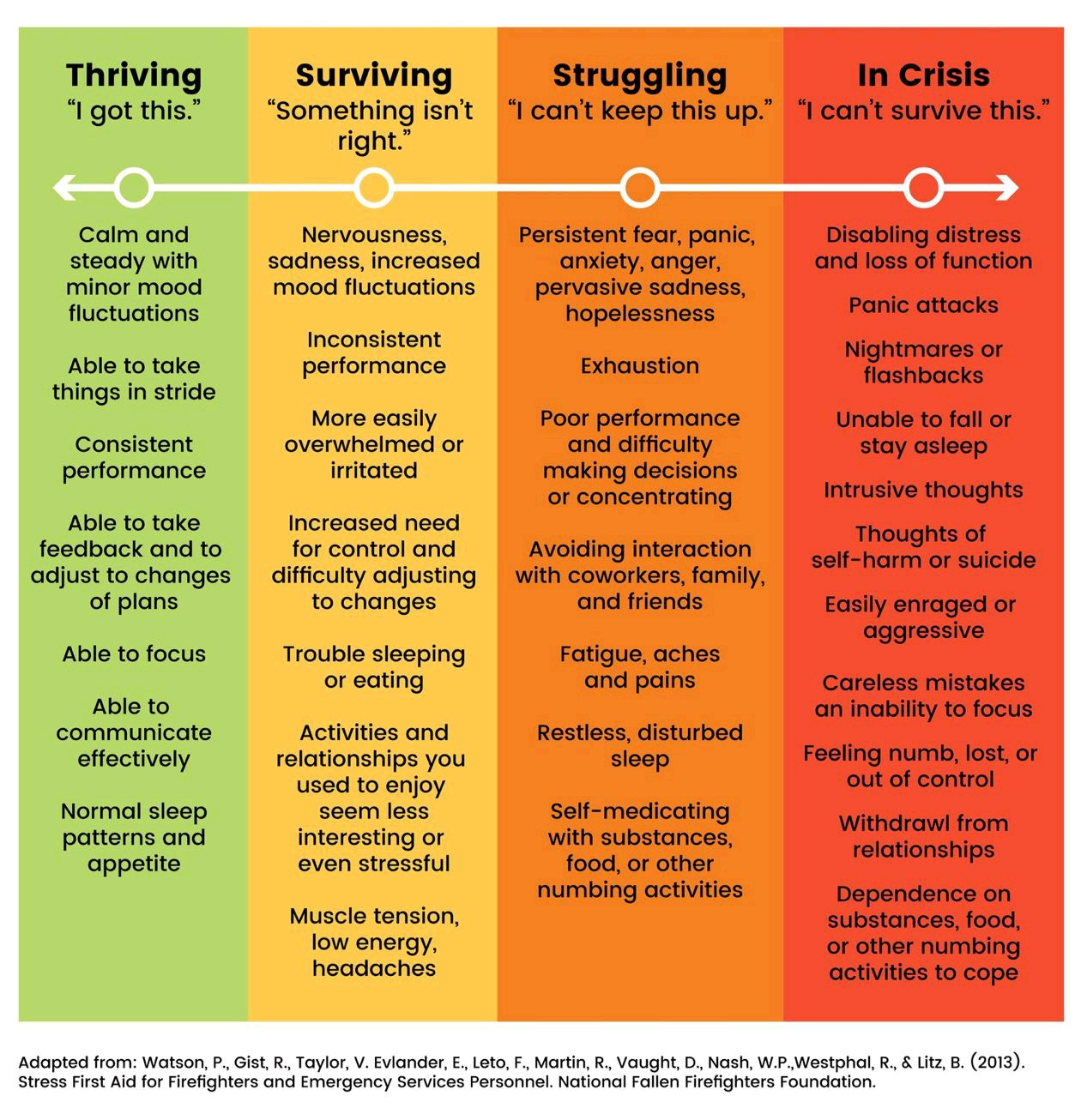
Having posted about some of the struggles earlier this month, and with another couple of weeks on clinical cover looming, I wanted to talk about why I love the job I do, and how it is so much more than most people realise.
On my first week in Infection Prevention and Control, I received a call and was asked to make a risk assessment about bringing in a Komodo Dragon in from London Zoo as it needed an MRI. It was at that point I knew that this was the job for me. I loved it then and, even in a pandemic, I love it now.
