You may have noticed that I’ve been a little poor at keeping up with the Girlymicrobiologist site admin, and missing the odd weekly blog post. This isn’t because I’ve been slacking, honest, it’s more because I may have become a little distracted by a new project. I promise to get back on top of things soon, but in the meantime I thought I owed you an update.
Many of you have been kind enough to support last years project, which was a book aimed at supporting people to engage with research and research degrees, and I couldn’t be more grateful for your cheer leading. This new project, however, in the words of Monty Python could be described as ‘and now for something completely different’. It couldn’t be further from a book about academic study. This one is all about something else I love passionately, movies and TV.
I finished and launched the last book last October, and to be honest it hadn’t occurred to me, prior to letting it go into the wild, that I would write anything else till my retirement – when I’m planning to write some pathology based murder mysteries. It was never the plan to do something again, at least so soon. Frankly though, my brain tends to disrupt all my best laid plans, and ideas come meaning I just can’t help myself but get swept up. I’m blaming Ian McKellen inspiring me to ‘practice any art’.
Despite having no plans to do more, I have to say that I really enjoyed writing the first book, and I found the process of being able to write in a different way very fulfilling. I love writing this blog, and the first book is based on a lot of the pieces I have written for here, but it was nice to see them come together and take on a new and different life of their own. I also enjoyed mixing up the writing of something on a single theme with writing blogs on different topics for here, although I did rely a lot on Dr Claire Walker bringing together many guest blogs to allow me some writing time. It was lovely to see what those guest blogs brought to the site, and I really enjoyed seeing how including those voices really makes this feel even more like a community space. Without realising it, I think I caught ‘the bug’. Now, I’ve always enjoyed writing, this is my happy space, but I had never seen myself as an author, having held a book I’d written in my hands though, I can see how it could become a little addictive.
As I was sitting watching horror movies as part of my post release recovery, and researching for my 2025 Halloween post, I suddenly realised what I’d like to do next. I really wanted to write about some duel loves of mine, movies and TV plus infection.
Without any expectation of writing another book, all of a sudden I had a structure in my mind, and Don’t Open That Door had began…
You all know how much I am a movie and TV buff, everything from guilty pleasure reality TV, like The Secret Lives of Mormon Wives, to documentaries, and all genre of film (with the exception of torture porn horror movies, I’m a Blumhouse girlie). Whilst enjoying some down time with Mr Girlymicro, I realised how widely infection is featured in all kinds of different genera settings, some of it was actually pretty good, whilst some of it was really poor. So the first step was to do a whole bunch of research about what kind of examples were out there, by hitting up a bunch of different lists that have been collated by others, internet searches, and sourcing opinions from my movie loving friends. All of which led to the creation of a list of 138 options that needed a review to see if if they were actually linked to infection, and if they were infection based….was the infection content any good.
If you follow me (Girlymicro) on Instagram, you will have probably seen a number of stories that I’ve posted recently linked to movies I’ve been watching with some Infection Prevention and Control/micro commentary:
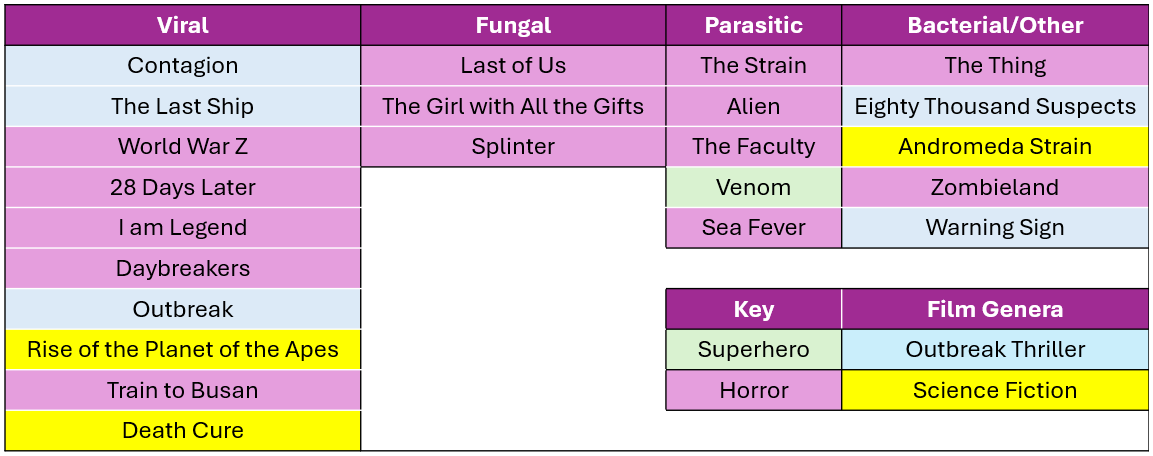
These have come about whilst I’ve been watching the 138 films/series with Mr Girlymicro to decide which ones make the cut to be included. I’ve watched some awesome films, some like Sinners, weren’t based on infection so couldn’t be included. I have also watched some truly bad movies, I even gave Resident Evil another go, and have spared you all by making sure that it is not included on the list. One of the considerations was that, even if the science wasn’t dreadful, I haven’t included anything that I or Rotten Tomatoes include as being truly horrible. I’m not just saving you on this, but also myself, as I’m having to watch included examples many times as part of the writing. I also felt it was really important to cover infections linked to viral, fungal, parasitic, and bacterial causes, just because they behave so differently and the interventions needed are so different. So the final list for inclusion involves movies and TV series that sit across infectious agents, although viruses are more represented than any other cause.
There are plenty of horror movies on the list, purely because they represent A LOT of the infection genera, but I was surprised at how many options there were outside of horror movies. I also tried to mix up certifications where I could, so that there are some options that everyone might enjoy.
Not everything could be included however, and there were also some exclusion criteria that impacted what I could include. Exclusion criteria included factors such as availability – no point including things that people can’t access, language options – I sadly only speak English so it needed at least English subtitles, and most importantly not based on real life events – this is about fiction.
For inclusion examples also needed to have infection as a central theme. This meant that health dramas could not be included as they only feature infection in some episodes, but at some point I do really want to write something that compares different medical dramas (House, New Amsterdam, Holby City etc) and maybe do a ranking scale….let me know if you think that would be a fun blog post.
Image credit The Red Dress
The reason it felt timely to talk about this today, is that the Biomedical Scientist magazine has been kind enough to do a whole feature on what the new book will look like, with a bit more detail, and some examples of what chapters will look like. It dropped on the 27th March and you can check it out the link here: https://thebiomedicalscientist.net/2026/03/24/infections-films. Also, how awesome is the art work they’ve done, can’t say enough how awesome The Red Dress are.
