You may have noticed that I’ve been a little poor at keeping up with the Girlymicrobiologist site admin, and missing the odd weekly blog post. This isn’t because I’ve been slacking, honest, it’s more because I may have become a little distracted by a new project. I promise to get back on top of things soon, but in the meantime I thought I owed you an update.
Many of you have been kind enough to support last years project, which was a book aimed at supporting people to engage with research and research degrees, and I couldn’t be more grateful for your cheer leading. This new project, however, in the words of Monty Python could be described as ‘and now for something completely different’. It couldn’t be further from a book about academic study. This one is all about something else I love passionately, movies and TV.
I finished and launched the last book last October, and to be honest it hadn’t occurred to me, prior to letting it go into the wild, that I would write anything else till my retirement – when I’m planning to write some pathology based murder mysteries. It was never the plan to do something again, at least so soon. Frankly though, my brain tends to disrupt all my best laid plans, and ideas come meaning I just can’t help myself but get swept up. I’m blaming Ian McKellen inspiring me to ‘practice any art’.
Despite having no plans to do more, I have to say that I really enjoyed writing the first book, and I found the process of being able to write in a different way very fulfilling. I love writing this blog, and the first book is based on a lot of the pieces I have written for here, but it was nice to see them come together and take on a new and different life of their own. I also enjoyed mixing up the writing of something on a single theme with writing blogs on different topics for here, although I did rely a lot on Dr Claire Walker bringing together many guest blogs to allow me some writing time. It was lovely to see what those guest blogs brought to the site, and I really enjoyed seeing how including those voices really makes this feel even more like a community space. Without realising it, I think I caught ‘the bug’. Now, I’ve always enjoyed writing, this is my happy space, but I had never seen myself as an author, having held a book I’d written in my hands though, I can see how it could become a little addictive.
As I was sitting watching horror movies as part of my post release recovery, and researching for my 2025 Halloween post, I suddenly realised what I’d like to do next. I really wanted to write about some duel loves of mine, movies and TV plus infection.
Without any expectation of writing another book, all of a sudden I had a structure in my mind, and Don’t Open That Door had began…
You all know how much I am a movie and TV buff, everything from guilty pleasure reality TV, like The Secret Lives of Mormon Wives, to documentaries, and all genre of film (with the exception of torture porn horror movies, I’m a Blumhouse girlie). Whilst enjoying some down time with Mr Girlymicro, I realised how widely infection is featured in all kinds of different genera settings, some of it was actually pretty good, whilst some of it was really poor. So the first step was to do a whole bunch of research about what kind of examples were out there, by hitting up a bunch of different lists that have been collated by others, internet searches, and sourcing opinions from my movie loving friends. All of which led to the creation of a list of 138 options that needed a review to see if if they were actually linked to infection, and if they were infection based….was the infection content any good.
