics during our life and have never given it much thought. Some women may have had the odd bout of thrush when they’ve taken antibiotics for a urinary tract infection and that is the closest they’ve seen to side effects. The case of a woman getting a fungal infection (thrush) because they’ve taken antibiotics that have wiped out the non-harmful colonising bacteria in their vagina is a pretty good example of exactly what can happen in less obvious sites when we take antibiotics. For example, there’s plenty of data that the use of antibiotics can impact on the bacteria in your gut, providing selective pressure and changing what the population of bacteria looks like. Usually this returns to normal over time. However, in a world where the bacteria we encounter are increasingly resistant, that return to normal could take longer; if they got out of the gut to another location due to surgery during that time they could be more difficult to treat.
Colonisation vs Infection
Most of the time if we have resistant bacteria onboard we would never know. They are colonising us, just like our normal bacteria, and not causing us any harm. There’s good data to show now that when we travel abroad to countries with a high prevalence of antibiotic resistant bacteria in food or the environment, that we may exchange some of our sensitive bacteria for resistant ones. You’d never know, especially as when we get home they will usually be replaced again with sensitive versions. However, if you happen to get an infection whilst you have them onboard because you’ve had an accident on holiday, or you’ve travelled for medical care overseas, then the infection may be more difficult to treat.
It’s not just the antibiotics we use in humans that can make this situation worse. Antibiotics are used as growth promoters in farming. We use antibiotics to treat our pets. Because of how expensive and difficult antibiotics are to develop, we are not really developing new ones and so the pool of available antibiotics is getting smaller.
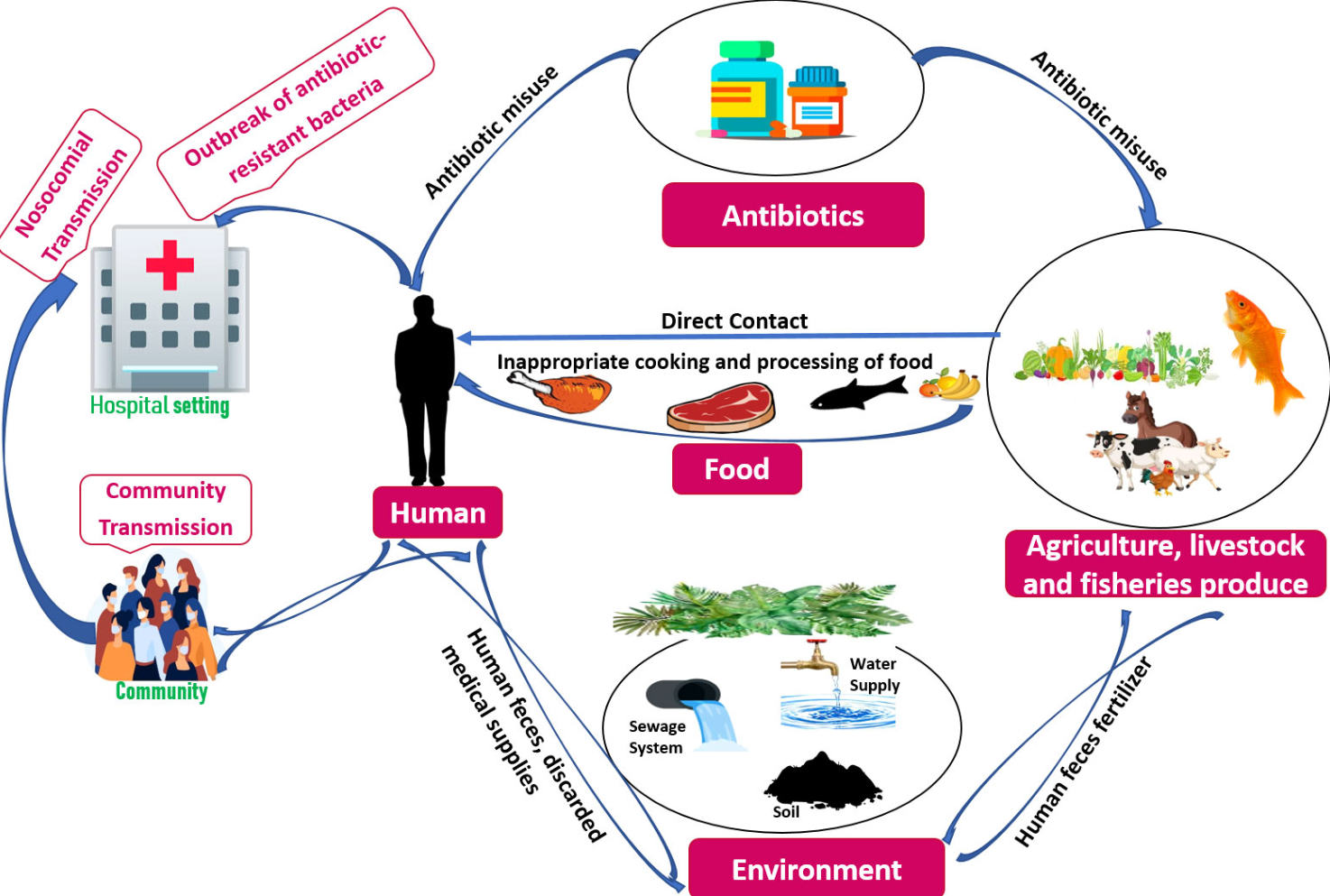
Because antibiotics are used in so many different ways in solving the issue of how to impact levels of antibiotics, resistance is complicated. It requires us to be able to diagnose and detect resistance faster, to work with drug companies in order to tackle the drug development pipeline, and to take a ‘One Health’ approach, looking at farming and veterinary approaches as well human.