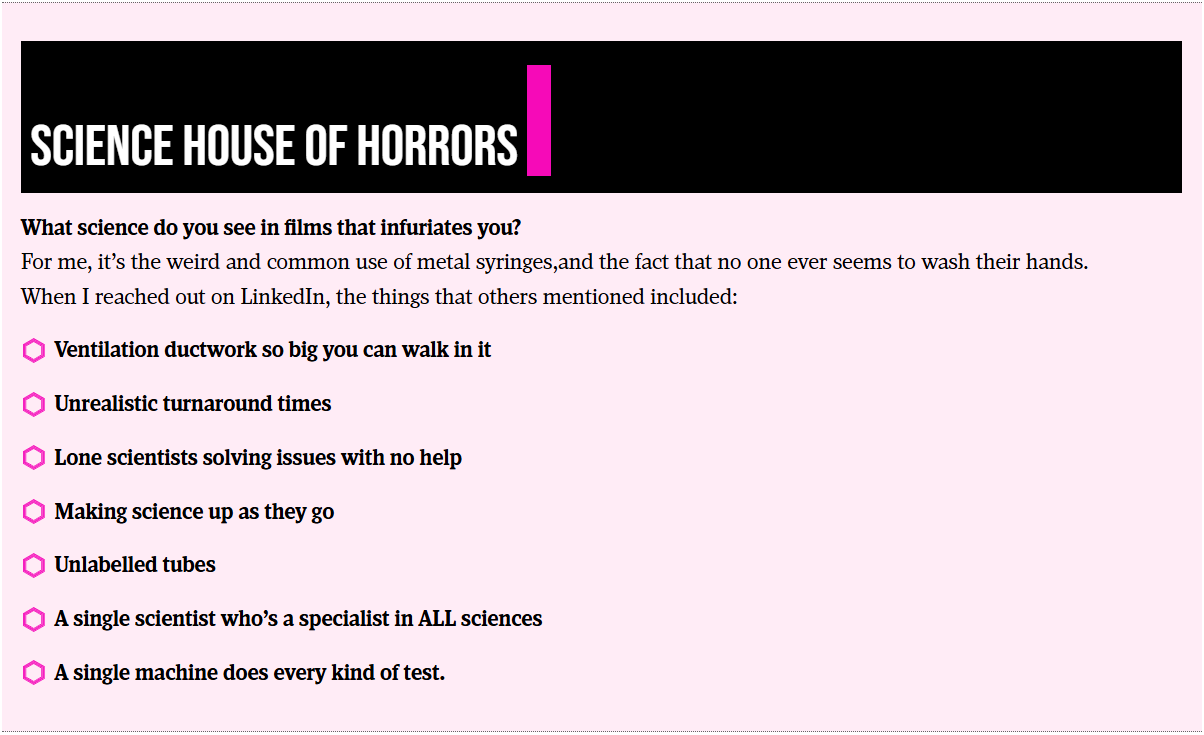
Whilst writing the article for the Biomedical Scientist and watching the example movies, I couldn’t happen but note how many weird and wonderful things are included as part of the science representation. Things that in my scientific career I rarely if ever encounter, but seem to crop up time and time again in Hollywood depictions of scientific life. I’m collating these for one of the final chapters in the book called ‘Science House of Horrors’ as I find them a bit fascinating. I’ve included some of the ones in the Biomedical Scientist article that I noticed, as well as those sent through as responses from social media, but I’d love to know if you have any others that I should include.
There are other opportunities to get involved though, I have 23 films and series examples, but there is room in the book to cover 25. I’m really keen to get other examples that include fungi, but if there is just something brilliant I haven’t included please let me know. There will also be a chapter called ‘Hall of Fame’ that covers both amazing movies that just don’t have enough infection in them to be included, or ones that were great but not quite as good an example of an infection characteristic as the ones already included. There is also the ‘Hall of Shame’ for examples, such as the TV series The Rain and Resident Evil, where the science is so bad that it is note worthy in itself.
Anyone who drops me an email to elaine@girlymicrobiologist.com and inputs into the House of Horrors, volunteers film examples I’ve missed, or suggests contenders for the ‘Hall of Fame’ or ‘Hall of Shame’, will get their name included in the list of contributors at the back of the book. Science takes a village, so does pulling together a book, and I’m really keen that this feels like it comes from our community. I hope you enjoy the article and I can’t wait to hear from you about your suggestions.
I am so excited by todays’ guest blog post. I’ve been so eagerly awaiting sharing it with you all. I don’t have any tattoos myself but it is something that is common amongst my friendship group, and I get asked about tattoo related infections A LOT. Partly as I was involved in some of the investigations when there was an issue some time back. So, a post that could help address some of the risk assessment and best practices linked to this art form felt very necessary, even though I didn’t feel I was best placed to write one. Then I saw this great article from Julie Russell on LinkedIn and I just had to reach out and see if she fancies writing a guest blog for me, and thankfully she said yes!
I first met Julie as Head of Culture Collection at Public Health England, that has since changed it’s name to the UK Health Security Agency. She was an inspiring microbiologist, who just had so much knowledge, and she became a great phone a friend. Since then she has moved on to work in a really different area where she still gets to put her microbiology and infection prevention and control knowledge to good use, as the director of a tattoo/art studio in Muswell Hill. No one is better placed therefore to answer the questions that I always get asked and have not felt best placed to answer.
Blog post from Julie Russell
After years in NHS microbiology laboratories, I joined the Public Health Laboratory Service, where I provided external quality assessment schemes and reference materials to laboratories worldwide. After that, I decided to do something completely different. I now co-own and manage Old Marine Arts Group, a tattoo studio in Muswell Hill, London.
It hadn’t occurred to me that tattooing, one of the oldest art forms in the world, essentially creates controlled wounds on people to decorate their bodies. I’ve had tattoos since my 20s – my first done in a legalised squat by a friend who’d never tattooed anyone in his life before. There was no personal protective equipment (PPE) involved; it healed beautifully, and I didn’t think about it anymore.
Many thousands of people across the UK have similar stories with no ill effects. Yet infections linked to tattooing have been recognised since the 19th century, and the government quite reasonably seeks to minimise such risks.
Tattooing, Skin, and Infection Risk
Bear in mind that the skin has a rich, diverse microbiome consisting of millions of microorganisms, some of which can cause infections if the skin is broken. Tattooing involves puncturing the skin with needles thousands of times, to a depth of approximately 1.5-2 mm, to place pigment into the dermis, creating a permanent design. Invariably, the tattoo process causes some bleeding, and after it’s finished, short-term redness, swelling and scabbing are normal. Resisting the urge to scratch is essential to minimise the risk of infection.
A July 2024 YouGov1 poll suggests 28% of UK adults – around 15 million people – now have tattoos. The UK Health Security Agency (UKHSA) notes that the true prevalence of tattoo-associated infections is unknown. There are no statutory notification procedures in place for infections specifically caused by tattooing, and no indication that such infections significantly burden the NHS. Various estimates suggest that approximately 1-3% of tattoos become infected in the UK. Most infections are mild local skin infections that can be treated with a single course of antibiotics; severe infections remain rare.
