I spent a long time agonising about whether I should publish this post. I really felt that it would come off as boastful and all about me, me, me. The main reason I wanted to post it, however, is that it is absolutely not all about me. Too often science is played as a solo event, when nothing could be further than the truth. Science is a team sport and no one can succeed as a scientist without untold others getting them across the finish line.
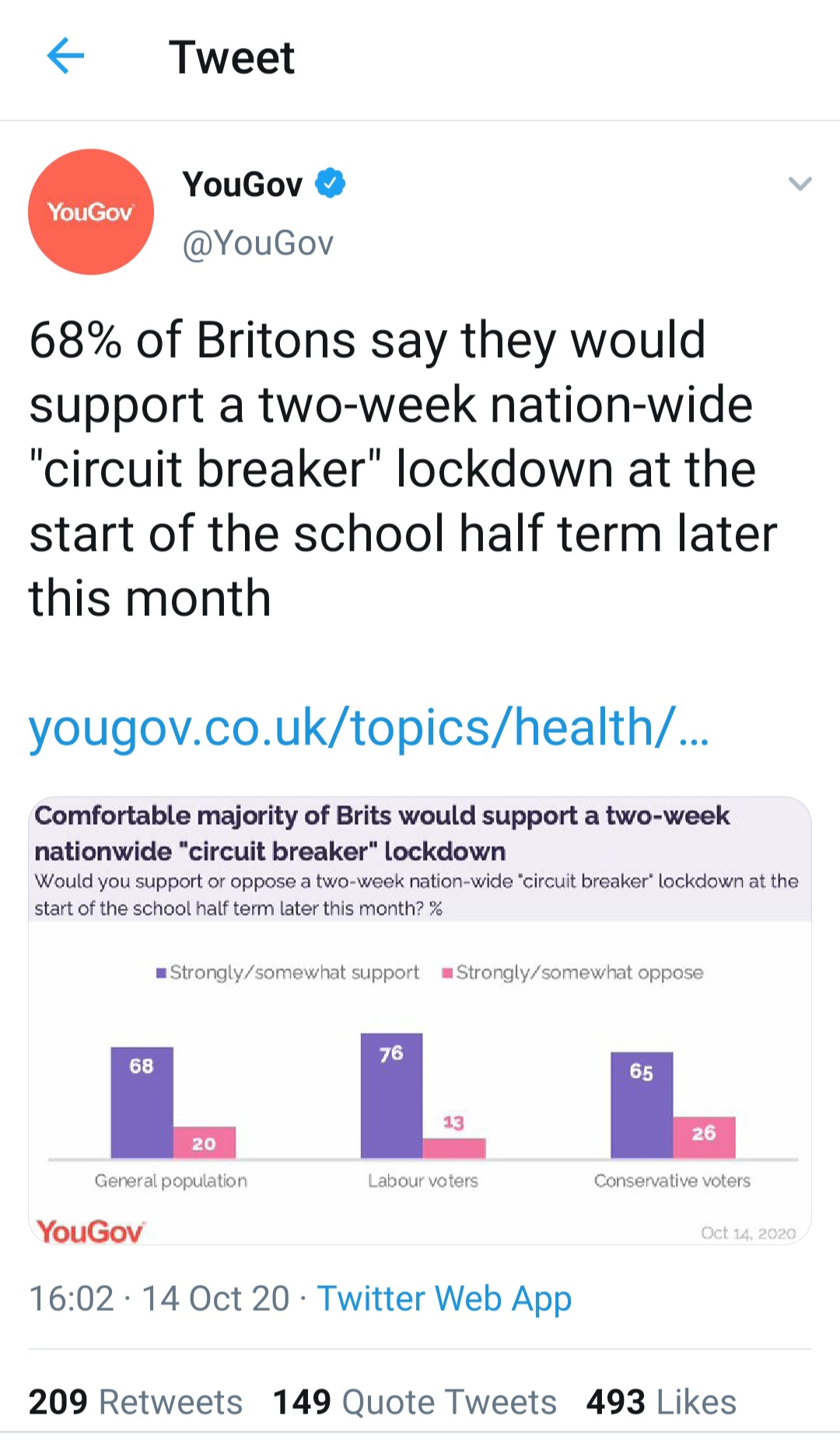
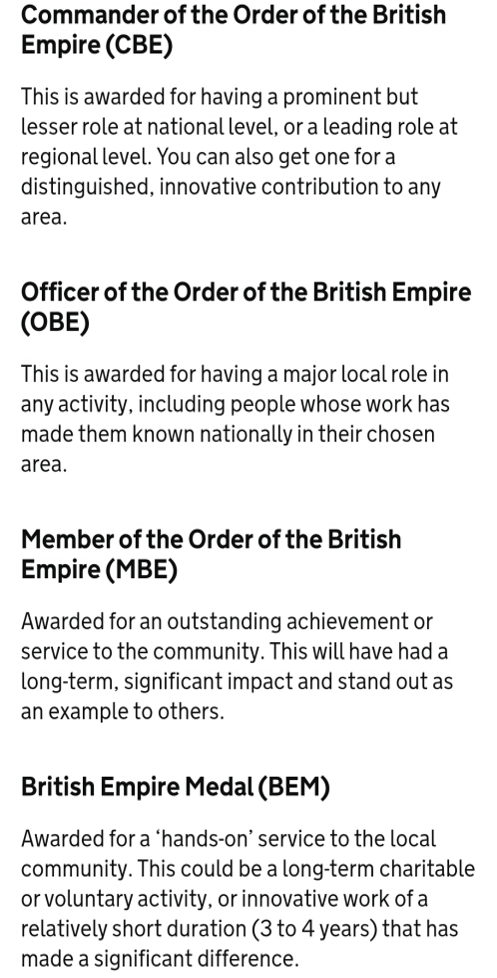
I should probably start by saying what a B.E.M. is. It stands for British Empire Medal, and I’m lucky enough to be awarded it as part of the New