So, what can I do?
Be aware that not all mild respiratory and other conditions require antibiotics. Many are viral and will improve with rest and hydration. Therefore, consider waiting before requesting a prescription for antibiotics.
If given a prescription, make sure you complete the course. Do not just stop because you start to feel better. Stopping early might mean that you have not completely treated the infection and the remaining bacteria can grow back and sometimes develop resistance.
Do not buy antibiotics when you are abroad in a country that permits an over-the-counter purchase.
Do not store antibiotics and use them at a later date. Neither should you use antibiotics that were prescribed for a family member or (and I know people have done this) a pet.
Think carefully about whether travelling abroad for healthcare is the right choice; make a risk assessment about where you are planning to travel.
If we want to continue to experience healthcare in it’s pre-COVID-19 form, we all need to work together to change the way we use antibiotics so that the modelling predictions do not come true
As I write this, it’s the morning after the Antimicrobial Guardian Awards 2020. We were lucky enough to be considered for the Public Engagement category for the Nosocomial Project. Much to my jaw-dropping shock, we were lucky enough to win. This post isn’t really about that, though. This post is about why I think it’s important that such awards exist, which is not a universally held opinion.
Every year there are a number of local and national awards for NHS and Public Health related activity. I’ve been lucky enough to have been nominated for, and won, some of these awards. I have experienced many lovely responses but I’ve also received negative ones. These have indicated that the same people always win everything and that my success makes others uncomfortable. So would I put my awards somewhere where they can’t be seen? There is obviously a whole blog topic on how we do a better job at celebrating others’ success and taking it as an opportunity to lift up the whole; but there are also some very practical reasons why these kinds of awards are important.
Why Do I Think Awards Matter?
The NHS has traditionally been a very siloed environment, with professions working very separately. Many awards have categories that are targeted at, or recognise, collaboration across silo’s. This is one way of getting people to actively think about their working environment and start to take steps to break down barriers that have long existed.
If you work in a professional group that is often pretty invisible at organisational or national level, these awards present a wonderful opportunity to highlight the work that these groups do, which might go unnoticed in the general day-to-day workings of healthcare. This can have a direct impact on how valued these groups feel, but also in inspiring how practices could be integrated for the benefit of the system.
Many of these rewards are for projects that are done on top of the day job. Although there are prizes for individuals, a lot of the time these projects can only be delivered by teams. Within the day-to-day NHS, we don’t really have a way to recognise these teams when compared to private industry. It’s important for me, as a leader, to acknowledge the hard work of my teams by nominating them and ensuring they feel seen and their work appreciated.
Projects such as Nosocomial require external funding to be able to develop and progress. Winning awards for the work is pretty much the same as a paper going through external peer review and being accepted. When applying for further money to continue the work, or for other project applying to Trust Board for support, having an external stamp of approval can be the thing that moves decisions in your favour. They can also provide valuable free promotion to support building new collaborations or expanding the work to increase impact.
Nominating work for awards can provide a great moment for reflection and self-evaluation of the project. Projects often develop organically and, because they are often done in addition to other work, we don’t always take the time to reflect on the strengths and failures of what we’re doing. The process of nominating can highlight gaps, especially when it comes to evaluating work. These can then be addressed and you may decide to hold off on the nomination until you have the extra data. Most importantly it will make the work itself better, irrespective of whether you win.
Something I feel really strongly about is the removal of hierarchies and empowerment in terms of the future of healthcare. Many awards now have specific categories for inclusion of the public in work, or a focus on diversity and inclusion. These specific categories demonstrate the values of the NHS and encourage work that lives up to those values. If we really want to create an NHS that works for the modern world, the more that can be done to embed these values in everyday working, the more successful the change will be.
Lastly, and most significantly, these awards offer the chance to share learning. To discover what works. To be inspired by the work of others. Although awards are often considered to primarily benefit the individual or team, the truth of the matter is that that the people that really benefit are those that are part of the system that the awards represent. This is fundamentally why we should work to support these events, not for the ‘me’ but for the ‘we!’
