Whilst @Girlymicro is taking a well-earned break buying all her Christmas presents in New York, I’ve been loaned this wonderful platform to discuss all sorts of important matters in science and education.
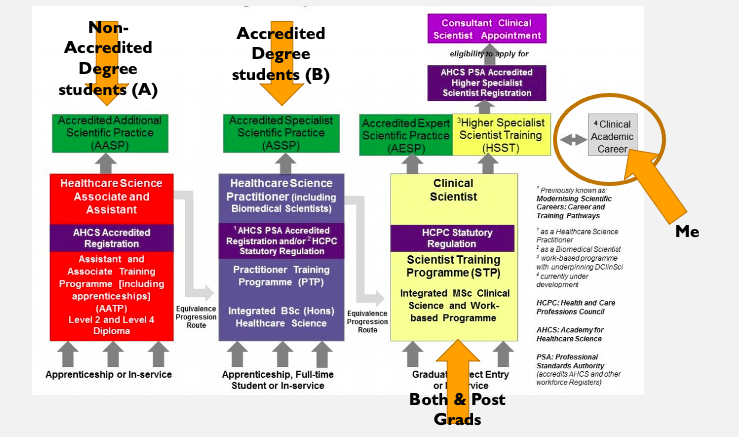
Recently I’ve been speaking a lot with students of all levels about different opportunities they have in the University environment. Things have changed a lot since my day, it’s not just a BSc then a PhD if you like research. There are so many exciting pathways for students in biological and biomedical sciences to follow, but it can become a bit of a quagmire trying to work out exactly which path you might want to take. I often start the conversation with students describing my own experiences at university and how I came to be in my current role, but increasingly I feel that they are now out of date and just aren’t relevant in the modern system.
It can feel overwhelming when you look at the decisions you have to make when starting university – do you take an iBMS accredited course, should you do a placement in industry or the NHS or maybe a year abroad, how about a Masters by Research degree, and what the heck is an MBio? Where are the best resources and who should you ask? Dusty old lecturers like myself will be able to tell you about the content of the courses, and all about our love of research. But we aren’t going to be able to tell you what doing a placement feels like, if it’s worth spending the money on an MRes or how to choose the right undergraduate course for you. To that end, I have asked some of my most engaging and eloquent students who are completing all sorts of different degree pathways to give us all some insight into what we can gain from the university experience in 2022 rather than, let’s be kind and say, my experiences which were more than a little while ago. And with that I’m going to hand over to reins to their expert hands.
Blog post from Daniel Nash
Who am I to write a blog post about placements?
As a Biomedical Science student on an accredited Biomedical Science course, the obvious path for me was to get myself onto a placement year working in an NHS laboratory to complete my portfolio and finish my degree ready to slot into a lab and begin helping patients. However, throughout my degree I felt this was not the path I wished to take and began feeling research was better suited to who I am. A placement is, I think, regarded as one of the best from to gain experience and improve employability while remaining a student and with all the perks that brings. And so, while looking into my options for getting into research positions and postgraduate degrees, I decided a placement year in another area would be a good idea.
My application process didn’t go amazingly, I don’t mind admitting, but given the competitive nature of placements, I’m still happy I got where I am. I was rejected from every single place I applied except for here, many on the grounds that from my biomed background, I didn’t have the specific skills demonstrated for the labs I applied to. So what placement did I get?
My Placement
I am working as a lab based analysist at Reckitt, specifically working on the Nurofen team, where I work in a lab to investigate and run tests on products across the Nurofen brand range. I have been working here for 2 months as I write this and have to say I have had mixed experiences so far. I know after this short amount of time that working in industry is not for me, but I also appreciate all the things it has and will teach me. The equipment I get to use, the analytical & investigatory techniques I will learn to use, and the independence and team working skills I will develop. All will be invaluable to be as I come out of uni looking for opportunities.
This placement was always going to be a learning curve, disregarding the skills I would learn, coming from Biomedical Science my chemistry knowledge was limited, and yet I landed smack bang in the middle of an analytical chemistry lab for complex drug formulations that I’m learning all the chemistry, toxicology, molecular interactions, analytical techniques, and terminology for. I alluded to before that this wasn’t even my first choice of placement and fighting through all the admin of a drug company at the same time made motivating myself to embrace the role harder than it should have been. but I have to give credit to my supervisor, Chander, for changing my mentality on this. We have weekly one to ones where he really emphasised the importance of using this year to learn take on new challenges and understand what I am doing. It shifted my mindset to try and look around the aspects I didn’t enjoy, and find what I could learn from it.
This is now my focus for the year to learn the skills & chemistry, understand the scientific method, and how the pharmaceutical industry works, better than I did before. Some would argue I should have thought this prior to embarking on a placement but being truthful, I think most people applying for placements know this to a degree but hadn’t internalised it like myself, (or at least need reminding of it when it gets tough as I did).
Aside from the academics
My placement was slightly unique in that there is a large cohort of around 20 students working across teams at the Reckitt R&D site, and so-far good friendships have forged, they have been great people to rely on through the chaotic onboarding stages. and we a placement group will work together on charity events, workshops and the all-important pubs nights throughout the year. I hope these friendships stand the test of time.
I’ve played with toxic chemicals, taken part in development of the newest yet to release medications going, and met some really great people all in the sub 3 months I’ve been here. I have to recommend a placement year or summer long, to anyone in a STEM field or beyond. You can’t beat the experience and growth possibilities it provides.
This week is pretty momentous for me. My boss and mentor of over 18 years officially retires. His name is Dr John Hartley and to be honest he’s a bit of a microbiology legend, so much so we are talking about having a sign up in the IPC office that says ‘what would John do?’. He is a completely different personality type to me, he’s an efficient, detail orientated perfectionist and most of all completely calm. When John is in a meeting he sits there in calm contemplation and then swoops in to ask the one question that cuts right through all the noise, right to the heart of the matter.
John has been my boss from my first day as a trainee Clinical Scientist 18 years ago, when i didn’t even know what S. aureus was, right through till last year when I got my Consultant post and became his replacement as Infection Control Doctor. He has been with me through marriage, deaths, PhD, FRCPath and every other significant career moment and so to say that I’m affected by his going is somewhat of an understatement. So how do we cope when these moments of big change come around and we have to find a new way forward?
Trying to remember I am enough
John is loved by so many people and I have looked up to him for most of my adult life. It is normal therefore that everyone is mourning his moving on, it is almost like we are all grieving the loss of the familiar. I definitely feel this. I also find it hard in another regard, as we all grieve as part of the change there is a lot of understandable discussion about how amazing he is both as a person and in his job. I feel this keenly. I also feel very exposed by it as the person who is stepping into the space he occupied. It plays into all of those aspects of imposter syndrome where you ask ‘am I good enough?’. As I said, we are very different people, John has an eye for details that I just don’t, he is calm and measured whilst I have a tendency to jump first and process everything of the fly. This means that I will never live up to ‘what would John do?’ and still be authentically me. There is therefore the inevitable chain of thought that if John is amazing at his job and I can’t be like John, does that mean that I will never be able to be equally amazing at that job? Am I doomed to mediocrity before I even start? It’s not like I’m a little bit ‘not like John’, the way we interact with the world is quite obviously different and so I’m very obviously not like him in every meeting I have and every interaction I’m involved with. It’s easy therefore to let the self doubt and panic set in.
So how am I managing it? I’m trying to not get too sucked into the John conversations. Not because I don’t think he is truly one of the most inspirational people I’ve ever met, but because for the sake of my sanity I can’t get drawn into comparisons. I’m trying to remember that despite the fact that he has occupied that role for my entire career that his way isn’t the only way of doing things, and that I have to try and play to my own strengths rather than attempting to imitate someone elses. I am also trying to hold onto the fact that at no point in the last year where I have had the role instead of him has anyone questioned my right to be in it, or has he disagreed with any of my decisions when I’ve sat down and chatted them through with him. He has been nothing but supportive of me being in post, and therefore if I’m going to emulate anything it should be the faith that he has in me that I struggle to have in myself.
I don’t have to have all the answers…….yet
John was Infection Control Doctor at my Trust for over 20 years, I have been ICD for 18 months, so what I need to ask myself is ‘am I comparing like with like?’. It’s tempting to benchmark in the moment, it’s tempting to compare how well respected and how established he is against how I feel I’m perceived. The thing is I’m benchmarking in completely the wrong way, I need to be benchmarking against how he was 20+ years ago. Otherwise I’m setting myself an impossible task; I can’t benchmark against him now as I’m setting myself up to fail, and I can’t benchmark against him all that time ago as I don’t have the data. That said, I suspect that Dr Hartley was probably born amazing and so it would be a challenging thing either way. So, should I be benchmarking against him at all? Should I instead be taking the time to reach out to my contemporaries to see how they are feeling and how they are dealing with similar changes?
The other thing that occurs to me whilst I write this post is whether anything has in fact changed, and whether benchmarking is actually the way to go at all. You see, the thing is, I’m not really comparing like with like. John is a Consultant Microbiologist from a traditional medical background, I’m a Healthcare Scientist. I’ve spent my entire career being the only person who was doing quite what I was doing and carving my own path. Why suddenly now that John is leaving am I abandoning the approach that has stood me in good stead and trying to be the same as everyone else, instead of embracing that difference in a way I always have? Why am I so tempting to discard everything that has previously made me, me? The more I question, the more I doubt and so I need to return to embracing my gut and knowing that I am exactly where I always wanted to end up, and stop being so scared that it will all be somehow taken away from me.
Take a leaf out of his book
If I’m not going to benchmark against him, what am I going to do? Well, first things first I’m going to reflect on what it is about him as a boss, a clinician and a leader that makes me and others respect him so much. I want to do this not in order to copy him or compare myself to him, but in order to be inspired by him to be better.
One of the things that John has done for me be, ever since I joined, is that he has championed me in rooms where I wasn’t present or wasn’t invited into. He has never let our difference in professional backgrounds stand as an obstacle to what he thought I could achieve and, when I’ve needed him, he’s fought tooth and nail to guard my corner. He has also sometimes been more honest with me than I could handle in the moment, and never stopped pushing and challenging me to be better than I believed I could be.
No matter what room he has been in John has always been his honest and authentic self, he’s not tried to curry favours, he’s not tried to manipulate or play power games. He has always gone into every room with both his staff and his patients at the centre of his decision making. The ability he has therefore demonstrated to handle conflict and disagreement is something that I can but admire. He’s not scared of being the lone voice in a room if he believes that he is doing it to give a voice to others.
All of these things are things that I want to do, want to be better at and strive towards every day. There will be times when I don’t achieve them, but by using him as a continued source of inspiration, rather than a benchmarking tool I use to beat myself up, I hope to become a better version of myself rather than a shadow of John.
Find my new allies
One of the other actions I’ve realised will be important for me in moving forward is be proactive in identifying new mentors and allies. People who will push and support me in being brave, and in standing up for both myself and others. Losing a keystone of your network and support mechanisms is always jarring, but it is also an opportunity to evaluate what your needs are now, and where you need to develop your networks further for the fresh challenges ahead of you. Finding mentors is often a fortunate accident, but there are also times when you need to actively seek out those people who will be able to help in any new phase of your career.
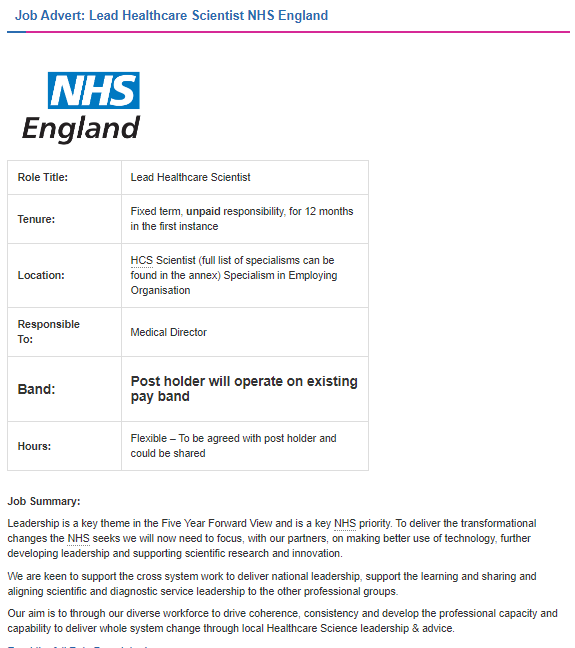
I’m also beginning to realise that I need to maximise my horizontal networks as well as looking upward for improved learning and guidance from those ahead of me. I’ve always found peer support like this organically, but I think the time has come to undertake deliberate action and to actively invest resources into it. This has been of great benefit in my role as Lead Healthcare Scientist but isn’t something I’ve attempted so much in my clinical role, partly because I suspect I’ve been too comfortable and had such great existing support. I have plenty of connections in this area, but turning those connections into something more requires time and the building up of trust and shared experiences.
I will have different battles and different challenges
Firming up networks and identifying new sources of support is important as well because I think the challenges ahead of me are going to be different to the challenges I’ve already faced. John has done an amazing job of leading the way and has built excellent foundations for me to stand upon, but the world of healthcare has changed so much in the 20+ years he’s been in post, and it would be naive of me to think it won’t continue to fluctuate. All of this means that if I am going to be able to tackle these new challenges and prepare for a dynamic future, I can’t just rely on what has been before. I need to have my toolbox ready to enable me to deal with what lies ahead, and a really important part of that is making sure that I have people around me who will challenge my thinking and inspire new ideas. If we want to create real change and improvement we have to be prepared to take a leap into the unknown. Sometimes this is helped if you have people around you who are both supportive but who can als give you a little push to get over any hesitancy. Although, in my case, it’s more likely they may need to stop me gambolling down the road with too much alacrity. Finding your tribe has always and will continue to be important to me.
Perhaps one of the reasons I find this all so hard is that the reality is hitting me that I’m no longer the new kid on the block. I’m no longer the young whippersnapper who is coming in and seeing the world in a completely different way. I myself am becoming the old guard, I’m becoming the person who has been somewhere long enough to harken back to different times when things weren’t the same. This presents a lot of cognitive dissonance when at the same point you still feel like you are new and haven’t quite got a handle on things. Just merely realising this helps, it helps to see the strength in where I’m at. I am still young, I am still new, and the position is novel enough to me that I can see 101 ways where I would like to grow it and me for (fingers crossed) the better. I have also been in the Trust for long enough that I know how things work, I know who to speak to, I know where the barriers and opportunities might be. If you look at it in this light, I am in the best possible position to embrace what is to come. So, although I am still grieving the loss of the past, I am beginning to be excited about the future.
It’s that time of year again and many of us will be taking on new trainees, getting to know new students or supervising new PhDs. I thought it was time therefore to share something that I’ve found increasingly useful and have now set out to cover in initial meetings with learners, and that is the development of learning agreements.
What is a learning agreement and why is taking this time worth while? Surely everyone knows what they’ve signed up for when they take a training place? The truth of the matter is that students often know the logistics of what they’ve signed up for, but any learning placement is a whole lot more than just the nuts of bolts of the curriculum. There’s a lot of expectation setting/management required for one thing. We’ll cover what learning agreements look like in a bit, but in short they are agreements based on conversations between the learner and their supervisor where they actively set out the expectations and boundaries of their relationship.
At STP/HSST and PhD level it can be the learners first experience of formal education routes within a professional setting. As supervisors we often expect learners to be able to undertake independent study at this point, identifying their own learning objectives and being responsible for any escalations. If this is the students first experience however, they may believe it will follow the pattern of the prior learning they have experienced, which may have placed a lot more focus on structure and consistency.
What is a learning agreement?
In light of these complexities what is a learning agreement and how can it help? Well they take quite a few different forms depending on what it is that you want them to fulfil. In short they are a working (and therefore dynamic) agreement between you as the supervisor/education officer and your new student/trainee. I tend to refer to them as learning agreements rather than contracts as the term contract to me implies penalties and learning contracts are what I escalate to if challenges occur during the time someone is with me.
They can include all kinds of things:
What topics are in or out of the learning objectives
How deadlines will be set and a broad plan of work
Expectation setting around students identifying additional learning objectives
Ideas for how the learner will benchmark their progress and/or learning
How the educator will assess progress/learning
Although the above is often the framework the most valuable parts of a learning agreement for me are less structural. It is my time to ask:
What kind of learner are you?
What kind of support do you prefer (close vs supportive supervision)
What are your main objectives that may or may not be topic based?
What are you hoping this will lead to?
How do you prefer to communicate, face to face, email etc?
Why this course? Why this training? What attracted you? In order to understand their drivers
Making the implicit explicit
In general I think most of us are good about talking about the nuts and bolts of what a course/placement entails. We are good at giving the ‘this is the bathroom’ tour and ‘this is where your desk is’ plus ‘our supervisor meetings are on Tuesday’ type of information. What I have discovered over the last few years however, is that imparting curriculum or logistic based information just isn’t enough to support a good supervisor-learner relationship, where both get what they want out of it.
I think as supervisors we have quite a lot of expectations that we don’t necessarily voice, after all for many of us this is something we do a lot of. It can therefore be easy to make assumptions about the level of awareness of these expectations from someone coming into that supervisor-learner relationship with us. The thing is, you may have been doing this a loooooong time, but your learner almost definitely hasn’t. They won’t have that implicit and often organisational linked cultural knowledge that you have been embedded in for so long. Worse than that even, they are likely to have a whole lot of different assumptions based on their last educational experience that they are bringing with them. Unless we all work therefore to make things that we implicitly understand explicit, you won’t know where those differences in practices and expectations lie. It is when this happens that problems often occur that could easily have been addressed early on, but have significant impacts on learner experience and supervisor stress levels.