Year’s Honours scheme for services to Healthcare. I had to look it up as it wasn’t a name I was familiar with, but it’s basically one down from an M.B.E. Just typing that makes me feel a little stressed out…
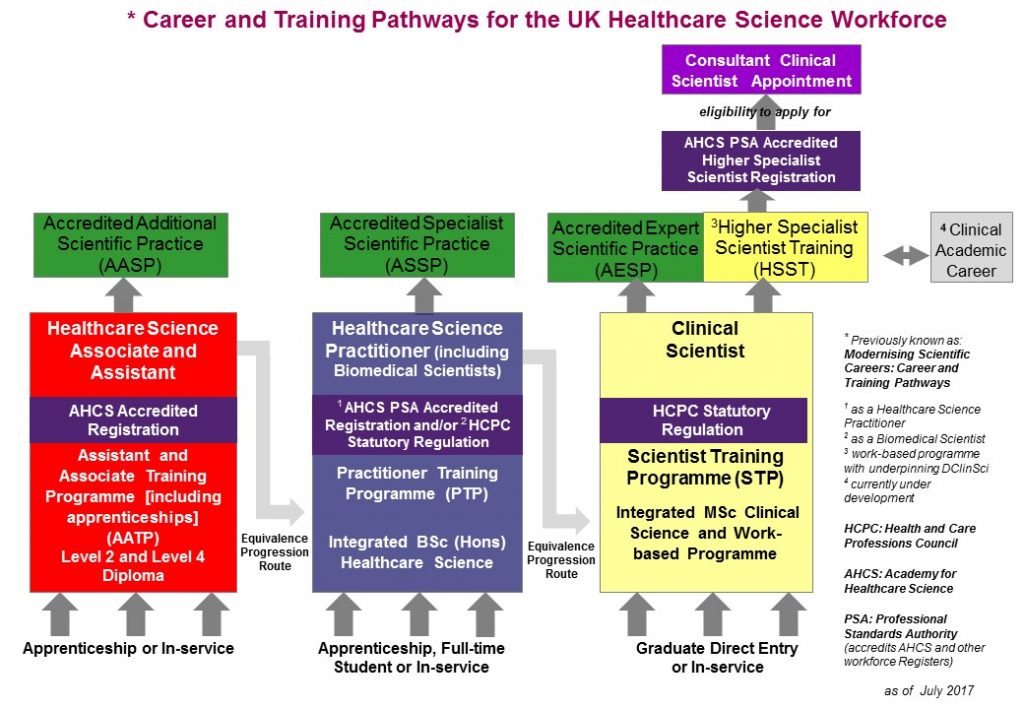
So here I sit on the 30th December 2020, writing this and thinking about how my scientific, Infection Prevention and Control and Healthcare Scientist career is filled with wonderful individuals and teams who have enabled me to end up where I am today. I’ve tried to capture a gallery of just a few of these amazing people below but there are more, such as my IPC team and brilliant HSST Francis, that I don’t have team photos of.















