
This blog is late. I make no apologies for that as last night was Eurovision, one of the highlights of my year. It’s been one hell of a week and so, in an attempt to find some work life balance, I had the evening off. Malta and Iceland were robbed (in my personal opinion), and I now firmly believe that all teams should have jumpers with the faces of the team upon them #bonding. Well, now that’s over with, onto the other thing that was on my mind this week.
I recorded a podcast with the wonderful Martin Kiernan for the Infection Matters podcast just over a week ago. The podcast series is on Spotify and definitely worth checking out if you have a moment (link below to the 1st episode). We had a chat about the role of Healthcare Scientists within Infection Prevention and Control (IPC) teams: a subject you may have noticed I’m pretty passionate about. Just being asked to have that conversation felt like an enormous step forward, in terms of recognition of the role and the benefits we can bring.
So, imagine my disappointment when last week I received a grant review which reminded me of just how far we have left to go…
The grant was about the detection of bioaerosols in hospitals to support rapid IPC interventions and changes to patient management in regard to their infection/colonisation. The reviewer, a respiratory consultant, responded to the proposal to say that, as there was no medic on the proposal, the team could not possibly have an understanding of the risks associated with respiratory infection, and that one was needed for the grant to be funded. I must admit to being more than a little peeved by the response.
For context about what Healthcare Scientist career pathways look like in IPC, I have previously written a blog for the Healthcare Infection Society which might be useful. The main take away points for me are these:
- I have the same post graduate qualifications as my medical colleagues (MSc Clinical Microbiology, Medical Microbiology part 1 and Medical Microbiology Part 2 by examination leading to Fellowship of the Royal College of Pathologists)..
- In addition to the qualification required for my medical colleagues, Healthcare Scientists require a PhD (usually) to attain a consultant post. Mine is in the ‘Role of the Environment in Transmission of Healthcare Associated Infection.’
- Healthcare Scientists are required to be engaged in research as part of their state registration (needed to practice within the role). I currently hold £21 million+ of grant funding.
My point, therefore, is this. I am not a wannabe medic who became a scientist because she couldn’t get into medical school. Neither I am a second class medic, where the Trust hired a scientist because they didn’t have the money to hire a doctor instead. I am a proud scientist who chose this career path, knowing what being a scientist can bring to the conversation. I add to the team, not subtract from it. I bring something different, and that something different is not only important for where we are now, but crucial for what we can achieve moving forward.
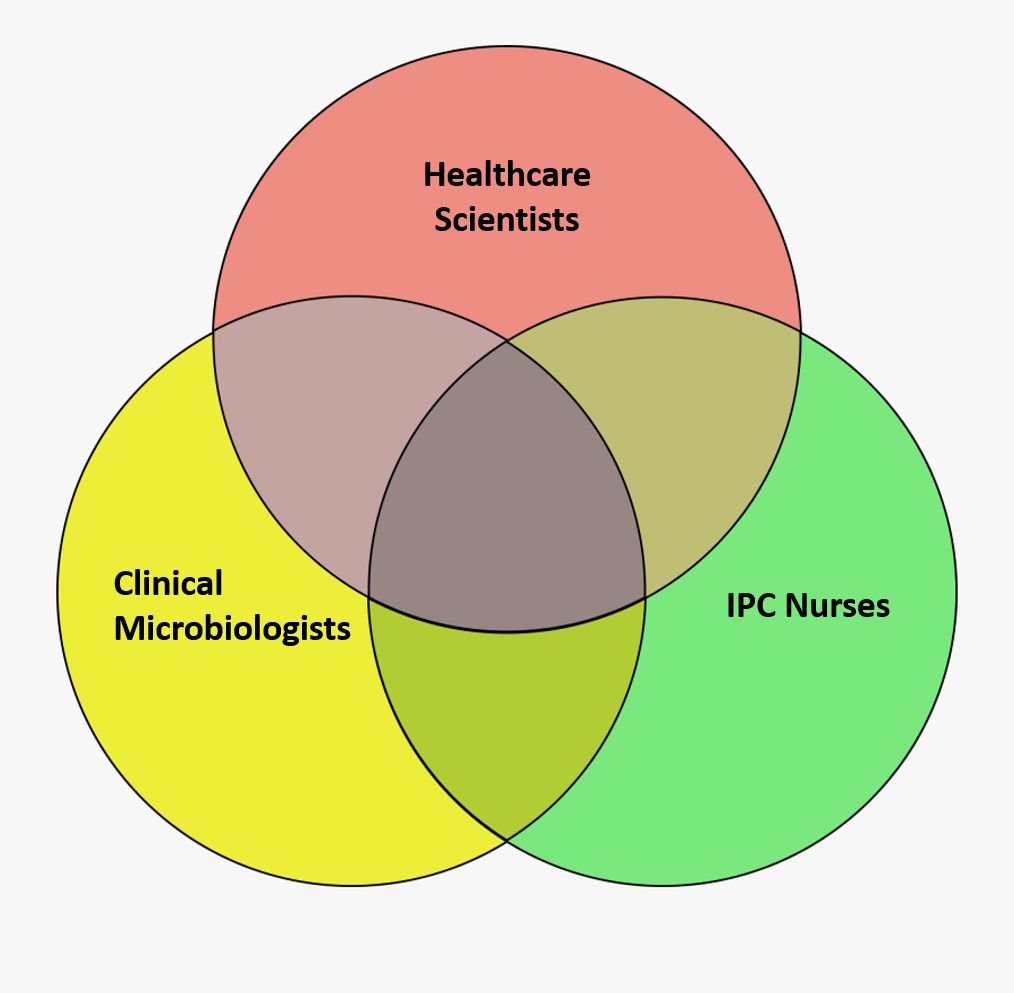
Infection control is a highly complex discipline requiring complex thinking in order to address the problems we face. The strength of a multidisciplinary approach is that we bring all of the advantages of our different approaches to the table, whist compensating for each other’s weaknesses. As a scientist I can be focussed on standardisation, consistency and evidence evaluation. This is useful, but can sometimes be limiting. My colleagues push me to be more flexible in my thinking, thus helping me innovate. They ask questions and then push me to see what solutions could be used. I can also sometimes be too engaged in the ‘vision piece’, which enables us to acquire grant funding to support changes in practice. My team ground me and keep me focussed on impact by asking ‘so what’. We learn from each other and crucially appreciate what one another add to the mix.