Supports orientation to a new field/culture
As I’ve said a few times culture matters, as culture and cultural norms are intrinsically linked with the expectations we all have. Having these conversations is about more than expectation management however. Learners are coming into an environment that may be pretty alien to them. This can make students feel like they are floundering, right from the start, meaning that they don’t feel like they fit. A small percentage of students are likely to walk away because of this, not really understanding the cause. This is often combined and amplified by the fact that they may have moved or lost their support networks in the transition.
Talking about your role (and similar roles) with learners helps, not only to build your relationship and set expectations, but also to support them in making the transition into being a scientist in practice, not just in name. It took me years to feel like a scientist, to feel comfortable calling myself that, to feel like I belonged. Having conversations where students understand what it takes to succeed as a scientist, not just in a placement, can be invaluable to learners re-establishing support networks. Also, supporting learners to find other trainee groups, to join twitter, or of timings for lunch clubs, can help them settle into their new role and their future profession.
Setting matters
Having these conversations can feel uncomfortable and challenging, mostly because of the fear of the unknown. They may also take time we may not have. All of these are reasons to make sure they are done correctly and given the time required. If you are nervous having them with your learner then imagine how nervous they may be to have them with you. You are asking for a lot of honesty and self reflection from someone who doesn’t know you well, in a relationship where trust may not yet have been built. Furthermore, you are asking for all of this in a relationship where you probably have all the power and where your learner is likely to be highly keen to please, rather than representing their true self..
So how do we hold these conversations and support them getting the best outcomes? I think there a couple of things we can be mindful of. The first is not dropping them on the learner. If we want the conversation to deliver we both need to do the work. I need to be honest with myself about time and also what kind of supervisor I am. The student needs to be given the questions or a framework beforehand and supported to have time to reflect on themselves to be able to answer the questions asked. They may need to be encouraged to speak to friends or family to support them in this reflection if they’ve never done it before. They can then start the process of reflection by thinking in the presence of people they trust, if needed.
Think about where you physically want to have the conversation. I tend to take learners out, to a none Trust space where we can have tea and cake (or other suitable consumables). I’ve written before about the power of tea. The main reason that I do this is that it means we are no ones turf, we are in a neutral space, and the provision of food further helps to reduce/remove hierarchy. When thinking about where however, you need to consider privacy. Your learner may need to share things that are private or important to them, and so considering the type of location is also important.
The other important thing about getting the conversation right is setting the conversational scene before you start the conversation itself. You need to be clear about the objectives that you want to achieve, why they are helpful to both parties and set some ground rules. It’s key to say that honesty is the most important part of this process. It’s OK to have styles that don’t match, by knowing this early you can sign post and find additional support to ensure that the learning process itself still works.
What happens when the expectations don’t match
Hopefully by going through the process of creating a learning agreement you will avoid any significant bumps along the way later on. The process needs to be done thoroughly though, so you don’t just hear what you’d like to hear. As stated above it’s ok to have areas of difference, it’s what you can flex in response to that information and how you respond that matters.
For example, I am never going to be a good micro manager, I have neither the time or personal inclination to work this way. I have fallen foul of not having had the learning agreement conversation and subsequently had learners who felt they were inadequately supported. If I find out that I have a learner who feels they need close support I need to therefore make some pragmatic choices. Is it they will need close guidance for the transition period? If so I can likely change my style for a period of a couple of months in order to support that orientation to a new location. Is it that this is their learning style long term? In this case I need to think about pairing them up or seeking support from a colleague who is better able to provide that close support during the periods in between our catch up sessions.
I have also struggled previously with learners who have not met the outputs that I had expected. This may be more of an issue with PhD students, but to be honest if I’m not clear about publication expectations how will they know? Therefore if it becomes apparent that the timeline expectations don’t match it is worth considering drawing up a broad, high level, delivery plan so you are both working towards the same mental models
Finally, it may be that learners make it clear that they have pastoral care expectations that you may or may not be able to support. Prior to going into these sessions it is important to be aware of the different additional support services that learners have available to them. Whether they need them or not in the moment it is crucial that you sign post to these, especially if you are not the kind of supervisor who will take on this kind of support role. Additionally, there are likely to be plenty of networks that offer peer support that you can sign post learners to. There will always be things that they want to talk about that they won’t want to talk to you about. Let’s be honest, no matter how well you get on there will be times they need to moan about you as a minimum. Being open about this being OK and linking them into peer groups can be incredibly valuable
No matter what you hear in this space it’s important to be open and judgement free, in order to support honest sharing. If you hear something you don’t agree with it’s important to take a beat and try to understand the drivers of that view point. By being open to opinion and challenge now you are investing in success later on. I don’t know about anyone else but I studied in a different time, my undergraduate degree finished 20 years ago. My expectations of learners and learner experience therefore is, to be frank, well old. I’ve also worked in one place for 18 years. It is naïve therefore to believe my experience and expectations are going to perfectly match the learners who are coming through now.
There is a big difference between being someone’s educational supervisor and someone’s manager. In some cases we are both, but we need to understand that they are different roles with different requirements on both sides, and be aware of what hat we are wearing when. Techniques such as learning agreements can help make sure that we do the ‘education’ part better by having the kinds of conversations you would not have with someone you just had a managerial relationship with. It encourages self reflection, expectation management and consensus forming. All of which are skills that we should be modelling for those learners we are supporting. If you don’t ask, you’ll never know. So let’s start this new academic year by having conversations better and talking about how we can all be the best we can be.
Its 6am and I’m sitting listening to fire alarms go off in my hotel room at FIS/HIS. I’ve been up since just before 3 in a shame spiral of all the stupid things I said during day one of the conference and only just got back to sleep at gone 5am when the alarms started sounding. Frankly this feels like a metaphor for how my life has felt for the last 2 years, long and short the constant sound is exhausting and stressful. An hour later the alarms are still going and I’m now doing the only thing possible, which is to leave my room in some highly elegant nightwear and take myself, a laptop and a cup of tea to sit in reception to write. I may be looking a humiliating level of baggy eyed exhausted shell but at least it quieter and I have caffeine; which brings this metaphor all the way up to 2022. It’s better, I’m happier but oh lordy am I still broken. So as we sit in our 3rd year of dealing with the pandemic how are things different and how are they the same?
The things I love doing are so close to being back
One of the things that is currently saving my mental health and well being is that you can almost now envision the point where normality could return, or the new normal anyway. I know that if you have listened to politicians and social commentators recently you would think that normal is already here, but for me we’re not there yet. I can however do things like think about booking tickets for the future events (I cannot wait for Eurovision!) and hope they will go ahead, I’m contemplating planning trips and have started seeing friends in slightly less controlled ways. I’m even sitting here typing this at an in person conference, which has been surprising lovely and not stressed me out in the way I thought it would.
This being able to vision is important to me, it’s also important to me in the day job. For a long time all there was was SARS CoV2, you couldn’t plan, you couldn’t see a time when you would be able to do anything else. Now though things that give me so much joy in terms of education and research are coming back, papers are being drafted, grants are going in. I can see that we can begin to focus on other things with changes and improvements that need to happen. It may still feel like a shock but after all healthcare is NOT all about respiratory viruses and there are things beyond that which impact patient care that we need to take some time to focus on as well. All this said however, I have to re-state how tired I am and it is yet to be seen whether I have the inner resources to hit the ground running in the way that I would like.
Back on the carousel
Having just said how happy I am to be getting back to doing some of the ‘normal’ work of Infection Prevention and Control, there’s no getting away from the elephant in the room. We’re still dealing with a global pandemic, which a lot of the world seems to have forgotten. We’re still managing guidance changes, testing cases, investigating and managing hospital cases, but now with all of the funding support withdrawn and whilst being expected to also manage ‘business as usual’ on top of everything else. All that with having had 2 years of no sleep and no rest. In some ways, and this could be me, everything else is also more of a mess as we’ve been in crisis mode for so long. It’s not even as if the ‘business as usual’ is straight forward no even taking into account how much re-training needs to be undertaken.
Because of all of this sometimes it’s hard to tell whether you are on a nice gentle carousel or are actually on the waltzers, trying to manage everything thrown at you in a landscape that is still constantly changing it’s priorities and demanding responsiveness to everything that is being put in front of you.
Single interventions don’t work
Everyone in the world still appears to be an expert in IPC and there still seems to be so much reductionism linked to the idea that a single change will revolutionise everything. I’m a little ‘over’ trying to have the discussion with people that covers the fact that almost all IPC is about introducing packages of measures/interventions. It’s what is often frustrating as a researcher, in that single interventions are therefore quite difficult to evaluate for their impact, but the world we live in clinically requires us to be able to control multiple risks and therefore manage multiple risk mitigation strategies simultaneously. The truth of the matter is that a single change will rarely control risk in the complex environments that our patients are in, even without adding the complexities of human behaviours and human interactions. I’ve written about this before, but I strongly believe we need to become comfortable with complexity and that part of our role in IPC is to assimilate complex multicomponent information, process it to make a balanced risk based set of decisions to establish a strategy, and then to implement that strategy in a way that appears simple and practical to those that are implementing. Taking the complex and processing it so that it can be disseminated in an accessible way is, I believe, one of the key talents of many IPC teams. We need to communicate this better as being one of our strengths and move away from single intervention focuses.
Could do with a little less ‘interesting’
I don’t know about anyone else but i could do with less (take your pick) of monkeypox/lassa fever/polio/Burkholderia/invasive Group A Strep or any of the other ‘interesting’ alerts that we have had lately. I would normally love something novel to get my teeth into, but right now the ‘interesting’ seem to be coming thick and fast and I for one am only just managing getting back to MRSA and resistant Gram negatives. The constant ‘organism of the week’ just means that any return to balance feels like it’s going to be slow coming. I hate routine, it’s one of the reason I got into IPC, but even I could do with a little routine and boring for a while to find my centre and recover a little and recharge those batteries before embarking on the next new thing.
Summer down time isn’t so quiet
I think this has all been compounded by everything that has happened over spring/summer. Summer is usually the time in IPC where you can catch your breath a little, where you can plan for the inevitable challenges of winter and do the visioning piece to work out how you want to develop the service and move it forward so that everything works just a little better. This summer though there’s been little to no respite really, between new variants and waves earlier in the year and the new and ‘interesting’ since. Summer has been anything but quiet. This means that you know you are going to go into, what is predicted to be, a difficult winter without catching your breath and still trying to spin plates, with even more work having been pushed back to 2023. I think we will all still pull it off and I truly believe we will manage most of the things we were all hoping to achieve during the summer lull, I just fear that to make that happen we will carry ourselves into another winter running on empty. I think therefore we need to have the conversation with ourselves now about being kind, not just to other people but also to ourselves, and where you can plan accordingly.
Do more with less
All of this comes at a time when we are all very aware of the pressures on services and the resource limitation issues we are all facing. We can’t just do the same with less but we have to do more with less. The COVID-19 money has gone, the extra staffing support linked to it has gone, but a lot of that work hasn’t disappeared as we are all playing catch up on waiting lists and clinical work. It is easy therefore to feel pretty disheartened about the hill we need to climb, having already given up so much, both as individuals and as a collective.
The truth of this however is that some of the very pressures that sometimes feel like they are crushing us are also bringing some benefits. I am closer to my team than I’ve ever been. I’m more certain of the things that matter to both me and my service. I have significantly more clarity than I’ve ever had before both about my professional and personal life. Limitations on resource access have meant that we’ve had to worked harder to develop networks and build connections in order to use what we have better, and that connectivity has other benefits. So as much as I hate the words ‘better value’ I can see both sides of the coin, and not just about the money. I can see that it will make how we move forward better as we will move forward more together than we have ever been before.
The inevitable post mortem
One of the things that struck me when I went through my first pandemic, swine flu in 2009, was the way that you could do nothing right for doing wrong. One minute you are heroes and the next you are villains because it’s politically expedient and someone has to be the focus of dissent. I know people that were upset by headlines during the Tory leadership contest that basically went after many of us who had stepped up on top of our standard roles to offer help and support. We stepped up because we felt it was the right thing to do and despite (in many cases) significant personal cost. Sadly, having been here before i was not surprised. Worse than that, I think we need to prepare for the fact that this will be the theme over the next 12 to 24 months, and that we will be used as a political football by many people. Hindsight is 20:20 and retrospective data analysis is a very different beast to prospective decision making. So my advice on this one is that we all need to develop a thick skin, understand what the drivers are for the headlines, and let it wash over you rather than taking it as the personal attack it can sometimes appear to be.
So having said all of this what do I think the next few months will hold? I think we will continue to be challenged, both in terms of the patients that present in front of us and in managing the service demands this places upon us. I do think that IPC teams and healthcare professionals will continue to step up and do what needs to be done to make care happen. As leaders however, we need to be aware of what that ask looks like and have strategies for managing it in an already tired work force. For me being able to focus on the future is how I get through the present, therefore planning for normal times is key to my survival. People ask how I’m putting in grants, drafting papers and planning change. I do it not because I have time and capacity, I do it because I have no other choice. I’m aware that it’s key to my survival, to keeping me grounded and enabling me to cope with the stress that exists in the now. Some people ostrich, I plan. As people are different however, I also know that my planning can stress others and so I try to be aware of how much I talk about the future to those people who are opposite and survive by living in the present. Dealing in the best way possible right now is mostly about knowing who you are. The clarity provided by the last two years of the pandemic has helped me in this by forcing me to know more about who I am and how best to manage myself. I have learnt and I hope to continue to use this learning to grow. So I will continue to hit the day dream button and drink tea……….I hope you find a way that works for you.
I thought I should start with an apology, this one is all about me. There is a point to it but you may have to get through a chunk of stuff about me first. If you don’t fancy that there are links to some of my other posts at the bottom that you may fancy more.
Everyone tells you that academic qualifications aren’t everything and they really are not, depending on the path you want to take. In many ways the more qualifications I have the more I question their validity, but I get to do that now from a position of privilege where I no longer really have any skin in that particular game. That said A-level and GCSE results have come out in recent weeks and it got me remembering the day I received mine, more than that it made me think about every time I stood there waiting for a sheet of paper to be put up on a wall or to open an envelope (yes I am that old 😉).
If you look at my CV now you’d see a pretty good list of academic achievements but there are things that you don’t see. Past a certain point no one lists their GCSE or A-level grades. You also don’t see the fact that I have never been the smartest person in the room, I’ve never been the top. The reason you don’t see it is because none of that actually matters, it’s about the body of work rather than a single point in time. When you get those results however no one tells you that or even if they did you probably wouldn’t believe them. Those results are your whole future, they feel like your whole world. I wanted to just write something to put out there that shows that no matter what you received it doesn’t have to define either who you are or your future, it’s just one step on the way.
GCSE horror show
Frankly my GCSE years were a bit of a horror show. Not because I didn’t want to study or engage but health wise it was basically a disaster. I caught glandular fever (Epstein Barr virus) and ended up with such bad swollen lymph glands under my arms I couldn’t lower them for days at a time and turned yellow due to the hepatitis. On top of this I slept 23 hours a day and it just didn’t get better. I ended up with post viral fatigue and for my 5th year at school managed an hour a day, on a good day. I was withdrawn from all but the basics (maths, english and double science) and told I should plan for failure.
I sat no mocks and frankly had no idea what day it was let alone feeling on top of anything. School became a terrifying place where I could see everyone else moving on rather than a place where I fit in, as I had loved to study. I never really had a lot of school friends but all but one basically forgot I existed (cheers to Heather who always stood by my side). I missed all the big occasions, no last day of school with signatures for me, no last school disco. I was just left behind and I really started to believe the tale that I was being told that my aspirations were over.
Things got worse when I sat the exams. I managed a weekend of revision pre the written papers, although it really blew me out. I did that awful thing of not really reading the instructions as I was so nervous. My english literature exam was up first and instead of answering 2 of 5 essays, I answered them all. I couldn’t understand why I was furiously writing whilst everyone else looked so calm or had finished with loads of time. It just fed into my panic. With 5 minutes to go I finally finished and went back to the start to see the words 2/5 glaring at me from the front page. I felt like I’d screwed it on day 1.
Come results day I just didn’t even want to go. I was so convinced of my failure and that I had sealed my fate. I had no plans for next steps, I had no college or A-level plans. I picked up my envelope and I suspect other people’s tears were for very different reasons. My 2 A’s (english lit and language) BB (duel science) and C in maths were so far from what I had hoped for at the start but were so unexpected on the day. Everyone stood around me with 11 and 12 passes but my 5 meant that I was still in the running. I still had a chance. I went back home and went to bed for a week, there was no energy for celebrations and dreamt of what next.
A-level winging it
As I said I’d made no plans for A-levels as no one thought they were an option. My mum (who is loyal, devoted, loving and probably a genius) swung into action in a way that I will be forever grateful for and don’t deserve. She got me a last minute place organised to do A-levels at the secondary school less than 5 minutes from my home. My original school were so focused on grades and success that it wasn’t even discussed as an option. So 3 weeks later I’m due to start at mixed sixth form, having only studied in a single sex environment since 11, with no one I knew, having never even visited the school. Nervous was not the word. The school knew about my health issues and to be honest the word university was not being mentioned. So that I could manage health wise I started A-level biology, which happened in normal school hours, and A-level drama that had some evening classes so I could rest during the day. That was it. 2 A-levels. Only 1 of which was considered serious. I set to it.
In what will become a theme for my life I felt so far behind. For my GCSE exams I studied the minimum possible to be able to pass for a weekend, that did not enable me to keep up with my peers during A-level biology classes. I was the idiot who knew nothing, understood nothing. If I had had friends I probably would have understood earlier that most of my class mates felt the same way but I didn’t, the switch from GCSEs to A-levels is hard but I thought it was just me.