How Did This Happen?
On the 9th December, at 16:30, my husband phoned me at work. He was concerned that he had received a call on our landline. This never happens as we don’t really use it and, to be honest, I don’t even know the number. What was even more unusual was that he answered it. Mostly we never hear it and would check the messages once or twice a year. The reason he answered was because he happened to walk into the room as the message kicked in. It said the call was from the Cabinet Office. He picked it up, curious, and the woman on the phone said she’d been trying to get in touch with Dr Cloutman-Green and had failed to do so. Was it possible for him to give them my work email? He then phoned me at work to tell me he’d given it out and we both immediately thought it was a scam. So much so that I got him to give me the number of caller ID and then phoned back. When the phone was answered by the Honours office I nearly fell off my chair. They asked me if I wouldn’t mind staying close to my email for another hour or so as they were going to send an email which required a quick response, but that it was going to be nice (I was concerned I,d accidently broken some form of rule). Anyway, I stayed around until 6pm and below is what I was sent:

I then promptly fell into the cycle that I tend to do when something amazing happens that I feel undeserving of:

For the last three weeks I’ve been going through these loops, much to the understandable exasperation of my husband who believes I should hit excitement and stay there.
I’ve been wondering:
- What happens if this upsets other people?
- What if this isn’t the big deal it feels like it is?
- What will people think if I celebrate this? Will they think I’m arrogant and big headed?
Some of this is from experience. The first time I won an award at work, I was asked to put the trophy away out of sight as my ‘success makes other people feel uncomfortable’. Some of it is from cultural norms that make it embedded that celebrations are seen as arrogant: we should gracefully nod our acceptance and not make a big deal out of these things.
The thing is I want to celebrate is this. It is unlikely to ever happen to me again. I want to celebrate it for me, but I also want to celebrate it with all the vast numbers of people who have got me to this place. My amazing colleagues who make things happen. My friends and family who have put up with the missed events, forgotten birthdays and just being absent as work has been a focus. Most of all to my mum and husband who have always kept the faith, hugged me as I cried and held me up when I questioned if I was good enough to be a scientist, let alone be recognised.

I also want to support others to feel like they can celebrate when they get recognised, with the joy of us lifting each other up, not the fear of it making us a target to be torn down. Change starts with action and so this is mine.
So here I am waiting for this to be announced on New Year’s Eve. I’m hoping you’ll excuse me for trying to celebrate this one, for trying to sit back and smell the roses, and – for once – being in the moment rather than moving onto the next thing.
I’m also hoping that you’ll all realise that if someone as normal as me can be recognised, then we should all realise just what we can achieve and that our only limits are the ones we put on ourselves. Dream big and learn to fly.
All views on this blog are my own.