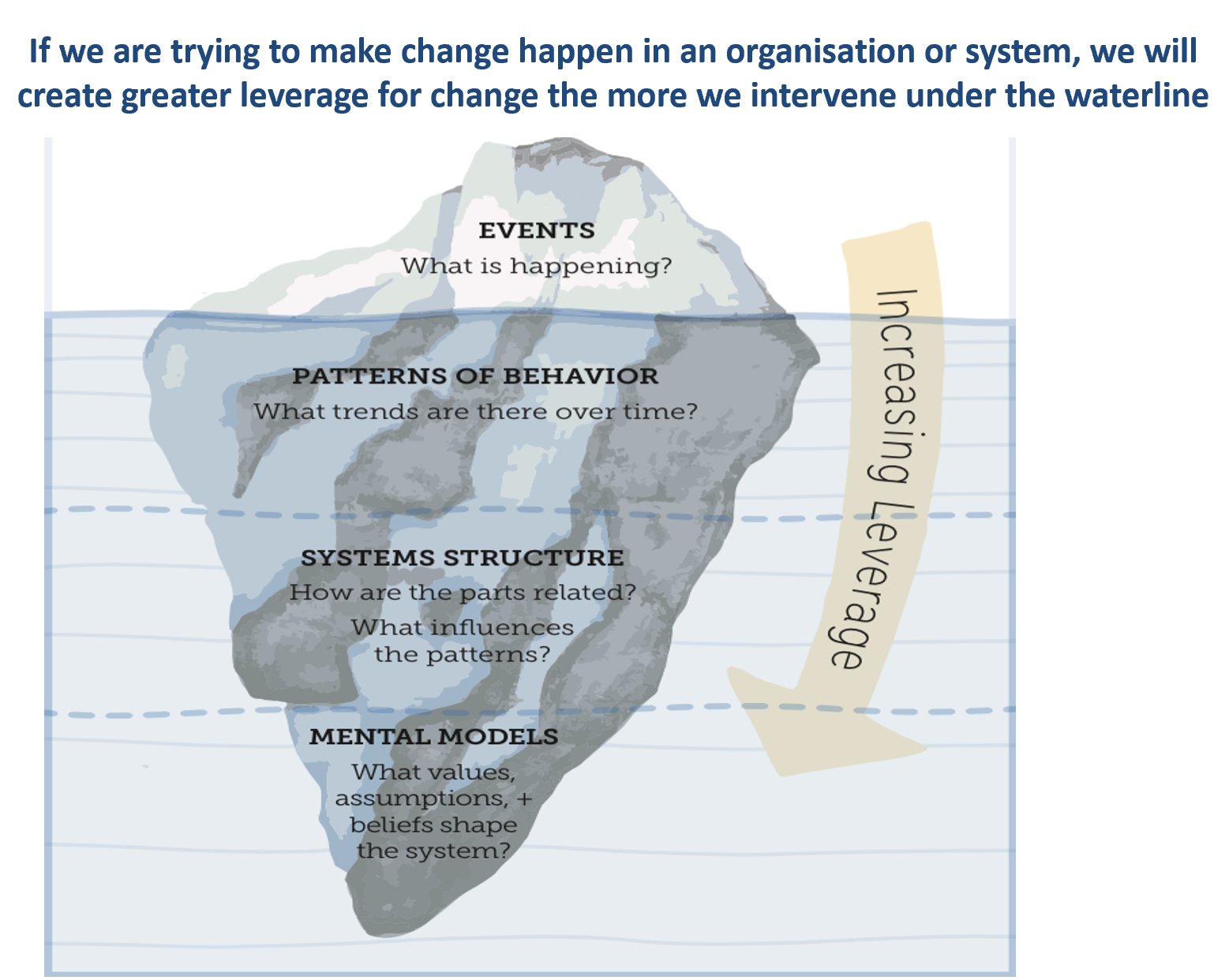
I feel we’ve made headway in achieving this recognition within individual teams and, more recently, across the IPC professional landscape. What the reviewer’s response has shown me is that we have a hell of a lot to do to get the same recognition for our contribution across the healthcare system. Moving away from the traditional structure is going to be key, however, if we are going to make the changes that need to happen to ensure the quality of NHS care.
I normally finish my blogs with advice or actions. This time I feel its more of a call to action, along with some questions:
- What can we do together to change this?
- How do we reach out more widely to show the improvements and the impact made by this approach?
I’d really value any thoughts. I would also value us all challenging opinions, when we hear them, that suggest we are not all equal within our teams. Maybe the main thing is to start the conversation. By doing so, we may bring these attitudes into the open, engage with discussion about them, and talk about how they impact individuals, teams and systems. This may, perhaps, stop them being voiced in anonymous reviews where the reader cannot engage with the source, in order for us to learn and move forward.
All opinions on this blog are my own

Leadership is key and co-designing the best model of multi-professionalism through courageous and open dialogue would allow the emergence of value based teams and systems. Leading care should not be about positional title but should be less boundary-driven in order to bring about a cultural environment where everyone is valued.
LikeLike