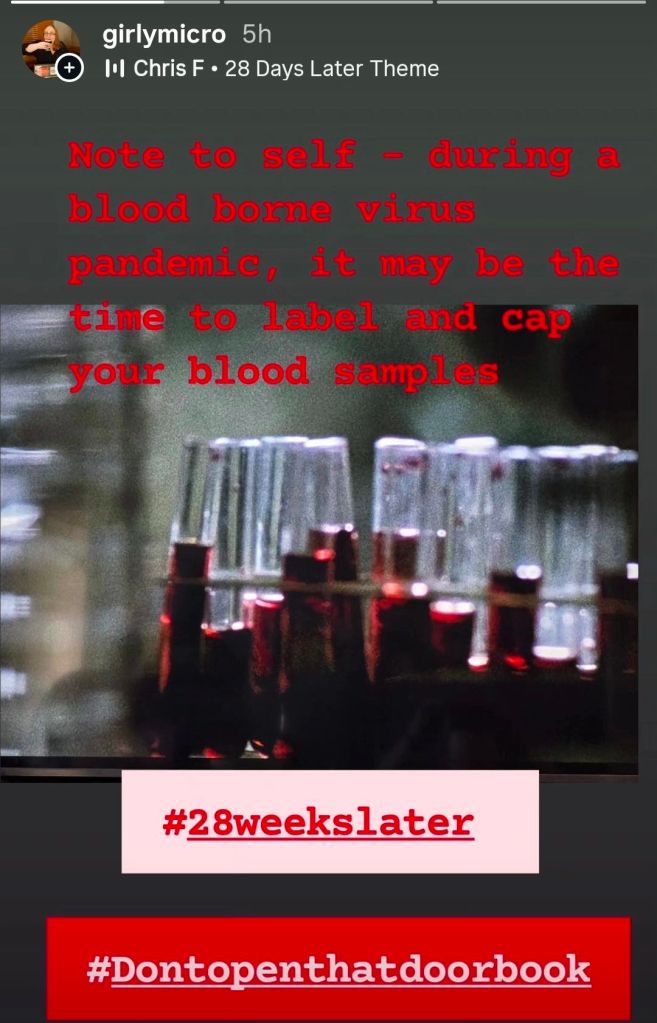
If you follow me (Girlymicro) on Instagram, you will have probably seen a number of stories that I’ve posted recently linked to movies I’ve been watching with some Infection Prevention and Control/micro commentary:
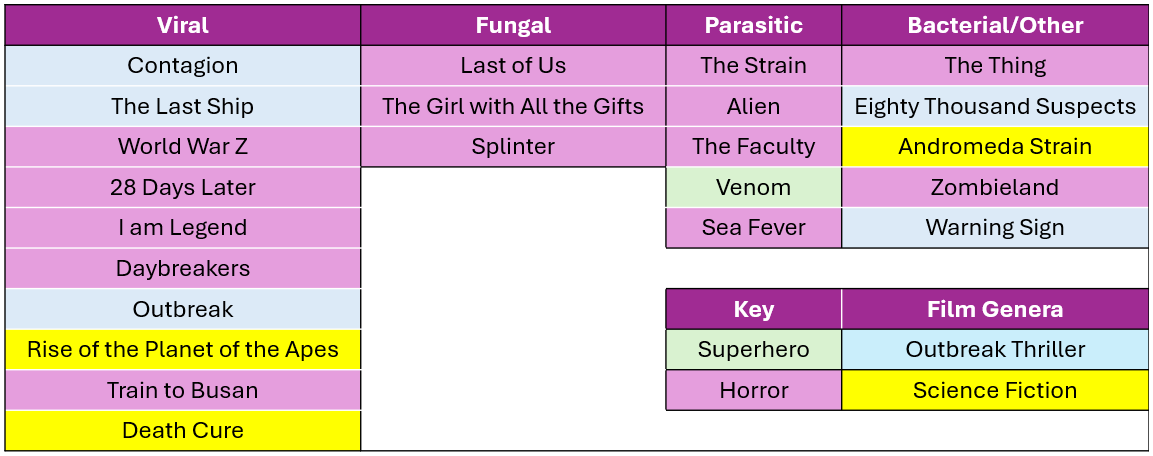
These have come about whilst I’ve been watching the 138 films/series with Mr Girlymicro to decide which ones make the cut to be included. I’ve watched some awesome films, some like Sinners, weren’t based on infection so couldn’t be included. I have also watched some truly bad movies, I even gave Resident Evil another go, and have spared you all by making sure that it is not included on the list. One of the considerations was that, even if the science wasn’t dreadful, I haven’t included anything that I or Rotten Tomatoes include as being truly horrible. I’m not just saving you on this, but also myself, as I’m having to watch included examples many times as part of the writing. I also felt it was really important to cover infections linked to viral, fungal, parasitic, and bacterial causes, just because they behave so differently and the interventions needed are so different. So the final list for inclusion involves movies and TV series that sit across infectious agents, although viruses are more represented than any other cause.
There are plenty of horror movies on the list, purely because they represent A LOT of the infection genera, but I was surprised at how many options there were outside of horror movies. I also tried to mix up certifications where I could, so that there are some options that everyone might enjoy.
Not everything could be included however, and there were also some exclusion criteria that impacted what I could include. Exclusion criteria included factors such as availability – no point including things that people can’t access, language options – I sadly only speak English so it needed at least English subtitles, and most importantly not based on real life events – this is about fiction.
For inclusion examples also needed to have infection as a central theme. This meant that health dramas could not be included as they only feature infection in some episodes, but at some point I do really want to write something that compares different medical dramas (House, New Amsterdam, Holby City etc) and maybe do a ranking scale….let me know if you think that would be a fun blog post.
Image credit The Red Dress
The reason it felt timely to talk about this today, is that the Biomedical Scientist magazine has been kind enough to do a whole feature on what the new book will look like, with a bit more detail, and some examples of what chapters will look like. It dropped on the 27th March and you can check it out the link here: https://thebiomedicalscientist.net/2026/03/24/infections-films. Also, how awesome is the art work they’ve done, can’t say enough how awesome The Red Dress are.
