
Yesterday the NCL Education Partnership hosted our 4th annual (bar COVID-19 related 2020) Healthcare Science Education conference (#HCSEd). These meetings came about as way to encourage and support Healthcare Scientists to recognise themselves as educators, in the widest possible context, not linked to specific training schemes or disciplines. It’s something we continue to be passionate about and if you’d like to get involved in future events please drop either myself, Ant De Souza or Vicki Heath a message.
This years theme was innovation in education and ended up including a lot about how we innovate, not just in terms of the technology, but in terms of our approaches in working with trainees, teams, workforce and the public.

The day was chaired by the Vicky Nash who is an established leader within medical education and is a great supporter of the Healthcare Science workforce. (NB apologies for my poor photography skills, all the good ones are from Rabbit Hole Photography and when the other ones come through. I will swap them out)

Nicola Baldwin, playwright and screen writer, kicked off our first talk on ‘Public perceptions of Healthcare Scientists during the pandemic’
Her talk was about her experience both as a member of the public and someone who works with Healthcare Scientists about how that perception has changed over the course of the pandemic and what some of the drivers for that change has been.


She told the story of how at the start people were engaged and interested, they felt part of the narrative and then they began to get lost as part of the conversation. We (Healthcare Scientists) lost our place in the story in the same way that the general public lost their ability to engage in the conversation as it became politicised and increasingly focussed on strategy and technicalities.
As someone who has previously written for Holby City she discussed that one of the reasons Healthcare Scientists are not represented on TV in the same way that doctors and nurses frequently are, is that doctors and nurses are presented as flawed human beings. They get the tests and they ignore them or they react to crash calls for good or ill, and frequently lack the information they need to make decisions. They are effectively glorified members of the public and therefore fulfil that role within the narrative of connecting with the view. In medical drama the guest stories i.e. patients, are only there to challenge the flaws or impact on the regulars i.e. the cast. In reality Healthcare Scientists do not visibly battle but work hard to remove their flaws from the equation, and therefore leave their emotions at the door. They live in a data driven world where patients do not always get better and we all die. Because of this Healthcare Scientists do not obfuscate and do not hope for the best, but make evidence based decisions and work in a world of these facts and may therefore make less attractive heroes for fictionalised drama. In the real world the longer the pandemic has gone on the more that scientists have been seen as messengers of doom as they deliver fact, not necessarily a message of deliverance.
So how do we move towards speaking the same language and engage?
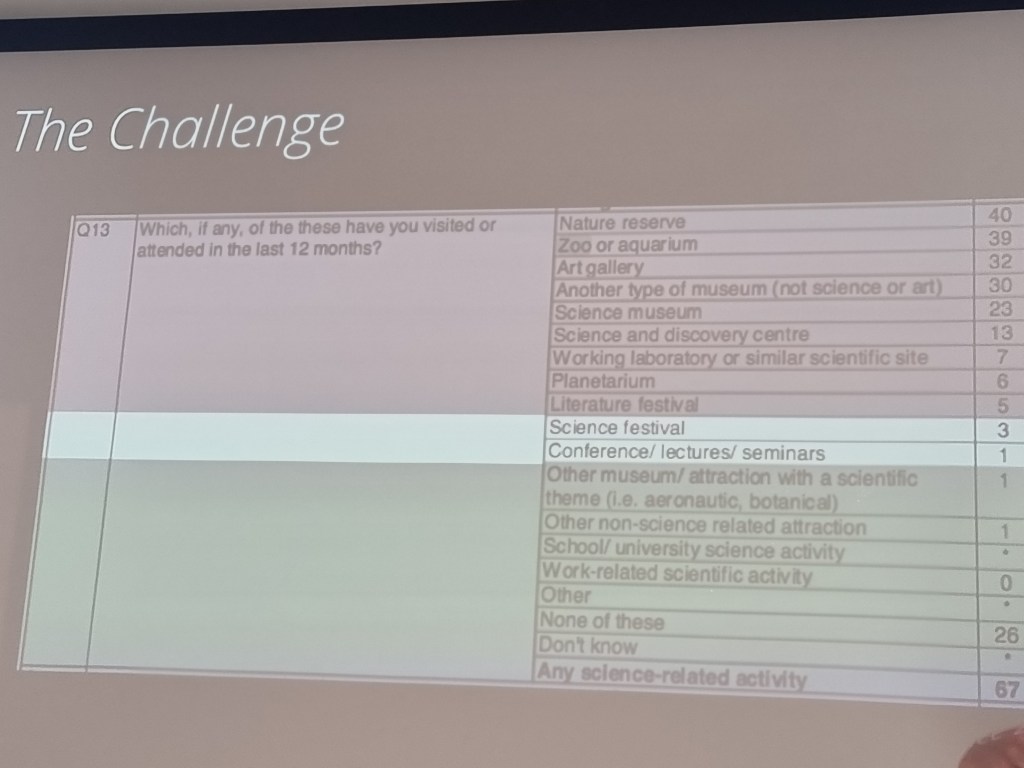
The challenge outside of the Healthcare Science profession is that the pandemic has laid bare a lack of scientific literacy and connection between scientists and the public domain and has therefore left reservoirs of fear. Our most basic measures of literacy are to read and obey basic instructions. Above this level educationalists have said is the ability to read and engage with newspapers and other sources. Above even this is the ability to compare, digest and analyse in order to support meaningful engagement. The same thing is needed in terms of scientific literacy and engagement. Connections between science and the public are needed to enable people to navigate the space and literacy is required to support analysis and evaluation of the information is available. Sometimes the connection between the Healthcare Scientist workforce and the general public is limited by a culture emphasises teamwork and there is a lack of individual promotion. In many ways this is great but it is important to be out there and therefore some form of promotion is needed.