Drama on the otherhand was a revelation. For someone who was struggling to find a refreshed version of her identity and new place in the world as the plan she’d had was falling by the wayside, drama was my safe space. You could choose to be loud or quiet. You could often choose to watch or engage. I was in a place where my choices were given life. Not just that but I didn’t feel behind, the texts were new to everyone, it was a very different space. I still didn’t fit, on the first day they thought I was their teacher not a student, but being able to academically engage in a place I didn’t feel like a failure was something that gave me hope, it kept me going. It’s partly why I’m still so passionate about the use of STEAM now. When I had no other way of being me it helped me find myself.
By the end of my 1st year of A-levels I was beginning to feel a bit more like me, a bit more able to think about the future. I still wasn’t physically right but my mind was a bit more back on track and I wanted to be able to plan again. I knew that if I wanted to even apply for uni that I would need 3 A-levels plus general studies and I only had 2. Let’s put to one side that I had no idea what I would apply to study I just knew that 3 A-levels was the first step. As I’ve said the school where I was doing my A-levels did evening classes that were open to everyone. I can’t even remember how it happened but I found an amazing psychology teacher who I spent some time talking to and who said she would help me. We came up with a plan. There was no way I could cover 2 years of psychology in 1 but I didn’t need to. The course was split into core and optional modules. If I took some of the evening classes and some of the day classes across years I could still cover all the core components. I then just had to cover 1 optional and make sure that I knew it super well as I’d have no essay options – I’d have to be able to answer the one that came up. I also registered on general studies knowing I would just have to turn up to the exam and hope as I wouldn’t be able to physically manage any more classes.
I also knew that despite ‘the plan’ I wasn’t going to be well enough to manage full time uni the next year and so I would give it everything I had and then defer my place for a year.
I basically spent that year working and sleeping. I didn’t have much left in the tank for anything else, but I had a plan. I also had an amazing cheer leader in my mum who repeatedly let me know that her love was unconditional and that she had my back, but I could also stop at any point if I wanted to. The choice was my mine. That word choice is so important when you feel like your options are taken from you. I chose to go for it. At the end of that year I got my envelop. The uni’s I’d applied to required ABB or 3 BBB with the A or B in biology. I got 2 As a B and a C. The C was in biology. The A’s were in psychology and drama. I didn’t get in. I can sit here and say that the fact that I managed to get passing grades was amazing, that to come from nothing to a C in biology was such an achievement, but none of that is true. I felt crushed. I felt that the people who told me I couldn’t make it were right and what was I thinking. Then someone stuck me a room and handed me a phone and told me to call clearing. I had no idea what clearing was or what I even want to study, but somehow an hour later I’m going to a city I’ve never even visited (Liverpool) to study a course (general science) which I didn’t even know anything about – apart from the fact that it would enable me to choose my science speciality later on which at that moment felt sooooooooo important.
Everyone moved past me once again as I deferred for a year and focussed on getting well. I also took a part time job, not only to help me earn some money for uni (we weren’t rich and I’d need it) but also so I could see how I managed to see if I was OK to go.
University catch up
I turned up for my first week at uni and if A-levels had been a shock they were nothing on this. EVERYONE and I mean EVERYONE seemed to be more prepared, understood more and frankly knew more than I did. I had been so relieved to just arrive I hadn’t planned for what would happen next. As it turned out 3 main things occurred:
One – I learnt the importance of finding my tribe
Two – I learnt to hide my fear and insecurities
Three – I found ways around things so that I could hide my knowledge gaps
Now, some of these I’ve written about separately on this blog, like finding your tribe, and as a life lesson it has stood me in so much good. I found a small group of people who I could learn with, who didn’t make me feel foolish and behind, even if I didn’t ever really share with them how I felt. One person in particular, Diane, became my study buddy and we would have late night chinese, work out pass margin requirements and all in all keep each other going. She was a bridesmaid at my wedding and I was maid of honour at hers, if it wasn’t for Diane I wouldn’t have made it through. She’s northern, straight forward and stopped me listening to the voices of doubt and fear that troubled me in the middle of the night.
As for the other two things I learnt they have their pros and cons. I’ve reached a point in my life now where I’m pretty open about my fears and insecurities, I write this blog after all. The thing is fear festers because we don’t talk about it and one of my motivations in writing this blog is so that others don’t feel alone in their self doubt and their challenges. I can do that now though as someone who has worked through a lot of them and who has (thankfully) gotten to a place in her life where I’m less bothered by what people think of me than I am in trying to help others find their way. That certainly wasn’t the case when I was a 19 year old who was still struggling to feel like she belonged. This is an after uni story, but I still remember my first week as a trainee Clinical Scientist and having people stare at me as I tried to pipette into an agarose gel, and having people comment on whether I was back pipetting and how interesting my style was. I had no style. No one had ever taught me how to pipette, I had never run a molecular test, I was a Zoologist who ended up in microbiology after all. I therefore had to learn, especially in the competitive environment I was in at uni, where the bottom 50% got booted every year, and as a trainee to cover and not let my lack of skills be seen for fear of what that might mean for me.
I spent my entire time at uni volunteering to do the drawing or take other roles because no one had ever shown me how to focus a microscope and I was terrified that I would be found out. This haunted me enough that when I sat FRCPath I actually had close friends run trials for me on different types because even the memory of it gives me panic attacks to this day. No one ever showed me how to do dissection and so again for my first 2 years at uni I covered and did the best I could. It was assumed that everyone had gone to schools that had access to equipment, that had run these types of classes and then to add onto to that my lack of experience due to illness, it all just meant I felt at sea. In my third year I faced an eight hour dissection exam and I knew it was going to be a disaster. After three years of uni though I had finally found a lecturer I trusted and a couple of friends who I felt would stand by me, and so we approached as a collective and asked to be allowed to have specimens and practice on weekends. Me and my dogfish George got an A in that exam and I cried in a way that is only rivalled by passing FRCPath. It took me three years to have enough trust in other people and myself to ask for help, not because I was afraid to do the work, but because I was afraid of what it would mean if they rejected my request.
So what does all of this mean and why have I written it. Firstly, I’ve written it because I want anyone out there to know that if things didn’t go well for you there are still pathways ahead. We may not take the most straight forward path but we end up in similar places and sometimes the learning that will give us will be invaluable for the rest of our lives.
Secondly, I want those of us who are now acting as educators, leaders and supervisors to bear in mind that not everyone is joining you at the same point. There will be smart people out there who are turning up at day one who will not necessarily have had access to the resources or opportunities you think they have. Making assumptions that everyone is started from the same place sometimes puts people back even further. This is especially pertinent as we have trainees about to start with us. Taking the time to have a non judgement based conversation about prior experience can make all the difference to those who feel lost in our world where we take so much for granted.
Believe it or not there are so many things I’ve learnt about myself that I see the way I got here as a strength and not a weakness. I’ve never been the one at the head of the class, and the route that I’ve taken, although circuitous, now pays real dividends as I understand so much more than if I’d taken the direct route. It’s also taught me valuable lessons about myself, what I value and what I can achieve if I can get over my fears of how people see me. I’m used to hearing no, I’m used to hearing that’s not how it’s done and that it won’t work for someone like me. All of those things felt horrible but now I’m so thankful. Those no’s have taught me to be strong and to break down barriers. Those no’s have in the end enabled me to truly be the person I wanted to become.
Finally, and I can’t say this enough, find the person who sees your value even when you can’t. Find the people like my mum, my husband, like Heather and Diane. Find them and even when you haven’t got the strength to articulate what you are truly afraid of they will still be the people who stand by your side and guide you. Find your tribe and you will never truly be alone again.
All opinions on this blog are my own
If you would like more tips and advice linked to your PhD journey then the first every Girlymicrobiologist book is here to help!
This book goes beyond the typical academic handbook, acknowledging the unique challenges and triumphs faced by PhD students and offering relatable, real-world advice to help you:
Master the art of effective research and time management to stay organized and on track.
Build a supportive network of peers, mentors, and supervisors to overcome challenges and foster collaboration.
Maintain a healthy work-life balance by prioritizing self-care and avoiding burnout.
Embrace the unexpected and view setbacks as opportunities for growth and innovation.
Navigate the complexities of academia with confidence and build a strong professional network
This book starts at the very beginning, with why you might want to do a PhD, how you might decide what route to PhD is right for you, and what a successful application might look like.
It then takes you through your PhD journey, year by year, with tips about how to approach and succeed during significant moments, such as attending your first conference, or writing your first academic paper.
Finally, you will discover what other skills you need to develop during your PhD to give you the best route to success after your viva. All of this supported by links to activities on The Girlymicrobiologist blog, to help you with practical exercises in order to apply what you have learned.
I posted last week about some of the reasons that I think social media can be powerful and positive. This week though I want to talk a little bit about the other side of the coin, the fact that social media can end up being a source of enormous pressure to the detriment of both our wellbeing and our career choices.
I’m a great advocate of the use of social media as scientists, I’ve even given the odd talk about it. That doesn’t make me naïve to its risks. We tend to talk about platforms as if they are formed of a cohesive community with the same rules of etiquette and values, but they aren’t. The reasons that people use social media are as variable as the number of people who have accounts. Therefore if you fall into the assumption that the posts you are reading are made using the same motivations and ethics as yours, you can end up in a position where posts and responses to them can cause upset, self recrimination or harm. So what review and thought processes do I try to undertake when I post and engage with posts by others, either emotionally or by responding?
Am I comparing like with like?
I’ve had conversations with a couple of my PhD students over the last month or so about the dangers of benchmarking against people who you don’t really know. You don’t know what their project is, you don’t know what their education and learning objectives are in comparison to yours, you don’t even know if their description of where they are at reflects the reality of what is being shared.
Even for me I can sometimes see posts on social media and when I’m having a bad day can fall into a spiral of asking myself ‘am I good enough?’ ‘do I work hard enough?” ‘do I know enough?’ ‘am I successful enough?’. The thing is that, especially on social media, posts are a projection of self but an edited one. The same thing happens when you have PhD get togethers down the pub but the reach is different and you have at least a better chance to evaluate what’s being said.
It’s easy to fall into comparison but you have to know what your comparing against. For PhDs and training programmes especially, you’ll have your own mile stones and training goals that will be personalised to you and your learning needs. It is folly therefore to compare yourself against someone else as their goals will be different. Discussing shared barriers and approaches can be helpful however but the race to compete about papers, data and presentations rarely is.
Are they only sharing the good stuff?
I personally am really wary of accounts that only share their successes. I know I go on about this a lot, but the most learning often occurs in the failures and if you’re not prepared to share the learning I’m less willing to engage with the success. Nothing is brilliant all the time, no job, no project, and so if an account only shares the hype I am less likely to use it as a benchmark. I’m also less likely to share it with the community, as I worry about the impact that amplifying those voices might have.
In a similar vein, accounts which are not about conversations and supporting the community appeal to me less. If you have an account that is only there to disseminate your success, your papers etc and you don’t also work to amplify others I am less willing to engage. To me, social media is about the opportunity to converse with a diverse group of people. Some accounts are the equivalent of standing on top of a hill with a megaphone and so I take that ethos into account when reading their posts.
Harder, faster, stronger
I see a lot of posts these days talking about how many extra hours someone works, about how many work hats they wear etc. There’s a strong push for this on some academic accounts where people make comments that if you aren’t prepared to work every weekend you can’t be an academic. I also see it more and more coming from some Healthcare Scientists and I’m not sure it’s a healthy trend. There are always times when we have to go the extra mile but wearing it as a badge of honour concerns me. I’m also aware that some of this doesn’t actually reflect the reality, it’s almost like it is what is now expected.
I’m sure that I am guilty of this one, but I hope that most people read my ‘I’m working this weekend’ as ‘my god I’m working again this weekend’. If not you have my apologies. Step up when you have to but also find the strength to have boundaries as it will make you better at all you do.
One last thing on this while I have my rant on. Discussing the ability to do long hours is a privilege, there are many people for whom is this not possible. Parents and carers are excluded from progression if this is what is required. I work hard but I physically suffer badly for it. I don’t want to have my face and hands swell for the rest of my career. I want 8 hours sleep and weekends off if its not an emergency. My mind may be willing but my body is most definitely not. So lets not imply that the only way to be successful is to get 4 hours of sleep a night and to become the job, we all owe ourselves and our families more than that. Rant over!
Whose is the driving seat?
I’m thinking I’m not alone in this one. There are times when I read something and it will send me into a proper shame spiral. Sometimes it’s something as simple as seeing a micro question and not getting the answer right, sometimes it’s seeing an opportunity that I feel like I should engage with and don’t have the energy to and sometimes quite frankly it’s seeing things like a meeting day on my specialist subject that I didn’t know about and makes me question my knowledge/impact. The thing is very few of these reactions are real. They are driven by my anxiety and 9/10 time I will have read exactly the same tweet and not raised an eyebrow. So if it’s about me and not about them what do I do?
Well to be honest I turn off Twitter, step away and have a cup of tea and check my thinking. What is it that has triggered me? Why has it led to that response? In short I make sure that I get back in the driving seat rather than being a passenger to my responses. It’s like those emails you get that you know you shouldn’t respond to right away – I always do and I always regret it, I have impulse control issues. At least on twitter if I step away immediately and don’t engage then I can do the self reflection to try to ensure I’m the best version of myself when I do. We’re all human, we all have moments of jealousy or self doubt, it’s how we respond to those moments that define us. This may be especially true on social media where your responses are out there for the world to see.
Is it helpful? Is it kind?
I definitely share my successes and challenges via both this blog and across social media. My aim in doing so is not to dwell in either but in the hope that sharing will help others, in seeing the opportunities available to them or on feeling less alone. I do have a constant conversation with myself about whether the level at which I share content from myself and other is correct. I know I’m never going to please everyone but I try to at least be honest with myself about my intent when sharing. I saw the tweet below a few weeks ago and it really enforced for me the need to continue with this evaluation. It can never be a response of ‘well I managed it so why haven’t you’. So much of social media strips away nuance and 280 characters will never tell the full story, and so we need to be clever about telling as much of the truth as we can. When people respond in a way that signals that we haven’t managed this it’s important to bear in mind not just what we believe we put out there but also what the reader received when they saw it. I’ve often found the 2 are not the same as they will be looking at it through a different lens to us. Sometimes just acknowledging this is what is needed to make the other person feel heard. I think this is worth remembering as both the maker and receiver of content.
Is seeing believing?
I am super guilty of this one. I’m nothing particularly special and so I fall into the trap of believing that because I did it anyone can do it. I think in terms of intellectual ability this is true as I’m no smarter than anyone else, but I also have a super supportive husband, no kids and research funding. Those things open doors and enable me to have the time to focus on things I want to achieve, whilst feeling supported to do so. This is not the case for everyone and so everyone’s scenario is different.
When you look every year on the day that FRCPath results come out, you see way more people posting that they have passed than those who post they have failed. People hardly ever post to say they failed their PhD viva’s or have come out with an MRes instead. It is worth therefore being wary of using the evidence before your eyes in terms of evaluating how many people actually succeed. I think when I took FRCPath the pass rate was about 40% and for my NIHR Fellowships it has been even less some years, not the 80 – 90% you’d extrapolate from what you see. Making career choices on the basis of this is pretty dangerous. It sounds easy therefore to say you should meet up and speak to people to understand what the reality is. That is sometimes easier than it sounds, not everyone will know someone who has been interviewed for an NIHR Fellowship for instance. We don’t want to limit ourselves and others by saying if you don’t have the connections you can’t strive for the opportunity. What we do need to do is make it easier to see the reality of those options and also make ourselves available for the conversation about what it felt like to attempt it. If we are going to celebrate our successes publicly we should also try to be generous with our time in order to make the same opportunities more widely accessible, with all the context specific information that entails.
You don’t have to take on board all that you hear
That said we’re scientists and healthcare professionals and should be able to look at information available and critically evaluate it. It is easy to get bogged down and not to be able to see the woods for the trees, you’ll get offered so many different opinions and perspectives that it can sometimes be hard to work out whose voice to listen to. Not all of those voices should however have equal value, some you will know more context specific information about than others. When I’m in doubt, when I start to spiral, or when people are critical I tell myself the advice below and then re-evaluate what I’m hearing in light of my relationship and the content of the advice received.
Finally, the other things are more about my own expectation setting. I try to remember why I set up my twitter account and what I was trying to achieve with it. My account is mainly professional, although I also like to share who I am a person, as I think that’s important. It is not my personal account which I maintain on Facebook for checking in on my family and use an occasional safe space to vent. If my Facebook friends have science questions I direct them to Dr Cloutman-Green on twitter because I like to have a safe space elsewhere where I’m not Dr or being reviewed or critiqued. I go back to this when I struggle with dealing with managing my posts or feeling low. I remember the lens through which I am supposed to be viewing the information. I also know that when I’m tired and in a place where my inner critic is running wild, that it is not the time to engage and to take a break, get some sleep and come back when I feel more like myself.
Social media, like most things in life, can be a double edged sword. It has the power to connect and inspire, it also has the potential to isolate and feed our inner demons. Like any adventure it’s therefore worth being prepared and ensuring that you know why you set out and what you want to get out of it. In times of stress know when to walk away and at the end of the day, know that you have friends who can act as a more rounded sounding board if they are not limited to 280 characters, they may even have gin.
I’ve talked previously about benchmarking and the pros and cons of trying to work out if you are doing OK by comparing yourself to others. As scientists we have a tendancy to look for evidence, in the form of numbers, to enable us to do this. In terms of research measures the main ones that I have heard of being used are the h-index (Hirsch index) and the i10-index. These numbers are not just used by us as individuals as marker of impact and progress but they are also used by promotion panels at universities and by external reviews as a marker of quality/excellence. The question is are they measuring the right things? More recently I heard of something completely new (to me), the K-index (Kardashian index) and finding out what it was about kind of blew my mind.
What are these measures?
The h-index is supposed to measure both productivity and impact. It’s calculated by using the number of papers published by an individual that have a minimum number of citations, for instance if you have a h-index score of 4 you have 4 papers that have at least 4 citations. You may have published 20 papers but they only count once they have reached the minimum citation score. The i10-index by comparison is the number of papers with a minimum of 10 citations, and so is a similar but simplified version.