Whilst writing the article for the Biomedical Scientist and watching the example movies, I couldn’t happen but note how many weird and wonderful things are included as part of the science representation. Things that in my scientific career I rarely if ever encounter, but seem to crop up time and time again in Hollywood depictions of scientific life. I’m collating these for one of the final chapters in the book called ‘Science House of Horrors’ as I find them a bit fascinating. I’ve included some of the ones in the Biomedical Scientist article that I noticed, as well as those sent through as responses from social media, but I’d love to know if you have any others that I should include.
There are other opportunities to get involved though, I have 23 films and series examples, but there is room in the book to cover 25. I’m really keen to get other examples that include fungi, but if there is just something brilliant I haven’t included please let me know. There will also be a chapter called ‘Hall of Fame’ that covers both amazing movies that just don’t have enough infection in them to be included, or ones that were great but not quite as good an example of an infection characteristic as the ones already included. There is also the ‘Hall of Shame’ for examples, such as the TV series The Rain and Resident Evil, where the science is so bad that it is note worthy in itself.
Anyone who drops me an email to elaine@girlymicrobiologist.com and inputs into the House of Horrors, volunteers film examples I’ve missed, or suggests contenders for the ‘Hall of Fame’ or ‘Hall of Shame’, will get their name included in the list of contributors at the back of the book. Science takes a village, so does pulling together a book, and I’m really keen that this feels like it comes from our community. I hope you enjoy the article and I can’t wait to hear from you about your suggestions.
It’s Halloween weekend, and in previous years I’ve talked about all things Zombie and infection transmission. This year, though, I thought we talked about something a little different, infection control precautions through the lens of the Alien movie series. Most importantly, I’m going to talk about those initial interactions with the unknown that we frequently see in both these movies and in infection prevention and control (IPC), and whether we too would open the door when someone presents at the air lock?
Spoiler warning! This post is going to mention things that happen in various Alien movies. If you haven’t seen them it may, therefore, contain spoilers – the best way to deal with this oversight in your viewing (if you are concerned) is to just get out there and watch them as Alien is the same age as me 😁
This post was inspired by watching Alien Romulus again this weekend, which, if you haven’t seen it is the best Alien movie in forever.
In preparation for the cinema release I also did a re-watch of a number of the movies in the franchise. Just in case you are less familiar, and inspired to do the same, the list includes a variety of films in different sub-genres as listed below:
Whilst watching these I was struck by a number of moments that made me think about behaviours during the pandemic, but also tales of heard of some activities that occurred during the response to the Ebola pandemic and other high risk clinical settings. Not all of these moments would have been massively out of place, in terms of parallels with these films, and demonstrate that both risk assessment and clarity of thinking can be impacted and lead to responses outside of what would be normally expected.
The thing to remember is that there are usually protocols for just about everything, so most of the decision-making should occur and have been thought out long before the situation ever arises. The problems are almost always linked to human factors in the way we respond to stress and unexpected situations, and when the protocols appear to go out the window. So, just like every character and every space ship in the Alien franchise has a protocol for how to behave when they encounter new life, strange situations or sick crew members, every healthcare facility also has protocols to help deal with illnesses we see less often or that get issued when new diseases are encountered. Healthcare facilities may not have air locks, but they do have labs and isolation facilities, so the parallels may be more present than you’d imagine.
Infection is not always obvious
One of the first themes that recurs throughout all the movies is that infection is not always obvious, either to those on the other side of the air lock, or to the individuals outside waiting to come in. Infection with the parasite sometimes occurs when the stars of our show are unconscious, be that due to trauma or medical interventions, and so they are unaware of the Facehugger on character action that has occurred.
In terms of IPC the same if frequently true, both for viruses and bacteria. Some viruses have what is known as a pre-symptomatic phase, where you are infectious to others before you even know you are sick. This was a big problem in the early stages of the SARS CoV2 pandemic. Even for bacteria, when we talk about antibiotic resistant bacteria, most people are colonised and have the potential to act as silent sources without even knowing it, with only small numbers going on to develop infections.
The truth is not always apparent
Even when an individual knows that something has happened, and are aware of their close encounter with Alien kind, the truth of their scenario may still not be apparent to either them or to others. If you look at the Facehugger situation, surely once the terrifying creature has dropped off without apparent poor consequences, then everyone breaths a sign of relief and is grateful for the near miss, not knowing that this is only the beginning. When you combine this with the fact that some people will determine this to be a low risk event and therefore not want to disclose, as they are aware of the inconvenience that will result, you end up in situations where not all the information is available.