Interpreting the Evidence
Publications on tattoo-related infections must be read with caution. A December 2024 paper in The Lancet Microbe2, “Microbiology of tattoo-associated infections since 1820”, highlights rare severe cases such as necrotising fasciitis, leprosy and atypical mycobacteria outbreaks. The authors state that, “Despite advancements in public health policies and increased awareness of tattoo-related risks, a notable rise in both the number and diversity of microbial infections has been observed with an increase in the population opting for tattoos, particularly since 2000”. However, they provide no population-level denominators and conflate expected irritation, redness and swelling with true microbial infections. The authors fail to note that severe cases are overrepresented in the literature precisely because they are unusual. The paper may be a useful clinical catalogue, but it is not an incidence study.
A Brief History of Safety
Tattooists and clinicians have long recognised infection risks in tattooing. In the late 1800s, some artists infamously spat into powdered ink and sucked the needles during the tattooing process. Meanwhile, London-based artists in the early 1900s, such as Alfred South, promoted “the most perfect antiseptic treatment, painless and absolutely harmless”, whilst Tom Riley warned: “Caution to Ladies and Gentlemen thinking of being tattooed – First see the work of two or three tattooists then make choice {sic}. See that a complete set of new needles are {sic} used at each sitting as well as antiseptics”. Some early tattooists even wore white coats to convey a clinical level of cleanliness.
Legal regulation, however, arrived much later. It was still legal to tattoo children in the UK until the Tattooing of Minors Act 1969. Some aristocratic families reportedly tattooed babies for identification – in case, for example, their children were hospitalised or kidnapped.
Modern Regulation
Mandatory licensing changed the landscape. Under the Local Government (Miscellaneous Provisions) Act 1982, tattoo studios need to be registered. More recently, there is the British Standard BS EN 17169:2020, which covers safe and hygienic practice, although not many councils use it as a benchmark. This standard covers workplace preparation, equipment sterilisation, PPE, client consultation and aftercare. It requires studio owners to implement a comprehensive hygiene protocol to protect clients and staff, and tattoo artists to provide evidence of continued professional development.
Wales now requires tattooists to complete and pass a regulated Level 2 Infection Prevention and Control Award. Requirements in England and Scotland are less specific. Barnet Council licenses my studio; their Code of Practice 13 details the specific requirements for tattooing activities, in addition to those laid down in the Regulations applicable to all special treatment licensed premises. It notes that tattoo artists who are unable to demonstrate hygiene competence may be asked to complete a Level 2 hygiene certificate.
Reducing the Risk
Infection risk can be reduced through:
Good personal hygiene (artist and client)
Effective cleaning
Separating clean and dirty materials
Correct sterilisation or disposable equipment
Artists must assess clients for skin issues (including rashes, moles and scarring), alcohol or drug use, and relevant health risks (e.g. allergies, immunosuppression, pregnancy). Artists must be vaccinated against Hepatitis B.
Tattoo stations should be treated as clinical areas. Equipment must be protected from contamination; inks must be decanted into disposable cups; distilled water used for dilution of ink and ‘green soap’ (a vegetable-oil-based surgical soap used in the tattoo industry) or for washing the needles between colours.
Dressings applied afterwards are usually transparent, self-adhesive, polyurethane film (known as second skin in the industry), similar to those used for burns and post-operative incisions, or cling film attached to the skin with surgical tape. Clear aftercare guidance should be provided verbally and in writing about how to care for the tattoo whilst it heals (no swimming, spa pools, sunbathing, perfumed soaps or scratching).
Unlicensed Tattooing
Although it is illegal to tattoo in unlicensed premises, this is rarely enforced. Anyone can buy machines and inks online and tattoo friends at home, often with limited knowledge of hygiene.
Inspections across the UK vary, with some councils inspecting only once when the studio opens, while others do so more regularly. Licensing rules differ widely outside the UK. Excellent tattoo studios can be found abroad, but so too can be deplorable hygiene. Getting a tattoo may be a more permanent souvenir of a fun holiday than a fridge magnet, but it can be risky, and alcohol and sunshine don’t help healing.
Final Thoughts
Tattooing in the UK, when performed by licensed professionals, carries a low risk of infection. I believe the demand for tattoos will grow, and I support nationally enforceable, pragmatic safety standards.
Takeaway messages:
Tattooing by licensed professionals in the UK is low risk
Nationally recognised training and regulation are likely to emerge
A tattoo is a controlled wound—so please, as I once observed, don’t let your dog lick it
Kondakala, Sandeep et al. Microbiology of tattoo-associated infections since 1820 The Lancet Microbe, Volume 6, Issue 4, 101005
Training For Aspiring Tattoo Artists:
After two years in the tattoo industry, I now work with licensed tattoo artist, TomCatTatt, to provide introductory training for aspiring tattoo artists, covering the basics in safety and hygiene, legislation and licensing, and an introduction to tattooing techniques. Contact me for more information: julieru13@hotmail.com.
The World Health Organisation (WHO) talks about it like this:
Antimicrobial Resistance (AMR) occurs when bacteria, viruses, fungi and parasites no longer respond to antimicrobial medicines. As a result of drug resistance, antibiotics and other antimicrobial medicines become ineffective and infections become difficult or impossible to treat, increasing the risk of disease spread, severe illness, disability and death.
I think it’s easy to forget that although AMR is a big part of the professional life of most Infection Control and microbiology professionals, even for other healthcare professionals it features less often, let alone for members of the public. It can be surprising therefore when you do go out and about, or even just talk to friends and family, to hear some of the ways that non infection professionals think about how AMR works and who it impacts.
Common misconceptions I hear when talking to people about AMR:
It’s the body that becomes resistant to antibiotics
I have never taken antibiotics so I cannot get a resistant infection
Antibiotics treat all types of infection
Antibiotics can be stopped when the symptoms stop
Only infected patients can transmit antimicrobial resistance
If you reflect on some of these myths, it’s actually pretty easy to understand how they come about. Most people are focused on themselves and act from a human centric point of view. Many people give little, if any, thought to the multitudes of living bacteria that co-exist in their bodies. Once you accept this as the starting point, most of these myths are actually based on pretty small mental leaps. If, however, you don’t switch your point of view before you start having conversations about AMR, you can unwittingly end up reinforcing the very misconceptions you were aiming to address.
One of the reasons that I think this post is timely right now, is that I am already seeing more posts linked to how we should not be putting artificial medications into our bodies, alongside the back lash against vaccines, and so it seems to me a good time to remember what a difference these, now common, medical interventions have made to the lives of individuals and public health in general.
Let’s start with a little bit of context
Hardly any of us will have living memory of life without access to antibiotics and what life was like in a world without vaccination. One way to really get a feel for the impact these common interventions have made is to look at the impact in the last 30 years on reducing child mortality (death). Even in this recent time period, massive progress has been made due to advances such as the rota virus vaccine, but also in getting more global access to antimicrobial therapy where it is most needed.