That brings me onto the first reason that I love it:
You Never Know What You’re Going To Get!
Those of you who have read the other articles on this blog know that patience is not one of my virtues. I thrive on, and really enjoy, variety and situations that force me to think creatively around challenges.
No two days in infection control are the same. In fact, it sometimes seems like no two hours in infection control are. I think that’s why I’ve found SARS CoV2 difficult: although there is responsiveness to the ever-changing guidance, the core of it is very much the same.
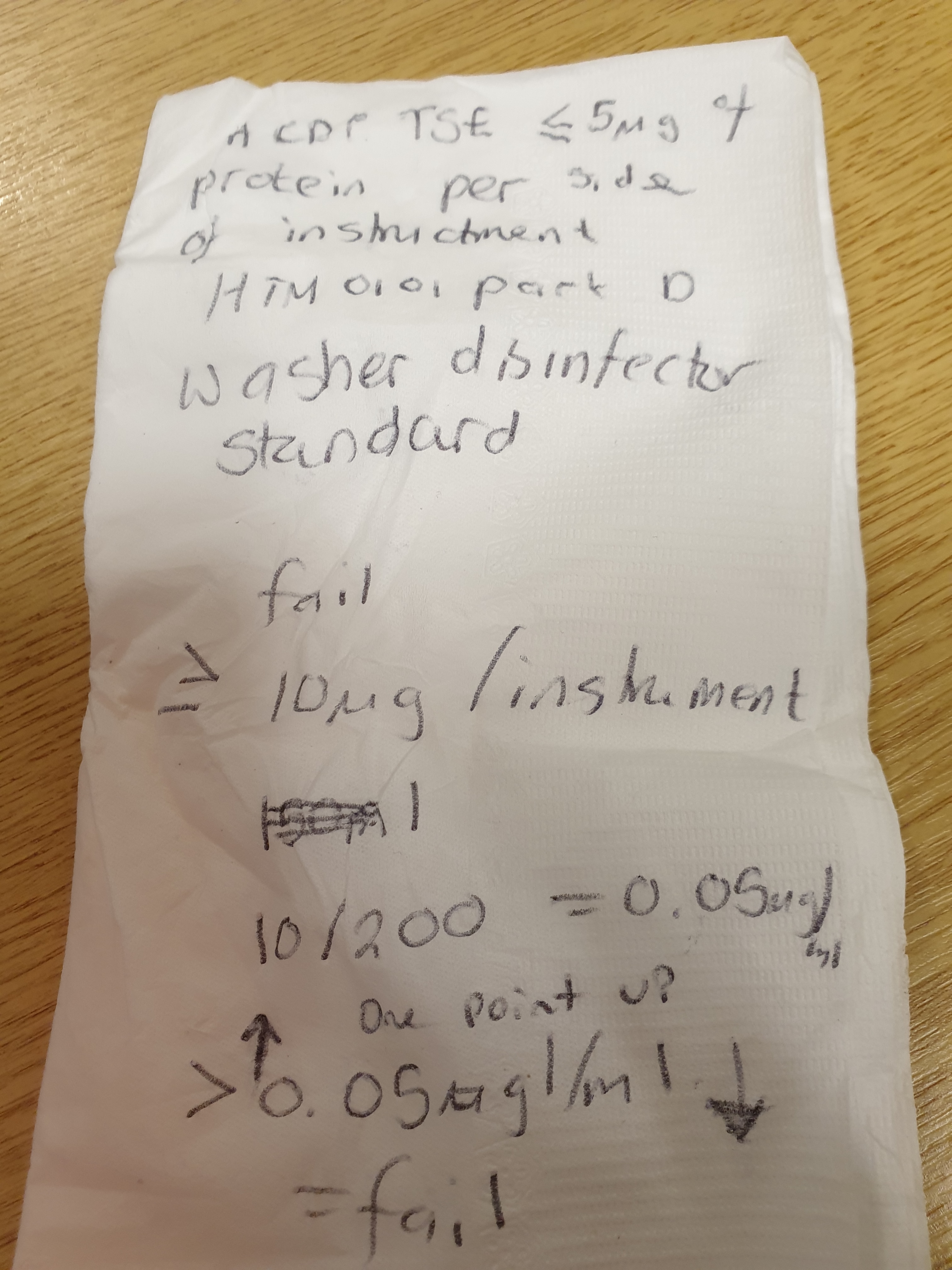
In infection control, one moment I will be speaking to a family and talking them through what an antibiotic resistant organism may mean for them. The next I will be talking to the wonderful scientists in the lab, discussing how we can improve typing to identify outbreaks and cross transmission faster. I’ll then move straight from that to a decontamination committee, where we will talk about how we need to manage surgical instruments to control prion (BSE) risk.