This can also be true in real life clinical situations. Patients may not know they have been exposed. Patients may also present with symptoms that they haven’t recognised as significant, or that they have risk assessed themselves and decided they aren’t concerned about and so don’t disclose. This can happen more easily they you think, especially at the start of something, where patients don’t feel particularly unwell, or they just have a couple of vesicles/small rash. In the latter stages, when patients are presenting because they feel unwell, they may be confused or not always able to accurately disclose what’s happened. Occasionally, this may be a deliberate attempt to withhold personal details, but most often it’s because they are rightly focussed on how they are feeling in the moment. Plus, if you asked me to accurately recall everyone I met and everything I ate a week ago, I’m not sure I could, even when well.
By the time you realise the condition is a threat it may already be a risk/out of control
One of the consistent themes across all of the movies is that situations get out of control before anyone truly understands the situation and the risks. It’s only when the person that you breached protocol for suddenly starts to writhe and the horror stands before you in all its glory do you truly understand the implications of the decisions you’ve made. At that point you are trapped in your glass med bay with a growing Alien and your self recriminations are not going to save your life.
This one is a rather more dramatic version of some of the conversations that happen amongst healthcare workers when you phone to give results and have conversations about whether patients had been in the right precautions and the staff member was wearing the right personal protective equipment (PPE). There have definitely been times when staff have made a risk assessment and not followed the protocols about what PPE to wear and have then responded to these phone calls with ‘what can you do?’ in relation to the exposure. Sadly, in some cases there is nothing that can be done once the guidance has been bypassed but to wait and see, which is the reason for the guidance in the first place. Fortunately, for most scenario’s in the real world, the consequence isn’t bloody horror, death and an alien threat to mankind.
Risk assessment is linked to risk management
One of the reasons that protocols are in place in the Alien movies is that someone, somewhere, has obviously recognised the risk of infection in a small contained community where everyone interacts and lives on top of each other. Even in Aliens, when you’re talking about somewhere the size of a colony, this principle stands. This is because you are unlikely to be able to access a clinical trial on a mining ship, or develop a novel antiviral on terraforming mission, even if what you’re importing is a more traditional style of infection, versus an Alien parasite. The extent of the risk mitigations needed will always align to the risk itself. If you are concerned about an introducing something that is untreatable, then your measures are going to be much more extreme than if your infection is likely to just mean someone goes to bed and takes paracetamol for a weekend. If you can’t treat, then prevention is your only option. After 9 movies there doesn’t appear to be a Xenomorph (Alien) cure and so measures taken to prevent allowing one into your space need to match the risk they present.
This approach is definitely seen in response to infection in IPC. If you have a condition that spreads easily, rapidly and can be incapacitating for a period (i.e. norovirus) then you will use a different set of precautions to those that you use to manage something which may not be as transmittable but is untreatable or has life threatening consequences such as a haemorrhagic fever. Having conversations and being open with people about the risks of getting things wrong and ensuring that individuals understand why responses are different in different circumstances are a key requirement for people working in IPC, and something I think we should all endeavour to do better at. I think the days of asking people to blindly follow protocols should probably be behind us, as I think the Alien movies demonstrate that if people don’t get the why, they often ignore some of the core components based on external drivers
So, what lessons can we learn?
Beware of acting on incomplete information
Decisions are consistently made in these movies based on incomplete information, which leads them to underestimate both risk and consequences. A great example of this is the way people use information related to the black goo, especially in Alien Romulus, maybe don’t inject yourself with a substance that doesn’t have a proper name let alone a full data set for you to understand what it does. The other thing is that information is often treated as static, and so there is very little rapid inclusion of new info, rather than being mindful of an iterative response to new data, so help constantly inform and improve your risk assessment. It’s always worth being conscious of when is enough is enough when it comes to information and decision making.
Emotions get in the way of logic
During the movie Covenant, the entire crew is made up of couples. I get this in terms of colonisation, but in terms of good decision making, and in relation to risk this is just a one way route to bad outcomes. There’s a reason that in a certain Zombie series husbands have kept their zombie wives locked in basements rather than removing the risk to them and others. There’s a reason medical professionals should not manage their loved ones. Emotions interfere with logic, and there is no way under this setting you are managing to make decisions without your emotions getting in the way. It’s a reminder that if we become aware that we are in an emotive place, it may be the time to step away and take a deep breath, before making that judgement call or even tap out entirely and allow someone more removed to take our place.
The contrast between human emotional decision making and evidence based decision making, usually undertaken by the android cast, is beautifully explored during Romulus via Andys story arch and is one of the highlights for me in terms of enjoyment.
