
This is the post I was supposed to get out last week but didn’t quite make it as my mind latched onto dealing with what was directly in front of me, rather than being in a more conceptual space. That said, after having just run a course, where the main theme was supporting participants to be able to use frameworks to make risk assessments, it still feels like an important conversation to have. Now, these are just my observations and thoughts. They are not meant to be criticisms of any person or indeed the system itself. I hope it will just continue the conversation about what serves us and our patients best, and we all know there is not a one size fits all approach.
Pre-pandemic it felt, to me, that there were guidelines frameworks out there, particularly linked to things like Carbapenemase Producing Enterobacteriales (CPE’s), but in the main part Infection Prevention and Control (IPC) teams used a lot of personal judgement and experience to determine routes to management, with input from Health Protection Units as needed. The pandemic led to a big switch, where a command and control approach was undertaken. This made complete sense, as resources were restricted and shared across the system. Therefore, frameworks supported us all practising in similar ways and with expectation setting. They also supported large scale evidence collection to improve interventions. We were also in a scenario where some of the diversity of what we were dealing with was removed, in terms of IPC, the focus was mainly on one key organism. Now we are moving back into ‘business as usual’ both in terms of patient flow, and in terms of organisms, that one size fits all approach feels like it may do us a disservice, as the challenges are now so much more diverse. We therefore need to think about how me move back to a much more risk based approach, where instead of having a single organism focus, we also take the setting and the patient into consideration.
Risk assessment and risk based decision making
Those of you who have read some of my other blogs, about the fact that I genuinely believe that IPC is 90% risk assessment will not be surprised that I believe that we need to empower people to undertake these risk assessments better. For 3 years we have given everyone very specific instructions for their actions on every part of the pathway, when to test, what test to use, what PPE to wear, all possible because we were focussed on one thing, much like the standard risk matrix below: risk = SARS CoV2, and all risk mitigations are rated against this in a 2:2 matrix.
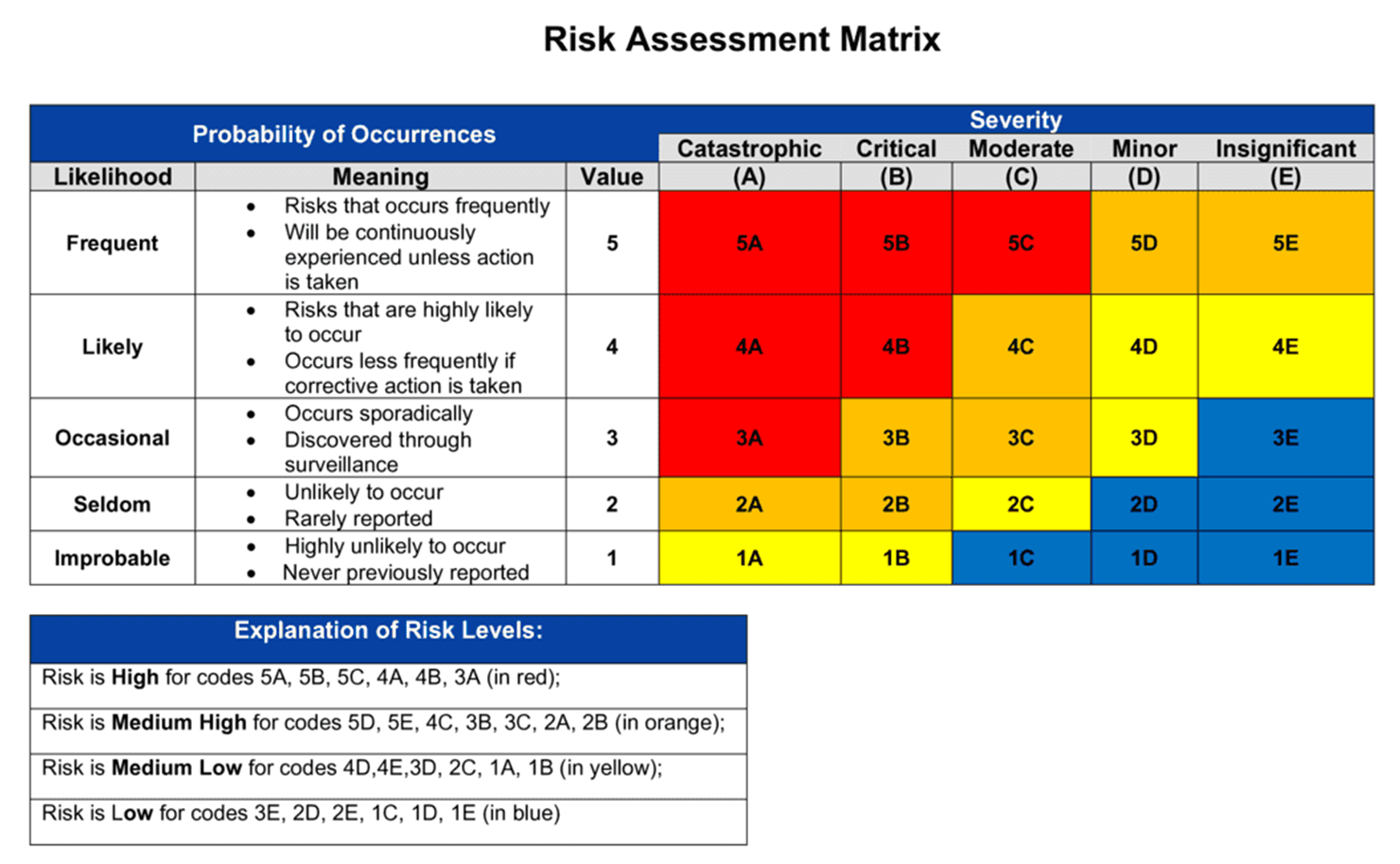
We are moving back to a world where, instead of using a matrix where everything is measured for it’s efficacy against against a single pathogen, we need to consider multiple pathogens, their characteristics, and how these play out differently in different patient populations and in different settings. Therefore a standard risk matrix approach does not serve the outcome of increased patient safety we all want to achieve.