As of August 2021 my scores for these benchmarks (as taken from Google Scholar) are:
I had on the other hand had never heard of the K score or Kardashian index until recently. The K-index is a measure of someone’s scientific productivity in relation to their social media score. It is determined by dividing the number of social media followers someone has on Twitter by the number of citations they have in peer reviewed publications. In my case (as of the 10th August) that would be 4939/703 = K-index of 7.03.
What’s in a number?
But what do any of these numbers actually mean. For the h-index a score of 20 for a scientist of 20 years experience is supposed to mean they are successful, 40 is outstanding and 60 is exceptional. Obviously these vary between disciplines, but as I haven’t reached my 20 years yet I’m OK with my 16. For the i10-index, only really used by Google Scholar, for a similar level of experience an i10-index of 25 is considered to be pretty good. Again, this varies between disciplines. It is also likely to differ between settings, as a Clinical Academic I am unlikely to achieve the same metrics as one of my academic colleagues, as I also hold a clinical role.
“I propose that all scientists calculate their own K-index on an annual basis and include it in their Twitter profile. Not only does this help others decide how much weight they should give to someone’s 140 character wisdom, it can also be an incentive – if your K-index gets above 5, then it’s time to get off Twitter and write those papers”
Hall, N (July 30, 2014). “The Kardashian index: a measure of discrepant social media profile for scientists” (PDF). Genome Biology. 15 (7): 424.
What is it that my K-index means then? Well my K-index is above 5 and therefore apparently means I may have a higher following than my scientific research credentials indicate I deserve. If I had a low K-index (i.e. 1 or 2) it would suggest that perhaps my science was being undervalued. This was actually seen for a quite a few female scientists in this rather tongue in cheek study.
Just call me Khloe
So I am a Kardashian, it’s official! Now if I could also be given their pay packet and I also wouldn’t mind someone who would follow me around doing my hair and nails – although that might be a little weird on ward round.
In all seriousness there have been a number of things that struck me about this as a concept.
The idea that scientists only attract followers in order to share their own science, rather than to share and discuss science or to raise awareness of the profession
That all of these measures try to claim they measure impact but all they do is measure the equivalent of ‘shares’ by scientists to scientists and I would suggest that that isn’t actually a measure of impact – just a measure of how well you are surviving at publish or perish
The lack of perceived benefit from science communication undertaken by scientists in comparison to the requirement to produce new publications. This has been seen in a bias against women in the promotions process as they are usually disproportionately involved in activities such as outreach, which are not perceived to have equivalent value. Only ‘hard’ science counts
What does the existence of this metric tell us (even jokingly) about the relationship between science and science communication?
I am aware that the author of this paper said in 2022 that it was satire and a dig at the use of a metric indicators, but I think it goes deeper than that and sheds light on a much larger set of issues and attitudes.
I have been told my people that I both respect and who are very senior that I should do ‘less of my nonsense and focus on both my science and clinical skills’. The nonsense they were referring to is my education and outreach work, work like the Nosocomial Project. The impact of this work in terms of recruiting future scientists, about the democratisation of science, and impacts on decision making, definitely aren’t captured by the number of citations I have on Google Scholar.
I think these metrics also fail to capture things like translation into clinical practice, inclusion in guidance and use by groups who may not be publishing papers, and therefore are not citing your work, but have applied it to their setting. That is the reason that I publish, to support change, not to chase a h-index, and so these metrics represent only a very traditional view of academic impact.
As for the K-index, as far as I’m concerned my research is funded by the public, the results therefore are owned by that same public and there is an onus on me to share with then what their funding has paid for, discuss with them whether they actually feel it brings benefit and where it can be improved for those with lived experience. I think the time of academics living in an Ivory Tower and only communicating with each other should be over. Yes we need to talk to each other, collaborate and inspire each other, but that shouldn’t be as far as the conversation goes.
There is obviously a difference between being a science communicator and a scientist who communicates science. The JD’s and the skill sets are over lapping but different. That doesn’t mean that scientists shouldn’t be out there talking about science with the wider public. I feel very strongly that sites like twitter shouldn’t be a single sided conversation. I’m not just going to talk about my science, I want to discuss and amplify content produced by others. I want to have, sometimes challenging, discussions in order to show that science isn’t about absolutes.
Communication on social media is about so much more than the sharing of data. It is a way to develop networks, show support and amplify, as well as to communicate information that is real time and may not have gone through the academic peer review process, such as guidelines or funding calls. So maybe instead of putting scientists with a high K-index and low other scores into academic purgatory we should look at developing a different way to evaluate the modern version of what it is to be a scientist. A score that could capture all of the invaluable work a lot of academics do to ensure that there is a workforce of the future and to support scientific literacy and co-production beyond the Ivory Towers in which we live.
Anyway, apparently I’m off to the paper mines to prove my academic worth. I intend to continue to smuggle out tweets whilst the WiFi permits however, because as much as its lovely to talk to scientists and people like me, science is more valuable when it is truly shared and available to everyone.
Many of us spent a glorious evening last weekend watching the Lionesses (England Woman’s Football team) finally ‘bring football home’ by winning the European Championship. If you don’t watch or have no interest in football this is significant as it’s the first Championship win for any English football squad in my lifetime and something that the male side failed to replicate last year. Listening to some of the commentary made me reflect on the power of winning to support change and why outside of sport sometimes winning can make some of us feel so uncomfortable.
I’m going to put this out there. I get called competitive A LOT. If I’m in, I’m all in. Not for the winning but for the being part of the process. For me it’s all about the learning and the growth. I’m not therefore so competitive with other people but I have a tendancy to, perhaps, push myself a little hard. I come from a family of super competitive siblings, my brother cannot stand to lose and my sister was a superwoman, she was going to start a PhD with a newborn afterall. So I suppose I grade on a curve and when compared to them I was always the one who was happy to lose at cards/games. Still, I was raised in an environment where every dinner discussion was basically debate club and so I carry that with me.
Growing up in this environment means that being competitive is a trait in myself that I’m not particularly comfortable with. Frankly I don’t think it’s a very attractive part of my personality. It does mean that I can single mindedly focus on task though, which has advantages for exams etc. It was interesting therefore for me to see the winning of something being talked about as a really positive thing, not just for the winners, but to enable and support change. Change not just in attitudes but in the way things actually work. I’ve always told myself it’s the taking part that counts (and I stand by this) but is winning something that does enables us to achieve change beyond ourselves? If it does, is this something we should think differently about and actively use more if we are fortunate enough to have it happen to us?
Winning can be seen as superficial achievement, but is it?
Winning something, especially on a large scale, has the capacity to change us. I’ve been thinking about the difference that change makes in us that might enable us to then support the wider change we want to see elsewhere.
There are some people who have an innate confidence that they are where they need to be, there are others who are over confident and come off as arrogant. For the vast majority of people I speak to however, we spend a lot of time striving and reaching to feel like we deserve to be where we are and to belong. It struck me whilst I was watching how much these girls are likely to be the same as me. There’s been a lot of ‘well they are only girls’ and ‘when it comes to it they’ll crumble’. When you’ve spent year after year hearing words like that, I’m not sure that winning is superficial. I know that for me having concrete markers of achievement, especially when given by or measured against my peers, really helps me feel like im doing something right and increases my sense of purpose and belonging. We shouldn’t need external reinforcement but when you have worked so hard having that acknowledged by those you benchmark against matters. It can change the way you feel about yourself and quieten some of those inner voices of doubt, at least for a while. That change in ourselves can embolden us to action, to feel more able to make the change for others, to feel worthy enough to enter the fight. So maybe winning isn’t as superficial for some of us than I had previously thought.
Why does visibility matter?
‘You can’t be what you can’t see’ (or become aware of to be less ableist)…….for me one of the amazing bi-products of this game is that I am writing this blog or more widely that people are talking about it. I’m a Aston Villa fan so I am used to supporting teams that win little and I am certainly not the kind of girl who switches her loyalties in order to follow success. I do get however that winning draws people in. There will be a lot of people who have never watched women’s football who watched that game. There will be a lot of people who don’t normally watch football, or maybe sport at all, who watched that game. Those people who aren’t normally reached, who aren’t normally impacted are now part of a conversation that might have happened anyway but with much smaller numbers. Winning may not just have changed the conversation but also changed the reach of that conversation. Girls who may not have thought that sport was a career option for them will now know that it is something that could be on the list. Wider than that though, girls who have heard that they will never be able to compete on the same stage as men in general will now have evidence that is just not true. The change that can be born out of that one moment in history has the capacity to impact beyond sport and that really matters.
Why am I sometimes ashamed of winning?
Worse than being seen as superficial, winning can actually be seen as an act of selfishness. I’m sure that this is true for a lot of men too but growing up in a competitive household it was still not seen as a particularly gracious trait to talk about winning, you won and you moved on to the next thing. I think on a wider level there has always been that thing that good girls are seen and not heard, you don’t rock the boat, talking too much about success is seen as rubbing others nose in if rather than a way to inspire others. This hit home for me as last week when the Lionesses won I was in a bit of a quandary about whether to share my own success. I was lucky enough to be on The Pathologist magazines 2022 Power List. This is really nice but also as there aren’t that many Clinical Scientists on it I wanted to share it so that more people are aware of it, so next year when nominations open we can work to get more of us nominated.
It came up on my LinkedIn and I stared at it for ages trying to decide whether resharing it was an act of indulgent arrogance or not. Then I went on the twitter and I saw the joy with which other were sharing their listings. So I decided the right route was to share and congratulate everyone I saw who was posting as well as my own. That felt right to me as it was about joining in the celebration of others and working together to try and raise awareness of the wonderful scope of our profession and the list itself.
Like all things the why is important
The why, therefore, to me is as important as the winning. Why was I involved to begin with? What were my motivations? Why am I choosing to share or not what the result was? I think one of the things I often challenge myself to do is share as many of those things I fail at as I succeed at. To remind myself that failure is not shameful as it is often where I get my best learning. I have to challenge myself that if failure is not shameful than succeeding should also not be shameful. As long as I’m being equally visible with both then I’m not doing it for the wrong reasons. My reasons for sharing winning and success should never be to stand on a pedestal and go ‘didn’t I do well’ but to stand where I can be seen in order to offer a hand up to others. Sharing success is not an intrinsically selfish act or an act of arrogance that should elicit eye rolling.
The other way that I reflect on whether success is something to be shared is to challenge myself about how I would respond to it if that post was coming from someone else. I love seeing and resharing the success of others on Twitter and other platforms. I get joy from seeing others succeed. If I get to the point where I am not amplifying others, hopefully more than myself, then I would need to really start questioning why I am putting info out into the world. At that point I feel I would have slipped into self congratulation rather than doing it for the right reasons and I hope I would stop and give myself a talking to.
Haters gonna hate
Having said all of the above let’s just get a reality check. Someone is going to hate whatever you do. That’s just the way of the world, especially as you work to raise the visibility of yourselves and others. The Lionesses are already getting grief and are being told that their success is worth less as they are women. In my opinion this is just more reason to celebrate and push for change. I have been told that my success makes others feel uncomfortable and that I’m only a Lead Healthcare Scientist in order to laud my success over others, that I’m all about winning. The thing is that all of that only matters if its true. If it is true then it gives you the opportunity to reflect, to change and grow. If it’s not true then no one else knows your motivations and so they don’t know your why, they therefore can’t really judge the results.
So my thoughts are that winning can be just as important to others as it is for you. Sometimes the winning itself can empower you to make a change happen far more widely than you would have been able to do otherwise, either due to increased visibility or just feeling worthy to have a voice. We will always be judged but that isn’t the reason to not play the game. Just make sure that you take the time to check in with yourself to know that whatever the outcome you’re doing things for the right reason. If you are lucky enough to win, shout about it, celebrate it, just make sure you celebrate others with the same energy and enthusiasm that you use to celebrate yourself. Winner is not a dirty word.
Anyway, I’m off to the Commonwealth Games this weekend to see more amazing individuals push themselves, break records and win. I may reflect a little more as I admire everything they’ve given to get to this point and you can be sure I will be celebrating them, win or lose, with every step they take.
I count myself super fortunate to be able to share with you a guest blog this week from Francis Yongblah, Higher Specialist Scientific Trainee and Laboratory Manager at GOSH. Anyone who reads this blog regularly will know how passionately I feel about being seen for our whole selves and so it is really special to me to share Francis talking about the importance of Pride in enabling individuals to feel seen and accepted. I hope by sharing this to celebrate Pride month it will help share his important message even further.
“2-4-6-8 – science doesn’t discriminate, 4-3-2-1 – Science is for everyone” – 13 years later, finally getting to be the true me.
A bit about me before…….
I had come out as gay when I was 20 years old at university when I was studying Biomedical Science. I had only at that point come out to my friends. I was terrified to come out to my family, particular coming from an Asian culture and background where being gay was not a common thing. After graduating from university I had got my first job as a trainee Biomedical Scientist.
A few months into my new role I was quite friendly with my colleagues. We all went to lunch one day, and I remember being asked “so do you have a girlfriend” I had responded “no”. The next question was “what’s your type”. At this point I felt my insides turn out as I felt so nervous and anxious to say that I was gay. I was so worried I would be judged and people would not treat me the same as before. Eventually I was able to speak and mutter the words “well I’m gay and interested in guys” at this point my colleagues said “cool, what kind of guys do you like” I felt so at ease and it was so nice to feel that I could be me. Not all experiences I have had in the work place have always been so positive. Although some of my colleagues knew about me, not everyone else did.
A few weeks later, I remember being in the lab when I heard one of the MLA’s talking with another colleague about someone in another department. She had said “hey….I did not realise that guy was a pufta” I started shaking in anger but also in fear as I didn’t want to be judged or labelled in my work place. We spend most of our lives at work and I want to feel safe and comfortable and most of all, be able to be me. I was still young and decided I’m not going to say anything. Reflecting back I regret that decision and wish now I had gone over and said something.
Another negative memory that will always be with me was when I was at a retirement meal for a colleague. Drinks were flowing and everyone was in good spirits. Everyone was free and had taken their work hats off to be themselves. It was near the end of the meal that a colleague had come over to me, put their hand on my shoulder and said “In future, you might not want to laugh like a little girl”. At first I was in complete shock about this, what were they trying to say? Don’t be me? Don’t be gay? That incident really shook me up and made me always feel that I had to have two separate hats. My work hat and my personal hat.
When I was at work I would never disclose anything to my colleagues about my personal life unless I was particularly close with people.
One question that gets asked is “Do we need Pride?” my response…..YES!
The examples I’ve given show that there needs to be support for the LGBTQ+ community so that people can be themselves.
10 years later……We grow!
Getting older you definitely learn and become wiser. I feel that reflecting back on myself I have become more confident and the experiences I have had have not only shaped my character but also given me perspective and allowed me to have that emotional intelligence that is required to understand people and be able to share the same perspective. I’ve since got involve in promoting equality by attending London Pride. I was so proud when my hospital organisation marched for the first time. I felt proud and felt I could be me. It was at this point I was thinking about my professional body “The Institute of Biomedical Science” and getting them to march. I got in contact with the Communications team who thought that this was a great idea and were so supportive. I worked hard to get the application in and low and behold we were successful and obtained a place in the Pride in London march 2021. Unfortunately this was cancelled due to COVID but we were then given the opportunity to march in July 2022.
The build up to this was exciting and heart warming. The IBMS team worked hard to help support the event by coming up with lab coats that we could wear, stickers and little fuzz bugs that we could hand out to the crowd.
It’s time for the healthcare scientists to March!
I was so excited to be marching. My fellow scientists all got ready, dawning on our white lab coats with a rainbow coloured IBMS logo. Everyone looked amazing. We all got ready to march. I remember feeling so anxious at this point. Once we had started to march the adrenaline was going and I started to feel so excited. Seeing the crowd cheer and yell. At this point I felt the need to lead the group and so took to the front of the march.
We were all working to try and come up with a phrase to yell as we marched and then our amazing IBMS communication lead – Matt, came up with the phrase
“2-4-6-8 Science doesn’t discriminate. 4-3-2-1, Science Is for everyone”
I was yelling this at the top of my lungs as it was so loud with the crowd cheering. Our amazing group echoed this. We also yelled “NHS, NHS” and “IBMS, IBMS”
Everyone participated and really integrated with the crowd. Handing out fuzzy bugs and stickers. The irony is that I was at a Pride event and I felt such pride and proud of having my profession represent myself and many other LGBTQ+ individuals and show that within our profession Equality, Diversity and Inclusion is key and that everyone needs to be represented and be proud of who they are. That they are able to be themselves in their workplace.
For the first time in my career as a Scientist, I felt that I was myself and able to be proud to say that I am a Gay healthcare scientist and I am proud of who I am. That my personal characteristics should not hold me back from reaching my full potential. This event will mean more to me as a scientist than anyone would ever know and as we got to the end of the march, I started to well up and cry. I felt amazing but for the first time ever, I really felt that I was me. As I said before, we spend most of our lives at work. I feel I’ve broken that barrier of having to be 2 separate people, the Scientist and the Gay Asian guy to now just being me. I hope that this is just the start of things to come. What has been most inspiring is to see how other IBMS branches and regions have now joined in and organising marches too. I look forward to seeing the pictures from their events and it’s such a good feeling to know that nationally, diversity, equality and inclusion is becoming a key part of being a healthcare scientist.
I previously wrote a blog post called 50 Shades of Grey where I spoke about why I believe we need to do a better job of articulating the fact that a) Infection Prevention and Control is basically 80% risk assessment and b) risk assessments therefore look different in different settings as patients and scenarios differ.