Science doesn’t change based on how much you wish the outcome to be different
One of the reasons that emotional involvement in decision making can be so challenging is that it can interfere with perspective and accurate interpretation of risk, thus impacting risk perception. Sadly the truth that wishing does not impact outcomes is hard to argue with, but it is human to try to persuade ourselves we have more control and ability to influence the outcome than we do. Under stress, our natural tendencies towards pessimism or optimism are definitely amplified. All of this means that when there is someone at the door banging and begging to be admitted, it is easy to persuade ourselves there is a) enough time to manage to open the door safely and b) the consequences of opening said door will not be as bad as we fear. Emotions don’t change outcomes but we are almost programmed to hope that they can.
An individual will always want to be the 1 in a million
The reason someone opens the door is the same reason that when one character looks at another and utters the fateful and true words ‘it’s too late’, and it almost definitely is, neither one acts before everything gets out of control. Humans are not good at dealing with numbers and risk when they are actively involved in the situation. One of the reasons we aren’t in that we throw sentences around saying it is a 1/million chance. We, as humans, have a tendency to focus the fact that, although it is a long shot, there is a chance that things can go your way. Sadly, as someone who has experienced the opposite, where my sister died in a 1/10,000 pregnancy, someone always need to be the one. The stats work both ways, whereas most of us survive in the world by only focussing on one side of the equation. This therefore impacts our capacity to evaluate any risk in situations we are involved with. Somebody always bears the cost and few of us can bear the vulnerability of acknowledging that that somebody could be us.
The people with the most experience are not always the ones making the decisions
One of the other main themes in these movies is that decisions, when not being made by friend and loved ones, are often being made by people in positions of power, not necessarily based on knowledge or even accepting of prior experience. This works well or not so well based on how well they listen to those who do have the information to help improve their decision making. Chains of command, especially in high stakes scenarios, are not necessarily bad, as we’ve already talked about the risks linked to emotional decision making, but so much depends on how well they work and how they place value on evidence based choices rather than hierarchy.
The other theme here is the trusting of unknown sources, especially ones with no evidence of expertise, over those who have either lived experience or expertise. I think this one resonates a lot right now, when there are so many sources of misinformation out there, and so many conspiracy theories that rely on speculation and rumour. Fact checking is key, be that on a space ship or deciding on your vaccination options.
Not everyone has the same thought processes
One of the other reasons decision making goes astray in these movies is because those involved in that decision making often have undisclosed values, beliefs or drivers that are impacting their choices, and this process is not always obvious to those others involved. This is true from androids that may or may not be obviously androids and who will have programmed ‘primary directive’, as well those working for the corporation. This is interesting as they often have more complete information than the others involved, as well as seeing the situation through a different lens because of how they view the world. This means that they can see others as disposable or views risks different, as they have a set of criteria that they wish to achieve which is more than just survival. Although in clinical life the juxtaposition is rarely so extreme, the challenge of reaching alignment when people come with different world views can definitely impact shared decision making.
Smart people can do stupid things
Having said all of that, smart people can in general do stupid things, even without all of these complications. Even when the experts are the ones making the decisions they can still make the wrong ones, especially when tired, stressed, or lacking all the information. This is the reason why protocols are key, drawn up and decided upon when all of the confounders to good decision making are not present.
You need to follow the standard operation procedures
In the end this entire post has been a very very long way of saying ‘JUST FOLLOW THE SOP!’
Many of these movies but have been much shorter with a much reduced body count, if those involved had just followed the pre-established procedures laid down for their safety. Obviously, we don’t have so many Xenomorphs as a daily risk factor in healthcare, but the same is true for us. SOPs are rarely there for the sake of it, they are there to support decision making so that in times of stress or information overload, you are not having to seek extra information to support good decision making, you have it freely pre-digested and available to you. So the next time you think twice about donning that PPE or the closing that isolation room door, ask yourself ‘would you open the airlock door?’, think twice and do the right thing.
And now for something completely different
Finally, because this is something that has amused me whilst watching these films and is probably not something that I can talk about in general down the pub. The computer in the Alien movies is usually referred to as Muthur, pronounced Mother. I just want to share my joy that the analysis software that is used to help analyse 16S rDNA runs, to give you microbiome analysis i.e. tell you what bacteria are present in your sample, is called Mothur, and also pronounced Mother. I’m sure the two things have nothing to do with each other, but allow me my scientific joy that something which was so ‘other world’ when it came out to me as a scientist has the same name as something imagined from ‘another world’.
Also, if anyone needs a science advisor on their next project, give me a shout as this post has brought me much joy and I think I may have missed my calling 🙂