This was something I had no idea about when I started. I thought, like many people, it was mostly about hand washing. Instead I have responsibility for any staff, patients and visitors in the Trust. I don’t just cover hand hygiene and line care but I also cover laundry, pest control and things like antimicrobial stewardship programmes.
I love the creativity required to apply scientific and clinical knowledge to an ever-changing set of questions and the challenges that are created. It can be many things, but life in infection prevention and control is never dull.

It’s All About Teamwork
I sit in a multidisciplinary team that consists of medical and nursing staff, in a department filled with the most inspiring Healthcare Scientists. On a daily basis I will work with healthcare professionals across backgrounds, as well as academics and families. I’ve always been a people person (I think), that is what initially put me off a ‘standard’ laboratory science career: I thought I would be confined to the lab and feel quite isolated. The reality of this job could not be further from that.
I am, by instinct, most at home when collaborating. At its core, that’s what infection prevention and control is: a collaboration. One small team sitting centrally in the Trust cannot act as command and control for over 3000 staff and over 300 beds. In order to succeed we need to collaborate, co-create and allow those we are working with to have ownership of the best solutions for their setting, their patients, their workforce.
We are all very different people within the team, coming from different professional backgrounds. We also approach problems and challenges from different directions. The great thing about being in a team that is made up like this is that differences of opinion and constructive challenges lead to solutions that no single one of us could have come up with on our own.
I also find that having an academic, IPC and Healthcare Science Education team means that there is always space to go and be revitalised – both in terms of energy, but also creative thinking when things get too much. Again these different environments can give you a different lens by which to view a problem, and a different group of people to bounce ideas around.
I Get to Use All the Skills I’ve Picked Up Along the Way
I’ve definitely had a meandering path to where I ended up in terms of the science I’ve studied and the topics I’ve really enjoyed. One of the marvellous things about where I have ended up in terms of IPC is that none of that time was wasted. The studying of colloidal science, as part of my physics MRes, has been incredibly helpful in terms of some of the decontamination and surface modification decisions that I’ve needed to face. Similarly, the applied biofilms work I undertook, as part of my thesis, comes in useful all the time when tracking down environmental sources of outbreaks and understanding how cleaning agents may impact upon biofilm. Even my zoology knowledge has been useful in terms of some of the pest control decisions, as well as risk assessing animal visits and dealing with zoonotic infections.
I suppose my point is this: clinical environments are multidisciplinary and so I love the fact that IPC enables me to maintain that diversity of scientific knowledge and that it actively aids within my role.
Travel the World in Order to Share Ideas
Percy the hamster (who is officially our IPC mascot) and I have been lucky enough to travel the world in order to learn how to do what we do better, as well as share what we do. We’ve been on sabbatical to Boston Children’s Hospital for two months to become embedded in how they do things. We’ve been to academic conferences on three continents. On these trips, we never fail to meet people who will ask questions that trigger new ideas and new approaches. We also meet people and develop collaborations where we get to share what we have learnt from our practices, our decision making, and our mistakes in order to add to the shared learning within our profession. This is so important in order make progress for patients, in order to improve the quality of care we can give. It’s also why applying for research funding, so we can have these opportunities to meet and to transition what we learn into clinical practice, is so important. It is really where the science of IPC happens in order to make things better.

Finally, I get to do the most AWESOME stuff. Like the annual reindeer audit to check that it is safe for patients to meet Santa and his reindeer. We check that all the hand hygiene is set up and that the guidelines are there, but it also means that once a year I get to feed a reindeer some carrots. That right there makes any bad days worth it!

All opinions on this blog are my own