Following on from this post I recorded a podcast with Martin Kiernan as part of the Infection Control Matters series where he reminded me that I said in that original post that I would write a follow up with more details about the components of risk assessment and the different ways you can capture your thinking around them. So continuing what appears to have turned into a bit of a risk assessment themed July here are some of my thoughts about the different ways you can go about developing your own risk assessment framework.
Firstly a disclaimer. The following are things that I have found useful for how my brain works. I hope that others might find it useful but if you do not I apologise, maybe you could share what works for you instead? Then we could have a collective resource around this.
What is risk assessment?
The basics of risk assessment are to understand what risks are present and to put measures in place to decrease those risks. Sounds simple right? The problem is that we throw around the words risk assessment as if we all have the same understanding of what the words really mean, in reality as that concept is applied in different settings or by different professions it can have very different meanings.
a systematic process of evaluating the potential risks that may be involved in a projected activity or undertaking
If you talk about requiring a risk assessment to someone working in engineering or Health and Safety you will get a very different piece of documentation to that I would expect in IPC. Now some of that is to do with the amount of information that needs to be processed in order to come to a conclusion and some of that is about how we convey information. The aim of an engineering or Health and Safety based risk assessment is to give a risk level and matched control measures. The aim of an IPC risk assessment is to support complex decision making. In IPC a risk assessment is more like a framework for ensuring you have taken into account multiple factors in order to support informed action. They are not a one and done process, they are dynamic and can change rapidly as more information is added to the framework. Patients for instance can become more or less infectious, more or less mobile, require more or less intense interventions and outbreaks have information that changes as they develop or come under control.
The use of a framework is nothing new, a lot of medicine and healthcare is based on algorithms we develop during training. The thing is that these are often integrated into our thinking as cognitive processes via experiential learning and we don’t often talk about them. There are two issues with this, one is if we can find a way to visualise or share how we go through our risk assessment framework it can prove helpful to others as they can have access to it without having to fully develop their own. The second thing is that, like anything developed through experiential learning, our frameworks may have intrinsic bias or weaknesses based on the scenarios used to develop it. I am much more likely to dive down a scientific vs ward practice approach for instance. By being able to share our frameworks we can therefore have better conversations with colleagues to both share our thinking and if needed modify our frameworks for future use. The framework itself isn’t static and should continue to develop as we see more, learn more, after all microbes aren’t static and healthcare is ever changing.
What is different between health and safety and IPC risk assessment?
Below is a matrix that I think most of us will be very familiar with and is commonly used in Health and Safety risk assessment. They are based on identifying how likely a risk is likely to be and the impact that risk would have if the incident occured. The thing is that for IPC risk assessments this misses a whole third axis, what are the implications of the intervention on other aspects of that patients care? What are the consequences of controlling this risk for the patient? When we are managing IPC risk we are not always talking about risk from an inanimate object we are often talking about humans that can experience negative impacts from risk interventions. There is for instance data on the impacts of isolation on patient care and also the impacts on staff from cohorting and other measures. I’m not suggesting we therefore don’t need to control risk in IPC, just that a 2 axis table may not be able to capture the complexity of the decision making associated with that risk.
The other difference is the dynamic nature of IPC risk assessments. Although Health and Safety risk assessment should be revisited and reviewed, they are for the most part fairly static. IPC risk assessments can change every time we received new information, results become available, patients become better or worse. Finally, risks in IPC are cumulative, and so the impact of the risk may be low during a 15 minute outpatient appointment but much more significant during a 7 night inpatient stay. All of which mean that a framework that can manage these changes will probably look different to the matrix we are used to seeing.
What are the components of IPC risk assessment?
Below I’ve included some of the key components that I use in my risk assessments and decision making. Overlaid on top of these specifics are always:
Length of exposure
Level of exposure
Susceptibility
Clinical consequences
These always need for each scenario to be looked at bi-directionally i.e. what is the risk from the patient or other patients, what is the risk from the organism to the patient themselves. Even if you’re looking at things like infrastructure or staff the same thing applies. What is my risk of contaminating the sinks with this patients’ Pseudomonas aeruginosa? What would that mean for other patients, visitors and staff? It’s also important to know where or what you are getting your information from? How does that information/data collection method impact the true extent of the information you have? For instance if you are only doing responsive screening you may miss out on asymptomatic carriage vs the information you may have using universal screening. Developing a framework that captures key information is essential but it also needs to be done is a way that acknowledges any knowledge deficits in what is being captured. These are important for the ‘assessment’ bit of risk assessment and impact final decision making. Knowing what you do not know is a large part of the process.
How do we develop a framework that will help us?
Some of the below is taken/modified from a session I gave on risk assessment at the 2021 Paediatric IPC course from the GOSH Learning Academy (shameless plug for the 22/23 sessions below) but the principles apply even if you are not looking at this from a paediatric perspective. Again these are just methods that work for my brain so you may have different formats that work for you.
I think the formats that I find useful to help both the process and to visualise for different audience fall into three main categories:
tabular
question based
flow chart or algorithm based
Each one has pros and cons depending on the amount and variability of the information you are trying to collect and the number of decisions that are open to you based on each piece of data.
Tabular recording
Tabular recording works well if you have electronic systems to record the input data and the decision making based on those actions are clearly defined. A good example of this type of risk assessment framework might be reviewing results for a new MRSA outside of an outbreak setting, and it is very similar to the way that data is collected on the HCAI reporting portal. The benefits of this kind of system is that it is very defined (each field can have definitions linked to it) and therefore it is a good way to ensure the capturing of a minimum data set, as you can require all fields have a response. It is also a good check list for those completing so that items don’t get forgotten. It also permits really good data analysis, you can run reports to see if, for example, everyone with a C. difficile diagnosis had a box ticked to indicate the ward was called and advised to start chlorine cleaning. You can then also run a report against the cleaning order to see that not only the advice was given but whether it was acted on. As a scientist I like this as it removes variability in response, however that inflexibility also reduces it’s usefulness in non standard situations, especially in outbreak scenarios where there may be a large number of possible actions. You can always add in open text fields to record that kind of open data but you then also lose some of the benefits of using this system as you then can’t analyse the inputs easily and you lose the consistency of recording. I recommend this kind of risk assessment framework for complex but standard tasks, where a lot of information needs to be gathered but the number of resulting actions can be captured in a defined list.
Question based
Question based frameworks are (I think) the one that most people working in IPC are most familiar with. You take a call and you work through a mental checklist of information gathering, decision making, and action taking. Even this common tool is often not recorded as a framework that is written down however. When I learnt I did so by listening to calls others took and then having experienced staff listening into mine, pointing out questions I may have missed and therefore data I had not captured. I think even in this scenario it is helpful to have a list of key questions (and sub questions) as prompts or at least a list of framework points to make sure you are capturing key items that would impact your decision making.
There are benefits to this approach, because it is a free framework it enables the capturing of unexpected or non standard information and further exploration of key points. This level of flexibility however does mean that it is possible to go down an information rabbit hole and miss the collection of key information that could have changed the decision outcome. It is especially useful for scenarios where there are lots of possible decision outcomes, such as in outbreak meetings. It also has a downside in terms of the requirement for conscious recording of all data components, which can be time consuming or fail to truly reflect the situation. The free nature of the information gathering can also lead to a lack of consistency between individuals and increase the experiential bias of how scenarios are managed. I would suggest that although this is the most frequently utilised approach it could be improved by having a question frame work recorded so that at least there is a structure, both for data collection and for recording decisions made on the basis of that information.
Flow chart/algorithm based
The main final risk assessment framework is probably the one most of us have become most familiar with following and producing during the pandemic. That is the use of flow charts or visual algorithms. Although in many ways these are the most intuitive for most people to follow they are actually pretty difficult to do well, I know we are up to versions 14+ on some of ours, a lot of those are changes because of guidance, but some are for clarity as it always amazes me how people can read the same info in different ways. This clarity can be especially challenging using this kind of framework as you have to minimise words to make it readable, which can lead boxes open to interpretation and you have no space to include definitions or other wordy items that would support their use.
The advantage of this sort of framework is that it often clearer to describe a process like this than to do so in words, where you would use many 1000s to cover what is shown in a 1 sided sheet of A4. That said this approach is only good for fairly straight forward processes with highly limited variability. The example below comes from a PHE document and despite how much I appreciate the effort that went into creating it, it is clear how easy it is to produce something that is quite hard to follow as soon as the data becomes complex or too many options are available. I would therefore tend to only use this kind of approach with a fairly linear risk assessment that needs to be circulated widely and does not have a high level of decision recording linked to it.
I thought I would mention here the final version of a risk assessment that I use regularly and that is a discussion based assessment. This tends to come after one of the three frameworks I’ve mentioned above and has a whole complexity in itself, both in terms of the decision making but also the recording process. I think I will cover this more separately as it is a slightly different thing but I thought I would just include the below info graphic. If you are going to go through a discussion based risk assessment process (which I think is important, dependent on complexity, to deal with some of the bias and potential for missed info) it is important to pre determine how those discussions are going to lead to decisions and how those decisions will be recorded. It is endlessly interesting to me that different professions will go into meetings with very different ideas about how decisions are reached and so, especially in an MDT setting, there should be clarity ahead of meeting in order to ensure a fair and equitable process.
How can we share our risk assessments with others to aid understanding?
We are re-entering a period of ‘normal’ healthcare where instead of us using a command and control approach, where algorithms for risk are determined centrally and based on test and response, individuals are being expected to return to individual risk assessment for patient care. This is fine but there are now a number of members of staff who haven’t experienced this form of risk assessment enough to have the experiential component, even those members of staff who have pre pandemic experience may now lack confidence due to the fear of consequences in this new world where many of the components of the risk assessment have changed. I’m hoping that by sharing some of my thinking on this we will be able to come together and share some of the frameworks that we use to make risk assessments to support learning, build confidence, identify bias and work towards improvement in all that we do.
Here are the links to the other posts I’ve done on risk assessment including the post the podcast above refers to, one on paediatric risks and one on environmental IPC.
To round off the posts about different opportunities for Healthcare Scientists outside of the laboratory/clinic this week for National Pathology Week I wanted to end by discussing opportunities for Healthcare Scientists as leaders. Now leadership is obviously possible at all levels and there are lots of different options, but as I accepted my Trust Lead Healthcare Scientist position 5 years ago this week I thought I would focus on that.
What is a ‘Lead’ Healthcare Scientist?
To continue the theme of this week, from my experience no two Trust Lead Healthcare Scientist jobs are the same. I share my post with the wonderful Dr Stuart Adams, and even our experience of the post is different because we lead on different things.
The main theme that I have been able to discern across Trusts is that the role of the Trust Lead Healthcare Scientist is to provide professional leadership for the Healthcare Science (HCS) workforce across specialism boundaries and to provide representation for the workforce either at, or to exec level, in order to ensure the integration of healthcare science provision across patient pathways.
In the role we have at GOSH there are three main areas of responsibility we share for the Healthcare Science workforce:
Research
Workforce development
Education
We report to the medical director and have a committee called the Healthcare Science Education Working Group which we work collaboratively with in order to try to get representation from across healthcare science involved and engaged in decision making. We also work really closely with the GOSH Learning Academy or GLA, which is probably why in all honesty I feel like we are making more headway currently with workforce and education.
The long term aspiration has always been to make these roles analogous to a Chief Nurse or Medical Director position but for now, just having a seat at the table is key.
How it started
These roles have come into different Trusts at different points and there are still a number of Trusts who do not have HCS representation at or to board level. My first awareness of this role even being a possibility was due our education lead in 2015, who I’d been working with on other things as part of my PGCert. She emailed me to see if I would be interested in working with others to set up a HCS group in order to have a cross Trust forum. This idea was a revelation to me. I’d worked at GOSH for more than 10 years and had met HCS from outside pathology on leadership courses and as part of trying to organise Reach Out for Healthcare Science, but we had never had a forum where we could regularly meet as a group, get to know each better and establish links, as well as identify shared barriers and opportunities. It was as part of this work that the Healthcare Science Education Working Group (HSEWG) was established.
Prior to the establishing of this group I also had no idea about the strategic set up of HCS outside of GOSH. Alex Milsom and Ruth Thomsen came to present to this new group about both Trust Lead HCS and the work being done of the CSO office and NHS England, suddenly my world increase in size. The HSEWG started to work towards creating a Trust Lead HCS post. As we had no funding we were hoping that we could at least get a named post that had recognition by the board and a defined remit. At this point however I had no intention of applying for such a post myself, there were so many others who were more qualified, better experienced and better placed.
Not long afterwards a letter went out from Chief Scientific Officer Sue Hill to all Trust CEO’s and in 2016s Lead HCS jobs started to be advertised (see above). Many of the posts, like ours being prepared, were unfunded. At the same time as these were being developed we got a new energised and inspiring Head of Education (Lynn Shields) who in her interview from the outset was determined to represent all professional groups. She found £15000 a year in development funds for HCS and from that created a 1 day a week band 8B Trust Lead HCS post. Thus the GOSH Lead HCS post finally became a reality in 2017. By this time I was about to start my NIHR Clinical Lectureship and had become so engaged and excited by the possibilities of what the HCS workforce could achieve that when it was advertised I ignored my fears and went for it. The complication was that I was also about to go on sabbatical for 2 months to Boston Children’s Hospital and so it was proposed that the post was split into 2 0.1 WTE roles. This was the best thing that could have happened, my co-lead and I have very different skills sets and I love not having to do what can be a challenging role in isolation.
Where we’re headed
The one thing I’ve learnt in this post is that nothing can be achieved well in isolation. The job is in itself all about collaboration and involves working both with GOSH and across the system to drive change and improvement. It took me a some time to really grasp the difference between an operational (doing role) and a strategic role. Lead HCS in my experience is definitely strategic, it’s about working out the vision for where you want to get to and a rough road map, but really working with others to actually achieve it. I think we (the HSEWG) have a good idea of where we as a team would like to get to, but in a world where we have clinical and other commitments delivery can be a little more challenging.
The vision that we have can’t exist in isolation however. There is amazing HCS leadership at regional level. I’m fortunate enough to have continued to work with Ruth Thomsen as our regional lead for London. She has taught me so much, listened to my woes and is a constant source of inspiration. I can’t advise enough finding out who your local leads are and building relationships with them. The ones I know are all both top notch scientists and top notch people. Even if you are not in a leadership position yet they can help orientate you to the world of HCS outside your Trust and if you’re lucky mentor you to help you achieve your potential.
Not only are there regional HCS networks but there are also national ones. Obviously most of us are aware of things linked to our specialisms but it’s definitely worth linking into the national work being done by the Chief Scientific Officer and her team, they even have a twitter account to make it easy. There are regular webinars and an annual conference that can be a great way to find out what is happening national at a strategic level and how it’s likely to impact you and your Trust. Current important themes like the implementation of ICS boards as well as HEE joining NHS England will filter down and impact us all. By being aware of this we can make sure we are part of the conversation rather than an after thought.
NB. Talking about orientation outside of your Trust now is also the time to find out a little more about Integrated Care Systems (ICS) as these come into play from the 1st July and will really impact on how we deliver services, what our training funding and support potentially looks like and where some of decision making occurs.
Why is it important to have these roles?
That brings me onto not only why I enjoy the role but also why I think it’s key that HCS at other Trusts see if they can bring in equivalent posts. This isn’t because I believe that I am in any way amazing, in fact there is lots that I wish I could do better and so much more I wish that I could achieve. That said, even if I struggle to get us where I want to during my time in post, I have managed to get a seat at the table. A lot of the time I get to be in the room when items are discussed and I can say ‘have you thought about how this will impact the Healthcare Scientists?’. This is especially true with new patient pathways or with new builds. Have they thought about the fact that opening X number of new beds will lead to X number of new samples, and so they can’t just increase the establishment on the ward but also need to increase numbers in diagnostics. There are also times when I can provide a solution that no one else in the room may have conceptualised, linking to triage or changes in flow, because I can suggest a rapid test or a modification. As Shirley Chisholm said ‘If they don’t give you a seat at the table bring a folding chair’. Once you get into the room, a chair will follow.
It’s also about visible leadership, this week we’ve talk a lot about different roles but if we are not out there and visible, both to our own profession and others, we limit both our own trajectories and our wider impact. Leadership roles are really common in nursing and medical disciplines and increasingly common for Allied Healthcare Professionals (AHP), but we will never have the same input unless we are seen and active in breaking down silos and fostering collaboration. I hope that by being seen and by being open about the benefits and challenges of these roles that others will feel inspired to see this as a route they would want to follow.
I have one more possibly contentious point that I’m going to mention here because it’s something that I really believe in, although others are free to disagree. I think using the collective name of Healthcare Scientists is key for us to have a voice in a lot of these conversations. I am a proud Clinical Scientist, I’m proud of the work I did to get my state registration and to get on the HSS register as a Consultant Clinical Scientist. However I switch the title I use based on the audience I’m speaking with and who I’m representing in that conversation. Using the term Healthcare Scientist helps as many senior people within the Trust don’t know the difference between a Biomedical vs Clinical Scientist. This is of course something that we can address over time but is often not necessary for the messaging we are trying to do. Registration titles are, currently, still also quite pathology linked, whilst using Healthcare Scientist can span so many other disciplines across the Trust. Registration titles also mean that we exclude our unregistered workforce from being included in these conversations or under the umbrella of the discussion. Using specific registration titles can therefore introduce unnecessary barriers to communicating key messages in the moment.
Numbers and representation matter. At GOSH HCS represent over 13% of the workforce and we have the numbers to get listened to if we discuss HCS using those numbers as a whole. If I start splitting us into smaller groups I lose impact, when someone says ‘how many people will be disadvantaged by that?’ me replying ‘4 ophthalmic visual scientists’ isn’t the same as ‘over 700 Healthcare Scientists’. At a national level it’s even more challenging as we are only about 5% of the workforce and are advocating and challenging for the same pots of funding or prioritisation as much larger groups. Yes we have have impact across pathways, but numbers do count. It is much easier for me to say we need to have a Healthcare Scientist on this group than to say we need to have a bioinformatician and a BMS and a Clinical Scientist, and a physiological scientist etc……..suddenly we are asking for 5 seats when we are more likely to succeed when we act together and ask for one and then show what we do with it. So I’m a Consultant Clinical Scientist working in Infection Prevention and Control but I am also a Trust Lead Healthcare Scientist representing all of the Healthcare Scientists within my Trust.