Public perceptions have been changeable and volatile, opportunities to explain that from early in the pandemic were missed and that has resulted in public scepticism. To change this engagement of Healthcare Scientists is key to ensure that scientific literacy and the best way to do this is to not be afraid to promote and make connections. You and your stories can change the world!
Dr Steve Cross, science communicator, talked about ‘Science and science communicators’
Following on really nicely from Nicola with her call to arms in terms of the need to start and be part of the conversation, Steve talks about the practical aspects and challenges of engaging as a science communicator.
The big challenge for UK science communication infrastructure is that is consumed by 13% of the population which mostly consists of white, wealthy, males, who are 35 – 50. This doesn’t reflect our population, patients or future workforce so how do we communicate outside of the 13%? Some of this stems from the official science communication structures, such as the media, believing that ‘The public love debates about genomics’.
As nobody has to engage you have to make it engaging? How do you make something that actually works rather than ticking a box?




So how do we go about thinking how we undertake engagement activity? A good place to start is using Design Theory.
- Empathise with the audience – remember ‘the public does not exist’ they are vastly different. Think about who you are trying to reach and why
- Define the problem – put in work to really understand what you are trying to address, what are the barriers, who are your stakeholders, what are the reasons why things haven’t work before and what have people already tried
- Have ideas – have lots of ideas, sensible ideas, crazy ideas, out of the box ideas
- Prototype – come up with lots of approaches to those ideas and try them out, be prepared to try loads of them and throw them away in order to refine the prototype
- Test and evaluate – once you have a prototype make sure you continue to test and ensure you evaluate and improve
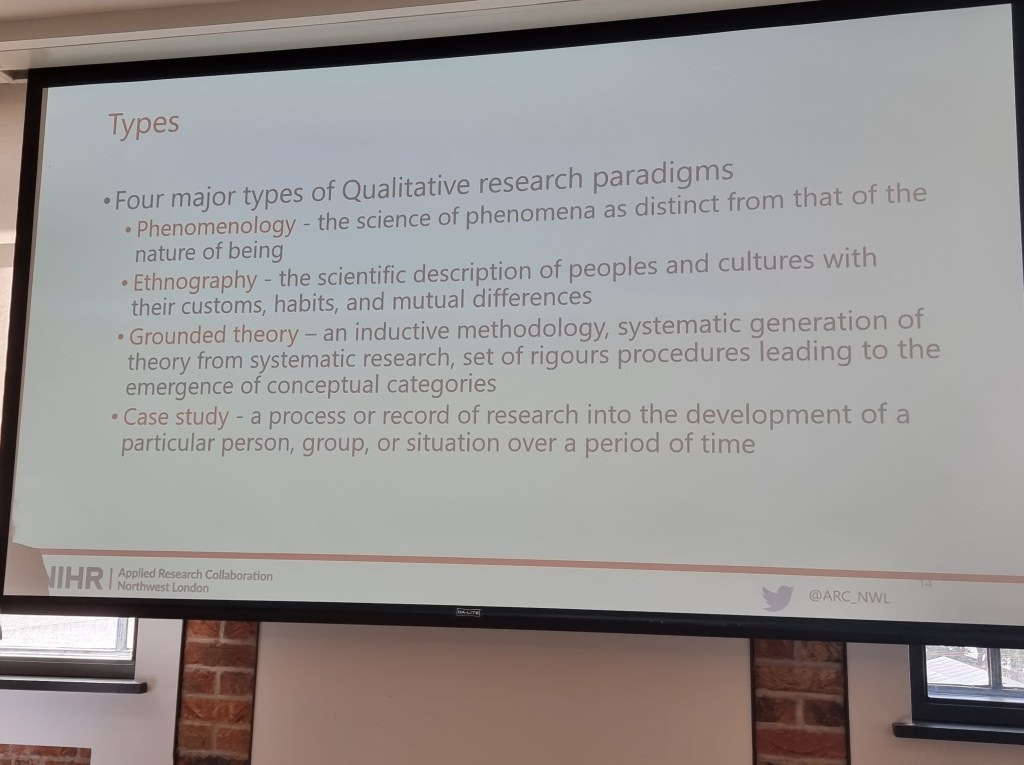
Dr Rowan Myron, associate professor of healthcare management, gave our keynote on ‘Qualitative data collection’
Rowan started out talking about the pros and cons of quantitative vs qualitative data: qualitative may not be generalisable but gives rich data set exploring how and why, whereas quantitative may enable extrapolation but may be less deep and doesn’t normally explore motivations.