Public health is multi factorial, with impacts being cumulative and made by more than just one thing, so not all of these impacts are made by antibiotic and vaccine availability. Other steps to reduce death linked to infectious disease include everything from clean water and sewer systems to pasteurisation and other means of food safety controls. The impact of these combined approaches is massive, but as the UN sustainable development goals show us, those of us who are access to clean water are not actually in the majority and more is yet to be done to ensure equality of access.
To aim to undo some if not all of this century plus of progress is something I find pretty hard to process. If you’ll forgive the momentary indulgence, I have to state that I think the current anti-vaccine and general anti medical stance that is being seen within some groups and communities is ultimately an act of extreme privilege It’s a privilege to be able to choose not to access something that is readily available to you and not available to others. It is a privilege not to have to live first hand the consequences of what the alternative might hold. It’s also a privilege to be able to change your mind and choose to access something later. Thinking of things in this light doesn’t necessarily help with having conversations in a supportive and open way when some of the underlying thinking may be so different, but it may mean we can flip the dialogue from one of imposition to one about the power of choice, and supporting evidenced based decision making for all.
Where does AMR come into this?
There’s a big stat that everyone quotes about more people dying from AMR than cancer by 2050, with an estimated 10 million deaths. As a scientist, I get the need to quantify and use numbers, as a human being however, I find that numbers that are so big can just be off-putting. They are so large it can make us, as individuals, feel powerless to impact them.
For me, the reason this conversation is so important to have in the right way, and pitched to the right communities, is because if we are going through a period of global push back against the common interventions, such as vaccination, that have successfully reduced mortality and provided first line protection, then our final line of defence in terms of treatment is now even more vital. 2050 isn’t that far away, and we are already seeing consequences linked to more resistant organisms being identified in severe infections. Therefore, the time to be having conversations and really raising awareness to impact decision-making is now. Sadly, this is coinciding with a period of time when trust in healthcare professionals and science in general feels very low. Instead of being defeated by this, however, we need to use it a driver to really focus on how we can do it better.
One of the other reasons that AMR is both important and challenging to communicate is that it is always in constant flux. You can’t just learn about it and move on. The mechanisms change, the diagnostics change, and the interplay of all of these factors within the bacterial host interactions can make it even more complex and hard to engage with. To exemplify this, the figure below was something I saw posted on Bluesky and fell in love with, as I adore the fact that it lists all kinds of routes to AMR in a single image, thus capturing the complexity of what we’re dealing with.
That said, you don’t have to understand all or any of this image to understand the core of why AMR is going to be a problem moving forward. The main thing to take away from it is that AMR is complicated, and as a result you will hear many different messages linked to it, and those messages will continue to change as we learn more and the impacts are felt differently. As a result, it can then sound like we don’t know what we’re doing, or just end up really off putting, as there isn’t one clear message we are getting out there for people to cling onto. We, therefore, need to build this flexibility into messages and link around core themes rather than trying to talk in absolutes. Otherwise, we risk losing more of the public confidence than has already occurred.
What is being done nationally?
This year, a new version of the UKs National Action Plan for confronting AMR has been released and within it there is a strong focus on the acknowledged need to educate both members of the public and healthcare professionals on AMR.
There is also plenty in there about increasing equitable access to antimicrobials, the need to improve diagnostics to help support both diagnostic and antimicrobial stewardship, and something that pleased me greatly, a special mention of the role of the built environment in managing AMR.
The thing is, top-down approaches will only ever get us so far. At some point, those of us involved in all things infection also need to be consciously including some of these drivers in our own every day practice.
No one can do everything, but whether you are collaborating with industry, undertaking research, or working in clinical practice, we have to embed AMR based action into our encounters. Do you include an AMR slide into all of your teaching? No matter the audience? Do you take the moment when it comes up with friends and family to just talk about the fact that this issue exists? Can you free up some capacity and undertake some public engagement?
Recognising there is a need is not the same thing as addressing that need, and we also have to be there to hold strategic partners and organisations to account in order to make sure action happens. So, let’s consciously match that top-down approach with a bottom-up drive for change.
What resources are there to help talk about AMR to other professionals
Having talked a lot about the need to talk to other healthcare professionals and seeing so much about #WAAW this year, it does really feel progress is being made to support us all to do this better.
Those of you who are UK based have probably heard of and support the Antibiotic Guardian programme (https://antibioticguardian.com/). This programme has lots of resources and supports personal action by asking you make a specific pledge about what you will undertake linked to addressing AMR.
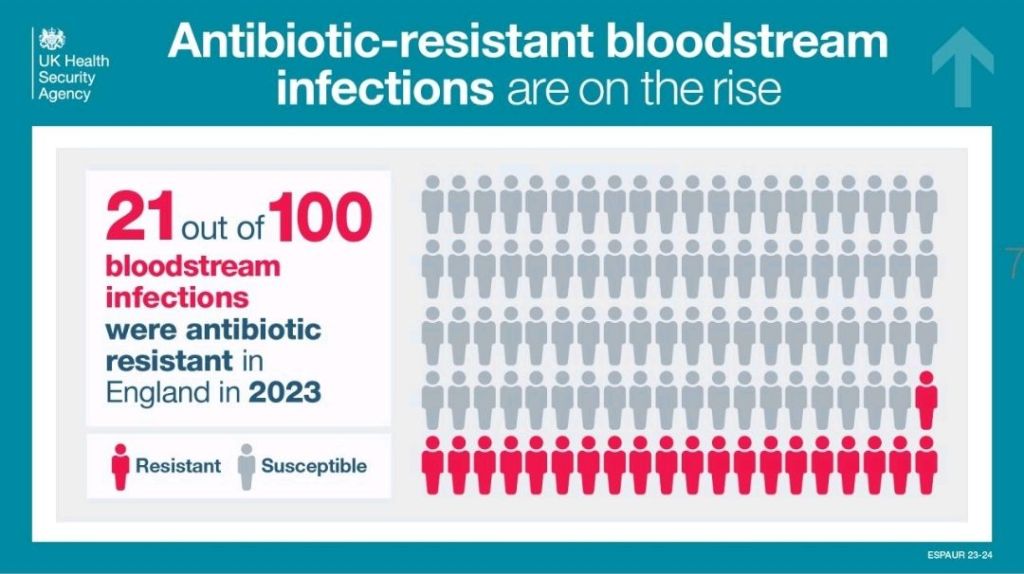
Every year, new infographics come out that talk about different aspects of AMR. Some of these, like the one above, link AMR into commonly known components of healthcare practice, such as hand hygiene, in order to support individuals to feel empowered to act. Others focus more on messaging about antibiotic courses, or as we heard a lot about at the FIS/HIS conference last week, things like IV to oral switches, and sending the right samples to enable a switch from broad to narrow spectrum antibiotics. There’s plenty of ones out there now that can be really useful to embed in talks or laminate and put up on walls. The UKHSA especially have recently released a lot for WAAW, and because there are so many, you can keep them on rotation so that they don’t just become invisible as people see them too frequently.