The potential of our work force to create and support change is immense, but to do that we need to be in the room and part of the conversation. Leadership matters, representation matters, being seen matters, so lets advocate for ourselves, get into the room and change the world!
Continuing the Girlymicro theme of raising awareness of roles outside the laboratory to Celebrate National Pathology Week 2022 today we have the inspiring Anthony De Souza sharing his journey from bench scientist to Practice Educator. I’ve already written about why I think it’s so important that Healthcare Scientists think of themselves as educators (see blog here) but Ant puts this into practice and talks about how he became a Practice Educator and why these roles are so important.
I was a geeky kid and was pretty obsessed with astronomy, pathology and nature. I was an avid reader and loved to immerse myself in my mother’s nursing textbooks! I mean, I used to peruse the BNF for fun and at church book sales I wanted medical textbooks.
In my teens I pondered whether to become a marine biologist, a science teacher, a dietician or scientist. After looking through four heaving A4 binders of job descriptions in our school careers corner I settled on Biomedical Scientist, more specifically in Microbiology.
It was a career that allowed me to immerse myself in the medical world without being too close to the patient, something which I thought I may struggle with. My first taste of Microbiology at A-Level was a lesson on bacterial culture which involved bacterial streaking. From this point microbiology sparked an interest that I knew would always be there. After completing my IBMS accredited degree I was very lucky to get a trainee band 5 position in my local micro lab closer to home!
As time went on, I developed within Microbiology spanning a ten-year period. I realised that some of the most enjoyable parts of my role were when I taught or trained others, especially if they shared the same excitement I did. In every job I had I always ended up being known as a good teacher, and knew I wanted to get more involved, but being a teacher full time didn’t appeal to me.
As an experienced band six I started to feel frustrated, felt like I had peaked within my current role and needed something to fundamentally change. It was at this point that I seriously considered leaving the NHS and using my transferable skills in a different place. I’ve always felt confident in my abilities to work in different settings and environments with different people, I just needed the opportunity. That’s when I was encouraged to apply for a job as a part time practice educator in our hospital. Up until this point, I had only ever heard of this role in a nursing context.
‘Most things feel impossible till it’s done’ – Nelson Mandela
During the application for this part time role, I had full on imposter syndrome and was talking myself out of applying. One of the biggest self-imposed barriers was feeling like I was leaving behind certainty and proven experience for a role in which I would need to build and grow within. I had gotten to the point where work felt comfortable, my knowledge and skills were developed for my role, and I felt confident in that. The thought of moving to an area outside of my core experience base was pretty terrifying but I knew I had to do it! I decided to apply and was successful in the interview!
Some of the key purposes of the role are outlined below:
Work to support learning and education and support specific workstreams, in my case this was Healthcare Science.
Create and maintain positive learning environments
Facilitating induction, education and continuing professional development
Encourage practice development, support service improvement
Promote high standards of care and act as a role model for others
Work multi-professionally, as needed
After being used to working in a small team within the lab my new role involved an even bigger and more diverse team. This exposed me to a greater appreciation for the work of other health professionals and the hospital as a whole.
At first, I found the job challenging; learning new names, getting to know the team, my place within it, learning new acronyms during meetings and adjusting to the different styles of communication. Some of my work involved supporting healthcare science learners, acting as a point of contact to raise issues, signposting relevant training & education and supporting outreach and engagement activities. As my role grew and developed, I was able to work more multi-professionally, increasing the visibility of our hidden workforce and even teaching nurses about healthcare science.
As a practice educator a PG Cert in Practice Education is essential to learn about educational theories and how this relates to designing learning for the learner. Whilst I may have been acting on natural instinct before gaining this qualification, the education and evidence-based practice approach to back up teaching has been important in the role.
This role could suit a range of individuals but ultimately this would suit someone who wants to make a difference, is passionate about education and training, has the ability to communicate well, work effectively with others and enjoys working both alone and with different teams. The job often involves taking yourself out of your comfort zone and identifying opportunities to share and develop learning.
Whilst I have now left the lab and am working full time as a practice educator, I still do look back fondly on my lab days and Microbiology. I love checking in on the lab and looking at exciting agar plates and learning about exciting cases, and who knows maybe one day I’ll go back for now though I am fully committed to this new direction. Just because I’ve left the lab, doesn’t mean its left me….
We are working through an exciting time within NHS careers, especially as Healthcare Scientists. Training pathways are becoming more formalised and alongside this diversity of opportunities are increasing, allowing Healthcare Scientists to have not only more options for their individual careers but also to increase the impact of this workforce across areas including academia, education, leadership, as well as clinical specialisms. Following on from this weeks Guest Blog by Dr Claire Walker discussing the transition from lab to lectern and life working as a Healthcare Scientist within the academic setting I thought I would write something on what it is like to be a Clinical Academic (CA), working with a foot in both camps.
So what is a clinical academic? I suspect that all of you who read this blog regularly will be able to picture my face when I googled and the top entry is the one below from the NHS Healthcare Careers webpage:
I believe it’s pretty self evident that I am not a medical doctor and that although this description may once have been true it is far from telling the full story.
Being a CA is not in fact based on profession, or even % time splits. It’s based on the role that is occupied. One of the big distinguishing features is that a CA holds roles both within a University and within a Healthcare organisation, usually one honorary position and another substantive. Throughout the lifetime of a CA career the substantive post may switch between being within healthcare or a University, its the maintenance of both that is probably the most CA universal theme.
The amount of lecturing vs research varies by individual. Most of the CAs I work with tend to be highly engaged with research, especially if they are mainly based in healthcare, as this provides them with funding to buy out their time. In roles where clinics are routine however this provides a buy out route in the other direction. Despite being more research than teaching focussed I still teach on a number of master and undergraduate courses, as well as speaking at conferences etc.
On the Healthcare Scientist career chart below there is a box for CA pathways, but to me it still feels a bit ‘to be developed’. This isn’t unique to Healthcare Science but provides particular issues for my colleagues in specialist laboratories, especially within the UKHSA as they don’t have such a clear progression route laid out for them. It currently doesn’t really capture the whole situation as many of us in the Consultant Clinical Scientist box will also hold CA responsibilities and so the pathways aren’t as split as they appear.
There are a variety of roles into CA careers, both formal and informal. There is a fairly specific skill set you need to develop:
PhD (usually a research PhD rather than a tought/professional doctorate)
Some form of teaching qualification (as determined by your university). Not required for existing post but usually required for new
Funding track record – as you need to demonstrate to your employer you can assure an income stream
Publication track record – needed both for funding and dissemination
These days an interest in public engagement/involvement doesn’t hurt
The most established formal route into a CA career is via the National Institute of Health Research (NIHR) and the Integrated Clinical Academic (ICA) programme.
This is a programme that provides skill development and funding support all the way through from taster sessions to funding support for you to run your own research group. I wrote an article about this route in 2016 for the ACB and not much has changed in terms of the benefits.
The NIHR schemes are great, they match your current salary and give both great training and consumables support. This does mean these schemes are highly competitive (20 – 40% success rate, depending on level) however these days you need a level of research track record (publications and funding) to even enter at Doctoral level – demonstrating a pre-existing commitment to a CA career.
What about the informal routes? As I said the skill sets required are pretty standard and so can be developed piecemeal rather than through a structured programme. It is possible to get funding to do both a PhD and a teaching qualification by going through other routes (I have a post linked to PhD funding coming). The other components, funding and publishing, you will get by applying for funding for the qualification based aspects and during your PhD, it just may take longer. That said the NIHR route is time consuming and far from guaranteed, so both routes require you to know why you want to become a CA and an understanding of the fact that getting there is not a 9 – 5 commitment.
Why do Clinical Academic careers matter?
So having said that it can be a challenging route to go down why should you put in the effort?
There are numerous reasons why CAs are essential in healthcare. Let’s start with individual patient benefits. Research, especially translational research, is key to providing the best possible patient care. If we want to provide cutting edge care then we need to be engaged in the research that is developing that care – from clinical trials to diagnostic development. Getting results that diagnose patients faster has great individual benefits for patients, as they get on the right treatment more rapidly. Being engaged with clinical trials means that patients may be offered treatment or management that would just not be open to them otherwise.
On a Trust scale research enables funding to support infrastructure or translation of new diagnostics/services that might just not be possible with normal budget constraints. I was recently the co-applicant on a grant which brought in over £500,000.00 of infrastructure funding, for both staff and equipment. This means that the initial financial burden of translating over something new is not placed on the NHS and the data to then support business cases for introduction can be collected with minimal financial impact. On a national scale this kind of funding also supports multi site projects which would be difficult to manage in any other way in order to support large scale changes within the healthcare system, meaning that the potential impact can be huge and provide wide scale change.
There are also so many benefits for you as an individual. My career and life changed the day I got my NIHR Doctoral Fellowship. It opened both my eyes and doors to paths that I could never have imagined. I wouldn’t be a Lead Healthcare Scientist now if it wasn’t for the NIHR. I’m not sure I would be a Consultant. I have travelled the world, given lectures to thousands of people, developed future CAs and been able to develop as a scientist and a leader thanks to the funding that was provided. Along the way I hope that I’ve also made a difference for patients both through being involved in national guidance and local change.
What does a day in the life of a clinical academic look like?
As with so many aspects of Healthcare Science no two CAs seems to be the same. The National School of Healthcare Science have a number of different profiles on their webpage which describe some of the different options.
For me my weeks are really varied, obviously for the last 2 years my clinical work has been a priority and so the academic side of my role has been less prominent. I’ve already talked about teaching but for instance this is what I will be doing this month:
Organising a specialist conference on Environmental Infection Prevention and Control
Reviewing papers for numerous journals
Reviewing a grant
Reviewing abstract submissions for a conference
Meeting with my PhD students
Editing a paper for submission
Meeting to review SOPs for a country wide clinical trial
Meeting to review data for an ongoing COVID-19 study
Meeting with the molecular team to talk about how we move our Gram negative typing forward
Carrying out an MSc viva
Attending 2 exam boards as an external examiner
As my clinical work is currently still pretty hard core a lot of this I’ll pick up for the moment in my own time. Also, none of it takes me as long as when I first started out and so it looks more overwhelming than it actually is – I hope you can see the variety however.
Photo credit – Rabit Hole Photography
There is no getting around the fact that being a CA is not a 9 – 5 post however, managing grant and other deadlines on top of clinical work often requires some significant juggling skills, and in my case a very supportive husband. It’s not something I would advise that people strive for if they don’t love research, if they don’t have so many ideas that they just need to do something with them, it is not a tick box career. You also have to grow to be comfortable with failure, only ~20% of grants are successful, paper reviewer comments can be harsh and your confidence will take repeated knocks. Every time this happens though I get better at what I do, I find the learning and try to make sure I do it better next time #lifeislearning.
Despite it’s challenges being a CA brings me untold joy, it provides me with an outlet for creative thought and means that even though I spend most of my days in an office not a lab, I still feel like a scientist. I get to collaborate with the most amazing people who are at the forefront of their fields to make improvements for patients that would either not be possible or would take years any other way. For me it’s been something that has more than repaid my investment in time, energy and creativity. It’s taken me to places I would never have imagined, introduced me to people that my life is better for having met and provided me with experiences that I didn’t think would ever happen to someone as normal as me. So if you love learning new things, making life better for patients and are happy to spend your weekends in front of a laptop then a Clinical Academic career may be the career for you!
To help us celebrate National Pathology Week the ever inspiring Dr Claire Walker has written a blog post to follow on from the talk she gave at HCSEd22 (videos to follow on YouTube). Healthcare Scientists work across the NHS and increasingly within academia, and so it’s important that we acknowledge the wide variety of roles that are open to us.
Dr Walker is a paid up member of the Dream Team since 2013, token immunologist and occasional defector from the Immunology Mafia. Registered Clinical Scientist in Immunology with a background in genetics (PhD), microbiology and immunology (MSc), biological sciences (mBiolSci), education (PgCert) and indecisiveness (everything else). Now a Senior Lecturer in Immunology at University of Lincoln.
The Clinical Academic Path – From the Lab to the Lectern
What can we learn from clinical academic scientists during a conference about co-production? Turns out, given a platform to shout loudly enough, rather a lot.
Minding the Gap
What steps did I take to move from the clinical laboratory to an academic position? Well, I did what any clinical scientist worth their salt who’s been through the transition from CPA to UKAS would do, I performed a gap analysis. Yes, I really am that person. I looked at job adverts for senior clinical scientists and senior lecturers looking for key similarities and points of difference. To my delight I found that we had far more in common than that which divides us. Yes, there are a few key extras like the commitment to completing a teaching qualification and learning exciting new quality systems but where better to learn a new skill than a university filled with professional educators? The similarities in the roles didn’t genuinely surprise me but it did confirm what I had hoped to be true. If we are to educate and, hopefully, inspire the next generation of healthcare scientist then universities are looking to recruit leaders who’ve been there, done that, and lived to tell the tale.
Clinical Academic Purgatory
In a recent lecture on roles in the NHS, a student asked me where I currently sit. I pointed to the training pathway for healthcare scientists at point 4 – the Clinical Academic Career. ‘Ah I see’ they replied, “you’re in Clinical Academic Purgatory whilst you have your kids, you’ll go back to your real job eventually”. Well that stung a bit! But it’s a valid point, I think that the move to a teaching role in a university is often seen as a bit of a soft option. Nicer hours that running your own lab with a better work life balance, just don’t mention the marking! It’s not completely wrong either, the chance to spend my evenings and weekends with my partner and children even when drowning in marking is a huge perk.
However, I view this move as more that a pause on my way to a consultant gig. I think that this collaboration offers us an incredibly important opportunity, the chance to share our stories. When I reflect on my many years in both universities and hospitals, the moments I remember are not learning the details of the complement cascade or T cell receptor VDJ recombination (though of course both are very useful) but the stories told by my mentors, colleagues and leaders that made me want to become the scientist I am today. To my mind, we have a responsibility to those who are following on from us. Through collaboration with our academic institutions, we can help perform this essential service to our profession.
As a clinical scientist turned lecturer, I’ve spent a good deal of my career bouncing between the laboratory and the lectern but I have often found that never the twain shall meet. I think it’s time we change that.
TLDR: What do we want? Co-Production! When do we want it? At the start of the next academic year. It is nearly summer after all.
Let me start todays post by sharing what on earth pedagogy is as my husband kindly pointed out its not a term that comes in up in most every day conversation. Well according to the Merriam-Webster dictionary it means:
So why am I talking about this on a sunny Sunday afternoon. Well I’m chilling on the sofa and recovering from one of the highlights of my year, the Healthcare Science Education Conference (this year #HCSEd22). Needless to say I therefore have pedagogy on the brain as it’s an event that although pretty intense also re-energises and inspires me. There is absolutely nothing like seeing a room full of scientists coming together for change, and in my world when you combine this with mindset shifts linked to education it doesn’t get much better. We had many really amazing speakers and workshop leads that put both the science and art into education, plus the wonderful Ant De Souza chairing. When I have time to mess with the recordings they’ll be up on the Healthcare Science Education YouTube channel if you couldn’t attend the day.
This was the 5th Healthcare Science education conference and it’s been running for 6 years since 2017 (we missed a delivery year because of COVID-19). Over the years we’ve had some pretty diverse themes including:
Co-production in Education (2022)
Innovation in Education (2021)
What is the Role of Collaboration in Education? (2019)
The Role of Leadership in Education (2018)
Healthcare Science Education: Where are we now and where are we going? (2017)
I think it’s probably pretty obvious therefore that I’m interested in education, especially how Healthcare Scientists educate both themselves and others. It wasn’t always this way though. To be honest when I finished my training and got HCPC registration I had only really experienced education delivered in one way, from the front of a lecture theatre/teaching laboratory. I imagine you’re all thinking but what about CPD? Continuous professional development is important and I obviously have undertaken it, as we all have, but it’s task focussed learning. What I’m talking about is the wider mind set switch and set of skill development that enables us to think about the educational experience as a whole:
what kind of learning are we trying to achieve – what are our learning objectives?
what kind of educational experience is best to deliver those learning objectives?
how much time do we have with our learners – is it a one off session or a repeat?
where is the education setting going to take place – are we going to be in a lecture theatre or a more flexible space?
where are my learners in the topic? is this an introduction session or are we aiming to achieve changes in practice? deep vs surface learning?
how do I assess learning linked to the learning objectives and delivery method?
how am I going to get feedback? how am I going to evaluate if I’ve achieved my aims?
is there a role for the learners in co-producing the session? learning outcomes/assessment/delivery?
How did I get here?
Between achieving state registration and taking the next formal steps along this pathway I was fortunate enough to undertake a one year leadership course at GOSH called the ‘Gateway to Leadership Programme’. This was a commissioned course with monthly sessions delivered by external providers with additional coaching. The sessions were delivered in a wide variety of ways and whilst I sat in the room learning about leadership I also started to ask myself if this teaching was being delivered in an MDT format with different structures could other teaching be different too? For those outside of Healthcare Science this may seem like a really naïve position, other disciplines in healthcare, such as medicine, have been using problem based learning and other structures for years. I know this now, I’ve done the reading on it and now experienced it, but in 2009 it was just not my experience of any form of formal education.