Traditionally Healthcare Scientists are considered to be Positivists, believing that data should give answers and therefore leaning towards quantitative data collection. Professionals that work with qualitative data are often considered to have more of a constructivist approach, where each piece of learning develops from the last and therefore permits exploration of how and why that development occurs.
It is also possible to have a mixed methods approach where some aspects of the work lend themselves to a quantitative approach, with other project components lending themselves to a qualitative collection method i.e. where you may use surveys to explore underlying attitudes but relate it to comparative quantitative bench marks.

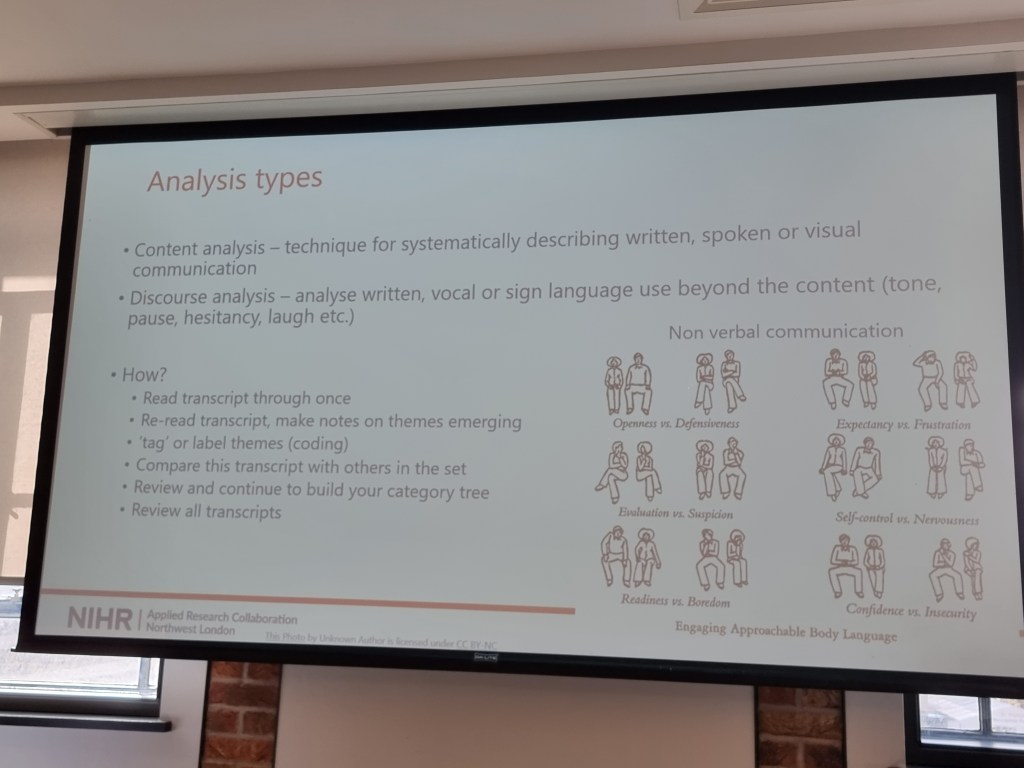
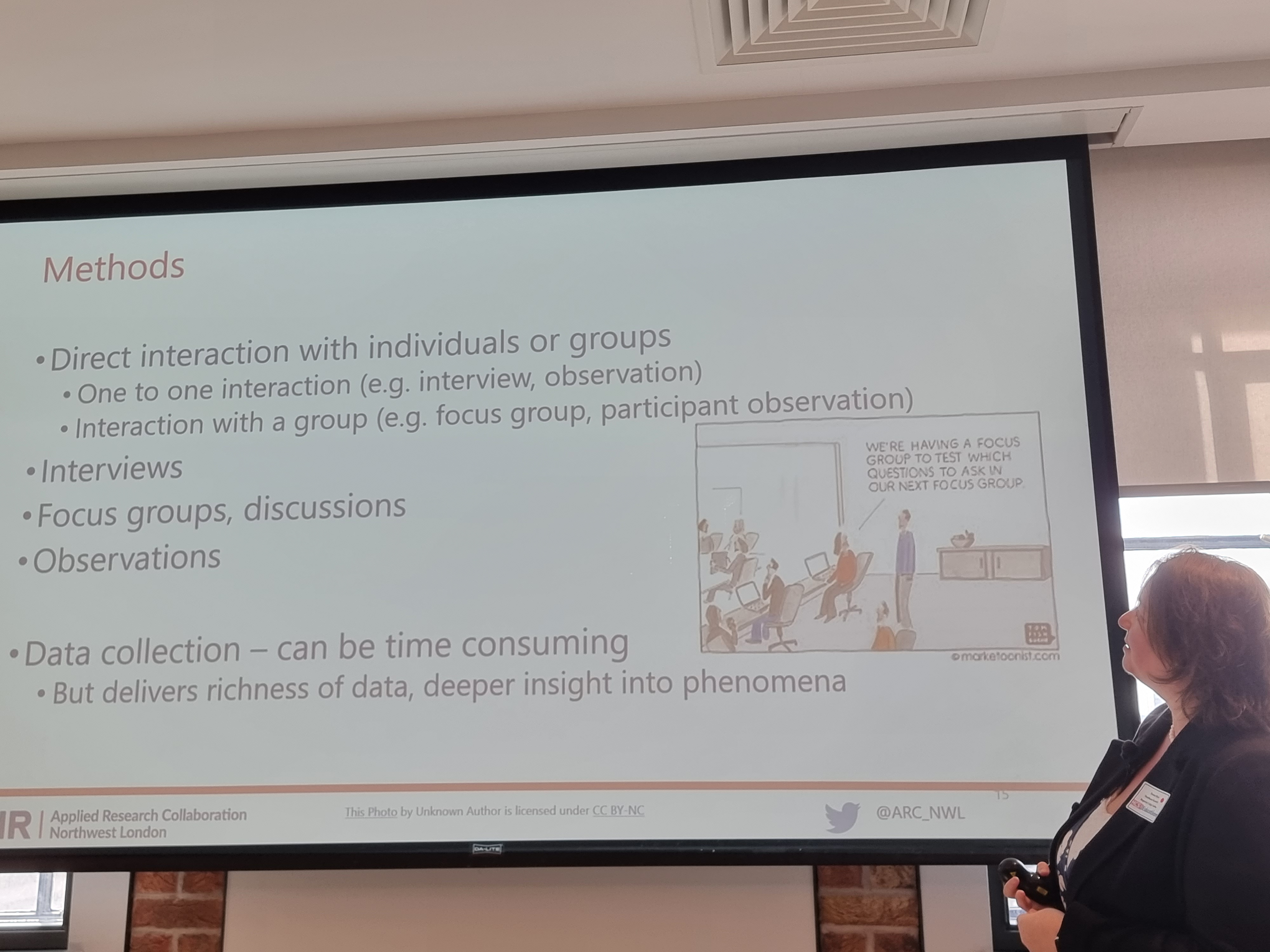
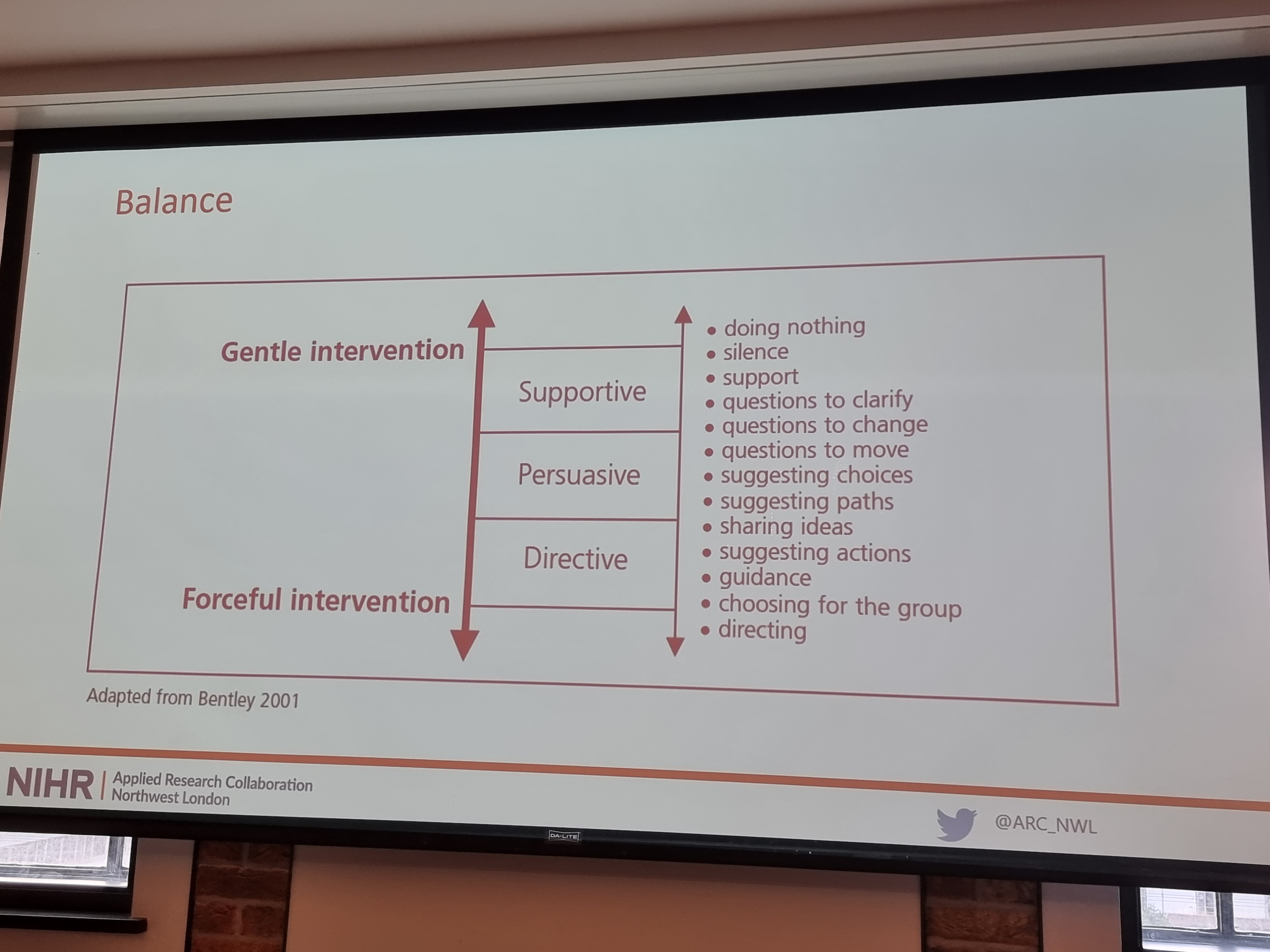