I’ve also been involved in creating various content this year, as have many others, including webinars and podcasts to explore some of the issues linked to AMR and provide different routes via which healthcare professionals can engage with information and CPD on this topic. I’ve included a link to just one of these below in case it’s of interest, but a quick internet search will provide you with all kinds of others.
The main thing to remember is that we all like to receive our learning in different ways, and so ensuring that we remember that when we’re designing our education strategies is one of the best ways to be impactful.
What resources are there to help talk about AMR to members of the public
The resources you might want to use linked to AMR will vary greatly based on your target audience. It’s important to remember that even if someone is a healthcare worker they are also a member of the public, and depending on their personal background or setting they work in, utilising content created for the general public may serve both purposes.
There is some really great video, podcast, infographic, blog, and other content aimed at public outreach on AMR. There’s even a musical called The Mold that Changed the World, about Fleming and Penicillin, as the first antibiotic.
There are lots of different entry points when you are thinking about content that might be appropriate, and you’re likely to go to different depths depending on whether you are doing a one off encounter or a more prolonged piece of relationship building.
The post that is linked to at the start of this article on AMR as a Super Wicked Problem may help with choosing your content. You may also want to consciously address some of the myths mentioned at the start or even start your conversation with the fact that many antibiotics actually started as products identified in nature, and so are not as far from natural compounds as may be frequently thought.
Some of you who have been reading this blog for a while will know how proud and passionate I am about The Nosocomial Project, which aims to use a science, technology, engineering, arts and mathematics (STEAM) approach to talk about infection and infection risks.
As part of this work, we organised a two part festival linked to AMR entitled Rise of the Resistance Festival. All of the content is split across YouTube and the website. I’ve included linked here in case any of it is useful in your own settings when you are looking for inspiration or planning content. The content covered in the festival included everything from a play aimed at pre-school aged children entitled Sock the Puppet, who is a hand puppet who is scared of germs, expert panels, comedy sets, and Klebsiella as a drag queen. I still have so much fun rediscovering this content, and I hope you’ll feel the same way.
I would make a plea that we all work together on this one to do some myth busting and get messages about AMR out there, but also find a way to get messages across that are entertaining/joyous and filled with hope for what we can achieve, rather than focusing on the horrors of what happens if we don’t get our act sorted. I think all of us, including healthcare professionals, have had our fill of trauma in the last few years. So, let’s focus on empowerment and positivity to make this change happen, rather than following in the footsteps of those who want a world of decisions driven by fear.
It has not been a great week for science, with many of us being concerned about how the presence of a vaccine denier on the successful ticket to the white house will impact public health initiatives and the quality of science communication in general. I’ve been thinking a lot about how we got here and how, even more than previously, embedding good science into mediums that are routinely accessed by the majority, will be crucial in ensuring the reach of accurate science communication when some of the more standard public health routes are bound to suffer in the coming years.
I think it will be a surprise to none of you that I am a bit of a lover of TV and movies, we’ve also covered a number of book reviews linked to this blog, and I like nothing better than snuggling down with a good book and a cup of Darjeeling. What does any of this have to do with anything? Infection, infection control, and science in general is a huge chunk of my every day, but this isn’t the case for everyone, or even most people. Many people are passive absorbers, meaning that they may not search out information but take on board when they encounter it when going about their lives. This means that the quality of what they encounter may be hugely variable, depending on how and where this happens. I’ve previously talked about the quality of the science in some of the books I enjoy, including the News Flesh series, as well as posting last week about how infection control is represented the Alien movies for Halloween. These are fun posts to do, but it made me think of the most popular movies that are linked to infection out there. How good is the science they represent? and by doing this better, could we support science literacy in general?
IMDB list of Top 25 Virus/Pandemic/Epidemic/Infection Movies
In order to think about this more detail I hit the Internet Movie Database (IMDB) which contains all kinds of lists, including a top 25 of Virus/Pandemic/Epidemic/Infection Movies (https://www.imdb.com/list/ls094715071/)
A Quiet Place (2018) (Girlymicro comment – I don’t know that this should count as it’s an alien invasion film)
Bird Box (2018) (Girlymicro comment – I don’t know that this should count as it’s an unknown enemy film that does not appear to be linked to infection)
Now, I have only seen 16/25 of these, Mr Girlymicro has seen 22/25, so between us we have most of these, so hopefully I’ll be to comment from a position of knowledge on a fair few of these. Before we even start however, as you can see from my commentary on this list, the poor science starts early during the classification of some of these as infection movies, even before we start to talk about the science content of the movie/show itself. Firstly, let’s look at the name of the list = Top 25 Virus/Pandemic/Epidemic/Infection Movies and how it related to the actual definition.
An increase, often sudden, in the number of cases of a disease above what is normally expected in a specific population and area.
An outbreak, which carries the same definition as an epidemic, but is often used for a more limited geographic area.
The CDC suggests epidemics occur when an agent and susceptible hosts are present in adequate numbers, and the agent can be effectively conveyed from a source to the susceptible hosts. Whereas a pandemic refers to an epidemic that has spread over several countries or continents, usually affecting a large number of people. The starting epidemic is usually due to a combination of factors including:
A recent increase in amount or virulence of the agent,
The recent introduction of the agent into a setting where it has not been before,
An enhanced mode of transmission so that more susceptible persons are exposed,
A change in the susceptibility of the host response to the agent, and/or
Factors that increase host exposure or involve introduction through new portals of entry
So you can see from the above that a number of movies on this list don’t actually count under the terms linked with to the title. Some of them are alien invasion, some of them are climate change related, and one is even on the topic of bioremediation. Yet there they are on the list.
For some of the others, I’ve already covered their concept during my Zombie post, so I’m not going to go through these in this blog, but focus instead on the ones that fulfill the epidemic based criteria. That said, give me a shout if you’d like a more in-depth zombie comparison post as Train to Busan is an awesome movie, and I’ll accept any excuse to re-watch it.
Let’s start at the very beginning
The first film on the list is Outbreak, a film that came out in 1995, with a description of ‘A team of Army doctors struggle to find a cure for the deadly Motaba virus that was transported from Africa to North America by a white-headed Capuchin monkey and is now spreading quickly throughout a small California town.’
This movie has an amazing cast, but I have to say I don’t want any of them in my team if it came to trying to lock down a high risk infection from an unknown source (vector). In terms of the escape monkey component. You’d think that it is far fetched, and if you’d asked me yesterday I would have said just that, but just today on BBC News there was a story on 43 escaped monkeys from a research lab in the US. So far fetched it may be, but not unheard of, in the case of vector escape.
Even if the vector component may not be quite as unlikely as I’d previously thought, I’d like to say that the rest of the practice in this is highly suspect at times. That said, I do have to admit, that I once went to a talk by a scientist who was looking for viral transmission sources of haemorrhagic fevers in Africa. They showed pictures of the table where they performed autopsies on found deceased animals in the jungle, under the same canopy as the table where they then sat down for dinner. So, as much as the way that high consequence infectious diseases (Ebola etc) are not portrayed as accurately as I’d like, maybe this is a movie of its time, as was that lecture. I really want to enjoy this movie, as it so defined how many of us had our first introduction to outbreaks and what they could mean, but almost 30 years on I don’t think I could recommend the scientific accuracy it portrays. The fact that this is still the top rated movie does not bode well for our scientific literacy hopes.