In response to the learning experiences I had on that course, and the fact that it was my first cross disciplinary learning (outside of my Clinical Microbiology masters) I used the opportunity to quiz others in the room, to speak to my coaches about the differences between 1:1 learning and group learning strategies………………..long and short I was probably a pain the ass. I started to sign up to other courses that were being delivered by the Trust and I found that the hospital had an entire education team, an entire team dedicated to education and learning. This team didn’t deliver the mandatory education, they didn’t just deliver education on specific topics, they used something called pedagogy to put together education and learning opportunities in conjunction with subject matter experts, as education was a field of expertise in itself. It was nothing short of a revelation.
What were the next steps?
The people that I knew in training positions in pathology didn’t have a formal education qualification, most had an interest in training but it was focussed, for the most part, on specific delivery mechanisms such as portfolio completion. Although obviously valuable, this again limited the scope of the education I would be being taught to deliver if I went on similar courses and the rest of the departmental offerings were things like train the trainer courses. I was more interested in really getting to grips with some of the theory as well as the practical aspects. At the time I had a wonderful IPC lead as my boss called Deirdre and she suggested that what I really needed was to do a post graduate certificate in education. She suggested this because it meant that I would be able to support the team and the Trust in running courses in conjunction with universities, as it was a requirement on most of the modules for module leads to hold formal qualifications. At the time I was also pulling together my NIHR Doctoral Fellowship and looking to take the next steps as a Clinical Academic. UCL requires lecturers to have a minimum number of credits linked to a formal education qualification and so it seemed fortuitous to cost into my grant the course so I could undertake a PGCert as part of my PhD.
Was it what I had hoped?
So in 2013 I started a 2 year PGCert in teaching and learning in higher and professional education at the Institute of Education (now part of UCL). I think the nicest way to put it is that it was a shock to the system.
It was like nothing I had ever done, the essays were first person present tense for one thing, it felt like I was back in primary school writing for my teacher. The first 6 months were hard, I was clinging to the educational culture I had always sat in as a scientist and the idea of moving away from being the ‘expert’ in the room to someone who facilitated learning was something that definitely did not happen over night. When it did however it caused me to completely shift my thinking about how we deliver on education and training in healthcare science and the need to move away from thinking of ourselves as people who deliver task based learning to the fact that we are all educators. Therefore learning about how we do it, why we do it certain ways and how those choices impact on the success of the learning is a key thing for all of us as a workforce moving forward.
Despite the fact that the transitioning into thinking like an educator took me some time I think it was one of the most valuable things that has ever happened to me. So much so that I have since worked with others to get 5 other Healthcare Scientists funding to go through the same process. I also utilised the course to attain Fellowship of the Higher Education Academy which has enabled me to have the credibility to be able to put some of what I’d learnt into practice on a larger scale when I applied to be part of the T-Level Healthcare Science Development panel as an employer representative. It also meant that in 2021 I was fortunate enough to spend time working with a wonderful Lead Practice Educator in IPC called Kate to input into the first paediatric IPC course.
Why does it matter?
It is sometimes easy to forget that as a Healthcare Science workforce we exist as part of a wider system. By taking steps to upskill and acknowledge ourselves as educators we achieve 2 main things:
we can do a better job of training not just our own work force, but of supporting the system by sharing our specialist and valuable knowledge
we can build links and break down silos by working across disciplines and healthcare professions by working as educators across those boundaries in order to maximise our impact, with all the side benefits that has to us as scientists
The students and others coming through education now will have had a very different experience of education to that I experienced when training, therefore their training needs and expectations are going to be very different to those I had when I joined the NHS. The new curriculums being delivered by the National School of Healthcare Science and Apprenticeship/T-Level groups are bench marked against teaching and education delivered in other specialisms/professions and so standing still is not going to be an option. The more we understand, the better choices we can make, in terms of influencing those choices for our workforce and how we like to work with others. So lets not just join the education revolution but take what steps we can to lead it, for the benefit of ourselves, our workforce and the NHS as a whole. Hopefully I will see you all at #HCSEd23.
I have written lots of posts on this blog about being brave and saying yes to opportunities. For once I’m going to write about something that for me requires even more courage, and that is saying no. It’s not that I don’t stand by those previous posts, saying yes is incredibly important. The thing is we all need to know why we are saying yes (or no) and to make sure that we are choosing our responses for the right reasons. Neither response should be driven by fear. There are times that for our own health and wellbeing we need to know when to choose our responses in a way that isn’t about career progression or opportunities, and we need to acknowledge that that saying no is also OK.
I’m a FOMO (fear of missing out) addict. I always want to be engaged, I want to both support and be seen to do so. I’ve worked so hard to get into the room that I live in some level of fear about not being in it. I worry that if I leave the room I fought to get in, not only will I be forgotten, but I will be barred from re-entry.
Over the last year a number of things have happened which have forced me to put this fear into context. FOMO is a fear of missing out on the possible, but by not being present for my life I’ve been missing out on the reality of my life that is happening every day. Recent events have prompted me to send emails resigning from a couple of things. I thought it would feel awful (it might still at some point in the future) but it didn’t, it felt great. Not because I am not heart broken to step away from those roles but because of the removal of the weight of those responsibilities that I had not realised I was carrying with me.
I feel like not only am I happy that I took the plunge but in fact I want to Marie Kondo my diary i.e. look at each item/commitment and say ‘does this bring me joy?’. If the answer is no then I need to follow up with asking myself honestly ‘why am I doing it?’. Obviously there are many things in our day to day working lives that just need to happen, but I think you would also be amazed at how many of those things that we feel obligated to do are actually just a routine or something that we are doing because we tell ourselves we should. It is these things we need to interrogate ourselves over and ask what it is that they are giving us: joy, experience, contacts? Are they still giving those things to us or are we attached to the memory/habit. Are we just scared to face up to what it would mean to move on?
Reasons to regularly review
What this current experience has shown me is that I don’t review my working life. The last couple of weeks have taught me that I should. I’ve spent some time thinking about it and the thought that has struck me (and you probably all knew this already – I’m often behind) is that you have to let go of the things that no longer serve you to make room for things that will let you continue to grow. I’ve not been letting go of things. Partly because I’ve finally reached the goal I was desperate to achieve in my working life and to be frank I’m so happy about that I’m still scared someone will take it away from me. I’m so used to having to tick so many boxes, often driven by the check list of others, that I’ve stopped reflecting on what was on the list for me.
If you, like me, have fallen into the habit of just taking on more, of just carrying on without reviewing your why, this is my plea for you to take a moment to see whether this is something you need to change. We should take a moment to put a review date in our diaries – I’m aiming for once every 6 months – to go through my lists of committees and responsibilities to see whether they are still a good fit for me and for those I’m working with. After all, it’s not just about my needs but also about making sure that I still offer what was required.
Carve out time to maximise impact
For me its not just a review of task, it’s also a review of mindset that is required. It’s very easy to become a human ‘doing’ and not a human ‘being’. Due to the pandemic I feel I’ve got into the habit of being in responsive mode. Constantly responding to changing information, changing guidance and the hundreds of daily emails. Don’t get me wrong, this is where I think many of us needed to be for the last couple of years, but we need to break ourselves of this habit. It’s nigh on impossible to be strategic in responsive mode. It is also not good for our own well being – at least it’s not for mine. I know get stressed and twitchy if I don’t access emails on the weekend. I worry about being judged for not immediately responding to every demand. The problem is that after the last 2 years I am broken and I can’t maintain it. Not just that but whilst I’ve been taking the time to reflect I’m pretty sure that it’s not where I do my best work. Responsive mode is fine when in crisis. Crisis is time consuming however and leads to focus on specific issues. To work on how to improve services and identify where we can do better requires us to take the time to step back, calmly reflect and then make plans. Switching from responsive to strategic mode is therefore important not just for me as an individual but is also key to doing a better job for patients.
Interrogate your reasons for saying yes
Not only am I a FOMO addict but I’m also a people pleaser. I feel the need to get feedback from others in order to feel like I succeed (I have another post coming on this). This can be an effective driver but when it takes over it can become a really destructive trait. You do not need to say yes to everything in order to ‘show up’. You don’t need to work 12 hour days ever day in order to be successful, in order to be enough. In fact by working those hours and becoming so focussed on the minutiae you may actually be performing less well than if you did your 9 – 5 and had adequate time off to reflect and recuperate.
These are my reasons for over committing but your may be very different. All of the different drivers we have are both good and bad, it all depends on how they are balanced. In times of stress it can become difficult to find that balance – and we have all been mighty stressed over the last 2 years. Now is a good time to look at ourselves and our decisions to make deliberate and mindful choices moving forward. Our judgement of worth needs to be internal not external if we’re to get out of this loop.
Know your worth
Self worth is a tricky thing. As I said above I’m a people pleaser, my self worth is often therefore derived from pleasing others. It is also linked to success, and like many in my field I define that success linked to outputs – presentations, guidelines, grant funding, papers published. Like many others I have lived, breathed, and focussed on pandemic management for the last 2 years. Therefore my sense of self has become distorted and my self worth has become even more focussed on work.
The thing is there is way more to me than my job. I have passions and interests both linked to work (like writing and The Nosocomial Project) and with my family. It is my family that have paid the price for the shift in how I behave and determine my value, and it is my family that now need to be my focus in order re-establish the balance I need to move forward. As teams, as managers and supervisors we need to support each other in shifting mindsets post this unusual period, and remind them that it’s OK to leave on time, to have weekends and eat lunch. It is OK to be the fullest version of yourself.
Give yourself permission to say no
So moving forward I am going to give myself permission to not just review options and step away from projects, but also to say no to new ones. If I lose traction, if I lose opportunities because I say no on occasion and if I’m not ‘always on’ then that is a price that I have determined I’m willing to pay. Those people who know me and have supported me will not disappear overnight just because I take more time to focus my energies on being the best person I can be.
Opening doors for others
I’m also not going to feel guilty about stepping back. This feeling of guilt has been difficult to manage but it’s not well founded. By stepping back from positions I’ve done for a while I’m opening up progression windows for others to make connections and gain experience in exactly the same that I did. By learning to say ‘no but have you thought about’ I am making opportunities for others and hopefully lifting others up by putting their names forward. Realising this has been crucial to me not feeling guilty about saying no. My saying no means that others can say yes and that is nothing to feel guilty about.
Situations change and the thing that was right for you 2 years ago may not be right thing for you now and that’s ok. Fear and guilt shouldn’t prevent us from letting go of things in order to grow and learn. So as much as I’m an advocate of yes I am also learning to become more comfortable with no. Find your joy, say yes to putting yourself first and know that by doing so you will become even better tomorrow than you are today!
Firstly apologies, this post was supposed to go up before ECCMID as I was hoping it would help others attending. Work was just too full on and I didn’t have the headspace to get it written. As there are still a lot of events yet to come I’m hoping it will still prove useful however.
We all know how very important networking is, especially at conferences. So much of a career that makes a difference in science is based on who you know and who you collaborate with. The problem is making those connections and getting to know people, especially in the early part of your career, often requires taking the plunge and being the one to open a conversion with someone you’ve never met.
I have an amazing friend called Diane who is a wonder to behold in these setting. She happily goes up to talk to people who she’s never met and just starts talking to them with great enthusiasm. Shes fearless and draws the best out of those she engages with. If you are a Diane you probably need read no further. For me however, there is little worse than that moment when you enter a room at a meeting/event, get your cup of tea and survey the 100s of people before you. In this moment you know that really now is the time, you HAVE to find someone to talk to. How do you choose who? What on earth do you say that means you don’t come across as an idiot? The very thought of it gives me palpitations. So here are some things I’ve learnt that take some of the stress out of networking at conferences.
Find an in
There are some moments and set ups at conferences when it is easier to start a conversation than others. There is always the chance that the person next to you in an interesting session will strike up a conversation to help them process what they’ve heard but in general they will be doing the same as you, ducking into and out of sessions that trigger their fancy, meaning they will be you focused on what comes next not starting a chat.
I find however there are two key moments when people are available for the cold start up conversation.
The first is at food breaks/receptions. During these moments there will be people who are there solo and also looking to develop their networks. I find the best thing to do in these situations is to get there early. There are always a limited number of tables where people can put down drinks, if you can find one and hold a place then people will effectively come to you. If this fails and there are no tables, just being close to the source of the refreshments often does the same job. Food and drink are great removers of hierarchy and being somewhere visible means that those in a similar position to you will be able to see you and hopefully will head your way. Worst case you make some small talk to the group that comes to your table and you can politely extricate yourself if it all feels too weird by saying you’re popping to get another drink.
The other place where people will be desperate to speak to you is during poster sessions. So many people will be waiting at their posters for an hour in the desperate hope that someone will come and show an interest. This is often a great time to make connections/exchange contact details (see NB below) If you scope out the listing you will know you are speaking to people who are interested in the same kind of work as you. This can shortcut some of the small talk you might otherwise need to make. It also enables you to know whether you are making a connection with a peer or whether you are connecting with a potential mentor/future employer.
The other thing to think about prior to these conversations is what you can offer, what is your unique selling point?
NB one of my biggest tips for all of these situations is to make sure you have some business cards printed – even if you print them yourself – this means that you can have something easy to hand out or pin to posters if you want authors to get in touch
Find your tribe
Anyone who reads this blog regularly will know that I’m a bit of a twitterholic (@girlymicro if we haven’t met). One of the many reasons that I’ve stuck with twitter since I initially signed up is that it has transformed my networking experiences. Twitter has offered me a way to circumvent the cold start up conversation by allowing me to find my tribe.
These days every conference/meeting has a hashtag. By following this hashtag you can find people who are interested in the same things as you, people who are in the same sessions or who even have shared connections. In many ways its an improved version of doing the poster walk. Not only does this give you a conversational in but also by tweeting yourself linked to the thread before you ever meet in person it allows you to have a low stakes initial introduction.
One of the things I also love about twitter is it enables me to find and arrange to meet up with people who I primarily know online in order to strengthen my networks by getting to know each other better. It also gives me the chance to arrange collaboration events, like podcast recordings, when we just happen to be in the same place for a limited time. Both of these can obviously be done by email but can be much easier to arrange when at an event when you suddenly have half an hour free. Especially at big conferences you could wander the halls for 4 days and not meet anyone you know, this way you can make the most of every second.
Take a study buddy
I absorb my learning best when I have someone to talk through my thoughts with. I have a couple of trusted study buddies that I will by preference attend events with. These guys help me get the most out of any event by:
Encouraging me to be braver – ask those questions I might talk myself out of, talk to that person that I should really try to connect with
Providing me with a sounding board for ideas when I’m in the moment
Enabling us to divide and conquer – there are often multiple sessions I want to be in at the same time, this way we can split up and meet at whichever session is actually proving most appropriate
Knowing me well enough to give me space when I need down time to re-energise
Crucially for me they are also there so I can feel safe from a health perspective if I have issues. They’ve helped me manage severe reactions, broken limbs etc and I trust them to get me where I need to be and give healthcare workers the right info if I need care
Mel and Lena have been my colleagues for years and they can not only get me out of a shame spiral if I do something stupid but also, by having them available to have conversations all together with new collaborators, we can make much more rapid progress on projects from the very start.
One of the other great things about going with a great study buddy is that you can also achieve other goals whilst at the conference. You can start to get papers drafted, do that research return or catch up about PhD students. If you do have supervision responsibilities whilst you’re away, as you have trainees with you, you can also share the load in terms of ensuring you have downtime. A lot of my most creative breakthroughs have happened with these guys whilst we’ve been away, surrounded both by new science and the time to reflect on how we could encorporate new thinking into our work.
Do some pre-work
I can get really insecure when going to high stakes meetings, like some of the ones I’ve been to at the House of Commons. I never really feel like I fit in and I have been known to hide in the bathrooms there until 5 minutes prior to an event start so I don’t have to face the ‘meet a stranger’ chit chat. In recent years I’ve learnt the value of doing some pre-work ahead of these meetings. This has taken different forms:
Reaching out on social media to see if any of my connections are attending
Approaching a professional body, especially if I’m on their guestlist, to find out who else they are sending so I can pre-arrange meeting at the session
Researching the event to look at speakers and attendance list (if available) so I can pre plan who I might want to speak to and what I could start a conversation with
In these events part of the value is in expanding your network and so really thinking about why you are going and what you hope to achieve is really worth it. Then you can match your elevator pitch (who you are, what you do and what you can offer) to your goals to help you achieve them.
Become the person others come to speak to
One of the things that has become lovely in recent years is that I’ve realised if you are presenting/organising/chairing people come to speak to you. This removes a whole lot of the stress of networking. As I mentioned above, people will often come to you even when you are presenting posters. Its always worth submitting work therefore to events you are attending, not only to get feedback on get science, but also to support you in developing your networks.
Even if you are not in a position to submit work then you should think about offering to support the organisation of events. Meetings are frequently looking for individuals who are happy to support the event organisation, both ahead of time and to do things like man the desks during the event itself. This will mean that you get to know other people who are supporting event delivery with you and give you an opportunity to network with delegates and speakers in a supported way. These connections can be transformative in terms of giving you further opportunities down the line.
Know your self and your limits
Most people assume I’m an extrovert when they meet me and I definitely have a lot of those traits. The things is, I can only manage networking for a fixed period of time. I’m good for a couple of meetings but then I need to retreat back into my bathroom office and answer some emails, otherwise I just feel progressively drained. The older I get the more I need my own space. This is usually fine but presents a real problem at places like conferences where I may need to be in full on extrovert mode for 16 hours a day. I find it exhausting.
One of the things that I’ve discovered about networking is that I therefore have to schedule it in a way that works for me. I can’t agree to go to lots of dinners on top of full day events, either from a health or a social resource point of view. I therefore pick the moments that work best for me and don’t over commit. This does mean I sometimes worry about missing out and not making the most of every opportunity but it also means that I put myself and my wellbeing first. It means that I don’t leave a conference unable to engage with work when I get back as I’ve already used up all my resources. Therefore my top piece of advice is to understand that networking is key but find a way to do it that works for you. Pick your key moments and do them well, rather than trying to be all things to all people.