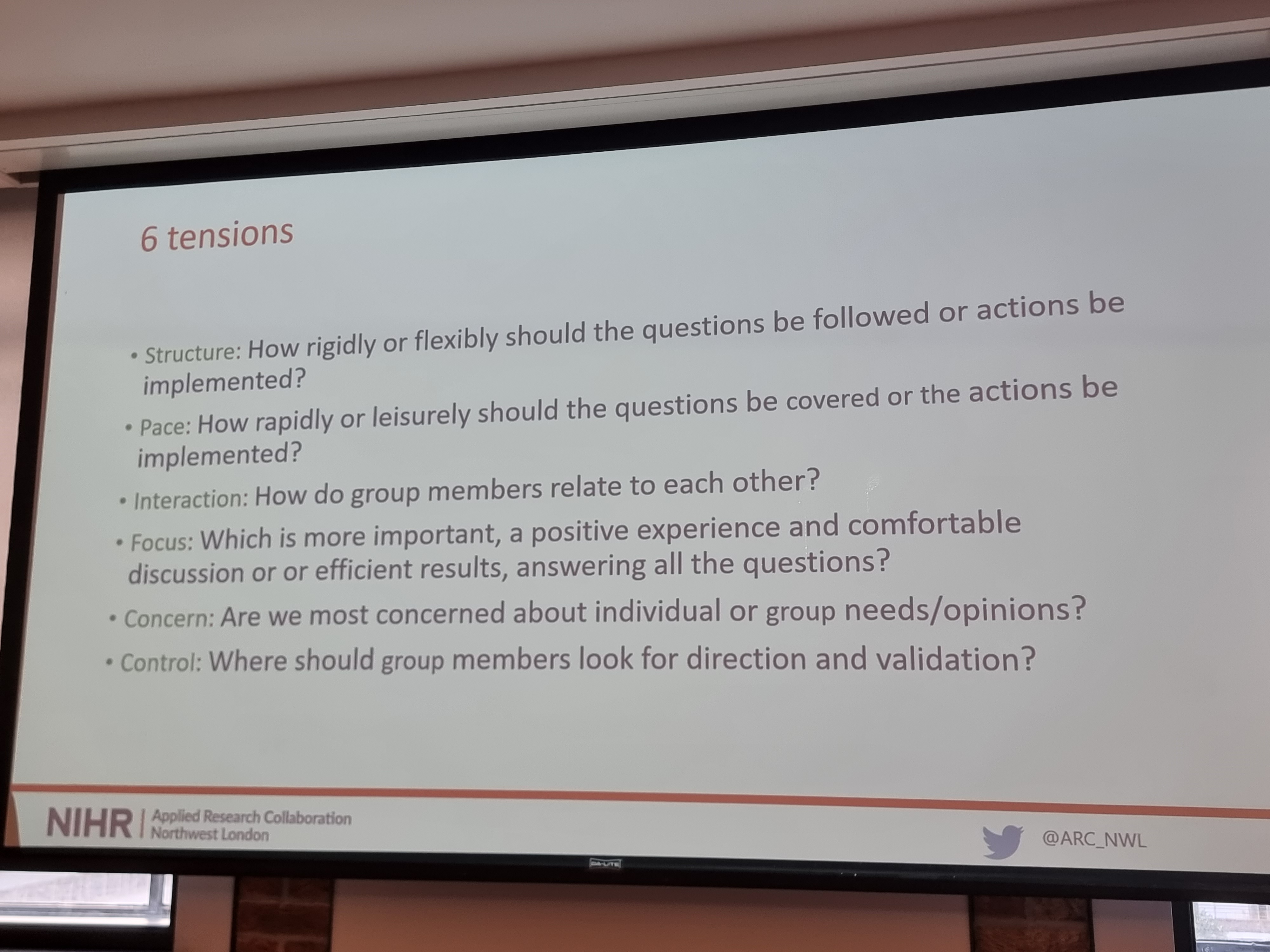
The best approach for facilitating these conversations can vary from free – semi structured – structured and the style of facilitation matters. Directive interventions may be appropriate in some clinical meetings but is less likely to be successful in terms of gaining information and insights in a qualitative research setting.
Being in the room can sometimes change what people tell you – as a qualitative researcher you can get some of the best responses when you turn the data recorder off and so how you record and capture some of that which doesn’t fit into your framework, however it is important to consider the ethics of this. It is also key to ensure that you are recording accurately and not interpreting, and therefore checking in with participants to ensure that recordings are accurate is key.