What a difference a decade makes
Almost 15 years after Outbreak, Contagion was released in 2011. This was the first of the infection movies on this list that I saw after I’d started working within Infection Prevention and Control. Contagion is described as ‘Healthcare professionals, government officials and everyday people find themselves in the midst of a pandemic as the CDC works to find a cure.’ I remember going to see this with a scientist friend and whooping out loud at the explanation of an R0, it gave me so much joy I was shushed by someone else in the cinema, to my ongoing shame.
The CDC defines an R0 as ‘The basic reproduction number (R 0), also called the basic reproduction ratio or rate or the basic reproductive rate, is an epidemiological metric used to describe the contagiousness or transmissibility of infectious agents.’ So, see if you share my joy at how the movie explains what this is, in a way that is so much more approachable than the CDC definition:
This film is not perfect, I clearly remember losing my mind about the glove use at one point, and SPOILER ALERT, it was that poor glove use that meant I was OK with one of the characters dying, but the underlying science is well explained and some of the approaches to containment and vaccination are definitely well routed in evidence. The differences in the quality of embedded science between Outbreak and Contagion are highly noticeable. Part of me wonders if some of the drivers for this heightened quality is linked to awareness of the topic due to the 2009 Swine Flu pandemic, or whether this was part of a wider shift towards improved factual grounding in these kinds of movies.
When talking to Mr Girlymicro about this movie, whilst writing this post, he has pointed out that despite my enjoyment he found it an act of ultimate depression which he will not be watching again, and that was when he watched it before the pandemic. It may therefore be, something that triggered my science joy may, in fact, be too depressing or triggering for other reasons to equate to true enjoyment for the general public. This may be an example of something that could risk being dis-engaging by being too close to the truth, despite being second on the IMDB list. Especially in a post pandemic world, this is a line that may prove difficult to walk and prove to be a barrier to movies and TV on this topic being commissioned in the short to medium term.
A completely different movie about primates
Still on viruses and re-visiting our primate theme from Outbreak comes Rise of the Planet of the Apes , which was also a 2011 release. It came out the same year as Contagion, and in the same discussion as Mr Girlymicro stated he would not re-watch that movie, for all the accuracy of it’s science, he would watch Rise repeatedly, and I can testify that in fact he has. Rise has the following description ‘A substance designed to help the brain repair itself gives advanced intelligence to a chimpanzee who leads an ape uprising.’ This is a really interesting addition to the category, as the pandemic aspects of it are mainly actually addressed in the closing credits which demonstrate how a pandemic can spread across the globe, with the film very much focused on the human (and primate) story behind the build up.
This film utilises a viral vector to try to address and revert brain abnormalities linked to Alzheimer’s, with a scientist desperately trying to find a cure for his father, whilst undertaking clinical trials on primates. Now, the clinical trial aspects of this film could not be further from the reality, and any scientist caught undertaking clinical trials and then sneaking the medication to treat their father would at best be fired and at worst been imprisoned. Somehow, because of the focus on the relationships rather than the science, the bad science in this movie bothers me significantly less than that represented in Outbreak, possibly because it feels deliberately portrayed as more like science fiction than science fact. There are some aspects of science to this one that I find interesting and like. The idea of a vaccine or medication behaving differently across species barriers is something that is interesting and could be deeply seated in evidence based plot-lines. I am aware, in this age of post truth and vaccine denial, having a film that focuses on how a vaccine or treatment could end life as we know it may not play into the goals I’m wishing to achieve using popular culture.
Let’s not forget about fungi
In recent years there’s been a rise in the quality of TV and the amount of choice has exploded, especially on streaming and other services. The switch to being able to film big budget TV over shorter film equivalents has provided storytellers with the capacity to really explore bigger and more complex tales that may not have been possible in under 3 hours.
This is last and most recent entry onto the IMDB list and is also the only TV entrant. It is our first step away from the world of viruses, into the world of mycology and all things fungal. The Last of Us came out in 2023, although it’s based on a computer game that was released in 2013. The series is set ‘after a global pandemic destroys civilization, a hardened survivor takes charge of a 14-year-old girl who may be humanity’s last hope.’ This is therefore a great combination of the way different mediums impact popular culture. The plot asks big questions about how far you would go to get a cure for the world, how much is one persons life versus the possible saving of mankind. It’s a real homage to the power that vaccination could hold to impact the world, and how when one isn’t available how desperately people might act in the search for a cure. This is the only entry on the list that came about post pandemic, and I think it is because of that (despite being a parallel to the game) that really resonates on where that desperation comes from, and despite the current vaccine back lash, shows how different outcomes could be.
The very first scenes of the series are a flashback interview from before the pandemic where a scientist talks about what they think the next bit pandemic will be, and I have to say the whole scene brings me unacceptable levels of science joy.
Anyway, this one played so much into my particular ball park that I worked with Liv Gaskill at ID Transmission on a series of articles that talked about the science behind both the Last of Us computer game and the resulting TV series, which pretty closely followed the same plot. This four part series was a real joy to be involved with and so I’m hoping that you might enjoy them too:
I wonder if fungi will be increasingly represented in this genre a) due to the success of The Last of Us and b) as viruses feel a little too close to home these days and so the fungal world might feel like a safer sand box to play around in. This could provide a safe way to have accurate science portrayal, alongside entertainment, as the real prospect of a fungal pandemic is thankfully pretty small.
A shocking oversight
We’ve reached the end of the list, but not the end of the blog post as I want to address an appalling over sight on the IMDB list, and that is the omission of The Strain on the list. This is also a TV series, where season 1 was released in 2014, covered a series of 3 books, and ran for 4 seasons. The series is described as ‘A mysterious viral outbreak with hallmarks of an ancient and evil strain of vampirism ravages the city of New York.’
The strain – episode one, season one
There are many reasons why I love this series (and at some point I should do a vampirism and infection blog to include things like Ultraviolet) is that some of the main characters are epidemiologists linked to the CDC and so some of the science exposition as part of the job based discussions is very pleasing. The other reason I like this series is there is a definite bait and switch, in terms of the causative agent, with all the initial dialogue being linked to your standard viral outbreak, with a gradual reveal that the culprit is actually a parasite. This adds a layer of interest as the approaches to dealing with transmission really start to reflect this, and provide an interesting change as the characters are also forced to pivot and discuss the differences. So, the use of a non-viral infection is not as unique as some of the coverage of The Last of Us may imply. That said, the general science outside of the epidemiology in this definitely becomes more to serve the horror plot than feasibility as time progresses.
Where are the bacteria?