Sadly, it also gets even more complicated. We have been living in a healthcare system for the last 3 years where everything, action wise, felt like it was determined by testing and test results. That means that we have been functioning using a test based action algorithm for a very long time. Now, I’m a scientist, and therefore love a good diagnostic test. However, in healthcare there are so many things that can impact on test outcomes: timing of the sample, factors such as antibiotics, quality of the sample, test requesting accuracy, specimen type etc etc etc. We are not just optimising all of our testing pathways for improved sensitivity in relation to a single organism, we are trying to use the best choice we can in order to maximise information output for a wide range, there will therefore be things that bias the accuracy of those results. So we are back in a healthcare world where we need to stop being so focussed on the test and the test result, and start seeing the patient in front of us again, irrespective of what the negative test may say. We need to move back from a test based approach to a symptom based approach. If my patient has respiratory symptoms, they should be in droplet/airborne precautions, irrespective of what the test results say. If my patient has diarrhoea, then we need to put them in contact precautions irrespective of a negative gastro panel, unless you have clinically evaluated other reasons for the symptoms. This clinical evaluation step is key, and you can’t put all of the information linked to that in a flowchart, therefore we need to switch from command and control responses, to supporting the experts at the bedside to use their clinical knowledge to evaluate patients, and support them in better risk based decision making to support IPC. We have to acknowledge that the assessment process is complex, but also feel that we have supported staff enough to be able to make those complex judgements.

Acknowledging the uncertainty in the system
The problem with a risk assessment based strategy, managed primarily at the bed side, is two fold. Firstly, you have to be prepared to support with the education to enable it to succeed and to know when to escalate and question. This can be time consuming and it is a task that needs to be continuously supported, as staff, patient mix and environments change. Secondly, we have to have honest conversations with staff to help them to understand and become more comfortable with some of the principles of uncertainty. This is because algorithm based approaches often offer, sometimes unreal, certainty. If I do A and then B in compliance with a flow chart everything will be alright. By increasing complexity in decision making, you also introduce uncertainty, and that needs to be acknowledge and addressed as part of our approaches. Otherwise staff will never feel empowered to take the steps required.

Types of uncertainty
The first thing to say, is that not all uncertainty is the same, and therefore you need to approach different types using different tools. Epistemic uncertainty, is the one in healthcare we can probably do the most about. It’s the kind of uncertainty which we can, sometimes, address by asking better questions. Questions like, I notice you seem to be using a lot of tissues, do you have have a cold or feel like you have a bad chest? Questions like, have you been in contact with anyone who has had an infection or been unwell recently? Or have you been travelling a lot recently? If we can support our staff to feel more confident in collecting the information they need, and then knowing what to do with it, they will feel more confident in making decisions without escalating all of those decisions up to someone else for sign off.

Other forms of uncertainty, such as aleatoric uncertainty are harder to address. This isn’t uncertainty that you can address by gaining more or better information, it’s the kind of random chance events that you have to manage by becoming more comfortable with the fact that healthcare is multifactorial, and you may never be 100% about any action or solution. An example I always use in my head for this is a 4 bedded bay where someone has just vomited due to norovirus. We know on the balance of evidence all 3 other patients are likely to acquire norovirus, as it will stay in the air for ~2 hours and up to a million copies of the virus will circulate prior to deposition. What we don’t know is, did 1 of those 3 patients have norovirus last month after a wedding, and therefore currently has sufficient immunity against the circulating strain? Is 1 of the others one of the small number of people who have receptor variance which means they are less likely to acquire infection? You can’t get that information by looking at them, you are unlikely to be able to get that information by testing or asking questions. Therefore you have to manage the uncertainty and deal with the decision making you can undertake, with the information available to you. That decision making also becomes much more complex when consensus making is difficult, and so supporting staff to know how and when to escalate when this occurs is really important.

So how do we deal with uncertainty better?
For me, the first step is to acknowledge that it is there, rather than trying to persuade ourselves that bedside risk assessment is a) easy and b) doesn’t come with any discomfort for the staff we are asking to undertake it. It takes time and space to be able to this well, both for the required educational component and for the staff to be able to have the cognitive space to ask and process the questions, as well as undertake any follow up. It also takes us to really recognise that we are a single team working across that healthcare pathway, this isn’t about IPC putting their responsibilities onto someone else, it’s about improving patient outcomes by having the people evaluating patients as close as possible to the ones making informed decision about those patients. It does not stop the requirement for complex decision making to be escalated or remove the need to be able to ask for support. It also requires feedback and monitoring so that staff do not feel like they are being left alone to carry a risk or fearing consequences for inappropriate decision making. It is about empowerment in patient care, not resource saving.
I personally believe that we need to move away from central dictates for IPC decision making, patients are unique, and combining that with different environments and organisms means that numerous factors need to be taken into consideration if we are to provide the best possible care. That cannot be done well centrally, where we never see the patient and are not aware of the minute by minute changes in their wellbeing. Supporting those at the bedside to make better decisions and empowering them to be the people who respond to those changes is key to moving away from the single organism focus of the pandemic. IPC teams are key, they should be the ones educating, empowering and being the escalation points, but there are simply not enough of them to have one at every bedside and so we need to look at spreading the knowledge and IPC love!
All opinions in this blog are my own