All opinions on this blog are my own
If you would like more tips and advice linked to your PhD journey then the first every Girlymicrobiologist book is here to help!
This book goes beyond the typical academic handbook, acknowledging the unique challenges and triumphs faced by PhD students and offering relatable, real-world advice to help you:
Master the art of effective research and time management to stay organized and on track.
Build a supportive network of peers, mentors, and supervisors to overcome challenges and foster collaboration.
Maintain a healthy work-life balance by prioritizing self-care and avoiding burnout.
Embrace the unexpected and view setbacks as opportunities for growth and innovation.
Navigate the complexities of academia with confidence and build a strong professional network
This book starts at the very beginning, with why you might want to do a PhD, how you might decide what route to PhD is right for you, and what a successful application might look like.
It then takes you through your PhD journey, year by year, with tips about how to approach and succeed during significant moments, such as attending your first conference, or writing your first academic paper.
Finally, you will discover what other skills you need to develop during your PhD to give you the best route to success after your viva. All of this supported by links to activities on The Girlymicrobiologist blog, to help you with practical exercises in order to apply what you have learned.
It has kind of snuck up on me, but this is the 100th blog post on Girlymicrobiologist.com. I’ve had such tremendous fun and learnt so much about myself writing them. Talking to people about them has also been an unanticipated joy. I don’t therefore think I’d realised how many posts had happened over the last 18 months or so. To mark the occasion I thought about writing some top tips and discussing the things I’d enjoyed most, but I cover a lot of that in my 1 year anniversary blog. Serendipitously this post coincides with me having been in a Consultant post for a year this week, so I thought instead I would share what it’s been like………….
Everything I thought and more
I’d worked with a fairly single minded focus to get here. At some points it really felt like it was never going to happen. The wonderful thing is that it has been everything I hoped for and more, something that isn’t always true for dreams and aspirations.
The interesting thing for me is that the core of my job isn’t really that different from my job before, I kept waiting for it to change but it hasn’t really. The biggest change I think is the weight of responsibility I feel for my team and that, for some of the big decisions, I end up advocating on my own. I am aware some days that I’m on a trapeze without a safety net. That said, as the Consultant Nurse for IPC/DIPC and I talk every day we always have each others back. I can’t imagine having spent the last year in a pandemic doing this solo, and so this relationship has been a god send.
I must however talk about the thing that has been strangest to me. I left work on a Friday and came back on a Monday as a Consultant. From one day to the next a lot of people changed the way they interacted with me. People who had known me in both roles. On the Friday they would challenge me routinely and call me Elaine. When I came back on the Monday, the same people called me Doctor and just agreed to things. When I sent emails that I anticipated would come back with nit picking or challenge from some medical colleagues they just responded with OK thanks. Don’t get me wrong there have been plenty of difficult conversations but far fewer than I had anticipated. Anyone who believes hierarchy doesn’t exist in the NHS should experience this transformation by just sticking Consultant into their job title. I still can’t quite get my head around it.
The other thing that I’d been really fearful of when I switched was using the Infection Control Doctor title and having people telling me I couldn’t as I wasn’t a traditional medical doctor. I agonised about having it in my signature and putting people’s backs up. You know what…..not a single person has mentioned it, let alone said anything bad. I can’t tell you how grateful I am for this. It was that title more than any of the others that held real meaning for me and I was so scared of being rejected in that post. The fact that people haven’t rejected it but in fact embraced it means so much. As someone coming from a different place via a different route it is hard to quantify how much that has meant to me and given me hope for how we embrace change/difference in the future.
The whole truth and nothing but the truth
Now I’d be lying if I said the joy and acceptance described above hasn’t come with a whole of heap of challenges. I’m going to talk about the challenges of becoming an IPC Consultant in the times of COVID-19 below, and some of the bits I’m going to cover here I don’t know whether they are the same or worse because I started in a pandemic. It is worth stating that most of these existed before the big P, but that like many things in a period of change they may have been exacerbated.
I talked about about how much the IPC Doctor role has meant to me, its been the goal for 16+ years afterall. I think because I assign so much mental value to it that I doubt myself and fear that everyone is going to realise the horrible mistake they made on a pretty much daily basis. The shoes I’ve had to fill are massive ones left by such an impressive and knowledgeable individual, you can’t help but worry you will disappoint. Taking over at this point is therefore challenging when there have been big decisions and big changes every week it feels. I’ve talked before about how failure is key to learning but every action right now feels like it is too important to fail. That fuels my inner perfectionist and means I have a tenancy to spiral. Deep breaths and ‘faking it until I become it’ have definitely been my survival tools for my first year in post. I’ll let you know when the ‘become it’ happens.
The acceptance has been great, I’ve been incredibly lucky but on some level I still know I’m never going to be part of the club. My micro consultant colleagues go for coffee and lunch together but I can’t join them. I’m the person setting the guidance that says you shouldn’t mix, even after work. They will always spend more time with each other in hand overs etc which means they have enhanced relationships with each other. This isn’t a bad thing. I have relationships that they don’t have and my job role is different. I guess it’s human nature to want to be accepted and part of the group however. The strength of my position is that it is different and in many ways my strength is that I’ve always followed my own path. There have been times over the last year that I’ve needed to remind myself of that. They have been nothing but supportive and inclusive when I’ve reached out and so it has been a lesson to me that if I need help I just need to ask for it.
This leads me onto the next thing. I’m a stand alone Consultant Clinical Scientist within my department. I have nursing and medical consultants that I work with but no one like me. This has meant that sometimes it requires specific focus for both myself and others to remember the scientist part of that title. Being a scientist is a huge part of who I am and my concept of self. It’s understandable that others may not always remember that. Doing the bits that mean I am still a scientist is hugely important to me, things like undertaking research and advocating for my professional group. Some of this is tied in to re-discovering my identify full stop having focussed for so long on reaching this point. I’ve crossed the finish line and so what does the next goal look like, how does that fit in with my scientific identity. How do I ‘fit’ whilst still maintaining that of which I am proud and makes me different. This one is definitely a work in progress and as I learn more I’ll share whatever conclusions I come to.
Here’s the one that will surprise none of you = the to do list never ends. I feel like I’m constantly running to stand still, working weekends just to keep sight of what’s going on. Some of this I think is linked to me wanting to do my best and being anxious about it, some of it is because I don’t want to let go of some things I used to be involved with, but to be honest I think a LOT of it is trying to do all the pre-pandemic work on top of a pandemic work load. The ever changing guidance and the constant messaging required to keep people safe. If life is like this three years from now I will definitely need to drop things that I would love to still be engaged with, for right now I’m mostly taking each week at a time and hoping at some point to see what a consultant post in non-pandemic times might look like.
IPC doctor in the time of COVID-19
Until that day arrives when SARS CoV2 doesn’t control my every moment I continue to spin that one enormous plate on top of everything else. One of the biggest things I’ve learnt over the last year is that leadership, in all its forms, could not be more important. There have been some pretty tough lessons about seniority that I’ve had to learn as well.
I’m used to being able to make decisions, decisions based on evidence. If the data is sufficient I’m not used to people challenging or not engaging with those decisions. I’m going to post about this more in a future blog I think, but one of the lessons I’ve had to learn is that my ability to influence has limits. That the risk assessment others are making is not necessarily the same as the one that I am, and the weighting of the different factors within it are not necessarily the same as mine. Sometimes my role is to advise but if that advice is not taken up because that risk assessment is different it is not a failure of me in the role that I hold. It is the reality of advising on a single part of a much greater puzzle. Try as I may therefore I have had to acknowledge that this isn’t a battle for an outcome, but a collaboration where the outcome may or may not be the one that I would have chosen. As long as I advocate to the best of my ability, live up to my values and embody the leadership I want to see, that is all I can do. If I see it as a battle we all lose, if I see it as co-production we all win. Changing my point of view on this has been key to my surviving at certain points, especially linked to Omicron.
Talking about leadership, I don’t think embodying that leadership has ever been more important. Everyone is tired and everyone has gone through a period of extraordinary stress. I’m still asking staff to behave in ways that add to that stress i.e. by not having lunch or even drinks with their teams together outside of work. This means that a key way that we normally support each other is no longer available. We haven’t been able to celebrate or commiserate with each other for over 2 years. I’m a really strong believer in not asking others to do what I’m not prepared to do myself. Over the last year that has included me leading the way with opting in openly and discussing the pros and cons of routine asymptomatic lateral flow testing. Being open with people about my reactions to the vaccines and booster but how I went ahead and had them for the protection of myself, my colleagues and my patients anyway. It has also included me missing out on that same support I have deprived others of by reducing their contact with colleagues. To me its about fairness and showing with actions rather than words that we are all in this together.
The importance of paying it forward
There are some people in my world who went all in to get me this post, people who I will never be able to thank enough. Mentors who have been with me every step of the way and who put their names and reputations out there vocally to support me, fought battles for me that I know no detail about. Those people have changed my life. So now it’s my turn. My turn to fight for others. My turn to act as a shield and as a mega phone. I have thanked those that helped me but I don’t think they will ever really understand the difference they made, so now I honour that by vowing to make that same difference to those who follow behind.
So here I am (successfully?) having broken my way through that glass ceiling. If anything this last year has shown me that this isn’t the end of the journey but the start. If I want others to not have to have the same fights as I did, then I have to work to make sure I keep that hole open and drop a ladder through it to help those who want to follow. Those coming after me will have different challenges but it’s important to share what I’ve learnt to help them where I can along the way. It’s one of the many reasons this blog is so important to me. So as a fitting message in this 100th post I wanted to say that for as long as you guys keep reading, I will keep sharing. Sharing so we can rise up, sharing so we can make change and sharing to make sure that we are seen and to help us all work every day to leave the world a slightly better place than we found it.
Healthcare Science Week performance based on the weekly ‘Girlymicro’ blog by Dr Elaine Cloutman-Green, followed by a discussion on blogging
“So, this is my first ever blog post. Bear with me as I don’t really know what I’m doing. I’m what is known as a Clinical Scientist and I work in Infection Control.”
Thus began the first blog post by Dr Elaine Cloutman-Green, Lead Healthcare Scientist at Great Ormond Street Hospital, in December 2015. It would be five years and one pandemic before her second post, in October 2020, began her weekly blog as ‘Girlymicro’ (‘scientist changing the world one swab at a time’).
Girlymicro blogged at first about the job, to promote Healthcare Science, offering professional exam or interview advice for HCS trainees, before ranging more widely, into women in science, the challenges facing HCS, exploring the limits of what overstretched teams and individuals can achieve, saving lives in labs through insight, accuracy and interpretation.
Each blog written in a snatched hour, Girlymicro became a mental space populated with personal reflection, meditation on loss, favourite microbes, special guests, puppet shows, and… zombies; always with Elaine’s trademark humanity and humour.
‘All Opinions In This Blog Are My Own’ is a showcase of a devised work in progress based on the Girlymicro blog by The Nosocomial Project, adapted by Nicola Baldwin, performed by two actors, Becky Simon and Peter Clements, and two Healthcare Scientists, Anthony De Souza and Dr Elaine Cloutman-Green.
The short performance will be followed by a conversation on writing and blogging. Why blog? What might you learn along the way? Does writing create a safe space for reflection? Or create new pressures? To blog or not to blog…. That is the question.
All welcome
Date and time
Fri, 18 March 2022 15:00 – 17:30 GMT
Location
South Wing University College London
IAS Common Ground, South Wing
UCL Gower Street London
London
WC1E 6BT
please register to attend on this link, please take a lateral flow prior to the event and wear a mask
I’ve talked a lot previously about the fact that we should only really compete with ourselves. We are all different as are our lives and therefore it makes sense that all of our success criteria will be different too. It’s too tempting to bench mark against others and find yourself wanting. This can be a great driver but it is also something that I for one find difficult some days as I don’t know if it can be turned on and off.
Three years ago today I ended up in a cast from shoulder to wrist. I fell out of a lift at work and protected my work laptop and phone and failed somewhat to protect myself. I’d never broken anything before and so was convinced I’d just sprained something (despite not being able to straighten my arm). I therefore took ibuprofen and paracetamol, went to three more meetings and told everyone I’d be back on Monday – this was a Friday morning. On Saturday morning I was forced to admit that maybe there was something wrong and finally went to A & E (after checking my emails). There I was told I broken my elbow and that I’d have a fracture clinic appointment in the week. I shrugged and said well it’s only and elbow and so worked from home as that didn’t mean I couldn’t type……..right. I finally turned up at fracture clinic and I had broken not only my elbow but also my wrist and then put a full arm cast on me and signed me off sick for 6 weeks. I’d never had a sick note before, I hyperventilated in the appointment and burst into tears saying that they couldn’t do it. They pointed out they could, insisted I took codeine for the pain and put me in the hands of my friend to take me home. What’s my point? My point is that that I don’t know when to stop. I was told by multiple people I should have gone to A & E on the day. I was told by many more to go home and not go to meetings? My husband was adamant that I was in pain and shouldn’t work prior to the fracture clinic as I had a broken arm. I made my wrist much worse and heal out of alignment because I typed on it for almost a week because I couldn’t stop.
So how do we stop when the person who is driving us to continue is ourselves?
I posted last week about the fact that I am often not that well, in fact today I am writing this post in bed as I just feel pretty rough. I’m used to needing to push through because if I didn’t I wouldn’t ever achieve anything very much. What’s probably worse is that I think I’m a fundamentally lazy person. Honestly if I could I would lie on a chaise longue in a library all day reading books and drinking tea. As I’m painfully aware of this aspect of my personality I do try (although my hubby may point out not always successfully) to counter it by being pro-active about doing things. The combination of these two mean that I don’t often know when it’s OK to take my foot off the gas and rest and when I need to knuckle down and push on.
There are times when this is useful
There are times when not knowing when to stop is actually useful. Pre-pandemic I used to run, badly. I’m not good at it, I’m not fast. What I am is stubborn. I continue to put one foot in front of the other no matter what. I’ve finished marathons and half marathons with blood up to calves and enormous holes in my feet but I get into a zone where I just put one foot in front of the other and the pain doesn’t matter so much.
When it comes to working in healthcare I find the same thing happens mentally as well as physically, you just keep going. No matter what the warning signs in terms of burn out of physical health, you keep going because that’s what we do. My auto immune condition entered a whole new phase when I was doing my PhD and I’d just finished a half marathon (whilst in my 3rd year of PhD) when my husband noticed I’d lost a patch of my hair. None of it stopped me. I still submitted my PhD a year early so I could do FRCPath and complete my consultant training.
I succeeded because I just pushed on, because of the habit of putting one foot in front of another. At the time finishing was everything, now I wonder if there were more sensible ways and if I should have listened to those around me, but I was on mile 9 (which I hate) and I just wanted to get the equivalent of mile 13.
Medicine and healthcare are hard places to break the habit
I work in an amazing organisation, filled with the most amazing people. They are all also super smart and world leading experts. I’ve worked there for almost 18 years, I trained there, I’ve grown into an adult there. Being surrounded by people that smart, that successful becomes an embedded driver in itself. You want to succeed for yourself but you also want to succeed for them. As someone who thrives on doing things differently I wanted to follow my own path, break glass ceilings and set the way. To do that however you have to succeed, you have to tick the boxes that people think you can’t tick and so you have to find the drive to continue even when it feels impossible.
As a Healthcare Scientist there is track that needs completing in order to reach the consultant end point I was determined to achieve, for me it was supposed to look something like this:
Masters (years 1 – 3)
State registration (year 4)
Membership of the Royal College of Pathologists (year 4)
PhD (years 5 – 10)
Fellowship of the Royal College of Pathologists (year 11)
Even though I’ve talked about not benchmarking against others the need to complete these goals become embedded in your psyche. You become very focussed on the track that you are on, in the same way that I run, you get into the zone and take one step at a time. Sometimes however when you are in that zone it’s hard to hear the voices that say you could do it differently, that you could take a break between stages, that you could take that afternoon off to refresh. In my case it was hard because I was on fixed term contracts for the first 13 years of my career, until after I had my PhD and FRCPath. There was therefore a ticking clock in my brain that if I didn’t demonstrate enough commitment, get enough done, that I would lose my job and a career I loved. Not only was I competing against myself but I was competing against time.
So how do we stop?
All of this drive has definitely had its benefits, as I said there are times when this self-competition is really helpful. I would not have managed to get a consultant post or tick all the boxes that needed ticking without it. The issue is that how do you stop when it is no longer useful or even harmful?
I’m still working on this one but here are some things that I’ve found useful. The first one being is to listen to the balancing voices. There’s a lot of good in social media but it’s sometimes easy to only hear the things that re-enforce the fact that we should be working harder and doing more. There are other voices out there however that should make you stop and think about whether you can stop and take a break or just do it in a different way altogether, try and pay as much attention to these as the ones that drive you to keep doing what you’re doing.
Think more about who you are listening to when getting face to face advice. The day I broke my arm at least 3 people told me to go to A and E. I knew something wasn’t right but I listened to others that re-enforced my inner voice to keep going. It was my friends and family who were the ones that said to stop, the ones who prioritise me over Dr Cloutman-Green. Do yourself a favour and listen to these people more. Their priority is you, not the roster, not the deadlines and not the work. Amplify their voices in your mind rather than listening to others.
Finally I’m trying to become my own critical friend. If I was giving advice to someone on the situation I find myself in, would I tell them to push on or would I tell them to stop and rest so they can come back stronger? This is definitely a skill and I am definitely at amateur level right now, but I am working on giving myself permission, permission to leave on time, permission to eat lunch and permission to do things I enjoy that have nothing to do with work. I know some of you out there are so much better than I am at this, and as I said, I am a work in progress. I’m trying to remember therefore to enjoy the learning and the journey. Life after all is just a ride.