You’ve survived ~3000 words of outbreak talk, covering viruses, fungi and even parasites. You may however be struck by the lack of bacterial cause in any of these listings. I’ve been thinking about this whilst I’ve been writing this blog and I’ve come up with a few thoughts as to why this might be the case:
Too close to home – many people have experienced bacterial infections themselves in their loved ones, sometimes with tragic consequences. It may be hard to therefore suspend belief enough to enjoy the offering. I wonder if this will be true to an extent for viruses now, or whether popular culture will be a safe way to explore collective trauma linked to the pandemic
Too slow – one of the features of many of the scenarios in these movies and shows is that the impact to fast and significant. This an important aspect of making events have real risk and in raising tensions. If accurately portrayed bacterial infections may be too slow in their impact OR the deterioration is so quick there is insufficient time for viewer engagement
Not dramatic enough – bacterial transmission (as described by R0) are not going to be as dramatic as their viral counterparts, so if you subscribe to ‘go big or go home’ this transmission route is probably not the one to drive a sprawling plot-line forward
Too commonly encountered – there are 101 medical shows which have bacterial infections and their consequences featured and so they may be too close to a different genre
The science is pretty hard to get right – as people are more familiar with the topic the less story flexibility there is and the greater the need to not be too jarring for those you are trying to engage. At least in the UK, many people will have been taught about Typhoid Mary and the John Snow Cholera outbreak, and so may have some familiarity. It may also be that these also make people think of the past, and this is not the feel many of these properties are trying to evoke.
So maybe bacteria are a harder sell, although I’d be intrigued to throw a little antibiotic resistance into the mix, or some bacterial toxin related drama and then see what cool things could be done as a result. Maybe that might be my future project 🙂 Let me know if you think that there is a bacterial based film/series that I’ve missed.
It’s Halloween weekend, and in previous years I’ve talked about all things Zombie and infection transmission. This year, though, I thought we talked about something a little different, infection control precautions through the lens of the Alien movie series. Most importantly, I’m going to talk about those initial interactions with the unknown that we frequently see in both these movies and in infection prevention and control (IPC), and whether we too would open the door when someone presents at the air lock?
Spoiler warning! This post is going to mention things that happen in various Alien movies. If you haven’t seen them it may, therefore, contain spoilers – the best way to deal with this oversight in your viewing (if you are concerned) is to just get out there and watch them as Alien is the same age as me 😁
This post was inspired by watching Alien Romulus again this weekend, which, if you haven’t seen it is the best Alien movie in forever.
In preparation for the cinema release I also did a re-watch of a number of the movies in the franchise. Just in case you are less familiar, and inspired to do the same, the list includes a variety of films in different sub-genres as listed below:
Whilst watching these I was struck by a number of moments that made me think about behaviours during the pandemic, but also tales of heard of some activities that occurred during the response to the Ebola pandemic and other high risk clinical settings. Not all of these moments would have been massively out of place, in terms of parallels with these films, and demonstrate that both risk assessment and clarity of thinking can be impacted and lead to responses outside of what would be normally expected.
The thing to remember is that there are usually protocols for just about everything, so most of the decision-making should occur and have been thought out long before the situation ever arises. The problems are almost always linked to human factors in the way we respond to stress and unexpected situations, and when the protocols appear to go out the window. So, just like every character and every space ship in the Alien franchise has a protocol for how to behave when they encounter new life, strange situations or sick crew members, every healthcare facility also has protocols to help deal with illnesses we see less often or that get issued when new diseases are encountered. Healthcare facilities may not have air locks, but they do have labs and isolation facilities, so the parallels may be more present than you’d imagine.
Infection is not always obvious
One of the first themes that recurs throughout all the movies is that infection is not always obvious, either to those on the other side of the air lock, or to the individuals outside waiting to come in. Infection with the parasite sometimes occurs when the stars of our show are unconscious, be that due to trauma or medical interventions, and so they are unaware of the Facehugger on character action that has occurred.
In terms of IPC the same if frequently true, both for viruses and bacteria. Some viruses have what is known as a pre-symptomatic phase, where you are infectious to others before you even know you are sick. This was a big problem in the early stages of the SARS CoV2 pandemic. Even for bacteria, when we talk about antibiotic resistant bacteria, most people are colonised and have the potential to act as silent sources without even knowing it, with only small numbers going on to develop infections.
The truth is not always apparent
Even when an individual knows that something has happened, and are aware of their close encounter with Alien kind, the truth of their scenario may still not be apparent to either them or to others. If you look at the Facehugger situation, surely once the terrifying creature has dropped off without apparent poor consequences, then everyone breaths a sign of relief and is grateful for the near miss, not knowing that this is only the beginning. When you combine this with the fact that some people will determine this to be a low risk event and therefore not want to disclose, as they are aware of the inconvenience that will result, you end up in situations where not all the information is available.
This can also be true in real life clinical situations. Patients may not know they have been exposed. Patients may also present with symptoms that they haven’t recognised as significant, or that they have risk assessed themselves and decided they aren’t concerned about and so don’t disclose. This can happen more easily they you think, especially at the start of something, where patients don’t feel particularly unwell, or they just have a couple of vesicles/small rash. In the latter stages, when patients are presenting because they feel unwell, they may be confused or not always able to accurately disclose what’s happened. Occasionally, this may be a deliberate attempt to withhold personal details, but most often it’s because they are rightly focussed on how they are feeling in the moment. Plus, if you asked me to accurately recall everyone I met and everything I ate a week ago, I’m not sure I could, even when well.
By the time you realise the condition is a threat it may already be a risk/out of control
One of the consistent themes across all of the movies is that situations get out of control before anyone truly understands the situation and the risks. It’s only when the person that you breached protocol for suddenly starts to writhe and the horror stands before you in all its glory do you truly understand the implications of the decisions you’ve made. At that point you are trapped in your glass med bay with a growing Alien and your self recriminations are not going to save your life.
This one is a rather more dramatic version of some of the conversations that happen amongst healthcare workers when you phone to give results and have conversations about whether patients had been in the right precautions and the staff member was wearing the right personal protective equipment (PPE). There have definitely been times when staff have made a risk assessment and not followed the protocols about what PPE to wear and have then responded to these phone calls with ‘what can you do?’ in relation to the exposure. Sadly, in some cases there is nothing that can be done once the guidance has been bypassed but to wait and see, which is the reason for the guidance in the first place. Fortunately, for most scenario’s in the real world, the consequence isn’t bloody horror, death and an alien threat to mankind.
Risk assessment is linked to risk management
One of the reasons that protocols are in place in the Alien movies is that someone, somewhere, has obviously recognised the risk of infection in a small contained community where everyone interacts and lives on top of each other. Even in Aliens, when you’re talking about somewhere the size of a colony, this principle stands. This is because you are unlikely to be able to access a clinical trial on a mining ship, or develop a novel antiviral on terraforming mission, even if what you’re importing is a more traditional style of infection, versus an Alien parasite. The extent of the risk mitigations needed will always align to the risk itself. If you are concerned about an introducing something that is untreatable, then your measures are going to be much more extreme than if your infection is likely to just mean someone goes to bed and takes paracetamol for a weekend. If you can’t treat, then prevention is your only option. After 9 movies there doesn’t appear to be a Xenomorph (Alien) cure and so measures taken to prevent allowing one into your space need to match the risk they present.