Using some of these techniques can also help in non-research settings, such as team meetings and 1:1 in order to improve communication quality
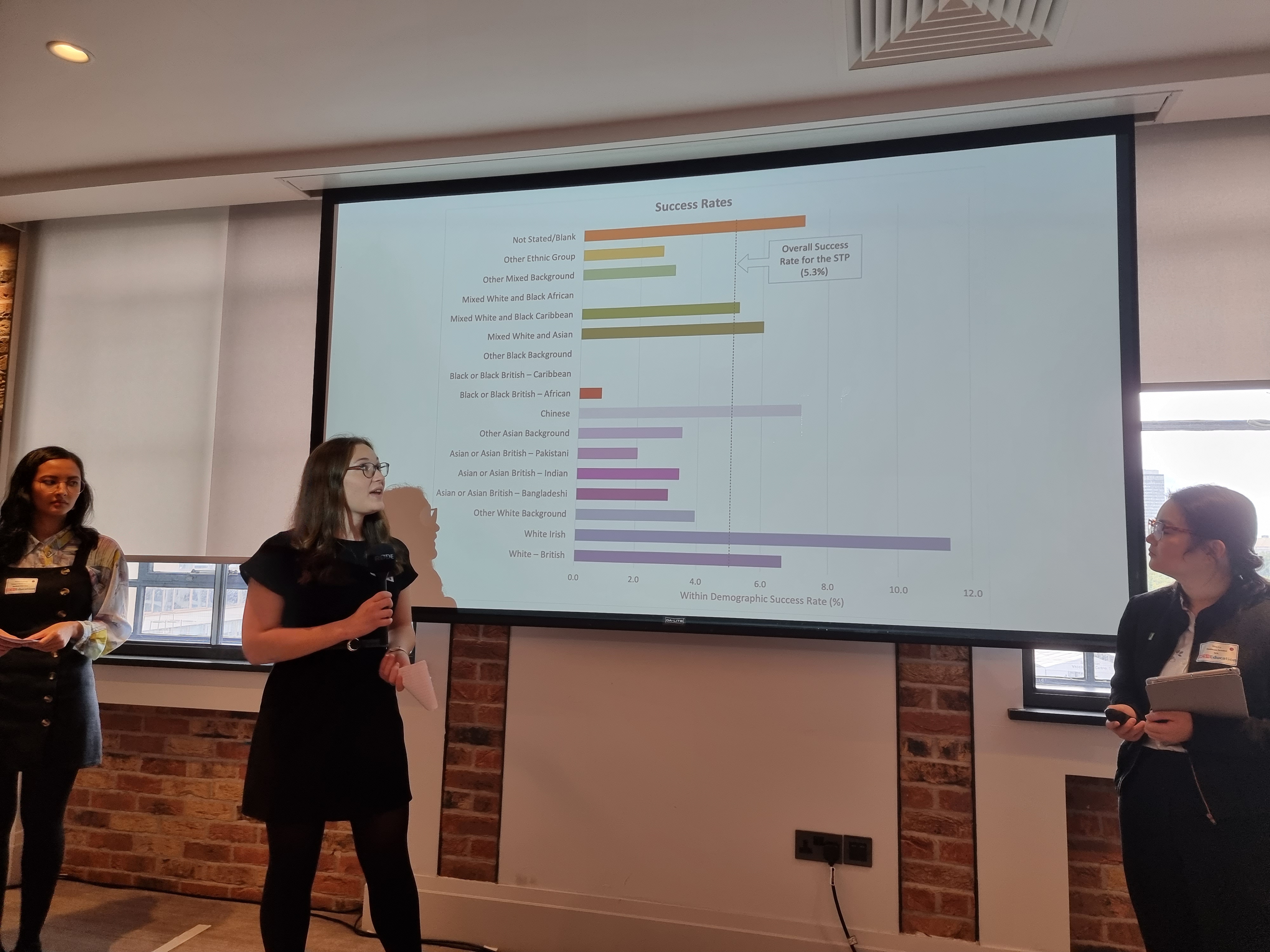
BAME Scientist Trainee Network gave a really important session on ‘Diversity in access to education’

The session was really impactful for me and I believe having these kinds of sessions and conversations is key if we are going to address some of the issues raised.
For those coming into the healthcare system as staff members, white applicants for posts across the NHS are 1.5x more likely to be appointed from shortlisting than non white applicants. In order to change the system that permits this we need to start with education and therefore understand the biases of the system that recruits into it. This challenge was shown to also be reflected in the STP appointment scheme, where the average success rate was ~5% but for Black/Black British – African applicants the success rate was ~1%.
When in post 1/3 of BAME staff report having been harassed or bullied at work either by patients or their colleagues.
For those coming into the NHS and healthcare systems as patients healthcare inequalities exist and are often based on myths that emerged from 18th century studies linked to slavery, such as black people feel less pain as they have less nerve endings. Within the NHS black women are 5x more likely to die in child birth and black patients at half as likely to receive pain medication.
Not only are the issues backed up by research and other evidence but there is also data to show that promoting equality, diversity and inclusion does not just benefit BAME groups, and therefore benefits the workforce and patient population as a whole.
So what can we do to support our BAME colleagues?
The following suggestions were taken as part of a qualitative research study from BAME and white Healthcare Scientists, rooted in their lived experiences (as we learnt from Rowen, this permits the exploring of why and how questions).