So celebrate the success of yourself and others! Know that by doing so you benefit everyone
Top tips for nominations:
Read the category criteria so you are applying for the right one.
Understand the scoring scheme (which is usually listed somewhere) so you know what the judges will be interested in.
If there are questions, make sure you answer the question asked, not what you think they are asking.
Think whether now is the time. Ensure that it is the right time to nominate, or consider whether you would be better to wait to the subsequent year to have appropriate evaluation data etc. to improve your chances.
Know that it’s not about the winning and that this (like submitting a grant or paper) is worth celebrating in itself.
This one gets a bit technical in places. Bear with me – the next one will be less so. Pinky swear.
This month has been a pretty one big for me. Last week, a clinical trial I’m involved with kicked off in Mali. 10% of Malian children die before their fifth birthday and this trial aims to reduce the level of infant mortality. The study is called the Lakana Trial and aims to recruit 100,000 infants born in Mali over the next three years.
In a separate post, at some point, I’ll tell you the ‘Mali not Bali’ story, but I’ll need a double G&T in front of me first. (Or register for free for Stand up for Healthcare Science on 6th November.)
At this point you’re probably thinking what on earth does this have to do with antimicrobial resistance (AMR)?
The thing is, to save all these lives, we’re giving antibiotics to every child (some will get a placebo). Nothing special about that, you might be saying, we give antibiotics to children all the time.
This is different because we aren’t treating symptoms of a known infection. We are giving antibiotics in order to reduce infection risk/inflammatory response in asymptomatic (symptom free) children under one.
The antibiotic we’re giving is a drug called azithromycin and it’s from a class of antibiotics called the macrolides (see my A Starter for 10 on Antimicrobials post).
The LAKANA study follows on from the MORDOR study (the best study name in the world, in my personal opinion!) which gave two doses of Azithromycin/placebo to >190,000 children born in Malawi, Niger and Tanzania. The difference between that study and ours: they always gave two doses and the infants recruited were up to 59 months.
Mortality in the MORDOR study was 13.5% lower overall in communities receiving azithromycin vs those that were given the placebo (paper link here if you’d like more detail). Interestingly, there were differences in the survival increase by both country and by age group, with the highest mortality reduction seen in Niger. The greatest effects were seen in the one-to-five month age group which is why the under ones were selected for the LAKANA study.
To decide how many doses of azithromycin are needed to reduce infant mortality, the LAKANA study will gather evidence to answer three specific research questions:
Does biannual azithromycin MDA (Mass Dosing of Azithromycin) to 1-11 month old infants reduce their mortality?
Does quarterly azithromycin MDA to 1-11 month old infants reduce their mortality?
Does quarterly azithromycin MDA result in a greater reduction in mortality than biannual MDA?
What has this got to do with antimicrobial resistance?
The AMR component of this study is the part that is being lead by UCL and the Institute of Child Health and so is sitting with me as a co-applicant. As we are giving antibiotics to children (and not treating a specific infection), it is crucial to understand whether this will impact on the level of antimicrobial resistance detected in them, their families and their communities.
Questions that we’re looking to answer (and that are currently running around my brain:)
If we do detect antimicrobial resistance is it stable? (I’ll explain this in a future post.)
Does detectable resistance return to baseline after a period of weeks, or does it lead to a permanent shift in their colonising bacteria?
Does any resistance detected make a difference to clinical treatment options? Macrolide resistance is usually due to accumulation of single nucleotide changes (single letters in the DNA code changing). This doesn’t necessarily mean the antibiotic will stop working.
Is resistance detected only in the Macrolide class of antibiotics, or does it lead to selective pressure that causes other resistance changes?
(Not AMR, but fascinating to me) How does azithromycin work? What is the mechanism? You would have thought this is well understood but, despite being available for decades, how it works as an anti-inflammatory is really not understood. Is the reduction in mortality because of its use as an antibiotic or because of this anti-inflammatory action.
What is incredibly important when doing this kind of work is that the first priority is to maintain the safety of participants. To that end we are working closely with the The World Health Organization who have recommended consideration of azithromycin MDA to under-one-year old infants, in areas with high childhood mortality.
Reducing infant mortality is so important: not just to survival but to quality of life and prosperity within these communities. These kinds of studies also need to be aware of their legacy. We are all incredibly keen to build laboratory capacity and infrastructure, not just in terms of equipment but also in terms of skills and skill infrastructure.
It’s early days and we won’t have any results from the AMR section for at least a year. I mostly wanted to record that this work is going on and the questions I have at the start. I also have some questions about balancing clinical outcomes which are pretty philosophical in my mind right now. If we see development of AMR, especially if it’s non-stable, but mortality is decreasing, where is the balance between those two things? How do you perform the risk assessment for the individual about short-term vs long-term outcomes? These thoughts convince me that this study is just the next step on a journey and that (as always) we have a lot to learn and a long way to go.