This approach is definitely seen in response to infection in IPC. If you have a condition that spreads easily, rapidly and can be incapacitating for a period (i.e. norovirus) then you will use a different set of precautions to those that you use to manage something which may not be as transmittable but is untreatable or has life threatening consequences such as a haemorrhagic fever. Having conversations and being open with people about the risks of getting things wrong and ensuring that individuals understand why responses are different in different circumstances are a key requirement for people working in IPC, and something I think we should all endeavour to do better at. I think the days of asking people to blindly follow protocols should probably be behind us, as I think the Alien movies demonstrate that if people don’t get the why, they often ignore some of the core components based on external drivers
So, what lessons can we learn?
Beware of acting on incomplete information
Decisions are consistently made in these movies based on incomplete information, which leads them to underestimate both risk and consequences. A great example of this is the way people use information related to the black goo, especially in Alien Romulus, maybe don’t inject yourself with a substance that doesn’t have a proper name let alone a full data set for you to understand what it does. The other thing is that information is often treated as static, and so there is very little rapid inclusion of new info, rather than being mindful of an iterative response to new data, so help constantly inform and improve your risk assessment. It’s always worth being conscious of when is enough is enough when it comes to information and decision making.
Emotions get in the way of logic
During the movie Covenant, the entire crew is made up of couples. I get this in terms of colonisation, but in terms of good decision making, and in relation to risk this is just a one way route to bad outcomes. There’s a reason that in a certain Zombie series husbands have kept their zombie wives locked in basements rather than removing the risk to them and others. There’s a reason medical professionals should not manage their loved ones. Emotions interfere with logic, and there is no way under this setting you are managing to make decisions without your emotions getting in the way. It’s a reminder that if we become aware that we are in an emotive place, it may be the time to step away and take a deep breath, before making that judgement call or even tap out entirely and allow someone more removed to take our place.
The contrast between human emotional decision making and evidence based decision making, usually undertaken by the android cast, is beautifully explored during Romulus via Andys story arch and is one of the highlights for me in terms of enjoyment.
Science doesn’t change based on how much you wish the outcome to be different
One of the reasons that emotional involvement in decision making can be so challenging is that it can interfere with perspective and accurate interpretation of risk, thus impacting risk perception. Sadly the truth that wishing does not impact outcomes is hard to argue with, but it is human to try to persuade ourselves we have more control and ability to influence the outcome than we do. Under stress, our natural tendencies towards pessimism or optimism are definitely amplified. All of this means that when there is someone at the door banging and begging to be admitted, it is easy to persuade ourselves there is a) enough time to manage to open the door safely and b) the consequences of opening said door will not be as bad as we fear. Emotions don’t change outcomes but we are almost programmed to hope that they can.
An individual will always want to be the 1 in a million
The reason someone opens the door is the same reason that when one character looks at another and utters the fateful and true words ‘it’s too late’, and it almost definitely is, neither one acts before everything gets out of control. Humans are not good at dealing with numbers and risk when they are actively involved in the situation. One of the reasons we aren’t in that we throw sentences around saying it is a 1/million chance. We, as humans, have a tendency to focus the fact that, although it is a long shot, there is a chance that things can go your way. Sadly, as someone who has experienced the opposite, where my sister died in a 1/10,000 pregnancy, someone always need to be the one. The stats work both ways, whereas most of us survive in the world by only focussing on one side of the equation. This therefore impacts our capacity to evaluate any risk in situations we are involved with. Somebody always bears the cost and few of us can bear the vulnerability of acknowledging that that somebody could be us.
The people with the most experience are not always the ones making the decisions
One of the other main themes in these movies is that decisions, when not being made by friend and loved ones, are often being made by people in positions of power, not necessarily based on knowledge or even accepting of prior experience. This works well or not so well based on how well they listen to those who do have the information to help improve their decision making. Chains of command, especially in high stakes scenarios, are not necessarily bad, as we’ve already talked about the risks linked to emotional decision making, but so much depends on how well they work and how they place value on evidence based choices rather than hierarchy.
The other theme here is the trusting of unknown sources, especially ones with no evidence of expertise, over those who have either lived experience or expertise. I think this one resonates a lot right now, when there are so many sources of misinformation out there, and so many conspiracy theories that rely on speculation and rumour. Fact checking is key, be that on a space ship or deciding on your vaccination options.
Not everyone has the same thought processes
One of the other reasons decision making goes astray in these movies is because those involved in that decision making often have undisclosed values, beliefs or drivers that are impacting their choices, and this process is not always obvious to those others involved. This is true from androids that may or may not be obviously androids and who will have programmed ‘primary directive’, as well those working for the corporation. This is interesting as they often have more complete information than the others involved, as well as seeing the situation through a different lens because of how they view the world. This means that they can see others as disposable or views risks different, as they have a set of criteria that they wish to achieve which is more than just survival. Although in clinical life the juxtaposition is rarely so extreme, the challenge of reaching alignment when people come with different world views can definitely impact shared decision making.
Smart people can do stupid things
Having said all of that, smart people can in general do stupid things, even without all of these complications. Even when the experts are the ones making the decisions they can still make the wrong ones, especially when tired, stressed, or lacking all the information. This is the reason why protocols are key, drawn up and decided upon when all of the confounders to good decision making are not present.
You need to follow the standard operation procedures
In the end this entire post has been a very very long way of saying ‘JUST FOLLOW THE SOP!’
Many of these movies but have been much shorter with a much reduced body count, if those involved had just followed the pre-established procedures laid down for their safety. Obviously, we don’t have so many Xenomorphs as a daily risk factor in healthcare, but the same is true for us. SOPs are rarely there for the sake of it, they are there to support decision making so that in times of stress or information overload, you are not having to seek extra information to support good decision making, you have it freely pre-digested and available to you. So the next time you think twice about donning that PPE or the closing that isolation room door, ask yourself ‘would you open the airlock door?’, think twice and do the right thing.
And now for something completely different
Finally, because this is something that has amused me whilst watching these films and is probably not something that I can talk about in general down the pub. The computer in the Alien movies is usually referred to as Muthur, pronounced Mother. I just want to share my joy that the analysis software that is used to help analyse 16S rDNA runs, to give you microbiome analysis i.e. tell you what bacteria are present in your sample, is called Mothur, and also pronounced Mother. I’m sure the two things have nothing to do with each other, but allow me my scientific joy that something which was so ‘other world’ when it came out to me as a scientist has the same name as something imagined from ‘another world’.
Also, if anyone needs a science advisor on their next project, give me a shout as this post has brought me much joy and I think I may have missed my calling 🙂