Advice for leaders:
- Unconscious bias training – manager and leaders have the biggest influence and it was felt could have the biggest impact on as inclusive environment, and that active allyship was key
- Diverse influence panels – decreases the collective effects of unconscious bias
- Monitoring for training opportunities – ensuring equality , measure and monitor metrics and review access
- Mentorship, including reverse mentorship
- Diverse teams
- Zero tolerance of inappropriate language, awareness of micro aggressions
- Equal opportunities for showcasing skills – ensuring that extra curricular activities or additional responsibilities were accessible to everyone, not based on connection to a manager
- Practical advice to address specific needs i.e prayer room location, halal food options, joining staff inclusion networks
Advice for non-leaders:
- Read WRES reports workplace race equality standards
- Actively learn about others perspectives
- Check in with colleagues when incidents witnessed
- Advocate for others
- Target outreach to schools in disadvantaged areas
- Review clinical practices and ask whether they are contributing to health inequalities
No matter what your role you have the ability to take steps to counter the data shown and so this is a call to action and take steps as individuals, teams and organisations to address these issues.
Dr Jane Freeman and Dr Kerrie Davies, NIHR clinical lecturers and clinical scientists, ‘Communicating differently’
To finish off the morning with a bang Jane and Kerrie called on us to really think who are we, and not just our scientific credentials……. what is our talent, not just our ability to plate 200 samples and hour…….and to think who are the audience we’re trying to reach? What is the message your trying to get across? How can you make it memorable? One size does not fit all??
Communication is about connecting with people and that involves taking risks, doing the unconventional, bringing whole self to work………..not just Dr XXXX but all of you. As I have said in a previous blog I do my best science over a cup of tea and Jane and Kerrie emphasized that talking is key, with conversations being the starting point to any success piece of work.
Actions however speak louder than words and so below is my (rather shoddy) recording of one way that Jane and Kerry show that actions speak louder than words. Enjoy the Small Faeces discussing ‘Quality’!
For the afternoon session we moved onto the workshops. There were three streams to choose from:
Stream One – Innovation in outreach by Victoria Heath and James Harkin, followed by Royal Literary Fund – Rooftop writers by Nicola Baldwin
Stream Two – Top tips for delivering educational activities online by Justin Poisson, followed by Evaluation of digital education by Ian Davies and Matt Coombes-Boxall
A starting reflection on the transition to digital delivery from face to face learning. A move from reactive remote learning to blended learning. Sessions were put together to lecturers and students. ‘Moving your lectures online’. Online induction resources’, ‘Talking into the void’.
The session then talked about learning technologists, and translating practice to the educational environment. Opportunities were given for staff to showcase how they moved their online to a digital format.
Retention research has highlighted that regular feedback was important and that to support this the community of inquiry model was encouraged as something to think about when delivering sessions.
There was also a demo different learning software’s that could to help with engagement: Flip grid, Wakelett, Mural
Stream Three – Maintaining your education during a pandemic by the London Healthcare Scientist Trainee Network, followed by Influencing upwards by Cherie Beckett

I was lucky enough to be supporting the stream three session which was kicked off by the LHCSTN who ran a really interactive session getting everyone in the room to explore and score (1 – 10) whether the pandemic had impacted on 7 key areas, either as a trainee or a trainer:
- Redeployment/role changes
- Exposure to practical clinical skills
- Rotations and placements
- Research projects
- Staying connected
- Virtual learning
- Wellbeing
We then talked through the learning and different ways those in the room has dealt with the high scoring impacts they had experienced.


Cherie then followed on with an equally interactive session exploring everything from how we introduce ourselves i.e. ‘just a trainee’ or using banding, to how to expand your influence. The group spent time identifying barriers to influencing up and reflecting on whether some of those were self imposed. Then we moved onto to talking about how to navigate around those barriers or coping strategies for the internal ones.
The final session of the day was the plenary given by Vivienne Parry, Science writer and broadcaster (and all around Healthcare Scientist champion)
Viv finished the day in inspiring style by reminding us all of why what we do matters, the impact that we have but also re-iterated the message of the day – that we have to be seen! We need to talk to people like we do to our families and explain what we do and why it’s important. Not speak like we do to our colleagues, not like we are speaking to a Guardian science reporter, but like we do when we are outside work. That is how we talk in a way that is heard and received. We are too important to be invisible and now is our time to shine!

NB – these are the meaning of the sessions as I received them as a member of the audience, hearing through my own lens, these are not verbatim notes, although I’ve tried to be as accurate as I can. All opinions on this blog are therefore my own
